
Abstract
Background
Doravirine is a non-nucleoside reverse transcriptase inhibitor recommended for the treatment of virologically suppressed and treatment naïve people living with HIV. The DRIVE-REAL study aimed to describe the characteristics, treatment patterns, and virological outcomes of doravirine users in a real-world cohort in the UK.
Methods
A retrospective, observational, multi-centre chart review was conducted for 300 adults living with HIV initiating doravirine-containing antiretroviral therapy.
Results
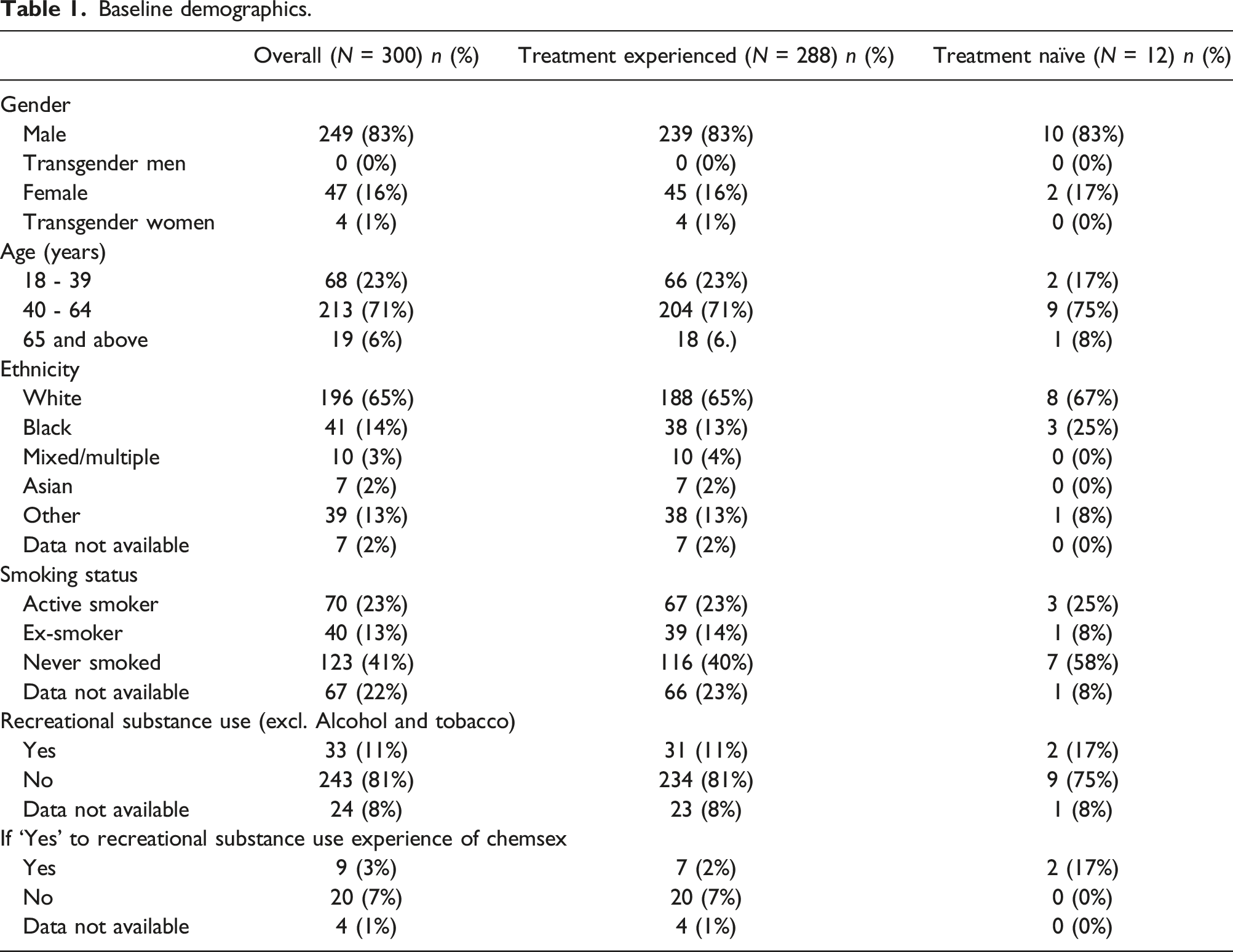
At baseline 83% of individuals were male, 45% aged ≥50 years, 65% white ethnicity. Median time since HIV diagnosis was 12 years. 96% were antiretroviral therapy-experienced, 87% had a HIV viral load <50 copies/ml, and 15% had resistance to at least one antiretroviral drug. 66% had comorbidities, most commonly depression (26%), and 70% were taking at least one co-medication. At six months, 94% (n = 283/300) were still receiving doravirine. Viral load data were available for n = 266/300 individuals and 95% (n = 253/266) had viral load <50 copies/ml.
Conclusions
Individuals initiating doravirine in this cohort are predominantly treatment-experienced white middle-aged males, with a high frequency of comorbidities and co-medication. The majority of individuals at 6 months remained on doravirine and maintained or achieved HIV viral suppression. This study provides epidemiologic characteristics that can inform clinical care and subsequent hypothesis-testing studies.
Introduction
The global roll-out and advancement of antiretroviral therapy (ART) for human immunodeficiency virus (HIV) over the last forty years has significantly reduced the global burden of HIV-related mortality and morbidity. Encouragingly in the UK, the UNAIDS 95-95-95 targets were met in 2020, with 95% of all people living with HIV diagnosed, 99% of those on treatment and 97% of those virally suppressed. 1 However, as the cohort of people living with HIV are ageing and new health needs continue to evolve, it is imperative that ART is optimised to meet these challenges, and that an array of effective, convenient and well-tolerated treatment options be made available.
Doravirine (DOR) is a once-daily non-nucleoside reverse transcriptase inhibitor (NNRTI) licensed for the treatment of HIV-1. DOR is available as a single entity and a fixed-dose combination (FDC) with lamivudine and tenofovir disoproxil fumarate (DOR/3TC/TDF). DOR was designed to address limitations of older NNRTIs, such as requirements to take with/without food, drug-drug interactions (DDIs) with commonly co-prescribed medications, and HIV-RNA viral load restrictions when initiating therapy.2–4 DOR has demonstrated virological suppression in high baseline HIV-RNA viral loads, where Phase 3 treatment naïve studies did not have a HIV-1 viral load restriction as part of the inclusion criteria, 2 and is effective against wild type viruses and most common NNRTI resistance-associated mutants, including K103N and Y181C.3,5,6 It has a low potential for DDIs 7 and can be taken with or without food. 8
Phase 3 clinical trials have demonstrated DOR-based regimens have a non-inferior efficacy compared with ritonavir boosted darunavir (DRV/r) and efavirenz (EFV)-based regimens in treatment naïve adults through 192 weeks. 2 A separate Phase 3 trial among treatment experienced adults switching from stable ART to DOR/3TC/TDF showed maintenance of virological suppression through 144 weeks. 9 DOR has demonstrated a favourable LDL and non-HDL lipid profile when compared to EFV and DRV/b.5,6 Additionally, DOR exhibits favourable neuropsychiatric tolerability, showing superiority over EFV in an analysis of dizziness, sleep disorders/disturbances, and altered sensorium. 5 DOR in combination with 3TC/TDF has demonstrated modest weight gain, similar to the average yearly weight change in adults without HIV-1. 10
DOR was granted European marketing authorisation in November 2018. 4 Current European treatment guidelines recommend DOR/3TC/TDF and DOR + FTC/TAF or XTC/TDF as initial regimens in ART-naïve people living with HIV and as a switch option in those who are virologically suppressed. 11 UK British HIV Association (BHIVA) guidelines recommend DOR/3TC/TDF or DOR + FTC/TDF or FTC/TAF as initial treatment in treatment naïve people living with HIV in certain clinical situations and as a switch in those who are virologically suppressed. 12
Large descriptive studies are needed to further our understanding of how DOR is being used in clinical practice and how clinical trial data on DOR has been translated into the real-world, as well as to provide the groundwork for hypothesis-testing studies. The Real World Utilisation of Doravirine among people living with HIV in England (DRIVE-REAL) study aimed to describe the characteristics, treatment patterns and virological outcomes among people living with HIV initiating DOR in a UK real-world setting.
Methods
This study was a non-interventional, observational, retrospective chart review study using electronic data capture. The study was approved by South Yorkshire Research Ethics Committee (reference: 21/YH/0062) in 2021. This study included both treatment experienced and treatment naïve people living with HIV who either switched to, or initiated DOR containing ART.
Primary objectives included a description of demographics, clinical and treatment characteristics at DOR initiation (baseline), reason for DOR initiation, prior ART regimen for treatment experienced individuals switching to DOR, and other antiretroviral agents combined with DOR. Secondary objectives included a description of laboratory parameters and ART resistance-associated mutations at baseline and virologic outcomes at six months. We stratified our findings by ART experience to provide further insights into the type of users of DOR in a real-world setting. Treatment experienced was defined as individuals already taking ART at the time of DOR initiation i.e., switching to DOR based therapy. Treatment naïve was defined as individuals starting ART for the treatment of HIV-1. This study was designed as a detailed descriptive study without formal hypothesis testing; therefore, statistical testing and modelling were out of the scope of the pre-defined study protocol. Differences between experienced and naïve individuals should not be interpreted as statistical differences nor the 6-months outcomes as causal effects.
Data were extracted, using an electronic case report form, from the clinic records of 300 individuals receiving DOR containing ART at three NHS HIV clinics, in London (n = 150 from Chelsea & Westminster Hospital, n = 80 from Mortimer Market Centre) and Brighton (n = 70 from University Hospitals Sussex), using sequential sampling to minimise bias. Inclusion criteria included adults living with HIV who initiated DOR-based ART from 1 July 2019 until 11 January 2021 who had at least one 6-months follow-up appointment. This time period was selected based on expectations of DOR utilisation over time in the post-launch period and standard UK practice of clinic appointments every six months.
Baseline mutations were defined and classified by the Stanford University HIV drug resistance database programme v.3.1.2 update 2021-03-21. 13 For this study, a major resistance-associated mutation was defined as any mutation listed in the Stanford University HIV drug resistance database described as causing low, intermediate or high-level resistance; minor mutations were defined as any mutation that appeared on the genotypic resistance test listed in the case report form but does not appear on the Stanford database.
Body Mass Index (BMI) was defined using the following criteria: below 18.5 is underweight; between 18.5 and 24.9 is healthy; between 25 and 29.9 is overweight; 30 or over is obese. Lipid abnormalities were defined biochemically using the following cut-offs: total cholesterol ≥5 mmol/L; low-density lipoprotein cholesterol (low < 2.25 mmol/L; high > 3.4 mmol/L); high-density lipoprotein (HDL) cholesterol ≤ 1.2 mmol/L; non-HDL cholesterol ≥ 4 mmol/L; triglycerides ≥ 1.7 mmol/L14,15. Hyperlipidaemia was included as part of a list of comorbidities and was reported based on stated comorbidities in the medical record. This question was independent of the measured lipid levels at the time of data collection.
Recreational substance use was defined as the consumption of one or more psychoactive drugs, this did not include the consumption of alcohol or cigarette smoking. Chemsex was defined as using certain substances immediately before or during sexual activities to facilitate, prolong and/or intensify sexual experience, mainly by some communities of men who have sex with men.
Results
Baseline demographics
Baseline demographics.
Baseline clinical characteristics
Baseline clinical characteristics.

Of those with body mass index (BMI) data available (n = 174, 58% of overall sample), over half (55%, n = 95) were living with overweight or obesity (BMI >25 kg/m2).
Baseline serum lipid data were collected for approximately 59% of individuals. For those with lipid data available and prior to DOR initiation, 44% had high total cholesterol (≥5 mmol/L), 29% had high low-density lipoprotein (LDL) (>3.4 mmol/L), and 38% had abnormal triglycerides (≥1.7 mmol/L). In general, treatment experienced individuals had higher levels of BMI as well as cholesterol and triglycerides profiles than naïve individuals (e.g., abnormal total cholesterol was 26% vs 17%).
Baseline comorbidities and comedication
Two-thirds (66%) had one or more comorbidities at DOR initiation, 67% treatment experienced and 42% treatment naïve. The most common comorbidities at the time of DOR initiation were depression (26%), documented hyperlipidaemia (19%), anxiety disorders (13%), hypertension (12%), acid reflux (6.7%), vitamin D deficiency (6%), cardiovascular disease (excluding hypertension) (6%) and diabetes mellitus (5%). The mean number of comorbidities experienced at baseline was 1.5.
Seventy percent of all individuals were taking co-medications alongside DOR containing ART, 70% (n = 201/288) treatment experienced and 75% (n = 9/12) treatment naïve. The most common co-medication were vitamins/herbal remedies (26%), psychotropic agents (including anti-depressants) (25%), lipid-lowering agents (16%), antihypertensives agents (15%), acid suppressants (proton pump inhibitors and H2 antagonists) (12%), anti-infective agents (9%) and non-steroidal anti-inflammatory agents (NSAIDS) (6%). Approximately a third (32%, n = 97) received 1 co-medication, and 13% (n = 40) received ≥4. The mean number of co-medications overall was 1.6. (Figure 1). Proportion of people living with HIV with co-morbidities (a) and co-medications (b) at baseline.
Doravirine formulation and antiretroviral therapy combination including prior antiretroviral therapy
ART formulation prior and at DOR initiation.

The most common ART combination received prior to switching to DOR was 2NRTI + NNRTI (38%), of whom 53% were on an efavirenz containing combination. This was followed by 2NRTI + INSTI (34%), 2NRTI + PI (18%). Ten individuals (3%) switched from dual therapy, majority PI + NRTI (n = 8/10). Two-thirds switched from an FTC/TDF backbone (66% n = 189/288), 15% (n = 42) from an ABC/3TC backbone and n = 34/288 (12%) from a FTC/TAF backbone.
Laboratory parameters and antiretroviral therapy resistance at baseline
Baseline laboratory parameters.
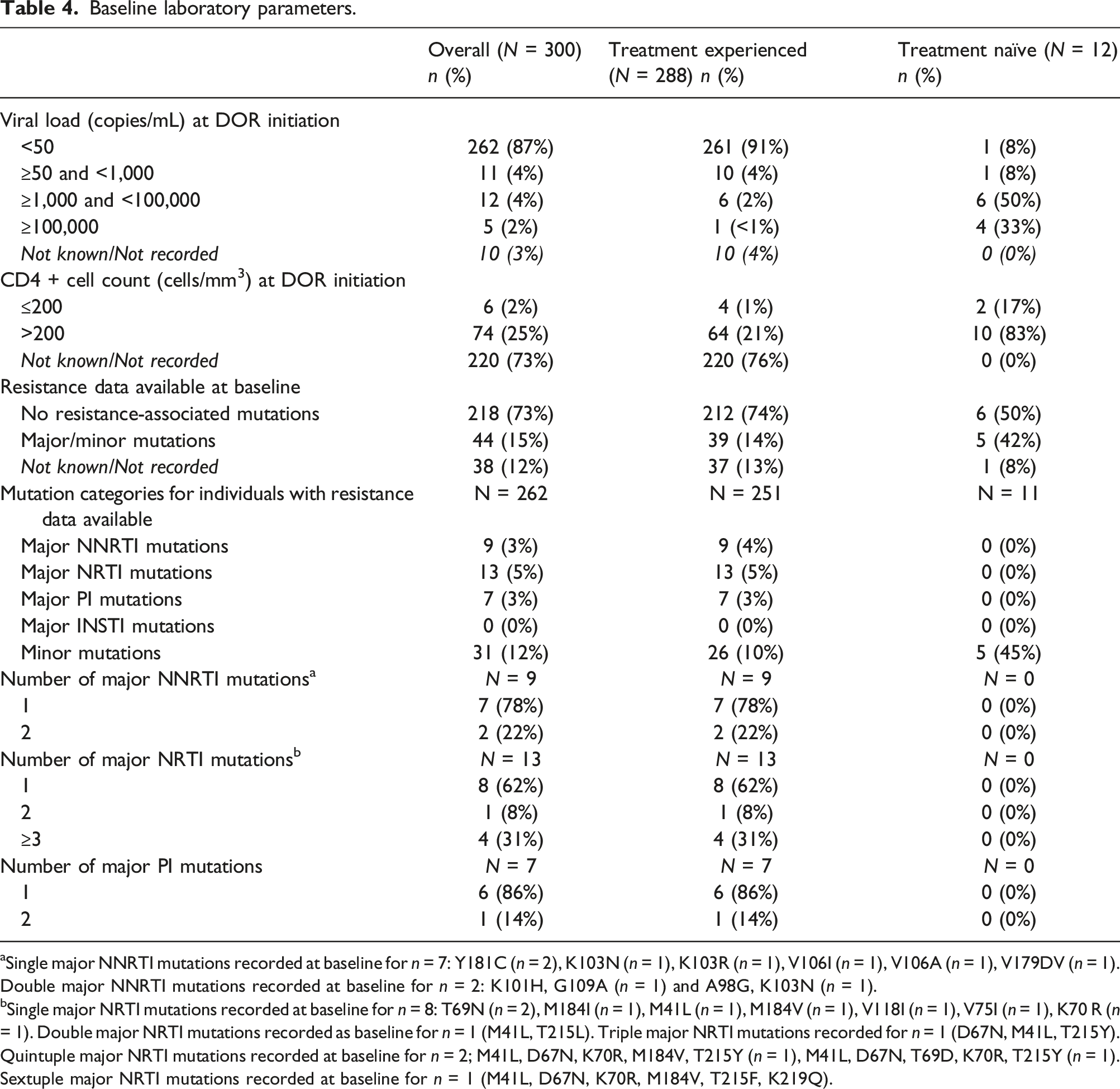
aSingle major NNRTI mutations recorded at baseline for n = 7: Y181C (n = 2), K103N (n = 1), K103R (n = 1), V106I (n = 1), V106A (n = 1), V179DV (n = 1). Double major NNRTI mutations recorded at baseline for n = 2: K101H, G109A (n = 1) and A98G, K103N (n = 1).
bSingle major NRTI mutations recorded at baseline for n = 8: T69N (n = 2), M184I (n = 1), M41L (n = 1), M184V (n = 1), V118I (n = 1), V75I (n = 1), K70 R (n = 1). Double major NRTI mutations recorded as baseline for n = 1 (M41L, T215L). Triple major NRTI mutations recorded for n = 1 (D67N, M41L, T215Y). Quintuple major NRTI mutations recorded at baseline for n = 2; M41L, D67N, K70R, M184V, T215Y (n = 1), M41L, D67N, T69D, K70R, T215Y (n = 1). Sextuple major NRTI mutations recorded at baseline for n = 1 (M41L, D67N, K70R, M184V, T215F, K219Q).
The majority of CD4 count data at baseline were incomplete, of those with available data (n = 80), median CD4 cell count was 573 cells/mm3 (IQR = 458.6). Of those with available data, 63% (n = 43/68) of treatment experienced individuals had a CD4 count >500 cells/mm3 and 6% (n = 4) with CD4 ≤200 cells/mm3. All treatment naïve individuals had CD4 count data available, of whom 17% (n = 2/12) had CD4 <200 cells/mm3.
Baseline resistance data was available for 87% (n = 262/300) of individuals (see Table 4). For individuals with resistance data, 17% (n = 44/262) had one or more recorded resistance-associated mutations. Among treatment experienced individuals 87% (n = 251/288) had resistance data available at baseline, of which 4% (n = 9/251) had major NNRTI mutations, 5% (n = 13/251) had major NRTI mutations, 0% major INSTI mutations and 3% (n = 7/251) major PI mutations. No treatment naïve individuals had major resistance associated mutations at baseline.
Laboratory parameters and clinical information at six months
Laboratory and clinical information at six months.
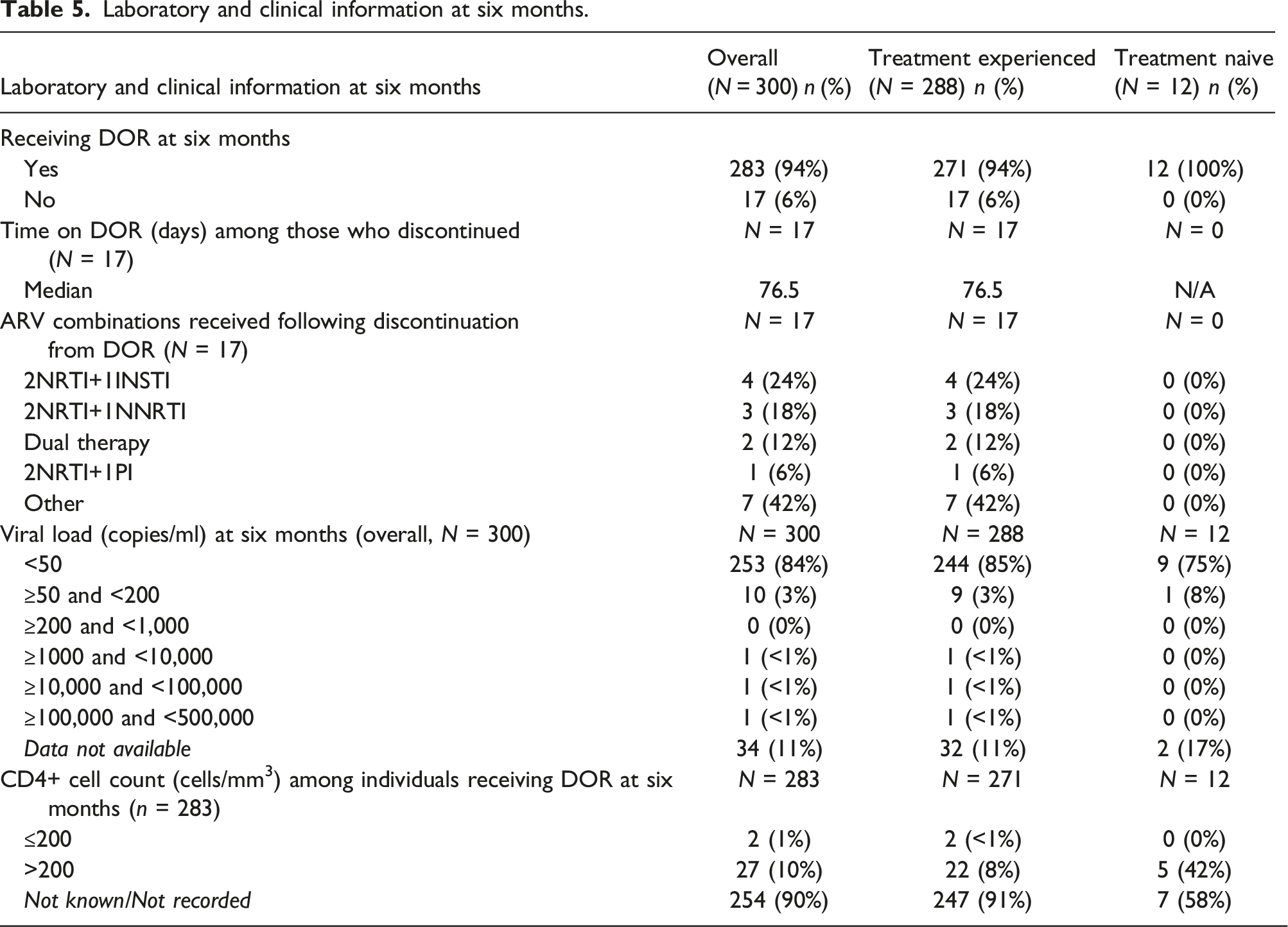
Of the 10 treatment-naïve individuals who initiated a DOR containing regimen and had viral load data available at 6 months, n = 9 had a viral load <50 copies/ml and n = 1 had viral load <200 copies/ml.
Of the 256 treatment experienced individuals who switched to a DOR containing regimen and had viral load data available at 6 months, 95% (n = 244/256) had an undetectable viral load (<50 copies/ml). At 6 months follow up n = 9 had a viral load <200 copies/ml, and n = 3 had a viral load >200 copies/ml. The 9 individuals with baseline NNRTI mutations all recorded viral load <50 copies/ml at 6 months. Nine of the 13 individuals with baseline NRTI mutations had viral load <50 copies/ml at 6 months follow-up, the remaining 4 individuals had no viral load data available.
Discussion
Statement of principal findings, interpretation and implications, comparison to other studies
DRIVE-REAL study aimed to describe characteristics, treatment patterns, and virological outcomes among people living with HIV- initiating DOR in a UK real-world setting. To our knowledge this is the largest study reporting real-world use of DOR in the UK. The demographics and clinical characteristics of our cohort were mostly male and of white ethnicity, largely similar to DOR Phase 3 clinical trial populations, and majority aged 40-64 years, slightly older than in clinical trial programmes5,6,16 Our sample comprised people living with HIV with diverse clinical and lifestyle circumstances, with nearly a quarter reporting being active smokers and 11% engaging in recreational substance use. Of those with body mass index (BMI) data available (n = 174, 58% of overall sample), over half (n = 95, 55%) were living with overweight or obesity. Two-thirds had at least one comorbidity, most commonly mood and cardiovascular disorders, highlighting the burden of mental health and metabolic issues among people living with HIV17,18. As many ART options are limited by DDIs and the polypharmacy burden of people living with HIV greatens with age, it is important to capture real-world outcomes of DOR use in people living with HIV taking commonly prescribed non-ART medications. In the DRIVE – REAL cohort, 70% of individuals were taking one or more co-medications, with 13% taking four or more, this reinforces the need for specialist pharmacists and regular medicine use review in this population given that many commonly co-prescribed medications have potential for DDIs with antiretrovirals. Among individuals with available lipid data, there were relatively high rates of dyslipidaemia at baseline. This may be attributed to a high proportion of individuals switching from EFV-based regimens, or perhaps due to our cohort being majority (77%) over the age of 40, however this should be interpreted with caution owing to the high frequency of unavailable lipid data. Compared to the general population of people living with HIV in England and Wales, 18 the DRIVE-REAL cohort had similar breakdowns of those who are living with overweight or obesity and active smokers, while our cohort slightly overrepresented individuals who were male, of white ethnicity and living with co-morbidities and slightly under-representative of people living with HIV who reported recreational drug use and chemsex. 18
The majority of individuals in our study were treatment experienced with a median time since HIV diagnosis of 12.3 years. Only n = 12 individuals were treatment naïve and this might be due to the data collection being performed soon after DOR’s commercial availability in England for this group, and at a time when new HIV diagnoses continue to decline in England. 1 The low rates of baseline resistance (3% major NNRTI, 5% major NRTI) seen are likely due to the DOR license not recommending use with past or present evidence of resistance to the NNRTI class.
The majority of individuals received DOR/3TC/TDF FDC vs. single agent DOR + backbone, indicating a preference for DOR/3TC/TDF FDC. DOR single tablet was most commonly paired with FTC/TAF (n = 21, 57%), allowing individuals the option of DOR as a third agent when 3TC/TDF may not be appropriate.
Among treatment experienced individuals, 41% switched within class at baseline, potentially reflecting the desire to remain within class while moving to an NNRTI with a resistance profile that is active against prevalent NNRTI-resistant variants, improved DDI profile, reduced CNS toxicity, improved tolerability including more favourable effect on lipids, and no food requirements compared to older NNRTIs.19–27
As previously mentioned, this was a descriptive study and the assessment of outcomes at 6-months follow-up was intended to provide further insights into DOR users and provide groundwork for hypothesis-testing studies. We report encouraging and reassuring virologic outcomes among individuals receiving DOR at 6-months follow-up in our real-world cohort. Of those with viral load data available, 95% achieved or maintained (given the descriptive nature of this study this could not be differentiated) viral load suppression (<50 copies/mL), similar to clinical trials in treatment experienced people living with HIV continuing DOR at 24 weeks. 16 The majority of individuals in DRIVE-REAL remained on a DOR-containing regimen at 6-months, and this low discontinuation rate (6%) suggests DOR is tolerable and durable in a real-world setting which will need to be further analysed in future research. Among those who discontinued, the median time on DOR was 76.5 days, indicating discontinuation is largely not immediate.
At the time of writing, only two peer-reviewed studies examining DOR usage in a real-world setting had been published. Both studies were conducted in Italy and only included treatment experienced people living with HIV. The first single centre study included n = 33 individuals, 28 the second multi-centre study included n = 132 individuals. 29 Compared to our DRIVE-REAL cohort, baseline demographics were widely similar with some variation seen in median time since diagnosis, 22 years for the multicentre study and 11.3 years for the single centre study. Interestingly, the most common ART combinations received prior to switching to DOR were 2NRTI + INSTI in both studies (23% and 36%), followed by 2 NRTI + NNRTI (14 and 33%), indicating an increased confidence among Italian physicians to switch persons living with HIV off INSTI regimens to exploit DOR’s resistance profile. This is also reflected in the multicentre study whereby 43% initiated onto DOR + INSTI dual therapy. Encouragingly, among the multicentre cohort at 6-months follow-up, only a small and comparable percentage (5.7%) to DRIVE-REAL recorded a detectable viral load >50 copies/ml and discontinuation rates were low and similar to DRIVE-REAL at 5.3%, providing further reassurance that DOR is an effective and durable treatment option in multiple real-life settings in Europe.
Strengths and limitations
Our study benefitted from a relatively large sample size considering the medical-chart review nature of this study and extensive data collection of comorbidities, comedications and lifestyle characteristics allowing the detailed characterisation of DOR users in a real-world cohort, outside the exclusion criteria constraints of a relatively homogenous clinical trial population.
Three treatment centres were included in this study to avoid single centre bias and although oversampling was required in the larger centre, a split of 150:80:70 (Chelsea & Westminster: Mortimer Market: Brighton and Sussex) was still achieved. This multicentre sample was selected to be representative of London and non-London based treatment centres.
A limitation of this study was its descriptive nature. While descriptive epidemiology can provide context to further our understanding of a disease by describing the basic attributes of populations and disease contexts, further analyses are needed to utilise these findings in clinical application. It was not within the scope of this study to test whether the outcomes at 6 months were different from those at baseline. Neither was to statistically assess the differences in terms of characteristics, treatment patterns, and virological outcomes between treatment-experienced and treatment naïve individuals. In addition, it was also out of scope to measure reasons for DOR discontinuation nor to analyse 6-months outcomes by baseline characteristics (baseline age, weight, resistance, viral load etc.). The retrospective study design limited aspects of data collection, and as such certain variables, most notably lipid data and CD4 count had incomplete data. The incomplete CD4 count data was likely due to national guideline recommendations to stop monitoring of CD4 if > 350 cells/mm3 on two occasions greater than 1 year apart. 30 As a real-world study, this level of missing data likely accurately reflects testing practices in the UK and would most likely only be rectified by a prospective study design dictating testing schedules. Our case report forms were designed to have robust options for completing physicians, however responses were not exhaustive and free text items limited to enable ease of completion and reporting. The use of data extracted from medical charts carries a possibility of information bias related to the validity of the data reported by the service providers, including missing, inconsistent or erroneous information. To minimize the potential for this bias, the data were checked by two independent researchers and suspected erroneous data was queried with the physicians or delegates and updated where necessary. Due to the COVID-19 pandemic, not all blood tests could take place at 6-month follow-up and were deferred in a small number of cases (n = 13). A sensitivity analysis was performed that demonstrated that the effect of receiving a deferred blood test appears to have been minimal, with the distribution of viral load and CD4+ cell count results unchanged.
Sites were selected with known DOR usage and who were willing and able to conduct this study, this however may have been a contributing factor to the high representation of male individuals. As such, our cohort may not be generalisable to all clinics and people living with HIV in the UK, most notably non-urban clinics and regions outside the South of England, and our sample not representative of all people living with HIV in the UK1,18 specifically women, individuals of minority ethnic backgrounds, and those with high baseline viral load.
Conclusions and future research
This descriptive study including 300 adults showed that individuals living with HIV in the UK initiating DOR-containing ART are mostly male, of white ethnicity, and aged between 40-64 years. Individuals prescribed DOR in clinical practice are majority ART treatment-experienced, with a high frequency of comorbidities along with the associated burden of co-medication. In addition, the majority of individuals at 6 months follow-up, remained on DOR and maintained or achieved HIV viral suppression. Our results may be useful in guiding clinical practice when considering DOR-based ART and in providing useful data to support subsequent hypothesis-testing studies assessing the differences between treatment-experienced and -naïve individuals, DOR effectiveness, tolerability, and reasons for discontinuation in cohorts not typically represented in Phase 3 studies.
Footnotes
Acknowledgements
Thanks to Ian Williams as principal investigator for Mortimer Market Centre. Edita Custic and Ute Pfaff of MSD for their input into study management. Ivana Rajkovic for study design work, Will Ambler for data collection and analysis, all of Adelphi Real World. Yohance Whiteside, Emiliano Bissio, Rebeca Plank and Benedikt Funke of MSD for review work.
Author contributions
COH, SG, YG, A Moore, OR-H, AM contributed to the concept and design of the work. SL, VC, CM, SR, CN were responsible for data acquisition. COH, NS, WH, A Moore, OR-H contributed to the analysis and interpretation of the data. COH and WH drafted the manuscript. All authors contributed to manuscript review, and all authors give final approval of the manuscript and agree to be accountable for all aspects of the work.
Declaration of Conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Ana Milinkovic has received honoraria for consultancy and speaker services, as well as support for conference attendance from Gilead Sciences, MSD, Janssen and ViiV Healthcare. Prof. Yvonne Gilleece has received honoraria for consultancy and speaker services, as well as support for conference attendance from Gilead Sciences and ViiV Healthcare. Olivera Rajkovic-Hooley and Adam Moore are employees of Adelphi Real World, who received funding from MSD for this analysis/manuscript development. Charlotte O’ Halloran, Nipur Siani and William Hickey are employees of MSD (UK) Limited, London, UK and may own stock and/or hold stock options in Merck & Co., Inc., Rahway, NJ, USA. Stuart Gaffney was an employee of MSD (UK) Limited, London, UK at the time the study was conducted. No other author disclosures or conflicts of interest to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Merck Sharp and Dohme UK.