
Abstract
Background
This case report describes the successful use of imiquimod to treat genital herpes in an immunocompetent individual with acyclovir-resistant HSV.
Case report
A 32 year old male patient, presented with asymptomatic non-healing ulcers over the genital region for 2 years. The ulcers initially responded to acyclovir but became persistent after a few months. He also received multiple courses of antibiotics. On examination, the patient had bilateral inguinal lymphadenopathy and multiple painless ulcers over the coronal sulcus. Routine investigations were normal. The patient was treated with oral and intravenous acyclovir but showed no response. He was then started on topical imiquimod cream applied on alternate days. After one week, the patient presented with pain, redness, burning sensation, and fresh ulcer over the glans which were suspected to be imiquimod-induced irritant reaction or ulcer. Imiquimod was withheld for one week and then restarted at a twice-weekly schedule. After 1 month and 7 days of treatment with imiquimod at a twice-weekly schedule, there was healing of the ulcers.
Conclusion
This case report illustrates the efficacy of imiquimod cream as a topical treatment for genital herpes simplex in an immunocompetent patient who had previously been unresponsive to treatment with acyclovir.
Introduction
Herpes simplex virus (HSV) is a widespread infection that can cause symptoms ranging from mild skin lesions to severe neurological issues. There are two types of HSV: HSV-1, which mainly causes oral herpes, and HSV-2, which mainly causes genital herpes. 1 Oral acyclovir is the standard treatment for HSV infection, but acyclovir-resistant HSV is becoming more common. The prevalence of acyclovir-resistant HSV (ACV-R HSV) varies among populations but is generally higher in immunocompromised individuals such as those with HIV (4.2% prevalence).2–4 This case report describes the successful use of imiquimod to treat herpes genitalis in an immunocompetent individual unresponsive to acyclovir.
Case presentation
A 32-year-old heterosexual male presented with asymptomatic non-healing ulcers over the genital region for the preceding two years. The patient had developed vesicles which progressed to asymptomatic ulcers over the penis. There was clinical evidence of first response, followed by no response, with acyclovir. There was a history of multiple sexual partners.
On examination, the patient had bilateral inguinal lymphadenopathy with freely mobile, non-tender, firm lymph nodes. Local examination revealed depigmentation over the glans and coronal sulcus with multiple painless ulcers and yellowish slough present over the coronal sulcus (Figure 1(a)). Investigations like complete blood count, peripheral smear, liver function tests, complete urine analysis were within normal limits. Pus culture and Gram stain was suggestive of Staphylococcus aureus. The patient tested non reactive for HIV Tridot Elisa test, Hepatitis B, Hepatitis C, VDRL and TPHA. There was no history of any infectious disease complications. (a) Depigmentation over the glans and coronal sulcus with multiple painless ulcers and yellowish slough present over the coronal sulcus. (b) Healing of Ulcers post treatment.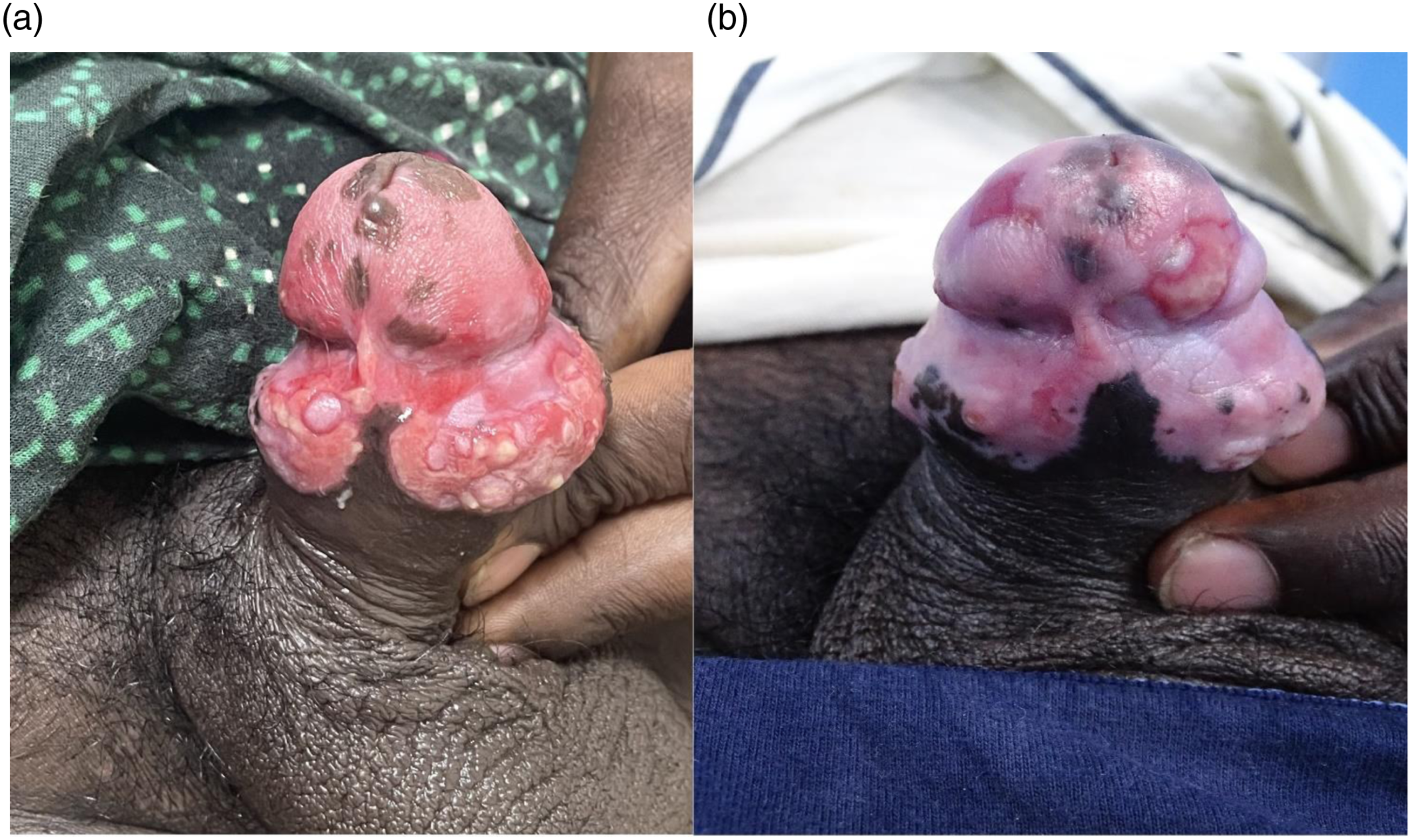
Tzanck smear revealed multinucleated giant cells (Figure 2). On histopathological examination, only inflammatory cells were seen. The patient was treated with oral acyclovir (800 mg) five times daily for 4 days but showed no response. He was then given intravenous acyclovir (400 mg) three times daily for 7 days along with doxycycline (100 mg) twice daily for 7 days to treat Staphylococcus aureus infection but again showed no response. Tzanck smear with multinucleated giant cells (depicted by arrow mark) and neutrophils.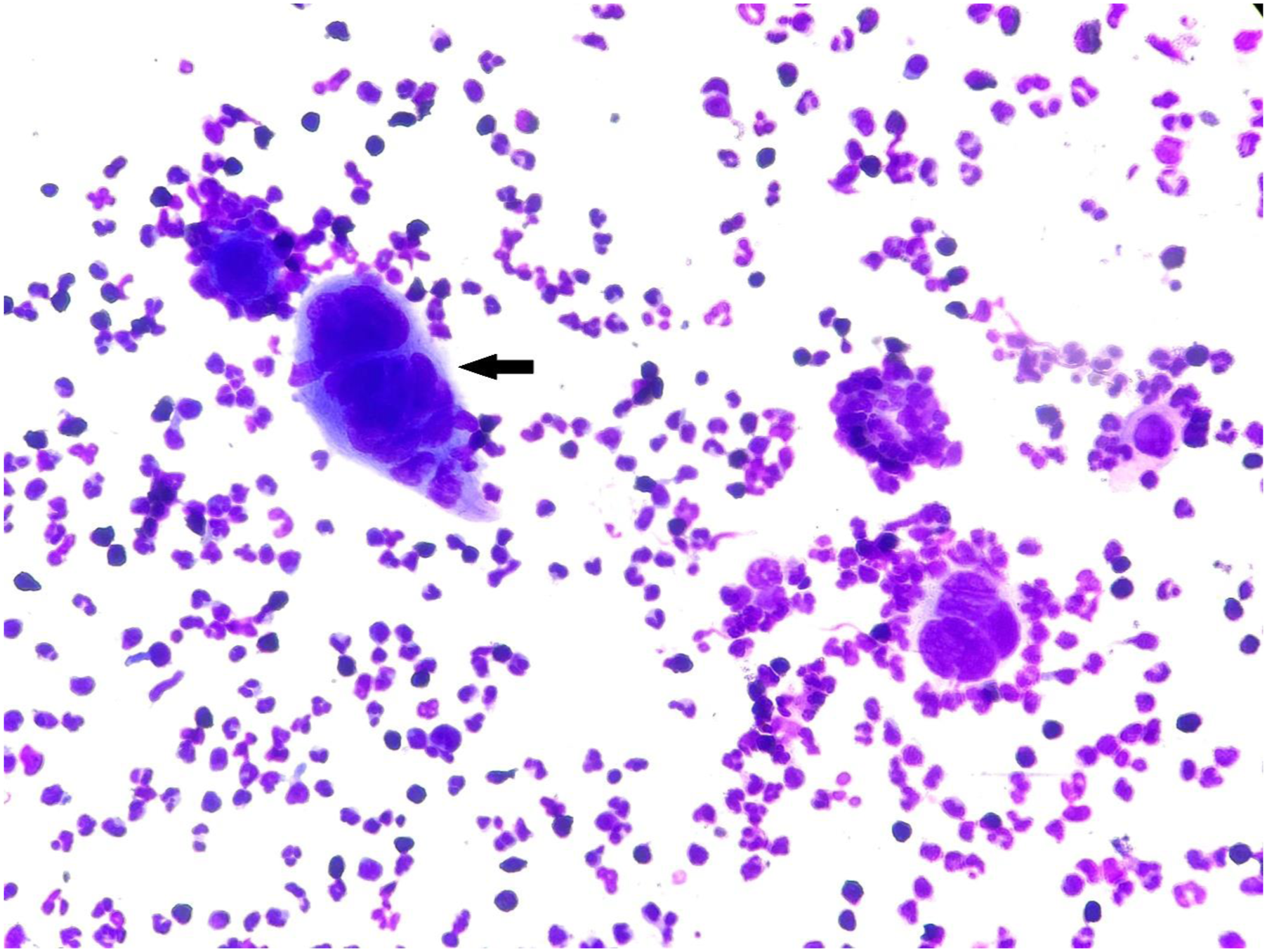
The patient was then started on topical imiquimod cream applied on alternate days. There was a mild reduction in discharge on days when imiquimod was applied. The patient applied imiquimod daily for a faster response. After 1 week, the patient presented with pain, redness, a burning sensation, and a fresh ulcer over the glans which were suspected to be imiquimod-induced irritant reaction or ulcer. Imiquimod was withheld for 1 week and then restarted at a twice-weekly schedule. After 1 month and 7 days of treatment with imiquimod at a twice-weekly schedule, there was healing of the ulcers (Figure 1(b)). There was no follow up beyond 1 month 7 days.
Discussion
There are case reports which had similar long history of ulceration. In their respective case reports, Susan M. Swetter and F. Mouly documented chronic, recurrent vulval erosions and of genital herpes in immunocompetent females over extended periods.5,6 Genotypic testing of viral resistance for acyclovir is not available in our country. There was clinical evidence of first response followed by no response with acyclovir. He failed ACV based treatment because strains of HSV may have acquired resistance by either eliminating thymidine kinase or decreasing thymidine kinase activity or altering DNA polymerase. Altered DNA polymerase mutants have been identified in clinical isolates of HSV recovered from immunocompromised patients but are rare. 5 There can also be mixtures of strains with different levels of thymidine kinase and susceptibility to ACV. 6 This case report illustrates the efficacy of imiquimod cream as a topical treatment for genital herpes simplex in an immunocompetent patient who had previously been unresponsive to multiple courses of antibiotics and antiviral therapy. While foscarnet and cidofovir are typically effective in treating acyclovir-resistant HSV infections, they are usually administered parenterally and have a risk of nephrotoxicity.2,7,8 Topical antiviral agents such as trifluridine have been evaluated for antiviral drug resistance but have only partial activity. 2 Imiquimod is an immune response modifier that stimulates cytokine production, including interferon-alpha, enhancing cell-mediated immunity against viral infections.9,10 Imiquimod has proven to be a non-toxic, well-tolerated, and successful therapy for atypical forms of genital herpes. Perkins et al., Tandon et al., and Bangsgaard et al. successfully treated genital herpes in immunocompromised individuals, a person living with HIV with recalcitrant hypertrophic herpes genitalis, and a 79-year-old woman with chronic lymphocytic leukemia respectively, using topical imiquimod and antiviral therapy, with no adverse effects.10–12
Conclusion
This case report underscores the potential of imiquimod as an alternative treatment for persistent anogenital herpes simplex virus infections, even in immunocompetent individuals. Imiquimod is a nontoxic, affordable, topical treatment option that can be easily available to treat ACV-R HSV. There is limited literature available on the application of imiquimod for herpes simplex infections in immunocompetent individuals.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.