
Abstract
Background
MPOX (Monkeypox) viral infection, a zoonotic disease previously confined to the African sub-continent, has caught attention worldwide recently due to its resurgence in a new ‘avatar’ among urban communities. Dermatologists in the U. A. E. started to see patients with fever and a self-limiting pustular necrotic rash that was negative for all other infectious investigations.
Methods
We performed a prospective observational multicenter clinical study of the demographics, skin manifestations, and outcomes of patients presenting with necrotic pustular lesions and/or fever.
Results
35 cases of PCR confirmed MPOX cases, mostly in the expatriate population, were followed up and found to have high-risk heterosexual contact on an average of 1 week prior to disease onset. We found that they have characteristic annular pustular lesions with necrotic center or “Smoke ring pustules’ in all cases. Lesion tenderness and predilection for the lower abdomen, pubic area, and genitalia were observed. Most cases were systemically stable, with fever lasting for an average of 4 days and elevated CRP levels. Genital lesions were prone to secondary bacterial infections. The disease was severe, with larger annular plaques in one of our patients found to be living with HIV.
Conclusions
The overall prognosis in healthy individuals is good, with lesions healing within an average of 2 weeks without scarring. ‘New world MPOX’ should be unclassified from zoonosis to a sexually transmitted infection (STI) capable of transmission in an urban population. Our findings can help in early clinical suspicion and differentiation from other STI’s for primary and secondary health care physicians.
Short summary
A study of patients with monkeypox infection in our region showed clinically unique features that can help clinicians to differentiate it from other sexually transmitted infections. We also found that MPOX showed an overall good prognosis except in patients living with diabetes or HIV.
Introduction
Monkeypox (MPOX) has been recorded in medical annals for several decades as a zoonotic endemic disease in Africa, caused by two phylogenetically distinct clades of MPOX viruses called Clade-1 and Clade-2.
Materials and methods
Fever with peculiar pustular and necrotic skin lesions in UAE was found to be MPOX by viral PCR and culture of skin lesions from the Central Veterinary Research Laboratory, U.A.E. Hence we did a
Results
Epidemiology of study population
A total of 35 patients were enrolled in our study, of whom 32 were men and 3 were women. Their ages ranged from to 20–56 years an average of 31.7 years. The patients were of Asian, African, or Middle Eastern descent. Twenty-one of these patients were married. Recent sexual exposure was reported in 30 cases (85.5%). The average time from exposure to rash was 1–21 days (average 7.52 days), excluding the patient living with HIV, which was 30 days. Of the sexual exposures, 17 were from sex workers and spa/massage therapists, five were from unmarried partners, three were from marital partners, and others were unspecified. Twenty-eight cases were heterosexual, and two were homosexual. Nine patients (25.7%) used condoms, which did not protect them from the disease. Similar lesions were present in the partner at exposure or later in only 3 cases. We did not obtain any significant contact history with sick animals or handling raw meat from desert animals or camel meat. Travel history was present in five patients within 3 months. There were no cases of households spreading to adults, children, or the elderly who lived in the same household or accommodation. None of the patients had a history of blood transfusions.
Clinical features of our cases
Fever was noted in 26 (74%) of the 35 cases. Fever was mild in eight, moderate in nine, and severe in nine patients. The fever ranged from to 1–21 days, with an average of 4.4 days. The associated features noted were lesion tenderness, itching, headache, sore throat, eye symptoms such as redness and discharge, dysuria, urethral discharge, and gastrointestinal symptoms such as diarrhea and abdominal pain. All except one patient had polymorphic lesions.
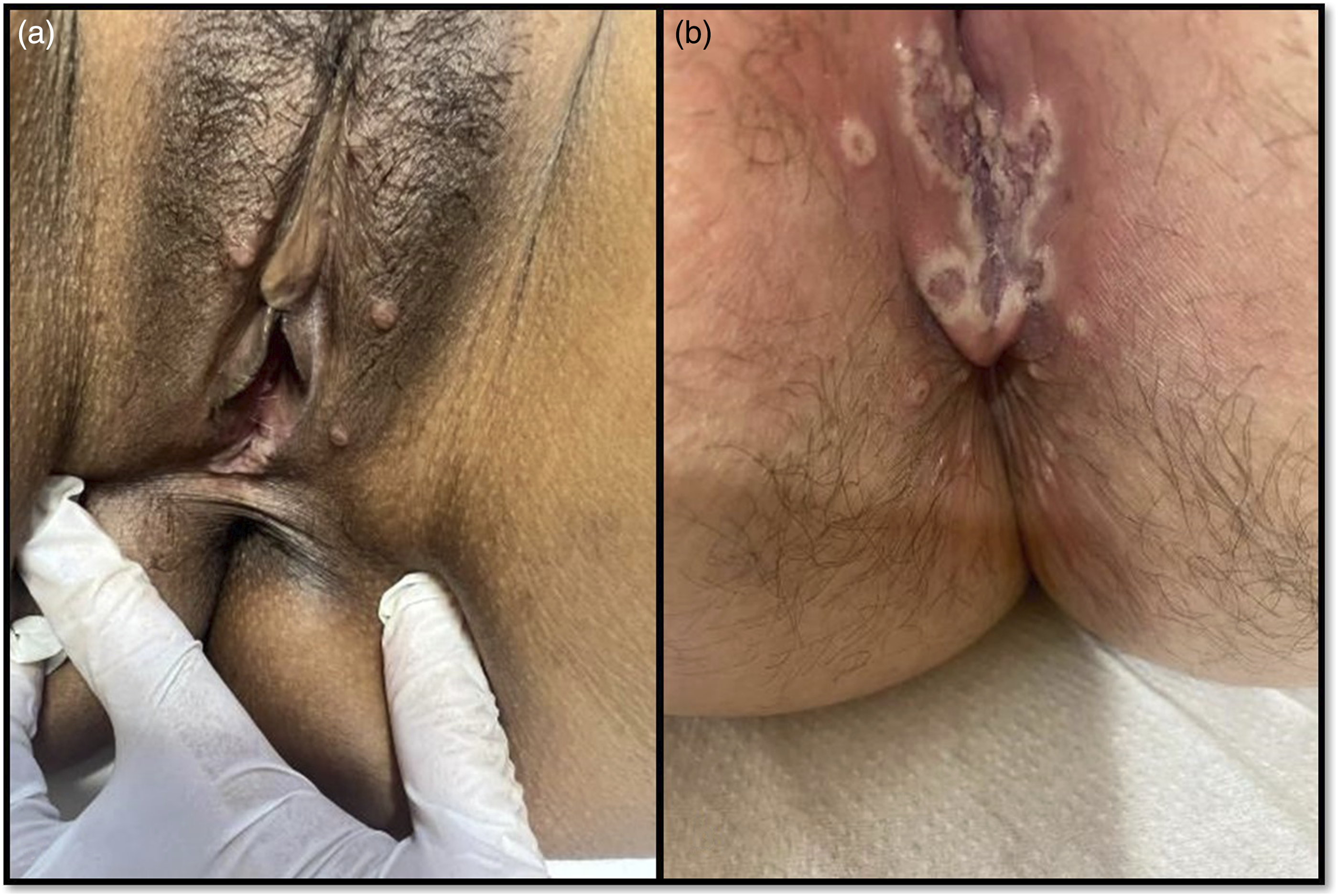
The types of skin lesions seen in our cases, in decreasing order of frequency, were necrotic annular pustules (27 cases), pustules (25 cases), papulo-vesicles (20 cases), genital ulcers (16 cases), umbilicated papules (13 cases), erythematous papules (10 cases), crusted papules (3 cases), inguinal ulcer (one case), and maculopapular lesions (one case). The primary and most frequent site of rash was the genitalia in majority of cases (71.4%). Of these, 22 showed penile papules/pustules/ulcers (Figure 1) and 3 females showed labia majora and minora papules or ulcers (Figure 2). The other affected sites (Supplemental material) were in decreasing order of frequency: upper limb (16 cases), abdomen (16 cases), face (15 cases), lower limb (14 cases), chest (13 cases), back of trunk (13 cases), scalp (8 cases), neck (5 cases), lower abdomen and pubic area (4 cases), buttocks (two cases), and inner thighs (1 case). New lesions arose for 1–14 days, with an average of 8 days. The lesions evolved from small papules to papulo-vesicle-like lesions progressing to papulo-pustule, to pustule with erythematous rim, then the center of the pustule changed color to pink, studded with red dots, and then grey and black, forming necrotic papules with annular pustules (Figure 3). During healing the central necrotic scab detached leaving a crateriform lesion, evolving to macules with peripheral scale, and healed mostly without leaving scars. The rash healed within an average of 13.3 days. Two patients had a prolonged course, one of which was newly found to be living with HIV (Figure 4) and the other was a diabetic patient with secondary bacterial infection of the genital ulcer (Figure 5). The vitals were stable in all cases. No hepatosplenomegaly was detected in any of the patients. Lymphadenopathy was found in 22 cases (62.8%) involving inguinal, cervical or submandibular nodes. Spectrum of genital lesions in male: MPOX cases shows necrotic annular pustule with inflammatory erythema and edema surrounding and satellite pustules on the shaft of the penis; discrete necrotic annular pustule in the pubic area and shaft of the penis without much inflammation; annular pustule with erythematous center forming an ulcer along coronal sulcus, skin colored annular plaques and papules reminiscent of condyloma lata on the shaft of the penis, confluent annular necrotic pustules forming scalloped pustular border resembling herpes genitalis; phimosis due to inflammatory edema from discrete annular pustules on the foreskin of the penis. Spectrum of genital lesions in female: discrete flat papules on labia majora reminiscent of condyloma lata, confluent annular necrotic pustules forming an irregular ulcer with scalloped pustular border and satellite pustules some with central necrosis on labia some of which are perianal. Shows evolution of skin lesions from small papule to papulo-vesicle like lesion progressing to papulo-pustule, to pustule with erythematous rim, then umbilicated pustule, then annular pustule with pink center studded with bright red dots, then annular necrotic pustule with inflammatory halo, then a crateriform papule that peeled off and resolved with a pigmented scar. MPOX co-infection with HIV: 3-5 cm annular necrotic plaques affecting left nostril, upper back, leg and glans penis. MPOX in a diabetic patient: Started as umbilicated pustules with intense inflammatory edema of genitalia, progressing to necrotic ulcers on the shaft of the penis, after debridement, and re-epithelization after antibiotics.



Investigations
MPOX PCR tests by PCR were positive in all cases. Other laboratory tests were done selectively according to the patient. An HIV test was done in 21 out of 35 patients and one was positive. Concomitant sexually transmitted infections (STIs), such as syphilis, urethritis, and hepatitis B and C, were ruled out in all tested cases (around 50% of cases). Few showed urine abnormalities like RBCs, WBC’s in urine, mucus thread, and leukocyte esterase positivity despite negative bacterial cultures and negative urethritis screening. Sixteen patients had an elevated CRP with average value of 36.67 mg/dl. Wound culture from genital ulcers grew several Gram-positive and negative bacteria which were treated appropriately.
Skin biopsy was performed in three cases (Figure 6). It showed ballooning degeneration of keratinocytes with eosinophilic inclusion bodies, diffuse neutrophilic infiltrate in the dermis, and peri-adnexal. No leukocytoclastic vasculitis was noted in any of the 3 cases. Biopsy from our patient living with HIV co-infected with MPV showed necrotizing myositis and fasciitis in the muscles and panniculitis with small- and medium-vessel vasculitis and extensive dermal necrotizing thrombotic vasculitis with mixed septal and lobular necrotizing panniculitis in the skin. Histology of MPOX skin lesions H&E: (a) shows low power view of skin lesion. Epidermal necrosis is seen with a protruding area showing serum collection and neutrophilic infiltrate that corresponds to an annular pustule seen clinically. Dermis shows perivascular and peri-adnexal neutrophilic infiltrate. (b) shows high power view of the necrotic epidermis with neutrophilic infiltrate up to the stratum corneum, and congested superficial blood vessels that correspond with dark red spots seen in early annular pustules (c) shows a closeup of peri-eccrine neutrophilic infiltrate (d) 40x magnification showing intra-cellular eosinophilic inclusion bodies inside keratinocytes (arrow).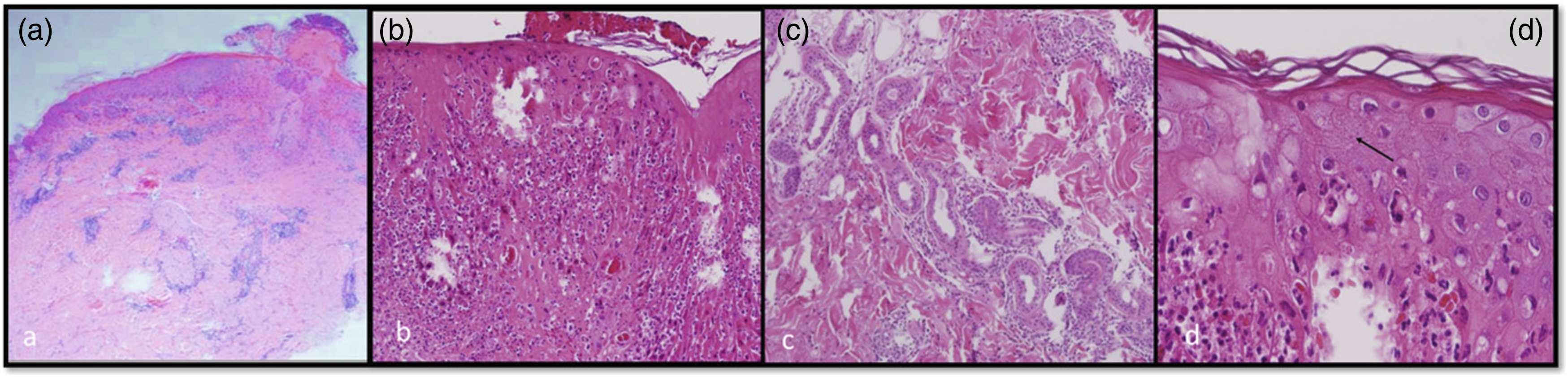
Discussion
Sexually active young adults affected
Young sexually active adults were mostly affected with an average age of 31.7 years which is comparable to the reports from other countries. 1 But compared to the case series by Patel et al 2 from Central London where the majority of MPOX infections were in bisexual or gay men, in our series only 5% of these cases reported same-sex contact. The cause of disparity is unknown, but the demographics of Central London, which has a large population of LGBT communities, the presence of a single working expatriate population in this area, and unwillingness to report same-sex behaviour due to legal or moral concerns could be contributing factors for the different demographics.
Route of transmission was mainly high-risk sexual contact
The average incubation period was difficult to precisely calculate, as 31% had multiple contacts with different partners. However, the average time from the last exposure to rash onset was 7.5 days except in the patient living with HIV where the skin lesions took 1 month to develop after the last heterosexual exposure. A higher risk was observed in individuals seeking sex workers or receiving sexual favors from massage therapists (48%). Condoms surprisingly did not give full protection, as nine cases occurred in men who used condoms and developed lesions on the lower abdomen and pubic area initially sparing the penis (Supplemental material Figure 6); this may be because monkeypox viruses can be transmitted by breaks in the skin or other body fluids like saliva. 3 There are reports of MPOX outbreaks from a tattooing center in Spain that resulted in 20 infections 4 ; however, we did not have a history of tattoos in our cases. Most sexual contacts were clinically ‘asymptomatic' and thus possibly become temporary carriers and transmitters of the disease. 5
Rare non-sexual close contact
One interesting finding was of possible skin-to-skin transmission after one male patient developed lesions after he helped to drain the ‘boils’ of his female coworker with his bare hands.
Predominance of rash in genital and pubic area
Genitalia were predominantly affected sites in our study. The pox virus is adapted to epidermal cells and thus the initial site of infection resulting from direct inoculation may be the skin, mucosal surface, or respiratory tract, as observed in rural African MPOX infections. The virus then spreads through the regional lymphatics to cause viremia and the involvement of the reticuloendothelial system with secondary viremia. 6 This could explain why the initial rash and predominant area of affection is genitalia in the majority of our cases and later rash became generalized; contrast this with only 30% genital involvement for endemic African MPOX infections. 6
Other areas of involvement
Apart from the trunk and limbs, a predilection for the face (60%) and scalp (32%) seems to be a differentiating feature in early disease (Supplemental material Figure 3, 5). Tenderness of the lesions and crowding of lesions in the lower abdomen and pubic area (Supplemental material Figure 6) were also differentiating features from other similar diseases. In our study predictors for secondary infection of ulcers and necessity for cultures and antibiotics/antifungals were as follows: frankly purulent discharge, progressive non-healing skin lesions beyond 2 weeks, enlargement of ulcers more than 1 cm, persistant high fever and edema of the genitalia. Oral lesions were seen in 17% of the cases as papules or erosions (Supplemental material Figure 7). Eye symptoms were observed in 8% of the cases and have been described in detail by Kaufman et al. 7
Disease course
The necrotic annular pustules seem to be specific to MPOX skin infection, and we would like to call this the ‘smoke ring sign’. This helps to differentiate MPOX from all other pox viruses and similar diseases early in the course of the disease. The Central London cases 2 had erythematous maculopapular rash in 13.7% of cases compared to only one case in our study, and the patient had a history of taking an antibiotic before the onset, and he improved on stopping the antibiotic.
Women with MPOX
Three female patients with MPOX had genital ulcers (Figures 1 and 2) with inconspicuous scattered body lesions. One patient developed conjunctivitis/episcleritis (Supplemental material Figure 7). The lesions on the genitalia in the women were easily ulcerated, were more painful, and needed constant pain medication compared to the male patients.
Urethritis like syndrome in MPOX in the absence of evidence of other STI’s
Another notable feature was dysuria and/or seropurulent discharge (11%) and/or abnormal urine routines (25%) in the absence of investigatory evidence for other sexually transmitted infections, such as gonococcal or common causes of non-gonococcal urethritis, by PCR and culture. This may aid in transmission in the absence of skin lesions. Hematuria, a clinical feature of monkeypox, has also recently been described. 8
MPOX in patient co-incidentally detected to be HIV positive
A 34-year-old Nigerian adult male patient was concomitantly diagnosed with HIV, CMV and MPOX when he presented with 3 weeks of a skin rash that started on the genitalia and then spread to the rest of the body. Skin lesions were larger compared to other cases in this series and were located on the trunk limbs and genitalia (Figure 4). Despite starting antiretroviral therapy and ganciclovir, the patient died of his disease 45 days after admission. Tecovirimat wasn’t started due to unavailability. A similar report of genital MPV lesions in a patient living with HIV was treated with tecovirimat with improvement in his condition. 9 Unlike our study which had STI screening selectively, other studies have found that a substantial proportion of monkeypox cases may be coinfected with HIV or other STIs, which is why CDC 10 recommends testing for other sexually transmitted infections once a diagnosis is established. However, compared to previous endemics in Africa, the death rates secondary to MPOX infections outside Africa is low (<5%) 11 according to the current literature.
MPOX in diabetic patient
We had one protracted case of monkeypox in a 41-year-old diabetic male (Figure 5), who presented with typical lesions that rapidly progressed, to genital skin necrosis and swelling and treated with antibiotics and debridement for secondary infection with carbapenem-resistant E. coli. The ulcer healed 3 weeks after with scarring. There is a theoretical review predicting susceptibility and severity of MPV infection in poorly controlled diabetes, which seems to hold true in our diabetic case. 12
Investigations in MPOX cases
Skin biopsy of necrotic papules showed viral cytopathic changes (Figure 6) and can be misdiagnosed as herpetic folliculitis, herpes zoster, smallpox, or leukocytoclastic vasculitis, and only PCR can help in this situation. The skin pathology of MPOX lesions has been described previously by Bayer-Garner et al 13 and for the current epidemic by Chalali et al. 14
Differential diagnosis
MPV infection can present only solely as genital ulcers.14,15 The main differential diagnoses assigned by non-dermatologists who referred such cases are discussed in Supplemental material Table 1, with useful pointers for correct diagnosis.
Conclusion
In our study, we found that the new wave of MPOX has some unique clinical features that differentiate it from other diseases, such as smoke ring pustules, lesion tenderness, and predilection for genitalia and pubic area/lower abdomen. The prognosis is good in immunocompetent patients, and the lesions heal mostly without scarring. Consider MPOX in healthy sexually active adults presenting with varicella-like rash/pustular genital rashes. In such cases, screening for other STIs, wound swabs, and topical/systemic antibiotics for secondary bacterial infections in suspicious lesions, and follow-up if necessary are advised. Advise self-isolation and sexual abstinence for around 3 weeks until the scabs fall off, and in immunocompromised individuals, consider starting tecovirimat. Health education that the disease can spread despite the use of barrier protection, such as condoms and vaccination for high-risk populations, such as men who have sex with men and sex workers, may help curb the infection in the future. Based on our study, we recommend adding MPOX to the list of STIs presenting with genital ulcers or urethritis.
Supplemental Material
Supplemental Material - ‘Monkeypox 2.0’: Case series on a reconditioned virus causing sexually transmissible disease in urban population
Supplemental Material for ‘Monkeypox 2.0’: Case series on a reconditioned virus causing sexually transmissible disease in urban population by aheersha Pakran, Amal Mohammed Alsaberi, Amani al Falasi, Tarek Mohamed Karam Husein Ibrahim, Amel Abdalla Eisa Fadl Alnuaimi, Srikumar Goturu, Muneer Mohamed, Reena Mary Abraham, Vidya Lakshmi Sundaramurthi, Aneesh Kunnath Parambath, Beena Jose, Divya Kamat, Thencheri Cheriath Satish, Juwariya Tasneem Syeda, Lubna Gul
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.