
Abstract
Introduction
We assessed trends in HIV and syphilis prevalence, HIV incidence, related risk factors, and preventive behaviors among men who have sex with men (MSM) in Vietnam from 2015 to 2020.
Methods
Data originated from the HIV Sentinel Surveillance Plus system, which sampled MSM at venues and hotspots in seven of Vietnam’s 63 provinces in 2015, 2016, 2018, and 2020 (N = 1100-1445 per year; ∼150-300 per province per year).
Results
HIV prevalence estimates increased from 6.6% (95% CI 4.5–9.6) in 2015 to 13.8% (95% CI 10.5-18.2, p = .001 for trend) in 2020 overall, and separately in An Giang, Can Tho, Hai Phong, and Khanh Hoa provinces but not in Ho Chi Minh City, Hanoi, or Kien Giang. Syphilis prevalence increased from 2.7% (95% CI 1.4-5.1) in 2015 to 12.6% (95% CI 8.7-18.0) in 2020 overall (p < .001 for trend), and separately in An Giang, Can Tho, and Hai Phong provinces but not in Ho Chi Minh City or Kien Giang. We calculated time-at-risk from first anal sex to first HIV-positive or last HIV-negative test to estimate HIV incidence. Estimated HIV incidence suggested increasing rates of seroconversion from 1.36 per 100 person-years experienced by participants in 2015 to 2.61 per 100 person-years among participants in 2020 (hazard ratio per year 1.13, 95% CI 1.08-1.18, p < .001). There was a statistically significant increase in HIV testing, STI testing, and receipt of free condoms over the period (p < .05 for trend), and a statistically significant decrease in amphetamine use (p = .043 for trend).
Conclusions
Despite prevention efforts and improvements in some risk indicators, consecutive cross-sectional sampling results provide evidence of increasing incidence of HIV and syphilis among MSM in Vietnam, especially outside the major cities. Aggressive HIV prevention and treatment services can be expanded while conducting deeper investigations into the causes of these increases.
Keywords
Background
For most populations around the world, progress toward control of the human immunodeficiency virus (HIV) epidemic has been made. 1 Many countries around the world, including Vietnam, have set the goal of ending new HIV transmissions by 2030. 2 A key component of ending HIV transmission is achieving the “95-95-95” targets: that 95% of people living with HIV have been diagnosed, 95% of people diagnosed with HIV are on antiretroviral therapy (ART), and 95% of those on ART have achieved sustained viral suppression. Nonetheless, HIV transmission continues and, in 2021, an estimated one to two million people were newly infected with HIV in the world. 1
Transmission continues particularly in populations who have borne the heaviest burden of HIV. HIV prevalence and incidence may still be rising or resurging for some key populations.3,4 Key populations around the world include prisoners, men who have sex with men (MSM), sex workers of all genders (SW), people who inject drugs (PWID), and transgender people. In 2021, these populations and their partners were estimated to account for 70% of new HIV infections globally.1,5 In Asia and the Pacific region, 30% of all new HIV infections in 2018 occurred among MSM, particularly in urban areas. For example, in Bangkok in Thailand, Yangon in Myanmar, and Yogyakarta in Indonesia, recent estimated HIV prevalence among MSM has ranged from 20% to 29%.6,7
The HIV epidemic in Vietnam appears to follow a similar pattern to other Asian countries. Since the first cases of HIV infection were reported in Vietnam in 1990, 8 HIV prevalence data suggest that the epidemic is slowing 9 from 0.4% in 2010 to 0.3% in 2021. 10 In 2021, it is estimated that approximately 240,000 (230,000-270,000) people were living with HIV, of whom more than 180,000 were on ART. 11 Vietnam observed an encouraging 65% reduction of estimated new HIV infections between 2010 and 2018. 10 HIV prevalence in remains concentrated among PWID (12.7%), MSM (13.4%), and female SW (3.1%), with low prevalence among the general population (0.23%).10,12,13 Fortunately, HIV prevalence and estimated incidence rates among PWID and FSW have been decreasing over time. 13 For MSM, unfortunately, HIV transmission may not be decreasing in line with the general population or other key populations in Vietnam. Data from three southern provinces (An Giang, Can Tho and Ho Chi Minh city [HCMC]) suggest increases in HIV prevalence among MSM from 8.1% in 2014 to 16.0% in 2018 (p for trend <0.001). 14 Additionally, the HIV case reporting system has shown that the proportion of MSM among newly reported cases has increased recently, particularly in the Mekong River Delta and South East regions. 15 A population size estimation study reported that there are a total of 178,000 (95% CI 122,000-512,000) MSM, accounting for 0.68% (95% CI 0.46-1.95) of the male population aged 15-49 years in Vietnam. 16 However, this estimate may be conservative because the method included only men between the ages of 15 and 49 years and those who accessed the Internet and/or used social network apps. According to the most updated guidelines (UNAIDS and WHO, 2020), country-wide MSM size estimates below 1% of the adult male population should be considered underestimates. 17
In Vietnam, the HIV epidemic among key populations is systematically tracked through three major strategic information activities: HIV sentinel surveillance (HSS), sexually transmitted infection (STI) sentinel surveillance, and the third component measuring risk and preventive behaviors. The HIV Sentinel Surveillance Plus (HSS+) integrates biological and behavioral measures and serves as part of the monitoring and evaluation component of the National Targeted HIV/AIDS Program. This article reports HIV and syphilis prevalence and estimated HIV incidence among MSM in Vietnam and associated factors from the HSS+ 2015 – 2020 data. Such information is needed to detect changes in epidemic patterns by person, place, and time and to inform HIV/STI control and prevention efforts specifically for MSM in Vietnam.
Methods
Overview and setting
Data originate from the HSS+ using a community-based cluster sampling design among MSM. Nine sentinel provinces were purposively chosen from Vietnam’s 63 provinces to include the three major regions (North, Central, and South) and a diversity of urban and rural geographic areas. Within the selected provinces, sentinel districts are chosen based on having known venues or “hotspots” where MSM congregate. Within sentinel districts, a sampling frame was built and updated every year by collecting data on where MSM meet in each of the venues or hotspots, such as swimming pools, saunas, parks, movie theatres, and coffee shops. Clusters of venues/hotspots were then randomly selected from the sampling frame to recruit eligible participants. For this article, we analyzed data from the HSS+ surveys among MSM in seven of the nine sentinel provinces that had consistent data collection from 2015 to 2020. Up to 2016, HSS+ data were collected annually; after 2016, HSS+ data were collected every 2 years. As such, we used available data collected from 2015, 2016, 2018, and 2020. HSS+ was conducted in the capital city (Hanoi) located in the north (Red River Delta region), and the largest city (HCMC) located in the Southeast region. The five other provinces were Hai Phong (North Coast, Red River Delta), Khanh Hoa (South Central Coast), and An Giang, Can Tho, and Kien Giang in the Mekong Delta (South). HSS+ data were not collected for Kien Giang in 2016. Syphilis data were not collected in Hanoi and Khanh Hoa.
Study population
MSM was defined as men assigned male sex at birth and currently identified as men, aged 16 years and older, who self-reported having anal sex with another man at least once in the last 12 months, and currently living or working in the HSS+ province during the data collection year.
Sampling design
For each HSS+ survey year, a multi-stage sampling approach was implemented with the targeted number varying between 150 and 300 per province, depending on estimated MSM population sizes and available local resources. Within the selected provinces, three to five districts were purposively selected based on HIV burden, estimated MSM population size and local staff expertise to conduct surveys. Within the selected districts, a sampling frame was built and updated every year by mapping venues where MSM congregate and estimating the number of MSM affiliated with each location. The mapping and size estimation exercises were performed in a formative phase that included key informant interviews, focus group discussions, and field observations with community guides. The number of venues to be selected in each district was calculated by taking the required sample size for that district divided by the average number of MSM in each venue. Venues were then selected randomly from the sampling frame. In the first selected venue, all eligible participants who are found during the survey dates were approached, assessed for eligibility, and if eligible were invited to participate. Recruitment continued sequentially in the next venues until the planned sample size was achieved.
Measurements
A structured, face-to-face questionnaire was administered in private areas in the community, such as near the venues or at district health offices if preferred. The questionnaire included demographic characteristics, history of drug use, sexual behaviors, and use of services including HIV and STI testing, and prevention, care, and treatment.
Specimens of 3 mL (ml) of blood were drawn for serological testing for HIV and syphilis. HIV testing was conducted using an algorithm of three consecutive reactive tests to make an HIV-positive diagnosis as recommended by WHO and required by national guidelines. HIV tests approved by the Ministry of Health included ELISA (SD Bioline HIV-1/2 3.0, Standard Diagnostics Inc., Gyeonggi-do, Korea; or Murex HIV Ag/Ab Combination, DiaSorin, Dartford, United Kingdom) and rapid tests (SD Bioline HIV-1/2, Standard Diagnostics Inc, Gyeonggi-do, Korea; Vikia HIV-1/2, BioMerieux Shanghai Biotech Co., Shanghai, China; Determine HIV-1/2, Alere Medical Co., Matsudo, Japan; Alere HIV Combo, or Alere Medical Co., Matsudo, Japan; or Abon HIV-1/2, ABON Biopharm, Hangzhou Co., Hangzhou, China). Syphilis screening was done using rapid plasma reagin (RPR Latex test kit, Diagnostic Automation, Inc., CA, USA carbon kit; or Anamol Laboratories Pvt. Ltd, Maharashtra, India) with positive specimens confirmed by Treponema pallidum hemagglutination assay (TPHA Syphilis Latex, Veda. Lab, Alençon, France). Reactivity on both tests classified the participant as having active syphilis. HIV and syphilis tests were performed and confirmed by the Provincial Centers for Disease Prevention and Control laboratories in each province. Data collected from HSS+ are anonymous. No personal identifiable information was collected. Data collection, administrative forms and laboratory specimens were identified and linked according to code numbers to maintain participant confidentiality.
Statistical methods
The distribution of key variables in the samples are shown as medians or proportions for each survey year, including demographic characteristics, indicators of risk, preventive behaviors and HIV and syphilis positivity. Estimates are shown for non-missing responses; missing data were minimal across variables and years. Point estimates and 95% confidence intervals (CI) were calculated using districts as the primary sampling unit (i.e., cluster). Data are not weighted for probability of inclusion as the number of MSM per hotspot per district are not known. Temporal trends in HIV and syphilis prevalence from 2015 to 2020 were assessed overall and within demographic and risk categories using linear regression analysis, using seropositivity as the dependent variable, survey year as the independent variable, and districts as clusters.
We estimated HIV incidence using the method suggested by Osmond et al. 18 In this method, HIV-positive cases identified in each survey round were considered potential seroconversions. The person-time at risk was approximated as the time from first anal sex with a man to the date of the interview for HIV-negative cases. For HIV-positive cases, the time at risk was estimated as halfway between age at first anal sex and the survey test result or the first reported HIV-positive to account for interval censoring (i.e., unknown time from the age at risk to the time of seroconversion). HIV incidence rates were calculated per 100 person-years using the Kaplan-Meier method. 19 We report the incidence rate among MSM by enrollment year; that is, the rate refers to the incidence experienced by the participants enrolled in that year over the period at risk up to that year. To assess the temporal trend in the HIV incidence rates, we used Cox proportional hazard analysis with year of enrollment as the independent variable and report the associated hazard ratio per year assuming proportional hazards. Analyses were performed in STATA version 17.
Ethical considerations
The HSS+ protocol was reviewed and approved by the Internal Review Board of the National Institute for Hygiene and Epidemiology (number IRB-VN01059-07). This project was reviewed in accordance with the US Centers for Disease Control and Prevention (CDC) human research protection procedures and was determined to be research, but CDC investigators did not interact with human subjects or have access to identifiable data or specimens for research purposes. All participants provided verbal informed consent. Minors provided informed consent as permitted for the provision of sexual and reproductive health services in Vietnam. Participants confirmed to be HIV or syphilis positive were referred for treatment, care, and supportive services at the local facilities.
Results
Demographic and HIV risk-related characteristics, men who have sex with men (MSM) participating in HIV sentinel surveillance, seven provinces of Vietnam, 2015-2020 (n = 5106).

aCategories do not always add up to total due to missing data.
bLinear regression analysis.
Trends in HIV prevalence among men who have sex with men (MSM) participating in HIV sentinel surveillance, seven provinces of Vietnam, 2015-2020 (n = 5106).
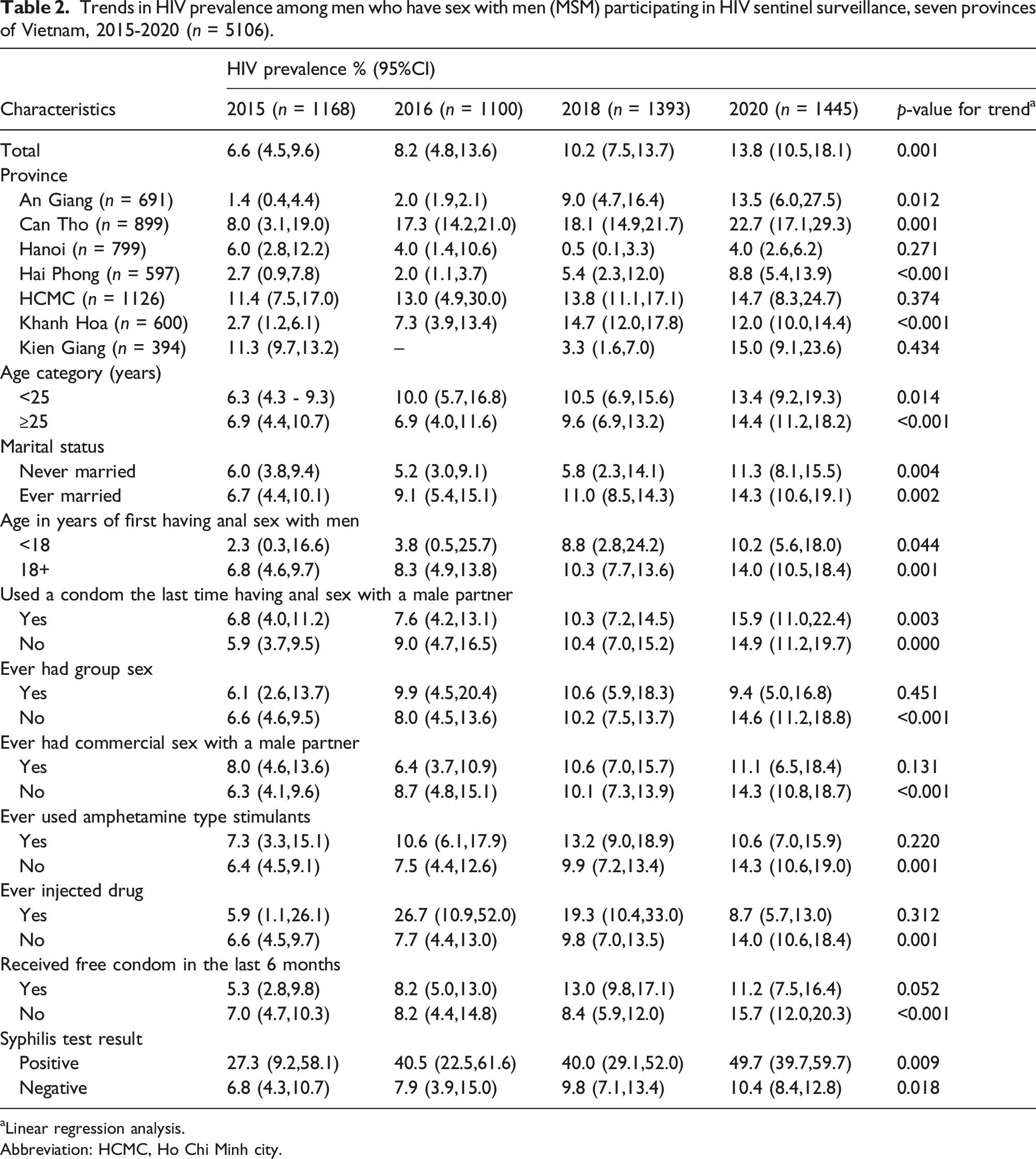
aLinear regression analysis.
Abbreviation: HCMC, Ho Chi Minh city.
Trends in syphilis prevalence among men who have sex with men participating in HIV sentinel surveillance, five provinces of Vietnam, 2015-2020 (n = 3707).

Linear regression analysis.
Abbreviation: HCMC, Ho Chi Minh city.
Figure 1 shows estimated HIV incidence based on the age of onset of male-male sexual behavior and reported first HIV-positive test. The annual increase from 2015 to 2020 was statistically significant in Cox proportional hazards analysis (hazard ratio for linear trend 1.13 per year (95% CI 1.08-1.18, p < .001). Estimated HIV incidence among men who have sex with men participating in HIV Sentinel Surveillance by enrollment year, seven provinces, Vietnam, 2015-2020 (n = 5106).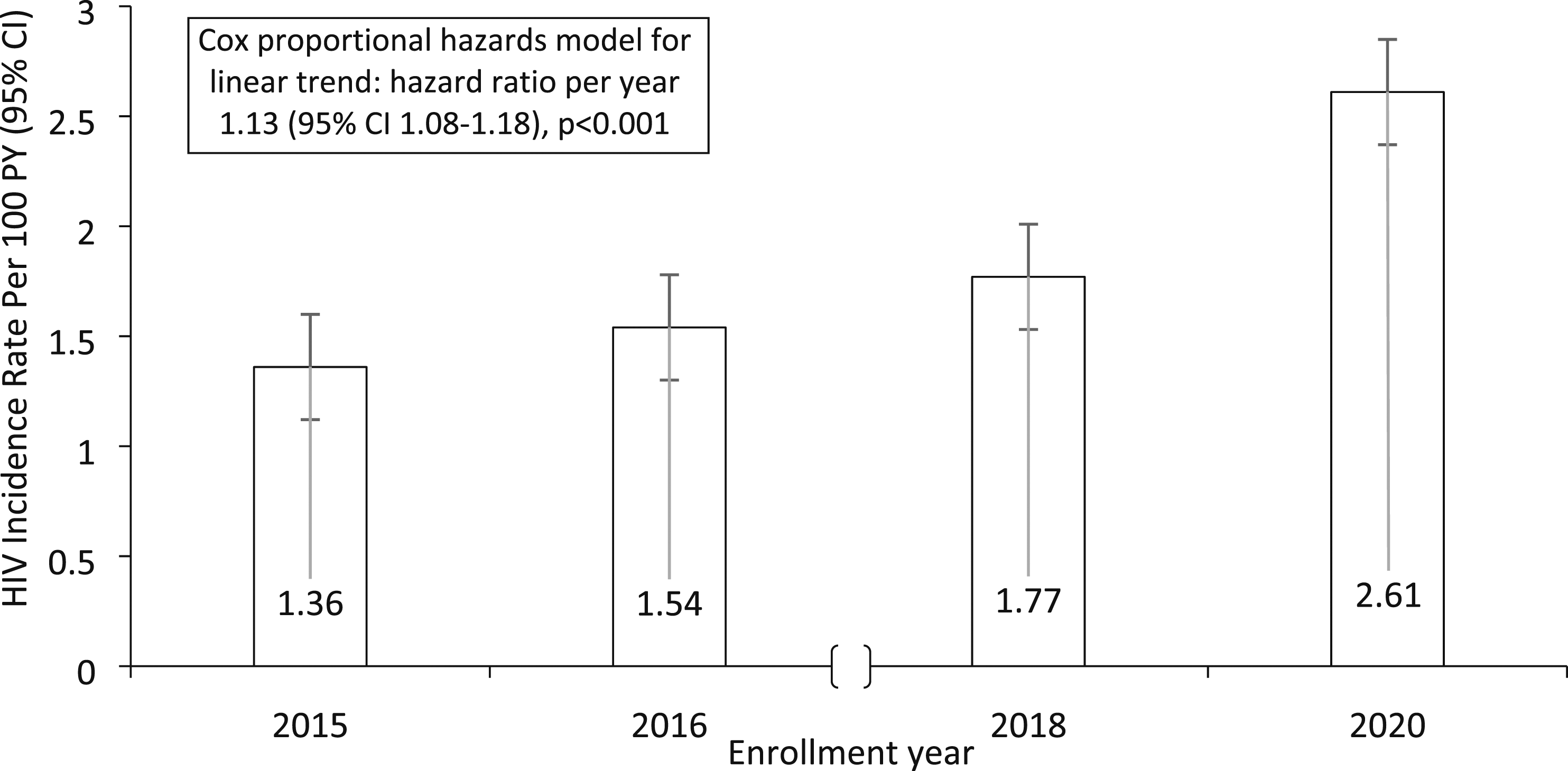
Discussion
Our data provide evidence that HIV prevalence increased from 2015 to 2020 among MSM in Vietnam. These sentinel surveillance data tracked a more than two-fold increase in HIV prevalence, from 6.6% in 2015 to 13.8% in 2020, in seven provinces across the country. The rise in HIV prevalence was observed across younger and older age groups, married and unmarried MSM, and the increase was statistically significant in four of the seven sentinel provinces. Our data add to the previous report on HIV prevalence among MSM increasing in three southern provinces (An Giang, Can Tho, and HCMC) from 2014 to 2018. 14 By 2020, the increases continued in An Giang and Can Tho and now also in Kien Giang in Mekong Delta, Hai Phong in the North Coast, and Khanh Hoa in the South Central Coast. Notably, the increased trends were statistically significant in four of the five provinces outside the two largest cities of Hanoi and HCMC. Although there was no statistically significant increase in HIV prevalence among MSM in HCMC, prevalence remained high at 11.4% in 2015 and 14.7% in 2020. Hanoi and HCMC were the focus of early prevention and care programs tailored for MSM and our data may detect a benefit of these interventions in slowing HIV transmission. Meanwhile, HIV programs are starting to expand to other provinces, particularly in the Mekong River Delta. We hope that future surveillance data will show benefits in this region.
A rise in HIV transmission among MSM in Vietnam is corroborated by other evidence. First, the increase in HIV prevalence temporally coincides with an increase in syphilis prevalence, a well-documented marker for HIV risk.14,20 Second, the rise in HIV prevalence among MSM in Vietnam is similar to the increases witnessed among MSM in Asia and other regions of the world.21,22 Third, our new estimate of the rate of seroconversion based on reported years of sexual activity and first HIV-positive test results suggests transmission may be accelerating, also by a two-fold increase from an annual rate of 1.36 per 100 person-years experienced by participants in 2015 to 2.61 per 100 person-years among participants in 2020. A baseline cohort study among MSM in Vietnam reported that 36% of those testing HIV positive had recent infection using AsanteTM HIV-1 Rapid Recency® Assay with a duration of recent infection of 161 days. 23 Recency testing conducted in routine HIV testing services also confirms a large and growing risk among MSM. 13 These independent studies corroborate our current findings that HIV transmission among MSM persists and may be increasing despite programming to prevent HIV infections.
Unfortunately, the serial cross-sectional design and limited number of measures in sentinel surveillance data make it challenging to identify why HIV transmission is currently rising among MSM in Vietnam. Paradoxically, we note no substantial increases in key indicators of risk behaviors (e.g., condom use, group sex, commercial sex, drug use), and a decrease in the use of amphetamine-type stimulants – a risk factor previously shown to be related to HIV acquisition risk. 24 Meanwhile, preventive behaviors substantially increased (e.g., receiving condoms, STI testing, HIV testing). Further, confounding did not appear to account for the apparent trends in Cox proportional hazards analysis and findings were consistent across demographic characteristics. The increasing prevalence of both HIV and syphilis regardless of risk behaviors measured in this study is a cause for concern and underscores the need for a reevaluation of traditional interventions which alone may not be effectively reducing new infections. To address this issue, it is imperative to explore potential factors behind this increase, and identify new points for future HIV prevention interventions in Vietnam.
We hypothesize that increased HIV transmission could be driven by structural-level factors related to the social context for MSM in Vietnam, including stigma, discrimination, and changing patterns in sexual networks. 25 For example, sexual networks may have recently expanded with the use of online technologies to find partners and are not limited to local venues and hotspots. 26 A cohort study among MSM in Hanoi, Vietnam indicates that there is an association between meeting sex partners through social networking technology and STI transmission. 27 On an international level, Vietnam’s MSM communities may be recently more connected to MSM communities in other countries. 28 HIV-related stigma and discrimination, particularly among MSM create significant gaps and inequality in access HIV treatment and prevention efforts. 25 These phenomena may be evident in the earlier peaks in HIV prevalence in the two largest cities with continuing spread to secondary cities and provinces. More in-depth studies, particularly with qualitative network-level data and molecular HIV testing, will be needed to identify potential reasons for increasing high levels of transmission and the spread of HIV across geographic areas.
We recognize limitations of our data beyond the measures and cross-sectional design. First, the sampling design is based on estimated relative numbers of MSM present in the provinces and at hotspots and cannot be considered representative of all MSM in the area. Data needed to weight inputs to adjust estimates (e.g., the underlying denominators or MSM in the districts and frequency of hotspot attendance) to be representative are not available. Second, recruitment methods at hotspots entail potential selection and participation biases in which MSM visit such venues. Data on proportions among those approached who agreed to the eligibility screening, among those screened who were eligible, and among those eligible who consented to enroll were not available. Third, self-report can lead to respondent bias due to underreporting of sensitive behaviors and overreporting of socially desirable responses among surveyed participants. These biases are difficult to measure and adjust for. Fourth, this mobile population was treated as if it were a fixed population affiliated with specific hotspots in each district. Fifth, the collection of PrEP usage data among participants in the HSS+ only commenced in 2021, coinciding with the national scale-up of PrEP. Consequently, information regarding PrEP usage among MSM was unavailable for this study. Finally, the sentinel surveillance sites do not include all areas of Vietnam; however, the sentinel surveillance system is implemented in areas that include a large proportion of the population, the main regions of Vietnam, and both urban and rural provinces.
Limitations notwithstanding, sentinel surveillance can help guide public health responses to the HIV epidemic in key populations. While not necessarily representative, the sentinel surveillance approach emphasizes feasibility, diversity of locations, capturing early signals of changes in the epidemic, and consistency over time and place. We believe these qualities have led to the identification of a real trend toward increasing prevalence and incidence of HIV among MSM in Vietnam, including outside major cities. These signals prompt a deeper investigation of the causes for the increase and the most promising points of intervention. Meanwhile, multifaceted prevention interventions with proven efficacy can be scaled up in MSM-specific programs, particularly addressing stigma and coupling with social network-based approaches to promote and engage MSM in HIV/STI services, such as network testing, community linkage to treatment, 29 viral suppression among MSM living with HIV (i.e., “U = U”), 30 PrEP and PEP demand creation to keep HIV-negative MSM uninfected,31,32 and integrating syphilis testing in HIV, care, testing, and PrEP referrals. 13 Leveraging digital tools and innovative technologies such as online platforms, social media, dating apps, and messaging have proven to be effective interventions to prevent HIV and STI among MSM in the context of the evolving of sexual networks landscape.33,34 MSM-friendly HIV testing programs with rapid linkage to care, immediate ART initiation, and efforts to achieve high retention and adherence may be particularly effective through sustained viral suppression. 35 Policy changes and legal reform are crucial addition to public health efforts in combating HIV related stigma. They are essential for creating an inclusive and supportive environment that ensure equal access to healthcare services. 25 Vietnam has achieved notable success in its HIV response with the global scale-up of ART and overall decreases in new HIV infections for other populations. 15 Moreover, the country has adopted the Fast Track Cities’ “95-95-95” goals for diagnosis, ART, and viral suppression to end the epidemic by 2030. Achieving these targets for MSM may be the final challenge to ending the HIV epidemic in Vietnam overall.
Conclusions
HIV national sentinel surveillance provides evidence of increasing incidence of HIV and syphilis among MSM in Vietnam, especially outside the major cities. HIV national sentinel surveillance can help guide public health responses to the HIV epidemic in key populations. Meanwhile, HIV/STI prevention and treatment services can be expanded for MSM while conducting deeper investigations into the potential factors causing increases in HIV and syphilis.
Supplemental Material
Supplemental Material - Increase in human immunodeficiency virus and syphilis prevalence and incidence among men who have sex with men, vietnam 2015 – 2020
Supplemental Material for Increase in human immunodeficiency virus and syphilis prevalence and incidence among men who have sex with men, vietnam 2015 – 2020 by Ha Thi Thanh Nguyen, Ly Thuy Nguyen, Ha Thi Thanh Hoang, Duc Hoang Bui, Huong Thi Thu Phan, Nghia Van Khuu, Hanh Thi Hong Ngo, Duc Anh Dang, Ali Mirzazadeh, Willi McFarland and Thang Hong Pham in International Journal of STD & AIDS
Footnotes
Acknowledgments
We also wish to acknowledge the support from the University of California, San Francisco’s International Traineeships in AIDS Prevention Studies (ITAPS), U.S. NIMH, R25MH123256.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the President’s Emergency Plan for AIDS Relief (PEPFAR) through the U.S. Centers for Disease Control and Prevention (CDC) under the terms of GH001628, GH001989 and GH161718. The findings and conclusions in this paper are those of the authors and do not necessarily represent the official position of the funding agencies.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.