
Abstract
Purpose
This study aims to elucidate the demographic characteristics, clinical features, diagnostic approaches, and medical management of patients with ocular syphilis, known as ‘the great masquerader,’ at a tertiary eye care center in Nepal.
Methods
We conducted a retrospective review involving 15 eyes from ten patients with ocular syphilis treated at a uveitis referral center between 2020 and 2022. Lumbar puncture was performed if neurosyphilis was suspected. Treatment success was defined as the absence of ocular inflammation in both eyes and a decrease in Veneral disease research laboratory (VDRL) titres after completing therapy.
Results
A total of 15 eyes of 10 patients were diagnosed with syphilitic uveitis based on positive treponemal and non-treponemal serological tests. The mean age of the patient was 39.9 years (range 22-54 years) with an equal distribution between males and females. HIV coinfection was not found in any of the patients. Syphilitic uveitis was the primary presentation in nine patients (90%), while one patient presented with recurrent nodular scleritis. Ocular involvement was bilateral in 50% (5 patients). The mean duration between the initial symptom and the first presentation was 8.7 weeks (range: 4 days to 24 weeks). The most common ocular findings was panuveitis (6 eyes). Eight patients with early syphilis received weekly intramuscular injections of benzathine penicillin G for 3 weeks whereas 2 patients with neurosyphilis were treated with intravenous ceftriaxone 1 gm twice a day for 14 days. Signs and symptoms of majority of patients improved with systemic therapy for syphilis.
Conclusions
Syphilitic uveitis should be included in the differential diagnosis of any form of ocular inflammation.
Introduction
The first recorded instance of a syphilis outbreak was documented in Italy in the late 15th century and was widespread across Europe in the 18th and 19th centuries. 1 However, in the early to mid-20th century, the prevalence of the disease declined significantly with the widespread use of antibiotics. 1 Since the beginning of the 21st century, there has been an increase in rate of syphilis in many countries, primarily among among men who have sex with men (MSM). 2
In the context of Nepal, a survey done by Storm et al. revealed a significant prevalence of active syphilis, reaching 4% in MSM and 11% among transgender women in terai highway districts. The susceptibility to the spread of sexually transmitted infections (STIs) is heightened in this region due to the open border with India, high population density, as well as sex work and drug trafficking activities across the border. 3
Syphilis, caused by the bacterium Treponema pallidum, follows a multifaceted clinical course that can be categorized into four stages: early (primary syphilis, secondary syphilis, early latent syphilis), and late (late latent, and tertiary syphilis). The disease is highly contagious in primary, secondary stage or early latent stage with mucocutaneous involvement. However, late latent syphilis and tertiary syphilis are considered to be non-infectious stages of the disease. 4 Also known as the “Great Masquerader,” syphilis can imitate a range of ocular diseases, predominantly uveitis, along with interstitial keratitis, chorioretinitis, retinitis, retinal vasculitis, optic neuropathy and cranial nerves palsies. 5 Uveitis is seen in approximately 0.6% to 2.0% of patients with syphilis at any stage, and the prevalence can rise to 9% in individuals co-infected with syphilis and HIV. 6 It’s important to identify HIV coinfection in all patients diagnosed with syphilis due to potential variations in clinical symptoms and treatment strategies for syphilis in such cases. 4
The mainstay of treatment is systemic antibiotics and depends on the stage of the disease. As per center for disease control and prevention (CDC) guidelines,
7
• Primary/Secondary syphilis/Early latent: single dose of intramuscular (IM) penicillin G benzathine 2.4 million units, or procaine penicillin, 2.4 million units IM daily for 14 days. In patients who are allergic to penicillin, ceftriaxone/doxycycline/azithromycin can be used • Latent latent syphilis: IM penicillin G benzathine 2.4 million units weekly for 3 weeks • Tertiary syphilis with normal cerebrospinal fluid (CSF): IM penicillin G benzathine 2.4 million units weekly for 3 weeks • Neurosyphilis/Ocular syphilis/Otosyphilis: aqueous crystalline penicillin G, 3 to 4 million units intravenous (IV) every 4 hourly for 10 to 14 days
However, ocular syphilis is treated as neurosyphilis even if CSF examination is normal. Regular monitoring through VDRL tests is recommended to ensure adequate response to therapy. Post-treatment VDRL tests should be repeated every three months for a period of 1-year as titers should become nonreactive within a year after therapy. 4
Despite the increasing prevalence of syphilis and its potential impact on ocular health, there is a notable paucity of data, particularly from regions such as Nepal. This study aims to address this gap by presenting a retrospective review of ocular syphilis cases over the past two years at a tertiary eye care center in Nepal. Through a detailed analysis of demographic characteristics, clinical features, and treatment outcomes, this research contributes valuable insights that can inform clinical practice, prompt routine syphilis screening in uveitis workups, and lay the groundwork for future investigations in this evolving field.
Methods
Study design
This retrospective review aimed to analyze cases of ocular syphilis treated at uveitis clinic of a tertiary eye center of Nepal (B.P. Koirala Lions Centre for Ophthalmic Studies) between 2020 and 2022. Our clinic, being a prominent uveitis referral center, routinely receives referrals from regional ophthalmologists, general practitioners, and local health facilities. The diverse patient population, comprising both urban and rural residents, ensures a robust representation of ocular syphilis cases in the Nepalese context. The clinic annually manages a substantial number of patients, providing a comprehensive clinical perspective on ocular diseases.
Patient selection
Patients included in the study were those with a confirmed diagnosis of ocular syphilis, established through positive treponemal and non-treponemal serological tests, and treated at the uveitis referral center during the specified timeframe.
Data collection
Demographic information, including age, gender, marital status, and occupation, was extracted from patient records. Sexual orientation, recorded according to national ethics guidelines, and history of drug abuse were also documented. Duration of symptoms before diagnosis, extraocular signs (such as rashes and ulcers), and other systemic features were collected.
Ophthalmologic examination
Patients underwent a comprehensive ophthalmologic examination, including measurement of best-corrected visual acuity (BCVA), intraocular pressure (IOP), anterior segment examination with slit-lamp, and fundus examination using 90D and 20D lenses at each visit. Uveitis was classified according to the Standardization of Uveitis Nomenclature (SUN) classification. 8
Laboratory investigations
Routine uveitis investigations, including complete blood count, random blood sugar, and serology for HIV, hepatitis B (HbsAg), and hepatitis C (HCV), were performed. VDRL screening was conducted, and if reactive, confirmation was done using the treponema pallidum hemagglutination test (TPHA).
Diagnosis of ocular syphilis
The diagnosis of ocular syphilis was based on positive results from both non-treponemal and treponemal serological tests alongside ocular examinations. Lumbar puncture was performed only in cases with neurological signs or symptoms (headache, visual disturbances).
Treatment protocol
Patients diagnosed with syphilis received treatment based on the stage of the disease, following the CDC guidelines. Early syphilis cases received weekly intramuscular injections of benzathine penicillin G for three weeks, while neurosyphilis cases were treated with intravenous ceftriaxone 1 gm twice a day for 14 days. Treatment success was defined as the absence of ocular inflammation in both eyes and a decrease in VDRL titers after completing therapy.
Outcome measures
Visual outcomes were assessed through BCVA at initial presentation and at final follow-up. Post-treatment VDRL tests were repeated every three months for one year to monitor the resolution of titers.
Statistical analysis
Descriptive statistics, including mean and standard deviation (SD), were used to summarize demographic and clinical data. Snellen BCVA was converted to logarithm of the minimum angle of resolution (logMAR) for statistical analysis.
Ethical considerations
The study protocol adhered to ethical standards and was approved by the institutional review board. Patient confidentiality was strictly maintained throughout the study.
Results
Demographics and Clinical Manifestations of syphilis patients.
M: Male; F: Female; RE: Right Eye; LE: Left Eye; BE: Both Eye; DOV: Diminution of vision; VA: Visual acuity; HM: Hand motion; CFCF: Counting fingers close to face; NPL: No perception of light; logMAR (logarithm of the minimum angle of resolution); IM: Intramuscular; IV: Intravenous, MU: Million units; bd: twice daily.
The presentations encompassed anterior scleritis, anterior non-granulomatous uveitis, intermediate uveitis, panuveitis, retinitis, and papillitis. Panuveitis was observed in six eyes (40%) from five patients, posterior uveitis in three eyes (20%) from two patients, acute anterior uveitis in three eyes (20%) from two patients, intermediate uveitis in one eye, and papillitis in one eye. Most common posterior segement presentation was peripheral millet like retinochoroidal infiltrates Figure 1. Concurrent integumentary findings were seen in 60% Figures 2, 3 and 4. Fundus photo of right eye with peripheral millet like retino-choroidal deposits and fundus fluorescein angiography (FFA) of superotemporal retina of right eye and inferotemporal retina of left eye showing multiple pin point leakage. Clinical photo before & after treatment showing complete resolution of the maculopapular rashes in the neck region. Clinical photograph showing normal findings in RE (A) and vitritis in LE (B). Fundus photograph showing normal fundus findings in RE (A) and a hazy view in LE (B). Cystoid macular edema in left eye (before and after dexamethasone treatment). Multiple annular violaceous plaques with silvery white scales over bilateral lower limbs.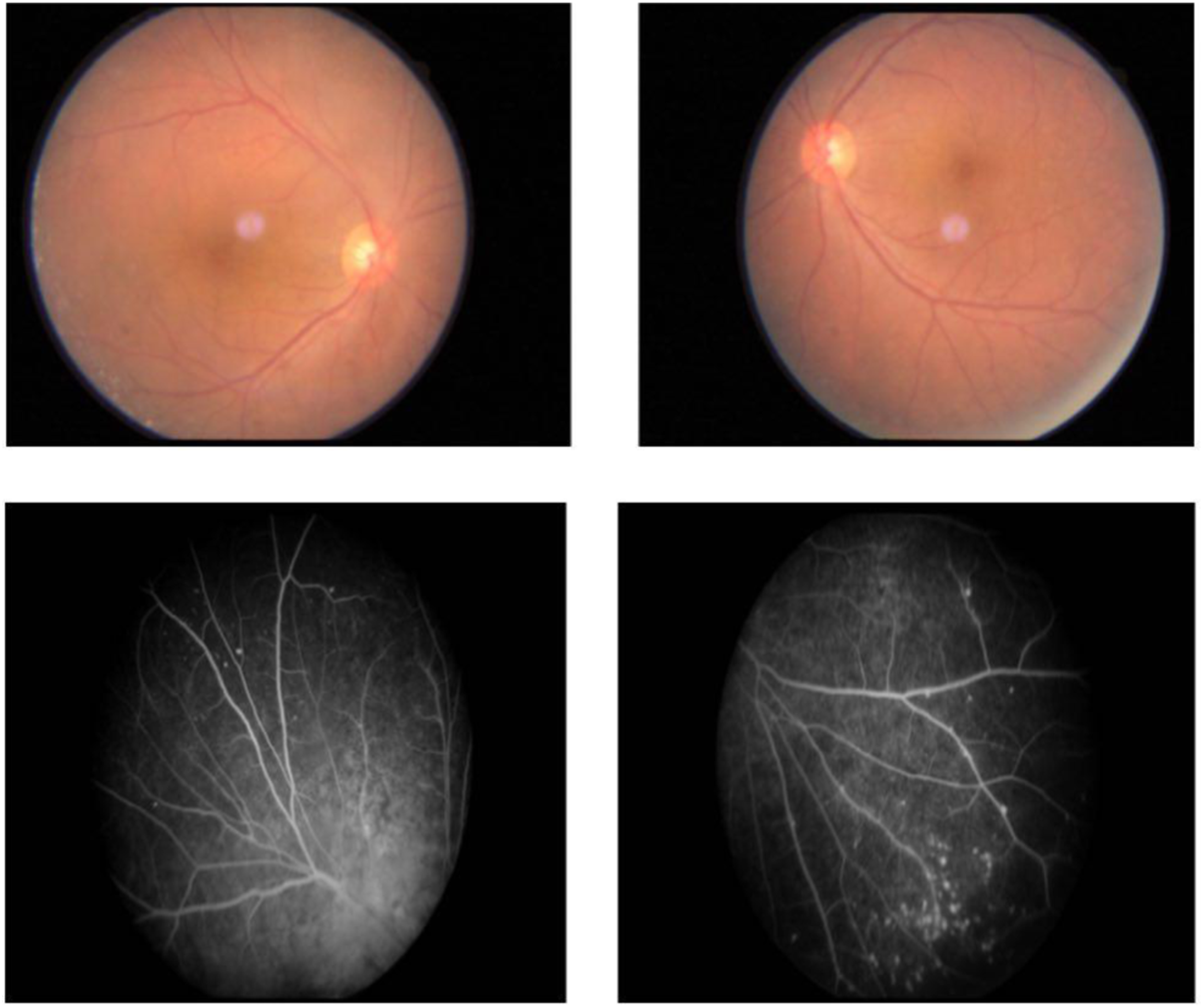



Seven patients (70%) were classified as secondary syphilis, two patients (20%) as neurosyphilis and one as early latent syphilis. Ocular involvement was bilateral in 50% (5 patients) of the cases. Among these, two cases had distinct manifestations in each eye – one case presented with posterior uveitis in one eye and panuveitis in the other, while the other case displayed anterior uveitis in one eye and panuveitis in the other. In a case of panuveitis (Figure 5), cystoid macular edema was also present and it responded well to treatment with intravitreal dexamethasone Figure 5. Maculopapular rashes with scales on the palm.
The mean duration between the initial symptom and the first presentation was 8.7 weeks (range: 4 days to 24 weeks). The most common initial symptom was diminution of vision (DOV) (70%). Most patients (90%) initially sought medical attention when the eyes were involved despite having other systemic symptoms. Upon diagnosing uveitis, 90% patients reported extraophthalmologic features such as rash or neurologic signs. Subsequently, the ophthalmologist referred them to relevant departments for additional evaluation. This also highlights the importance of early diagnosis and treatment of syphilis by ophthalmologists, even prior to confirming a diagnosis of systemic syphilis.
Two cases (case 1 and case 6) were misdiagnosed as idiopathic scleritis and Vogt Koyanagi Harada (VKH) respectively and were treated with oral steroids and immunomodulators prior to presentation at our hospital.
All cases were HIV negative. Screening for spouses was possible only in 4 cases, all of which were negative.
Lumbar puncture and CSF analysis was done in two cases (case 6 & case 9) and showed lymphocytic pleocytosis (100% lymphocytes) and increased protein (>50 mg/dl). CSF VDRL and TPHA were positive in both cases.
Eight patients with early syphilis received weekly intramuscular injections of benzathine penicillin G for three weeks, while two cases of neurosyphilis were treated with intravenous ceftriaxone for 14 days. Best-corrected visual acuity improved in 93.33% of eyes after treatment. Mean BCVA at initial presentation was 1.067 logMAR (range 0–3), improving to 0.1 logMAR (20/25 Snellen) at final follow-up. One patient had no perception of light (NPL) secondary to glaucomatous optic nerve damage.
Discussion
The resurgence of syphilis globally, coupled with its varied and challenging manifestations, necessitates a thorough exploration of specific clinical contexts. Our study contributes valuable insights into the demographic attributes, clinical presentations, and management outcomes of ocular syphilis. In a retrospective study conducted by Ranju et al. at the same center where this current report was prepared, spanning from 2012 to 2017, 4359 cases of uveitis were studied,with merely 3 cases of syphilis, further underscoring the current resurgence of syphilis in the global context. 9
Contrary to some existing literature,6,10,11 our findings revealed an equal gender distribution, challenging the prevailing notion of male predominance. This discrepancy may reflect evolving epidemiological trends in syphilis in Nepal or highlight unique socio-cultural factors influencing disease patterns in this region.
The most frequent form of ocular inflammation in this series was panuveitis, seen in 60% of eyes which is in accordance with other reports.11,12 The varied ocular presentations, ranging from scleritis to papillitis, reaffirm syphilis’ epithet as the “Great Masquerader.” Early and accurate diagnosis remains challenging due to its ability to mimic various ocular pathologies. This challenge is exemplified by the misdiagnoses of two cases as Idiopathic Scleritis and VKH syndrome, emphasizing the need for heightened clinical suspicion and comprehensive diagnostic approaches.
Contrary to many reports associating syphilis with HIV coinfection, our study did not identify any cases with concurrent HIV infection.
Early and accurate diagnosis is crucial, as highlighted by the delay in presentation seen in one case (case 3), contributing to glaucomatous optic nerve damage. Prognosis is good if treated early and most patients recover without experiencing long term complications. Poor visual prognosis have been reported mostly in cases associated with sequelae, in cases with delayed presentation/diagnosis and treatment. Moreover, syphilitic uveitis is commonly associated with raised intraocular pressure and is one of the leading causes of secondary glaucoma in uveitis which can also account to poor vision. 5 However, most of the cases in our study had normal IOP except for a case of intermediate uveitis with secondary glaucoma who had low vision at presentation and despite treatment no visual improvement was seen due to glaucomatous optic nerve damage.
In our report, most patients had syphilis diagnosed during the secondary stage of the disease. Ocular manifestations in secondary syphilis can emerge as late as 6 months after the initial infection, a timeframe in which many of the systemic symptoms have already subsided. So, in the context of clinical practice, it’s crucial to acknowledge that many patients showing ocular signs of syphilis might not necessarily display the systemic signs of the disease. Approximately half of the patients with ocular manifestations in tertiary syphilis have associated systemic signs of the disease. 4 Hence, the importance of detailed history taking cannot be overlooked while examining a patient suspected of having ocular manifestations of syphilis.
In general, acute inflammatory presentations like episcleritis, scleritis, iridocyclitis, and retinitis are more commonly associated with secondary syphilis, whereas chronic granulomatous inflammation of the ocular structures is typical of tertiary syphilis, even though a considerable degree of overlap exists between the two. 4
While the majority of reports describe the cohort as predominantly male gender, consisting MSM, and a significant proportion testing positive for HIV, our findings present a different picture: there is no gender bias, no presence of MSM, and no cases of HIV co-infection.
As ocular syphilis is considered a form of neurosyphilis, existing treatment protocols recommend addressing it in alignment with neurosyphilis treatment. However, in our study, we opted for different approach, treating all patients with weekly three doses of intramuscular Benzathine penicillin, except for two cases presenting with neurosyphilis. These particular cases received a 14-days intravenous ceftriaxone treatment due to the unavailability of crystalline penicillin. Visual outcomes were favorable in the majority of cases.
The successful outcomes observed in our study, marked by improved visual acuity and resolution of ocular inflammation, reinforce the effectiveness of the recommended treatment protocols. Although our approach deviated slightly from existing guidelines due to penicillin availability issues, the favorable responses indicate the potential flexibility in treatment modalities.
This study had several limitations, including its retrospective design, which may introduce inherent biases and rely on available records, potentially leading to incomplete data capture. Additionally, the sample size was relatively small, and the study was conducted at a single center, limiting the generalizability of the findings. Future research endeavors should prioritize large-scale, multicenter, and prospective studies to overcome these limitations, providing a more comprehensive understanding of ocular syphilis and enhancing the external validity of the results.
Conclusion
Our study emphasizes the pivotal role of ophthalmologists in the early identification and management of syphilitic uveitis. The atypical gender distribution, diverse clinical presentations, and successful treatment outcomes contribute to the evolving understanding of ocular syphilis. Typical risk factors may or may not be present or disclosed at initial consultation. So, it is crucial to incorporate syphilis screening as a part of routine workup for uveitis, optic neuritis, vasculitis owing to the varied presentations and the potential for ocular involvement as an initial manifestation. The multifaceted nature of syphilitic uveitis mandates ongoing research efforts, and our study sets the stage for future investigations in this evolving field.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent
Written informed consent for patient information and images to be published was taken from all the patients
Data availability statement
The authors confirm that data supporting the findings of this study are available within the article.