
Abstract
Background
Doravirine is a non-nucleoside reverse transcriptase inhibitor (NNRTI) showing high efficacy and tolerability in both naïve and experienced people living with HIV (PLWHIV) in randomized trials, but scarce data are available to date from the real-life experience.
Methods
We performed an observational, retrospective study of PLWHIV on suppressive antiretroviral therapy who switched to a daily single-tablet regimen containing doravirine 100 mg, lamivudine 300 mg, and tenofovir disoproxil fumarate 300 mg.
Results
As a whole, 62 suppressed patients (51 men, median age, 51.7 years; median CD4 T+ lymphocyte count, 577 cells/mm3) were enrolled. After 12 months, 58 (93.5%) patients showed HIV RNA <20 copies/mL and reasons for treatment failure were virological failure in one case, missing data in one case, and adverse events in two cases. At month 12, a significant decrease in median serum level of triglycerides (median change −61.2 mg/dL; p = .009) and total cholesterol (median change −38.4 mg/dL; p = .021) was reported, while a not significant median weight increase was registered (+0.55 kg).
Conclusions
In our study, simplification to a single-tablet regimen of doravirine/lamivudine/tenofovir disoproxil fumarate in virologically suppressed PLWHIV was effective and showed a good tolerability profile, in association with a significant improvement in serum lipid levels.
Introduction
Doravirine is a novel non-nucleoside reverse transcriptase inhibitor (NNRTI) with the potential to be an important therapeutic option in both antiretroviral therapy-naive and -experienced people leaving with HIV (PLWHIV). Doravirine shows a unique in vitro resistance profile among NNRTIs and is active against the most common NNRTI-resistant variants at concentrations achieved with once-daily dosing, can be taken without food, and has a low potential for drug-drug interactions, including with gastric acid modifiers, statins, metformin, and oral contraceptives.1–3
Randomized trials have shown efficacy and safety of doravirine-based antiretroviral regimens in both antiretroviral therapy-naïve and -experienced subjects.
In a phase 3 trial in tratment-naive PLWHIV, doravirine given once-daily with two nucleoside reverse transcriptase inhibitors (NRTIs) demonstrated noninferior efficacy to ritonavir-boosted darunavir plus two NRTIs. 4 Similarly, doravirine in a single-tablet regimen with lamivudine and tenofovir disoproxil fumarate showed noninferior efficacy to the single-tablet regimen tenofovir disoproxil fumarate-emtricitabine-efavirenz. 5 Moreover, in both trials the doravirine-based regimen showed a favourable tolerability profile with a negligible effect on plasma lipid concentrations, and two randomized studies demonstrated a lower incidence of neuropsychiatric adverse events in doravirine-treated patients in comparison with those treated with efavirenz.6,7
The efficacy of the doravirine-based single-tablet combination has been demonstrated in experienced patients too. In a randomized, open-label trial in virologically suppressed PLWHIV, the switch to doravirine/lamivudine/tenofovir disoproxil fumarate was noninferior to continuation of the previous regimen, with high rates of virological suppression and low rates of virological rebound, in association with a favourable safety profile and a significant improvement in lipid levels in subjects previously treated with protease inhibitors.8,9
Although data suggest that the prevalence of doravirine resistance mutations in historic NNRTI-exposed patients is low, 10 clinical evidence supporting successful doravirine use in antiretroviral therapy-experienced PLWHIV is lacking.
The aim of our observational study is to evaluate efficacy and safety of switching to the single-tablet regimen doravirine-lamivudine-tenofovir disoproxil fumarate in PLWHIV on stable antiretroviral therapy and with durably suppressed HIV viral load.
Methods
We performed an observational, retrospective study of PLWHIV referring to our Clinic of Infectious Diseases from September, 2016 through August, 2018, receiving a stable antiretroviral regimen for at least 12 months, with undetectable plasma HIV viral load (HIV RNA <20 copies/mL) for at least 6 months, and who were switched to a daily single-tablet regimen of doravirine (100 mg), lamivudine (300 mg), and tenofovir disoproxil fumarate (300 mg) (DOR/3TC/TDF). All the enrolled subjects were followed-up for 12 months.
Exclusion criteria were age <18 years, previous virological failure to lamivudine/emtricitabine or NNRTIs and/or genotypic testing showing reduced sensitivity to lamivudine/emtricitabine or NNRTIs, active opportunistic diseases or severe infectious diseases, alcohol abuse or intravenous drug dependence, alanine aminotransferase (ALT) or aspartate aminotransferase (AST) > 80 U/L, creatinine >1.5 mg/dL, spot urine proteinuria >20 mg/dL, phosphorus <2.5 mg/dL, pregnancy, an underlying treatment with medications or herbal supplements known to affect the pharmacokinetics of current antiretroviral drugs. Alcohol abuse and intravenous drug dependence were defined as a daily alcohol consumption >30 g and
Demographic, clinical, and laboratory data were recorded at the start of therapy and at 4-month intervals during the 12-months follow-up. All the plasma samples were analyzed for HIV-RNA level using the automated COBAS AmpliPrep Instrument for specimen processing and the COBAS TaqMan Analyzer for amplification and detection (Roche CobasAmpliPrep/Cobas TaqMan HIV-1 tests version 2.0; Roche Diagnostics, Mannheim, Germany). Virologic failure was defined by a confirmed plasma HIV RNA
Treatment failure was defined by confirmed virological failure or permanent discontinuation of current antiretroviral therapy. Genotypic testing was performed in case of virological failure. Virological success was defined as a HIV RNA <20 copies/mL on the study antiretroviral regimen at the end of the 12-months follow-up. Results were evaluated both in intention-to-treat (ITT) and per-protocol (PP) analyses. The ITT analysis included all subjects who switched to DOR/3TC/TDF and were enrolled into the study, and missing data were considered as failures. The PP analysis included all the ITT patients except those who discontinued the dual regimen for reasons other than a virological failure.
Data are presented as medians with interquartile range (IQR) for descriptive data, while comparisons between groups were performed by Student t test or Fisher exact test (where appropriate). The significance of changes in all the considered variables were assessed using the paired Student t test. The primary outcome of this study was the evaluation of both efficacy and safety of this antiretroviral regimen, while the secondary endpoints were changes in serum lipid parameters, weight, BMI, and renal function parameters.
The adherence to the current therapy were carefully checked on the outpatient visits by self-reported questionnaires. The study was approved by the Ethic Committee of the S.Orsola-Malpighi Hospital and all participants signed an informed consent after receiving information about the purpose of the study.
Results
Study inclusion criteria were met by 62 patients who were enrolled in the study. Median age (IQR) was 51.7 (45.4–58.8 years) years, 51 patients (82.2%) were males, 58 (93.5%) were Caucasian, median current CD4+ lymphocyte count (IQR) was 577 (338, 889) cells/mm3, median duration (IQR) of current antiretroviral treatment was 5.2 (2.3, 7.6) years, and median duration (IQR) of plasma HIV RNA <20 copies/mL with the current antiretroviral regimen was 58.3 (24.4, 83.6) months.
At baseline, median BMI (IQR) was 24.3 (19.1, 29.4) kg/m2 and nine subjects (14.5%) had BMI >25 kg/m2. The lipid parameters were frequently abnormal: 52 subjects (83.9%) had triglycerides >150 mg/dL, and 43 (69.4%) had total cholesterol >200 mg/dL.
Baseline characteristics of the 62 patients enrolled in the study.
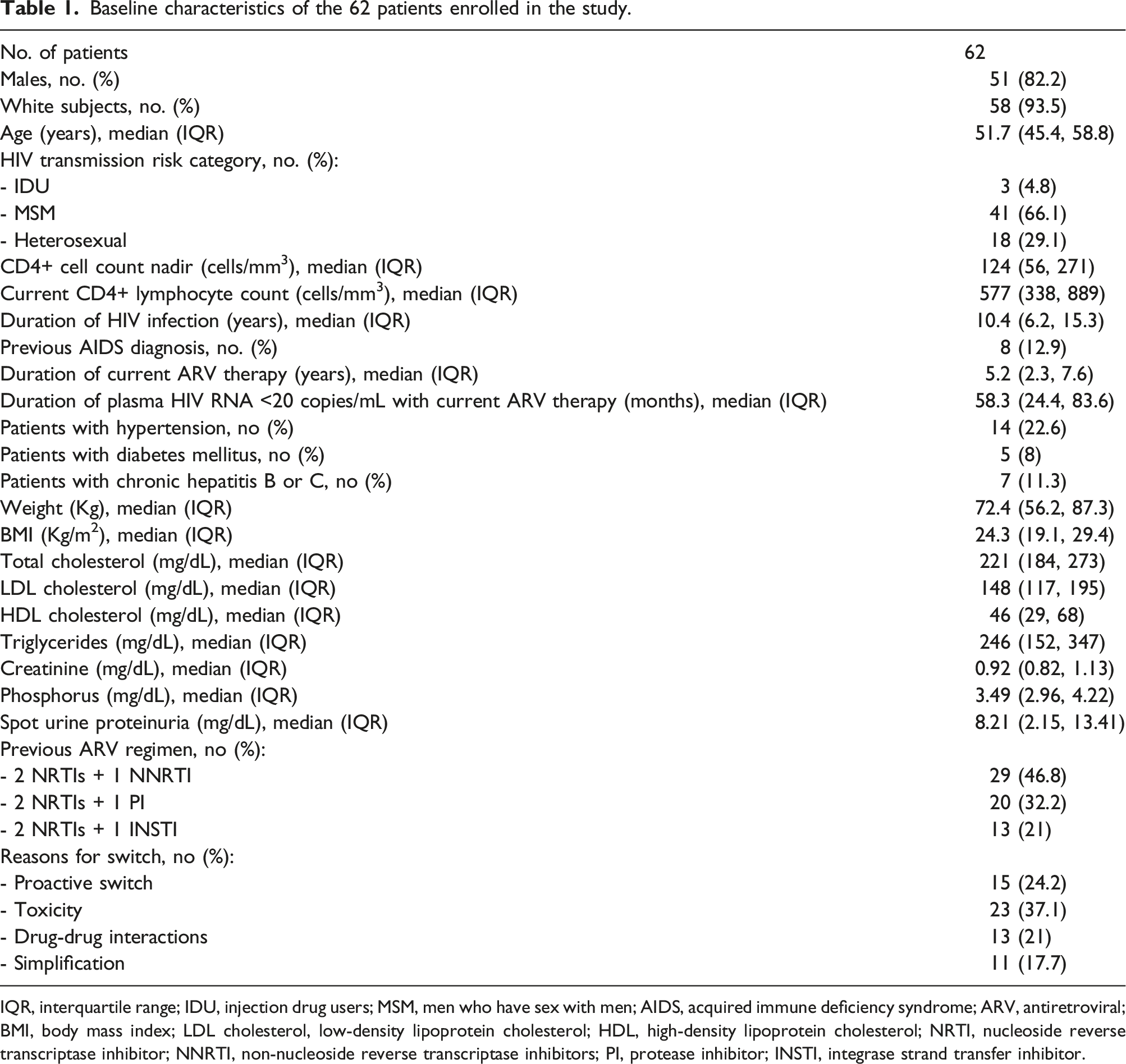
IQR, interquartile range; IDU, injection drug users; MSM, men who have sex with men; AIDS, acquired immune deficiency syndrome; ARV, antiretroviral; BMI, body mass index; LDL cholesterol, low-density lipoprotein cholesterol; HDL, high-density lipoprotein cholesterol; NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, non-nucleoside reverse transcriptase inhibitors; PI, protease inhibitor; INSTI, integrase strand transfer inhibitor.
Current antiretroviral therapy included two nucleoside reverse transcriptase inhibitors (NRTIs) plus one NNRTI in 29 cases (46.8%), two NRTIs plus one ritonavir- or cobicistat-boosted protease inhibitor (PI) in 20 (32.2%), and two NRTIs plus one integrase strand transfer inhibitor (INSTI) in 13 (21%). Current NRTIs were tenofovir disoproxil fumarate/emtricitabine in 38 cases (61.3%), tenofovir alafenamide/emtricitabine in 13 (21%), and abacavir/lamivudine in 9 (14.5%).
The reasons for switch to DOR/3TC/TDF were toxicity in 23 patients (37.1%), proactive switch in 15 (24.2%), drug-drug interactions in 13 (21%), and simplification in 11 (17.7%). Toxicity included high serum levels of triglycerides and/or total cholesterol in 19 cases (30.6%), sleeping disturbances in 10 (16.1%), and gastrointestinal symptoms in 7 (11.3%).
Immunological, virological and biological results 12 months after the switch to doravirine/lamivudine/tenofovir disoproxil fumarate.
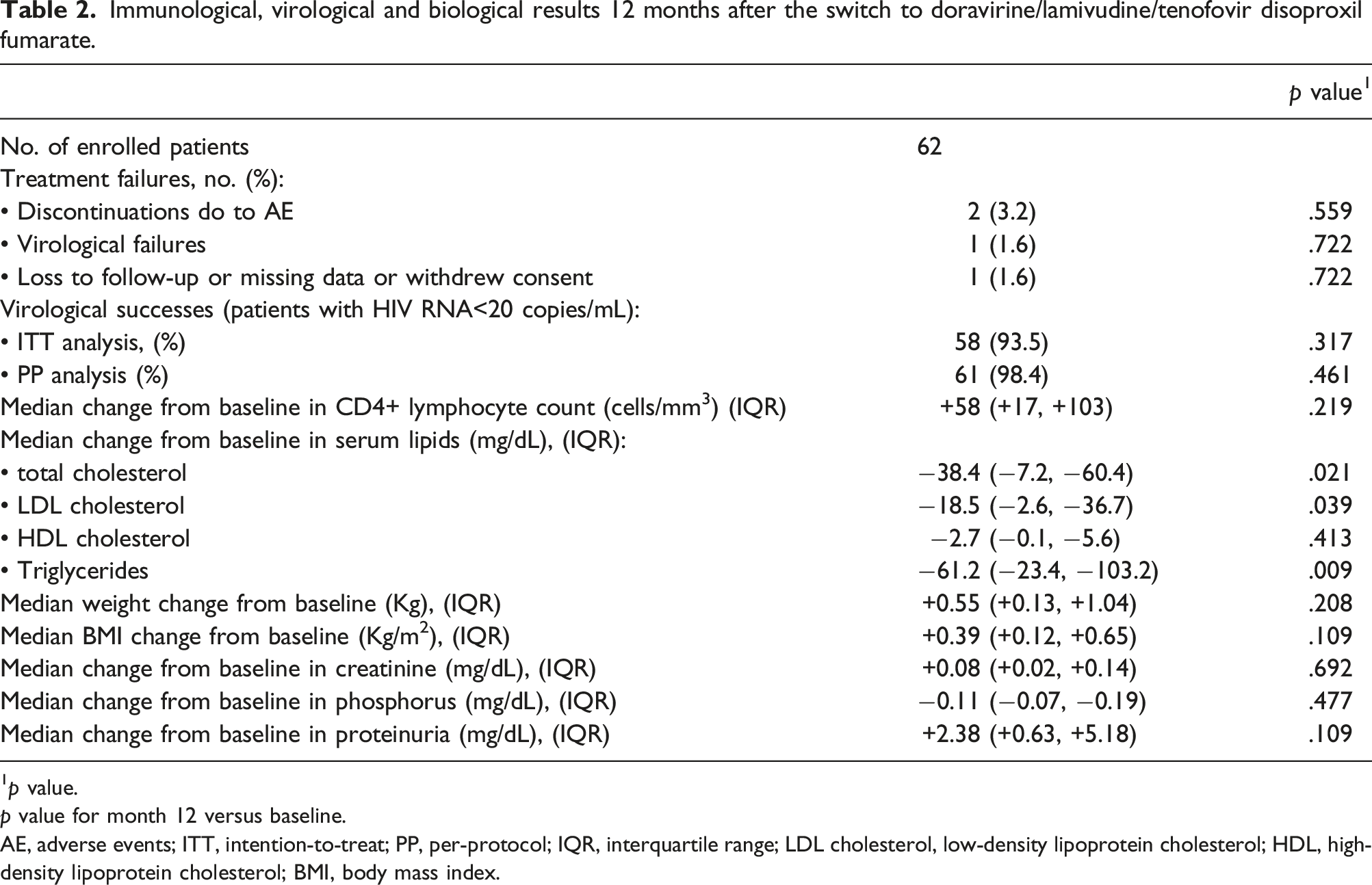
1p value.
p value for month 12 versus baseline.
AE, adverse events; ITT, intention-to-treat; PP, per-protocol; IQR, interquartile range; LDL cholesterol, low-density lipoprotein cholesterol; HDL, high-density lipoprotein cholesterol; BMI, body mass index.
After 12 months, four treatment failures were observed on the whole: one discontinuation due to virological failure, two discontinuations due to non-serious adverse events, and virologic data missing for one participant at month 12. Overall, virological success at month 12 was 93.5% in the ITT analysis and 98.4% in the PP analysis (Table 2).
The unique case of confirmed virological failure was observed at month 8 (HIV RNA rebound to 2610 copies/mL) in a patient who had been virologically suppressed for 48 months with the regimen tenofovir alafenamide/emtricitabine/darunavir/cobicistat. The patient’s adherence to cART was lower than 90% and genotypic analysis at virological failure demonstrated no resistance mutations for NRTIs, NNRTIs or PIs. After the virological rebound, this patient restarted tenofovir alafenamide/emtricitabine/darunavir/cobicistat and reached a plasma HIV RNA <20 copies/mL within four months.
Overall, at month 12 the adherence to the antiretroviral treatment was
The two discontinuations for non-serious adverse events were due to diarrhea with abdominal discomfort in both cases. The unique patient with missing data at month 12 had HIV RNA <20 copies/mL at the previous visit (month 8).
The unique patient with virological failure and both subjects with treatment discontinuation for adverse events returned to their previous antiretroviral regimen (tenofovir alafenamide/emtricitabine/darunavir/cobicistat in the first case, and tenofovir alafenamide/emtricitabine/rilpivirine in other two cases), and obtained plasma HIV RNA<20 copies/mL after 3 months.
The median change (IQR) in the CD4+ T lymphocyte count at month 12 was +58 (+17, +103) cells/mm3.
During the 12-months follow-up a significant decrease in median concentrations of total cholesterol, LDL cholesterol and triglycerides was reported (−38.4, −18.5, and −61.2 mg/dL, respectively). At the same time, a slight and not significant increase in median weight and BMI was reported at month 12 (+0.55 kg and +0.39 kg/m2, respectively). No significant changes were reported in the median values of serum creatinine, phosphorus, and proteinuria in comparison with respective baseline values (Table 2).
No serious adverse events were reported during the 12-months follow-up, and no grade 3 or 4 clinical events or laboratory abnormalities were recorded. Overall, the most common adverse events observed during the follow-up were diarrhea with abdominal discomfort (8 patients; 12.9%), nausea and loss of appetite (5; 8.1%), headache (5; 8.1%), and asthenia (4; 6.4%).
Discussion
Due to its favourable properties shown in randomized trials,8,9 including no effect on lipid values and minimal drug-drug interactions, doravirine-based regimens may be a valuable switching strategy in experienced patients with stable virological suppression, and mostly in aging people with comorbidities and polypharmacy. However, results from clinical trials do not always translate directly to the “real-life” setting, and data from observational studies are still limited.
An observational, retrospective report evaluated 33 virologically suppressed patients who started a doravirine-based regimen including a tenofovir-based backbone (with tenofovir disoproxil fumarate or tenofovir alafenamide). In the survival analysis, estimated probability of maintaining doravirine was 93.8% after 6 months and 80.4% after 12 months. 11
A retrospective analysis included 16 PLWHIV who transitioned to doravirine-containing regimens for various reasons, with baseline viral load <50 copies/mL in 11 of 16 subjects. A suppressed viral load was maintained or achieved in 12 patients after 6 months, and doravirine-based regimens were well tolerated, with no patients reporting adverse effects. 12
An observational, prospective study evaluated 77 PLWHIV who started a doravirine-based regimen, of which 73 were treatment-experienced subjects with baseline undetectable viral load in 66 cases. Overall, the global rate of virological failure at week 48 was 7%, and only one patient had a HIV viral load >50 copies/mL, with no resistance mutations detected to any of current antiretroviral drugs. 13
In a retrospective, multicenter cohort, 132 antiretroviral therapy-experienced patients switched to doravirine-containing regimens were evaluated. After 24-weeks follow-up, no significant changes were reported regarding the proportion of subjects with virological suppression (94.2%), CD4+ T lymphocyte count, body weight and serum creatinine level, while a significant decrease was observed in both total cholesterol and triglycerides. 14
In a retrospective cohort of 40 virologically suppressed PLWHIV switched to a regimen with doravirine plus two NRTIs, a significant decrease in median values of total cholesterol, LDL cholesterol and triglycerides were reported, in association with a reduction in median predicted 10-years risk of cardiovascular disease. 15
The coformulation of doravirine with tenofovir disoproxil fumarate (TDF) and lamivudine in a single-tablet regimen raised some concerns following the documented risk of renal toxicity and treatment discontinuation associated with TDF exposure. However, studies in healthy volunteers and PLWHIV have shown that concomitant administration of doravirine had no significant effects on the pharmacokinetics of tenofovir from TDF, suggesting a lower potential risk of renal toxicity of the DOR/3TC/TDF combination.16,17
In our study, switching to a single-tablet regimen of DOR/TDF/3TC was a valuable option for maintaining viral suppression in PLWHIV, with high rates of virological supression (ranging between 93.5% and 98.4%) after 12-months follow-up. Only one patient had virological failure but genotypic analysis demonstrated no doravirine or NRTI-associated resistance mutations. DOR/TDF/3TC showed a favourable safety profile over 12 months of treatment, with a significant improvement in lipid parameters and a not significant increase in median body weight.
Our work clearly has several limitations. First, it was a single-center, observational, retrospective study with a limited sample size. Second, sample size calculation, statistical power and confidence intervals were not evaluated. Third, the study population was predominantly Caucasian, elderly patients were absent, and a pharmacokinetic analysis was not performed. Fourth, the effectiveness of single-tablet regimen DOR/TDF/3TC was not compared with other standard triple or dual regimens. In spite of this, the rate of virological suppression was high and similar to that observed with antiretroviral regimens employed before the switch. Finally, some aspects, such as the control of viral replication in the central nervous system or other reservoirs and the effect on the immune activation markers or peripheral fat were not evaluated in the present study.
To conclude, in clinical practice switching to doravirine in a single-tablet regimen with tenofovir disoproxil fumarate and lamivudine represents an effective and safe option in virologically suppressed PLWHIV, especially in patients with dyslipidemia and weight gain.
Footnotes
Author contributions
Calza L. conceived the research study. Colangeli V. collected clinical data. Bon I. and Pensalfine G. collected laboratory data. Appolloni L. and Vitale S. performed the analysis. Calza L. and Viale P. finalized the manuscript. All Authors critically appraised the manuscript and approved its submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosure statement
Calza L. has received research grants from ViiV and Gilead Sciences, and has received honoraria for consulting (as advisory board member) and speaking from Merck Sharp & Dohme, ViiV, Gilead Sciences, Janssen, and Bristol-Myers Squibb. Colangeli V. has received honoraria for consulting (as advisory board member) and speaking from Merck Sharp & Dohme, ViiV, Janssen, and Bristol-Myers Squibb. Viale P. has received honoraria and/or support from Biomerieux, Gilead Sciences, Merck Sharp & Dohme, Novartis, and Pfizer.