
Abstract
Background
Antiretroviral therapy has increased the life expectancy of people living with HIV. However, this increase is not free of comorbidities, and metabolic syndrome is one of the most prevalent. Berberine is an alkaloid nutraceutical that has been shown to ameliorate metabolic disorders such as prediabetes, polycystic ovary syndrome, and non-alcoholic fatty liver disease. However, it has not been tested in HIV infection. Therefore, we conducted a randomized controlled trial to evaluate the efficacy of berberine in improving metabolic syndrome.
Methods and results
In this double-blind, placebo-controlled trial, adults living with HIV under virological suppression and metabolic syndrome received either berberine 500 mg TID or placebo for 20 weeks. The primary outcomes were a composite of weight reduction, insulin resistance decrease, and lipid profile improvement. A total of 43 participants were randomized (22 in the berberine group and 21 in the placebo group); 36 participants completed the follow-up and were analyzed. The berberine group showed a reduction in weight and body mass index, lower insulin resistance, and a reduction in TNF-alpha. The control group had higher total cholesterol, c-LDL, and IL-6 concentration.
Conclusion
In people living with HIV under virological suppression, berberine was safe and improves clinical and biochemical components of metabolic syndrome. However, further studies with more participants and longer intervention periods need to be explored.
Keywords
Introduction
With current antiretroviral therapy (ART), most people living with HIV (PLWH) achieve virologic suppression and immune reconstitution, leading to increased life expectancy. However, this is not exempt from other comorbidities. Metabolic syndrome (MetS), characterized by decreased glucose tolerance and increased insulin resistance, is gaining importance due to increased prevalence and earlier presentation in the HIV-positive population, predisposing them to cardiovascular diseases.1–3
Prevalence of MetS in HIV ranges from 7% to 45%.4,5 Among Latin American PLWH receiving ART, it has been reported up to 20.2%. 6
Some studies have investigated the pathophysiology and relation between MetS and cardiovascular complications in HIV infection.3,7 Maloberti et al. reported a higher prevalence of MetS in PLWH receiving ART (19.4%) and treatment-naive (13.8%) compared to HIV-negative controls (4.5%), suggesting that HIV infection per se plus HIV-related chronic immune activation are critical factors linked with these comorbidities. 8 Other coexisting circumstances, such as immune system dysregulation, chronic bacterial translocation, proinflammatory states, endothelial dysfunction, hypercoagulable state, adipocyte dysfunction, and activation of the renin-angiotensin-aldosterone-system have been well recognized in HIV infection and are conditions related with some components of MetS and higher cardiovascular risk.5,9,10
Recently, there has been an acknowledgment that ART plays a relevant role in obesity, insulin resistance, and cardiovascular risk. 5 Sax et al., conducted a pooled analysis of eight randomized comparative clinical trials of first-line ART initiation and found that regimens based on integrase inhibitors (INSTIs) were associated with more weight gain than second-line regimens such as protease inhibitors (PIs) or non-nucleoside reverse transcriptase inhibitors (NNRTIs). 11 A follow-up from the ADVANCE trial demonstrated that an INSTI + tenofovir alafenamide (TAF) combination was related to more weight gain and percentage of clinical obesity than INSTI + Tenofovir disoproxil (TDF) or than Efavirenz/Tenofovir Disoproxil/Emtricitabine. Also, this trial demonstrated that women were more affected than men, and this effect persisted through 192 weeks after initiation of treatment.12,13
Later studies have shown that INSTIs raise the risk of developing diabetes mellitus (48%) or having high blood glucose (31%) within 6 months of starting treatment.14,15 Additionally, nucleoside reverse transcriptase inhibitors (NRTIs) and PIs may be associated with an increased risk of developing MetS by 2.4 times. 3 For all these reasons, ART is now recognized as another metabolic risk factor. 2
The management of MetS can be divided into non-pharmacologic and pharmacologic. Non-pharmacologic strategies encompass nutritional therapy, physical activity (at least 150 min/week of moderate-intensity aerobic physical exercise), decreased alcohol intake, and improved quantity and quality of sleep. The principal pharmacologic strategies are (i) Medical or surgical management of obesity; (ii) pharmacologic strategies to reduce insulin resistance; (iii) Treatment of dyslipidemia; and (iv) hypertension treatment, that includes reducing salt intake and anti-hypertensive drugs use. 16
Berberine is an isoquinoline alkaloid i.e. isolated from some medicinal herbs, such as the Chinese herb Huanglian, Berberis aquifolium, and Berberis vulgaris. 17 It has proven beneficial effects on both glucose tolerance and insulin resistance in different scenarios,18–20 but it has not been tested in PLWH under ART with virological suppression. Berberine is considered a complement to the dietary lowering lipid approach but not as a treatment mainstay for lipid management. 21 We hypothesized that berberine would improve some clinical features, insulin resistance, metabolic profile, some inflammatory markers, and cardiovascular risk in PLWH on ART with virological control without significant interactions nor severe adverse effects.
Materials and methods
Study type and population
A pilot randomized, double-blind, placebo-controlled clinical trial was designed with two groups, each one with 20 patients: group A) Berberine 500 mg per capsule three times daily for 20 weeks, and group B) Placebo (calcinate magnesia) 400 mg per capsule three times daily for 20 weeks. Both capsules were of the same characteristics; the use of calcined magnesia as a placebo was chosen due to its availability among all substances approved for use as a placebo. The inclusion criteria were: age between 18 and 60 years; documented HIV-1 infection on stable ART (based on Bictegravir/Tenofovir Alafenamide/Emtricitabine) at least 6 months before enrolment with viral suppression; metabolic syndrome, defined by criteria according to the 2005 NCEP-ATP III criteria for MetS; 22 non-previously known kidney or liver disease; signed informed consent. Exclusion criteria were: prior atherosclerotic cardiovascular disease; diabetes mellitus type 1 or 2; previous use of hypoglycemic and/or lipid-modifying medication; pregnancy; poor treatment compliance (<90%); or failure to attend at the final visit for blood sampling; and withdrawal of informed consent.
Intervention
Participants were randomly assigned using an MS Excel program to receive berberine or placebo, one capsule after each meal for 20 weeks. All participants received medical, nutritional guidance according to the American Diabetes Association and the Obesity Society (AHA/ACC/TOS); we emphasized consumption of fiber according to weight, and avoidance of saturated and trans fats;23,24 also, we recommended maintaining the same physical activity that was part of their daily routine to avoid interfering with the final outcomes.
Berberine and placebo were obtained through vendor Farmacia Vidrio (farmaciasmexico.com). Treatment compliance of ≥90% was considered satisfactory, and it was evaluated monthly by medication counting during each medical visit. Adverse events related or not related to berberine were also evaluated. Unblinding did not take place until all protocol procedures were completed.
Anthropometric measures
Anthropometric assessments were performed in the morning; patients should be wearing light clothing and be in a fasted state. Height (cm) and weight (kg) were measured using a calibrated stadiometer and scale (Seca 700). Waist circumferences were obtained in triplicate at the midpoint between the lowest rib and the iliac crest in a standing position; hip circumferences were measured at the largest circumference around the buttocks with a flexible narrow non-stretchable tape by a nutritionist. Body mass index (BMI) was classified according to WHO criteria.
Metabolic measurements and general safety laboratory studies
Basal and final measurements of hematology, glucose, creatinine, urea, total cholesterol, LDL-c, HDL-c, VLDL-c, triglycerides, high sensitivity C-reactive protein (hs-CRP), total bilirubin, total proteins, albumin, AST, ALT, GGT, alkaline phosphatase, HBsAg, anti-HCV antibodies, insulin, C-peptide, glucagon and glycated hemoglobin (HbA1c) were obtained, with at least 8 h of fasting.
Cardiometabolic and surrogate indexes for the evaluation of insulin resistance
The following cardiometabolic indexes were evaluated in each subject in both groups: the ratio of triglycerides divided by the concentration of HDL-c (TG/HDL ratio); 25 cardiovascular risk was estimated with the cardiovascular risk scale in HIV from the Data Collection on Adverse Effects of Anti-HIV Drugs Cohort (D:A:D). 26
For the evaluation of insulin resistance, the Homeostatic Model Assessment of Insulin Resistance (HOMA-IR) was used. The HOMA-%β was calculated to assess pancreatic beta–cell function, and also the HOMA-%S to identify the percentages of insulin sensitivity; both HOMAs were calculated through the calculator tool available at the website (https://www.dtu.ox.ac.uk/homacalculator/download.php) and according to Matthews et al.27,28 Other surrogate indexes for the evaluation of insulin action were performed, such as the TyG index and the TyG index*BMI with cut-off values of 8.17 and 208 respectively used for insulin resistance, according to Almeda-Valdés et al.29,30
Serum proinflammatory cytokines and enzymes measurement
The serum collection was obtained immediately after recruitment and in the last visit per the protocol of each subject that complied with all visits. The serum sample was obtained in a serum separator tube where the sample was let to clot for approximately 10 min at room temperature; then, the sample tube was centrifuged at 1600 g for 10 min; finally, the serum was collected and stored at −80°C until use. Serum levels of proinflammatory cytokines: IL-1β, TNF-a, and IL-6 were quantified by ELISA (AVIVA system Biology, No. cat: OKBB00176, USA; R&D system, USA; TECAN IBL International GmbH, Germany, respectively), as well as the enzymes: insulin, glucagon, and C-peptide (ALPCO, USA; ABCOM, USA, No. cat: ab267567, and ABCOM, USA, No. cat: ab260064, respectively), all of them according to the manufacturer instructions.
Statistical analysis
The sample size was calculated through a formula for clinical trials with a statistical confidence of 95%, a statistical power of 80%, a standard deviation (SD) for triglycerides of 11.5 mg/dL, and an expected difference of at least 40 mg/dL SD of triglycerides between groups, 31 obtaining a total of 20 patients in each group that included 20% of the expected loss in the follow-up period. Data were reported as mean and SD or median and interquartile range (IQR) for quantitative variables (depending on the gaussian distribution) and frequencies for qualitative variables. The inferential analysis was performed with the paired t-student or Wilcoxon signed-rank tests to compare intragroup differences and the unpaired t-student or Mann–Whitney U-test to compare intergroup differences. In addition, ANOVA or Kruskal-Wallis test with Bonferroni-Dunn correction was used depending on the gaussian distribution, and proportions were compared using Fisher’s exact test. All statistics were calculated using GraphPad Prism version 6 (GraphPad Software, La Jolla, CA, USA). The difference between the variables analyzed was considered statistically significant if p < 0.05. The analysis of Cliff’s delta was performed on RStudio v. 4.1.1 (2021-08-10) with the package “effsize” (v0.8.0, Tochiano, 2020) the+ parameter of delta value were <0.147 negligible, 0.474 large. 32
Results
A total of 48 PLWH were evaluated, and 43 participants were randomized, 22 in group A (Berberine (BBR)) and 21 in group B (control (CTR)). 62.8% were male, with a mean age of 46 ±9 years. Three participants in group A and four in group B were discontinuations; due to lost to follow-up and noncompliance to take the drugs. (Figure 1). Flowchart of participants selection and treatment.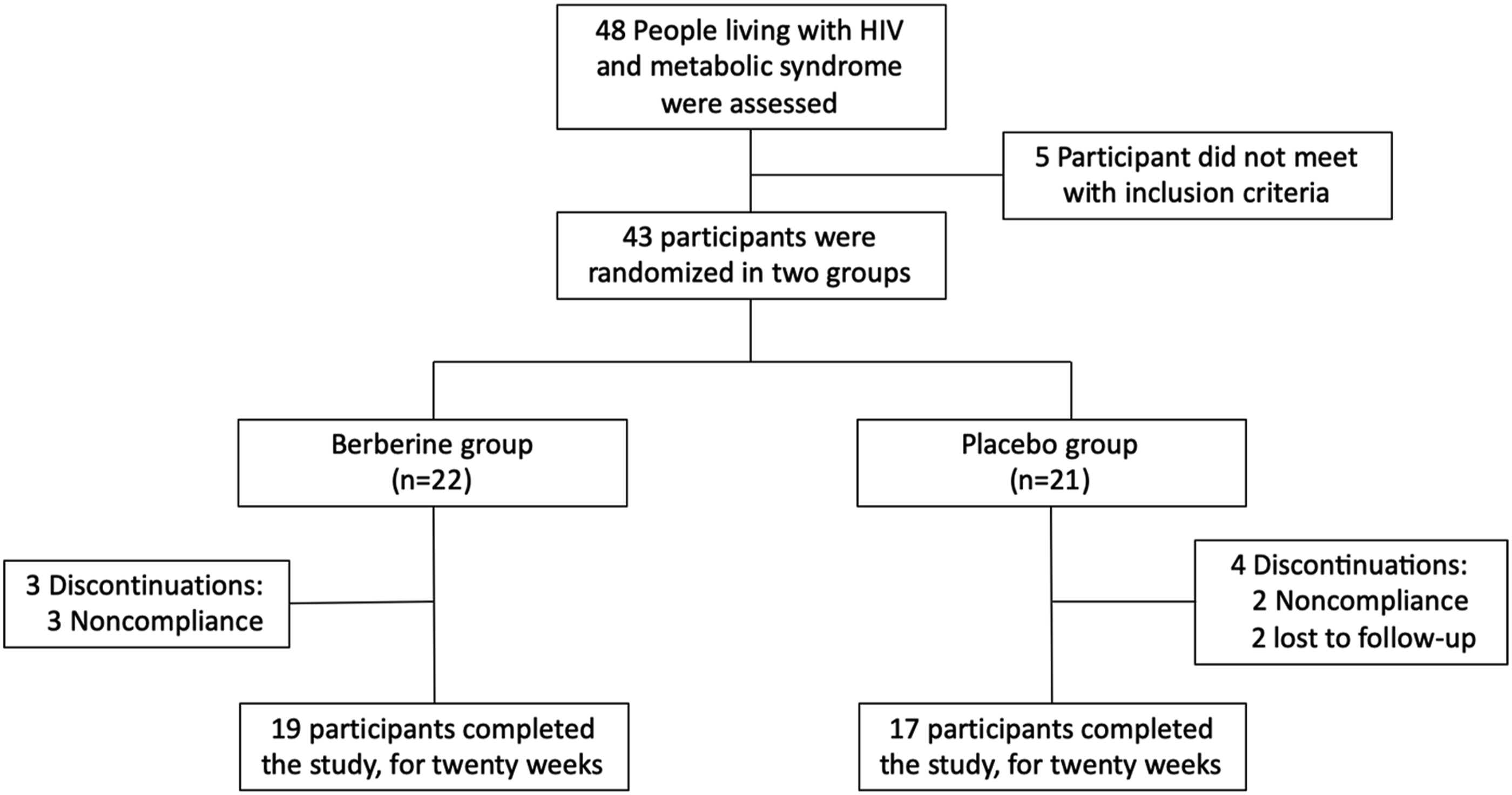
Demographics, clinical characteristics and laboratory tests of all participants.
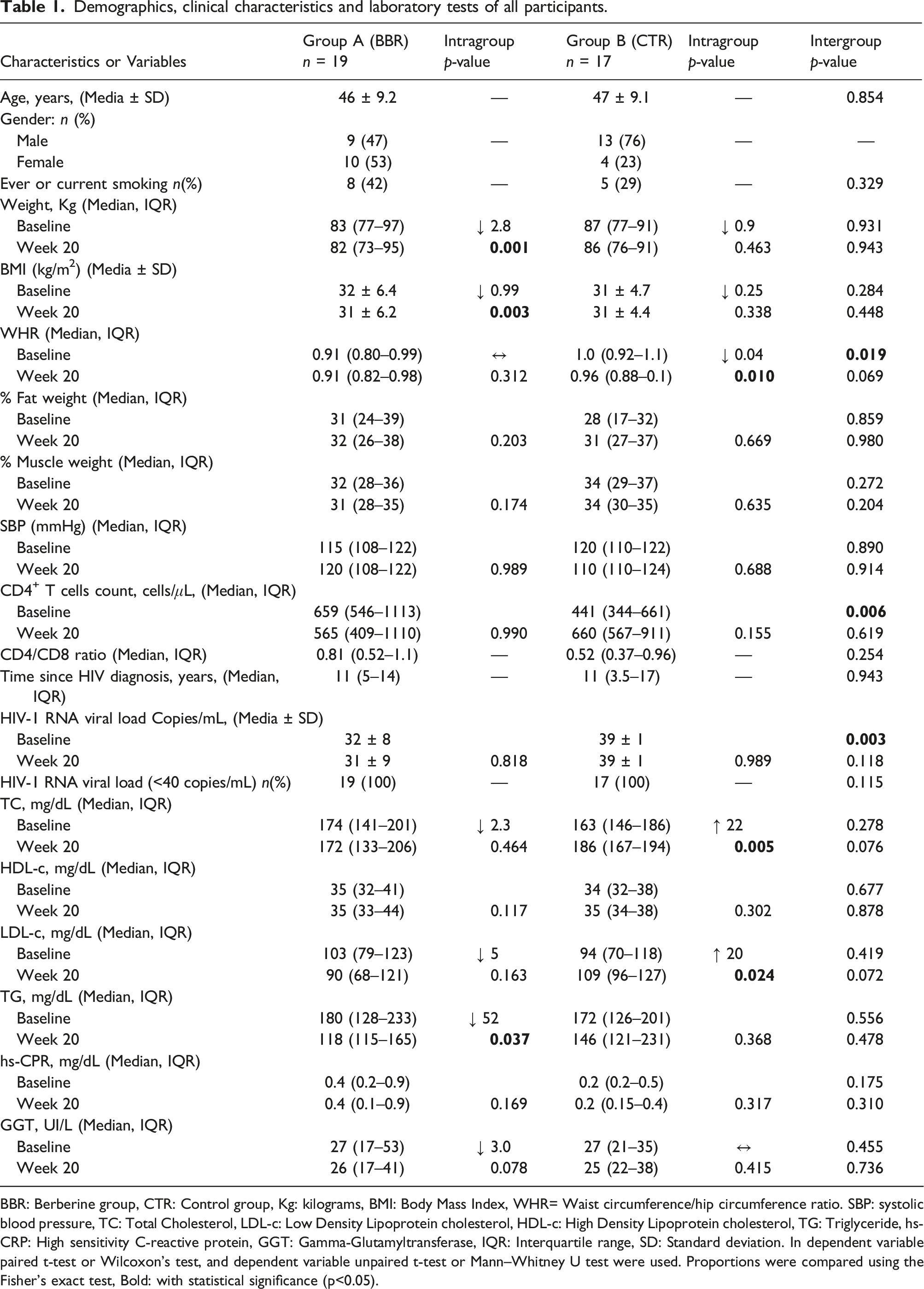
BBR: Berberine group, CTR: Control group, Kg: kilograms, BMI: Body Mass Index, WHR= Waist circumference/hip circumference ratio. SBP: systolic blood pressure, TC: Total Cholesterol, LDL-c: Low Density Lipoprotein cholesterol, HDL-c: High Density Lipoprotein cholesterol, TG: Triglyceride, hs-CRP: High sensitivity C-reactive protein, GGT: Gamma-Glutamyltransferase, IQR: Interquartile range, SD: Standard deviation. In dependent variable paired t-test or Wilcoxon’s test, and dependent variable unpaired t-test or Mann–Whitney U test were used. Proportions were compared using the Fisher’s exact test, Bold: with statistical significance (p<0.05).
The BBR group decreased weight significantly - 2.8 kg compared to 0.9 kg in the CTR group (p = 0.001), as well as the mean BMI (kg/m2) from 32 ± 6.4 to 31 ± 6.2 (p = 0.003) in BBR group versus from 31 ±4.7 to 31 ± 4.6 (p = 0.338) in CTR group.
CTR group showed a significant decrease in the WHR, median from 1.0 (0.92–1.1) to 0.96 (0.88–0.1), p = 0.010, while the BBR group kept the same measurements, from 0.91 (0.80–0.99) to 0.91 (0.82–0.98), p =.312. CTR group also had a significant elevation of total cholesterol (22 mg/dL; p < 0.005) at the expense of LDL-c (20 mg/dL; p = 0.024), contrasting with the BBR group in which a decrease in these variables was observed, although without statistical significance. Regarding triglycerides, only the BBR group showed a significant decrease (52 mg/dL; p = 0.037) (Table 1).
The CVR score increased significantly in both groups; however, at the end of the study, it was worse in the CTR group. With a median from 1.6 (0.4–2.8) to 1.7 (0.7–6.3), p = 0.004 in the BBR group compared to a median from 1.0 (0.4–2.2) to 3.6 (1.4–6.5), p < 0.0001 in CTR group.
Cardiometabolic, surrogate indexes for the evaluation of insulin resistance, and glycemia control enzymes.

BBR: Berberine group, CTR: Control group, HOMA-IR: Homeostatic Model Assessment of Insulin Resistance, HOMA-%β: Homeostasis Model Assessment estimates % pancreatic beta cell function (in steady state), HOMA-%S: Homeostasis Model Assessment estimates % insulin sensitivity, Hb1Ac: glycated hemoglobin, SD: Standard deviation, IQR: Interquartile range. In dependent variable paired t-test or Wilcoxon’s test, and dependent variable unpaired t-test or Mann–Whitney U test were used, Bold: with statistical significance (p<0.05).
Regarding lifestyle, 41.2% of participants in the CTR group reported having good compliance with changes in their nutritional habits and behaviors versus 10.5% of participants in the BBR group.
Immunological ratios and proinflammatory cytokines levels.
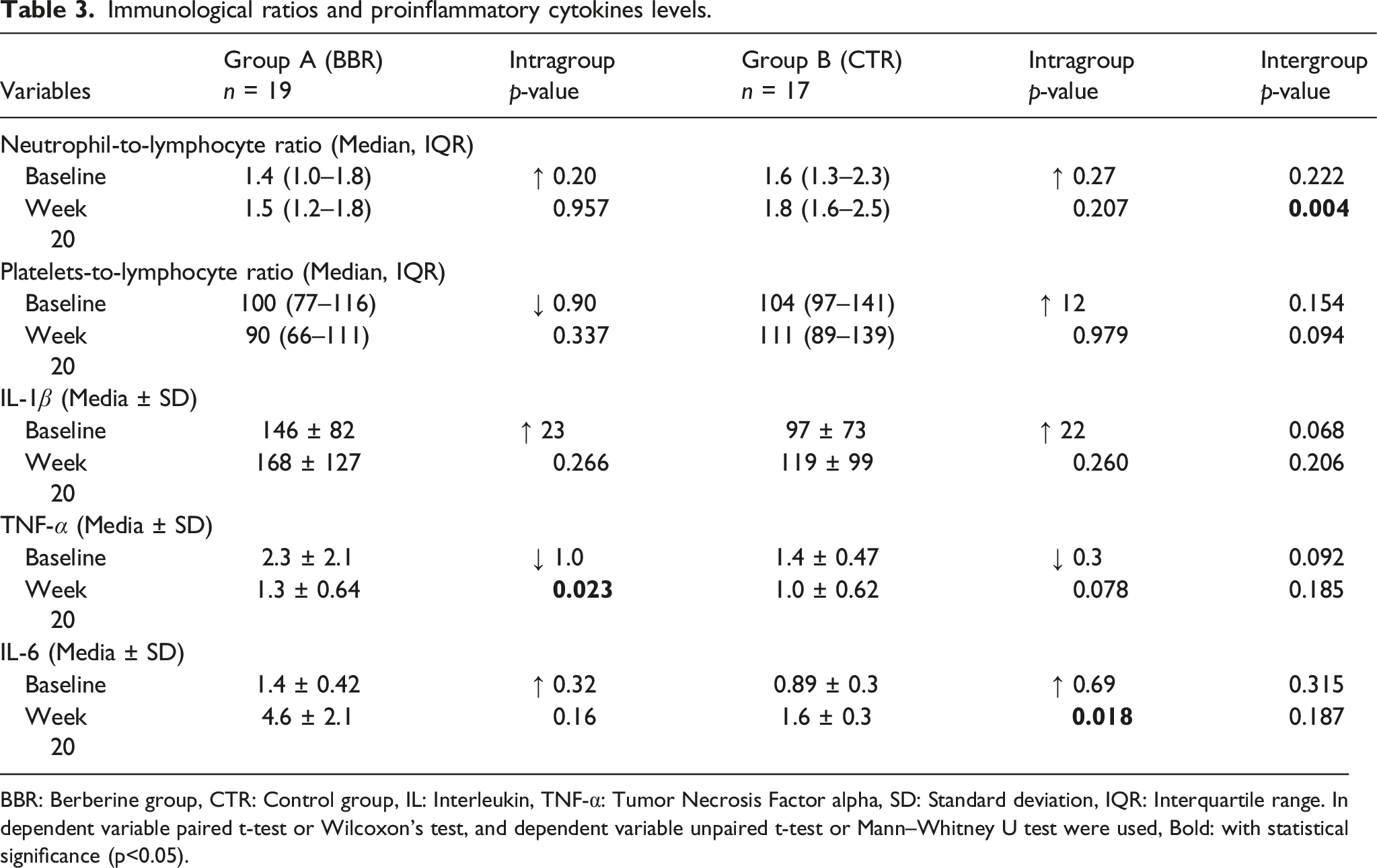
BBR: Berberine group, CTR: Control group, IL: Interleukin, TNF-α: Tumor Necrosis Factor alpha, SD: Standard deviation, IQR: Interquartile range. In dependent variable paired t-test or Wilcoxon’s test, and dependent variable unpaired t-test or Mann–Whitney U test were used, Bold: with statistical significance (p<0.05).
In the BBR group, some significant positive correlations were found between glycemia and TyG index*BMI (r = 0.8 (95% CI 0.5–0.9), p < 0.0001) (Figure 2(a)), hs-CRP and TyG index*BMI (r = 0.8 (95%CI 0.5–0.9), p < 0.0001) (Figure 2(b)), HOMA-IR and TyG index*BMI (r = 0.5 (95%CI 0.05–0.8), p = 0.014) (Figure 2(c)), and between hs-CRP and IL-6 (r = 0.7 (95%CI 0.4–0.9), p < 0.0003) (Figure 2(d)). Also, a significant negative correlation within hs-CRP and HOMA-%β was found (r=−0.4 (95%CI –0.7, –0.08), p < 0.044) (Figure 2(e)). Correlation of laboratory test correlation of (a) glycemia levels and TyG index*BMI, (b) hs-CRP levels and TyG index*BMI, (c) HOMA-IR and TyG index*BMI, (d) hs-CRP and IL-6, (e) hs-CRP and HOMA-%β in Berberine group. TyG: Triglycerides and glucose, BMI: Body mass index, hs-RCP: The high-sensitivity C-reactive protein, LDL: Low-density lipoprotein.
Hematology, liver, and kidney functions at baseline and final visit.
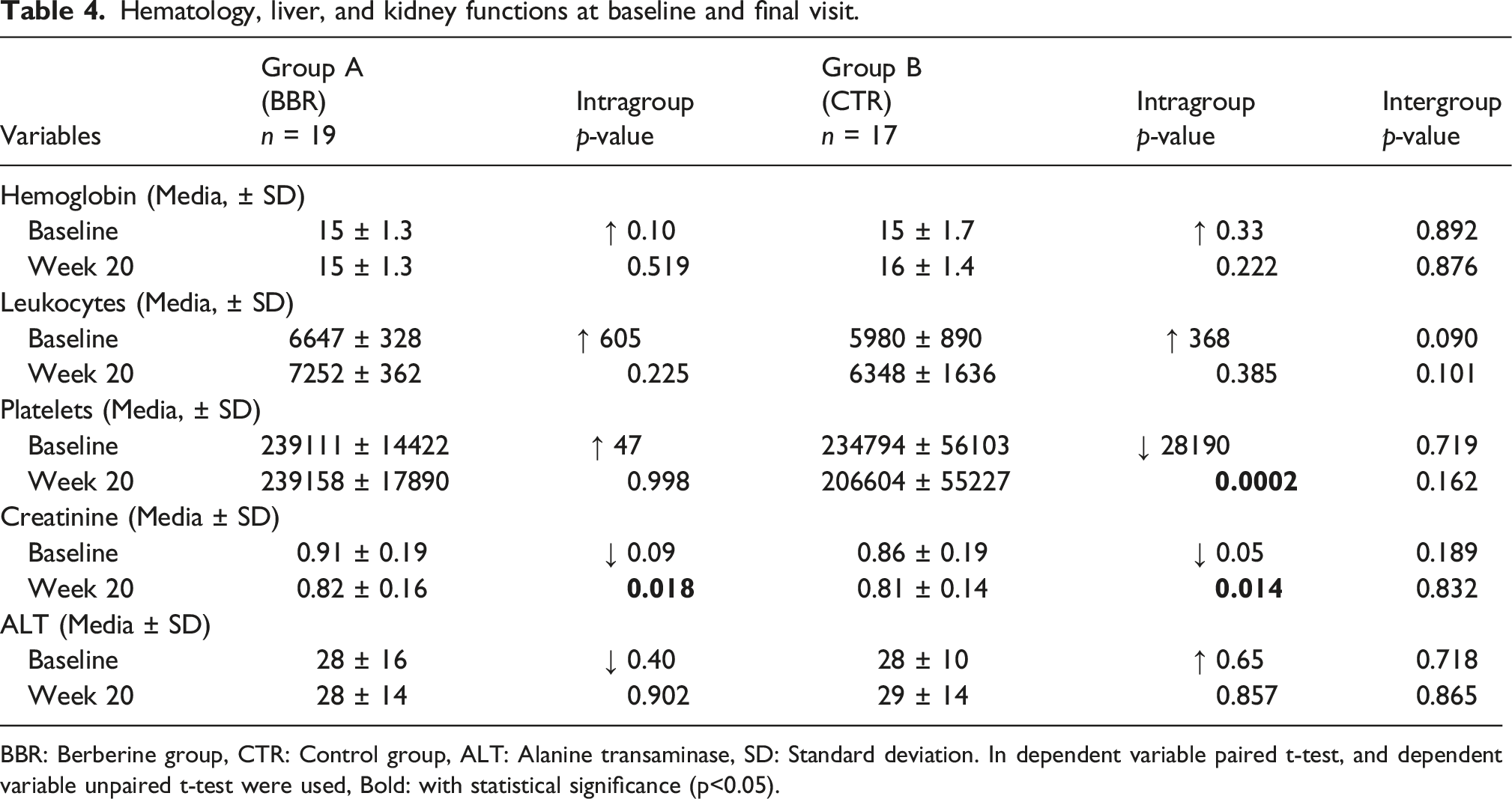
BBR: Berberine group, CTR: Control group, ALT: Alanine transaminase, SD: Standard deviation. In dependent variable paired t-test, and dependent variable unpaired t-test were used, Bold: with statistical significance (p<0.05).
Following the previous comparisons, we proceeded to evaluate the effect size of the significative results; we observed a Large effect in TNF-α (Δ: −0.5087719; CI: −0.114595, −0.7645359), Medium effect of the Triglycerides (Δ: −0.2631579; CI: 0.1241303, −0.5808671), Waist circumference/hip circumference ratio (Δ: −0.1468144; CI: 0.2294114, −0.4,848,721), Triglicerides-Body Mass Index (Δ: −0.1468144; CI:0.229743, −0.4851398), and Cardiovascular risk (Δ: 0.2354571; CI: 0.52185709, −0.09864852), however, the Weight was negligible (Δ: −0.1163435; CI: 0.2563809, −0.4589469) in the intragroup significances of BBR. In the CTR group, IL-6, we observe a medium (Δ: 0.449827; 0.72473987, 0.05136401) effect of the significance. On comparing the impact of the treatment at week 20 between BBR and CTR groups, the ratio Neutrophil-Linfocite (Δ: 0.5263158; CI: 0.7679683, 0.1534924) has a large effect, and the C-peptide presents a medium effect (Δ: 0.4117647; CI: 0.69349492, 0.02080806).
Lastly, the incidence of any adverse event was 10.5% in the BBR group and 5.8% in the CTR group. In the BBR group, the events included diarrhea (n = 1) and abdominal pain (n = 1); both events began at week 8 after starting the berberine capsules and were of a toxicity grade 1/mild; in CTR group, one participant had diarrhea, in the first week after starting the placebo, and also was of a toxicity grade 1/mild. None of the patients experienced severe adverse events, and none had to quit the protocol secondary to any adverse event in both groups.
Discussion
Life expectancy in PLWH has been increasing, with concurrent development of comorbidities. Current first-line regimens based principally on INSTIs and TAF have been associated with an increase in obesity, diabetes mellitus, arterial hypertension, and MetS;11,13 With the emergent identification of statin intolerance, a group of dietary supplements known as nutraceuticals was considered alternatives or adjuvants in lipid management due to their lipid-lowering, antioxidant, and anti-inflammatory properties. Berberine is one of the most studied.33,34 Since then, multiple trials and observational studies have been conducted with similar results. However, none of the earlier studies have recruited PLWH under ART and with virological suppression. To our knowledge, this is the first trial designed to evaluate the efficacy and safety of berberine in this population.
Multiple systematic reviews have consistently shown the therapeutic efficacy of berberine in non-HIV populations. Ye et al., evaluated 18 controlled trials, eight of which described randomization within their methodology and were placebo controlled. After assessing the risk of bias, notable improvements were observed, including a reduction in triglycerides, total cholesterol, c-LDL levels, as well as improvements in HOMA-IR and fasting plasma glucose levels. Although the therapeutic effect became apparent after a treatment duration exceeding 3 months, heterogeneity was noted in treatment dose and duration. 20
In our study, we found a relevant improvement in some components of MetS through weight and BMI reduction, insulin resistance amelioration (with a tendency to increase beta-cell function), and a better lipid and proinflammatory profile in the BBR group.
Validated indexes of insulin resistance were also evaluated, such as the HOMA-IR with its variant HOMA-%β and the TyG index*BMI. Since chronic inflammation drives glucose intolerance, proinflammatory cytokines were measured.7,35 Proinflammatory cytokine levels were higher in the intervention group, which may have attenuated the effect of berberine compared to placebo. However as can be seen in the delta value (Figure 3), decreased TNF-α levels in the intervention group and an increase in IL-6 in the placebo group were consistent with the previously proposed anti-inflammatory mechanisms of berberine.36,37 One possible explanation for the observed changes in the control group during the follow-up period is the natural progression of predisposing factors to metabolic syndrome. Persistent chronic inflammation, aging, and factors associated with antiretroviral therapy could contribute to these changes. We believe that with a longer follow-up period without intervention, the affected parameters will likely continue the same trend, although question is out of the scope of this trial. Non-parametric effect size of the significances of BBR intragroup (TyG: Triglycerides, Weight, CVR: CardioVascularRisk, WHR: Waist circumference/hip circumference ratio, TyG-BMI: Triglyceride Body Mass Index ratio, TNF-α: Tumor Necrosis Factor-α), CTR intragroup (IL-6: Interleukin 6), and BBR-CTR intergroup (C-peptide, Neu-Leu ratio: Neutrophil-to-lymphocyte ratio). Data are presented as Cliff´s delta with 95% of the confidence interval (error bars).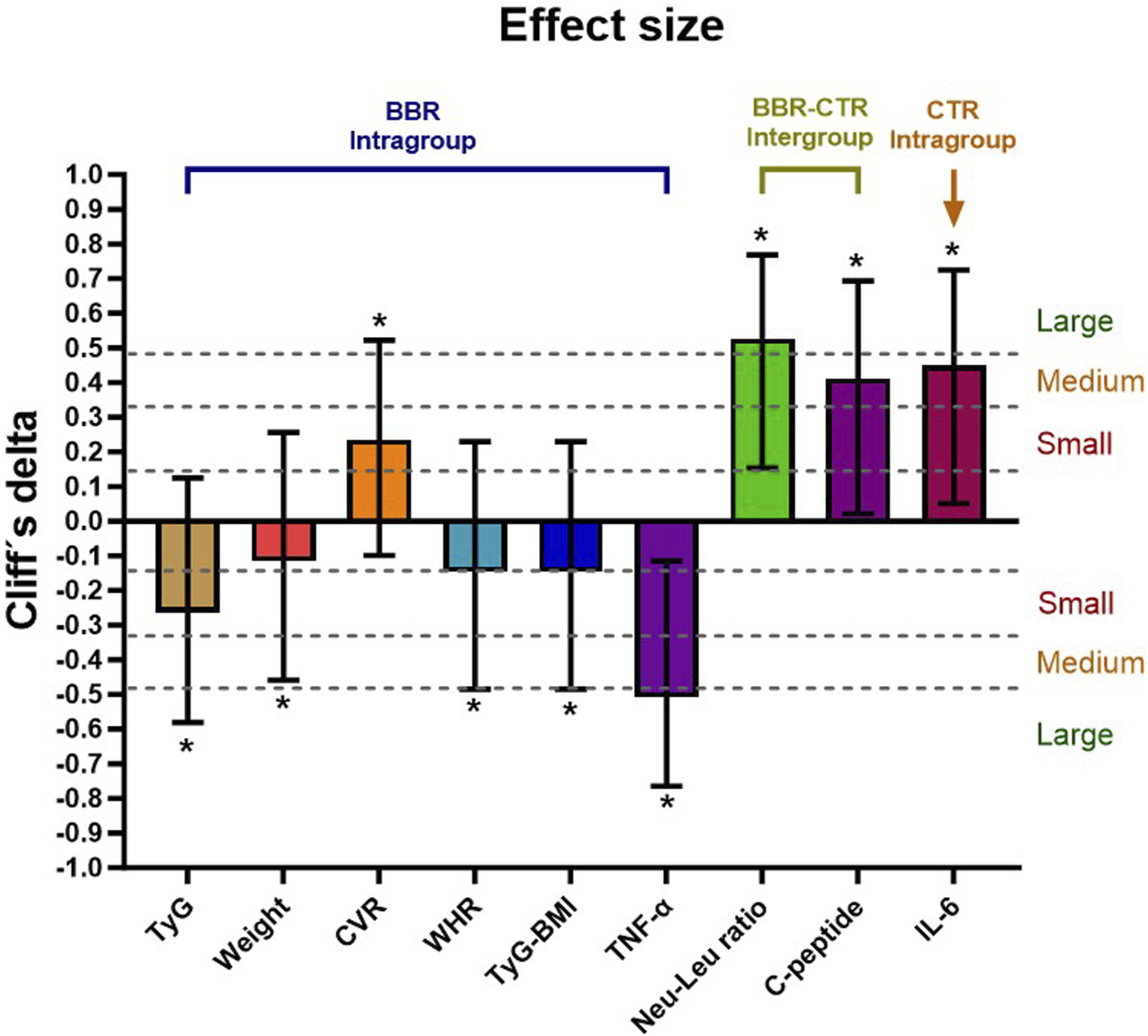
Relevant positive correlations in the BBR group were found, principally with the TyG index*BMI, glycemia, hs-CRP, and the HOMA-IR that could be useful in the clinic. It has been described that hs-CRP could be an excellent surrogate marker of IL-6 but more accessible and inexpensive to measure compared to IL-6.38,39 We found a significant positive correlation between the levels of hs-CRP and IL-6, corroborating these data. Additionally, the HOMA-%β was calculated to assess pancreatic beta–cell function, and we found a moderate negative correlation between this index and the hs-CRP in the BBR group. These findings suggest that high levels of hs-CRP could be associated with a less pancreatic beta–cell function and, thus, identify people at increased risk of developing diabetes. The CVR score increased significantly in both groups, and though these differences were not found to be statistically significant between groups, there was a marked tendency toward the benefit, especially with atherogenic lipids in the BBR group.
Regarding safety results, berberine was clinically safe and well tolerated; no serious adverse events occurred. Concisely, berberine could be considered a safe adjuvant therapy against metabolic syndrome in PLWH under virological suppression.
The limitations of our study are recognized. Our time of intervention was decided arbitrarily because of the availability of berberine, but the conditions of time >3 months and dose >1.2 g/day were met. All the participants were under Bictegravir/Tenofovir Alafenamide/Emtricitabine regimen, being the most related to weight gain. This may have attenuated the expected effects of berberine in some of the metabolic syndrome components but also added value to the ones that showed significant benefit. Although the number of participants who completed the study is higher than the initially calculated population, we acknowledge that the proportion of loss to follow-up is significant. The nutritional follow-up of patients was individualized, with each participant being assigned a personalized dietary regimen, considering the inherent limitations of this approach. There was no corresponding numerical record of intake percentages or exact quantification of consumed calories.
The nutritional follow-up of patients was individualized, with each participant being assigned a personalized dietary regimen, considering the inherent limitations of this approach. There was no corresponding numerical record of intake percentages or exact quantification of consumed calories.
Tendencies shown in our analysis may open the possibility of extending the time of follow-up in this population. The question of whether the positive outcomes persist or even get better the time remains to be answered.
Conclusions
In this pilot study we found that PLWH and MetS treated with berberine 500 mg TID for 20 weeks was safe and improved weight, BMI, triglycerides and proinflammatory cytokines. Although it is necessary to explore more studies that include more people and for longer intervention periods to support that berberine could be considered a safe adjuvant for the management of MetS in people living with HIV under virological suppression.
Footnotes
Acknowledgements
The authors want to thank the personnel and medical staff, especially research nurses María del Carmen Rivera and María del Carmen and María de Los Angeles González, who assisted in this project.
Author contributions
LAG-H, JFA-V, SAN-L, and VVR-H conceived the project and designed the experiments; VVR-H, AV-R, SAN-L, PM-A, MT-P, and JGT-A provided clinical evaluation and follow-up; MA-Z and KS-R performed cytokine determination and data analysis. LAG-H, VVR-H, SAN-L, and ASM-C created figures and tables, plus manuscript writing. LAG-H, JFA-V, ASM-C, and VVR-H reviewed and edited the manuscript. All authors reviewed critically and approved the definitive version of the manuscript to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This was partially supported by the “Programa de Impulso a la Investigación (PIN l-2020), Protocol No. 20-43”.
Ethics approval and consent to participate
This study was conducted at the University Hospital “Fray Antonio Alcalde” HIV Unit in collaboration with the HIV and Immunodeficiencies Research Institute (InIVIH) of the University of Guadalajara. The approval was obtained from the Ethics Committee from the University of Guadalajara (approval number: CI-06120). The study procedures were fulfilled and performed according to the Helsinki; all patients gave written informed consent before their enrollment. Moreover, the study was registered on ClinicalTrials.gov Identifier: NCT04860063.
Data Availability Statement
The experimental data and laboratory results that support the findings of this study are available in Figshare with the identifier, DOI: ![]() .
.