
Abstract
Treatment options for recalcitrant Trichomonas vaginalis (TV), when very high dose systemic 5-nitroimidazole plus intravaginal therapy for over 14 days has failed, are very limited. They have poor efficacy, unpleasant side effects, and are difficult and expensive to acquire. We report successful treatment with 24 weeks of daily dequalinium chloride vaginal tablets. Dequalinium is licensed in Europe where it is readily available and cheap. It offers a safe and pragmatic alternative for recalcitrant TV.
Introduction
Trichomonas vaginalis, a sexually transmitted parasitic protozoan, can cause symptoms of purulent vaginal discharge and vulvovaginal pruritis. The main treatment is systemic 5-nitroimidazoles (metronidazole or tinidazole). Resistance to these drugs has been observed. In such cases, or where they are contraindicated, options are limited. Some alternatives in the UK guideline, based on anecdotal evidence, 1 can be difficult and expensive to obtain due to licensing restrictions. The European guideline does not name alternatives due to lack of evidence. 2
Case report
An 18-year old white British female presented to her General Practitioner (GP) with vulval irritation and vaginal discharge. She had a regular male partner of 3 years who travelled between the UK and Dubai.
Her GP diagnosed TV and treated her with metronidazole 400 mg twice daily for 7 days. Within 3-month, she reattended with recurrent symptoms. Trichomonas vaginalis nucleic acid amplification test (NAAT) was positive, so she was referred to Leeds Sexual Health.
Treatments, duration, clinical and microbiological response.
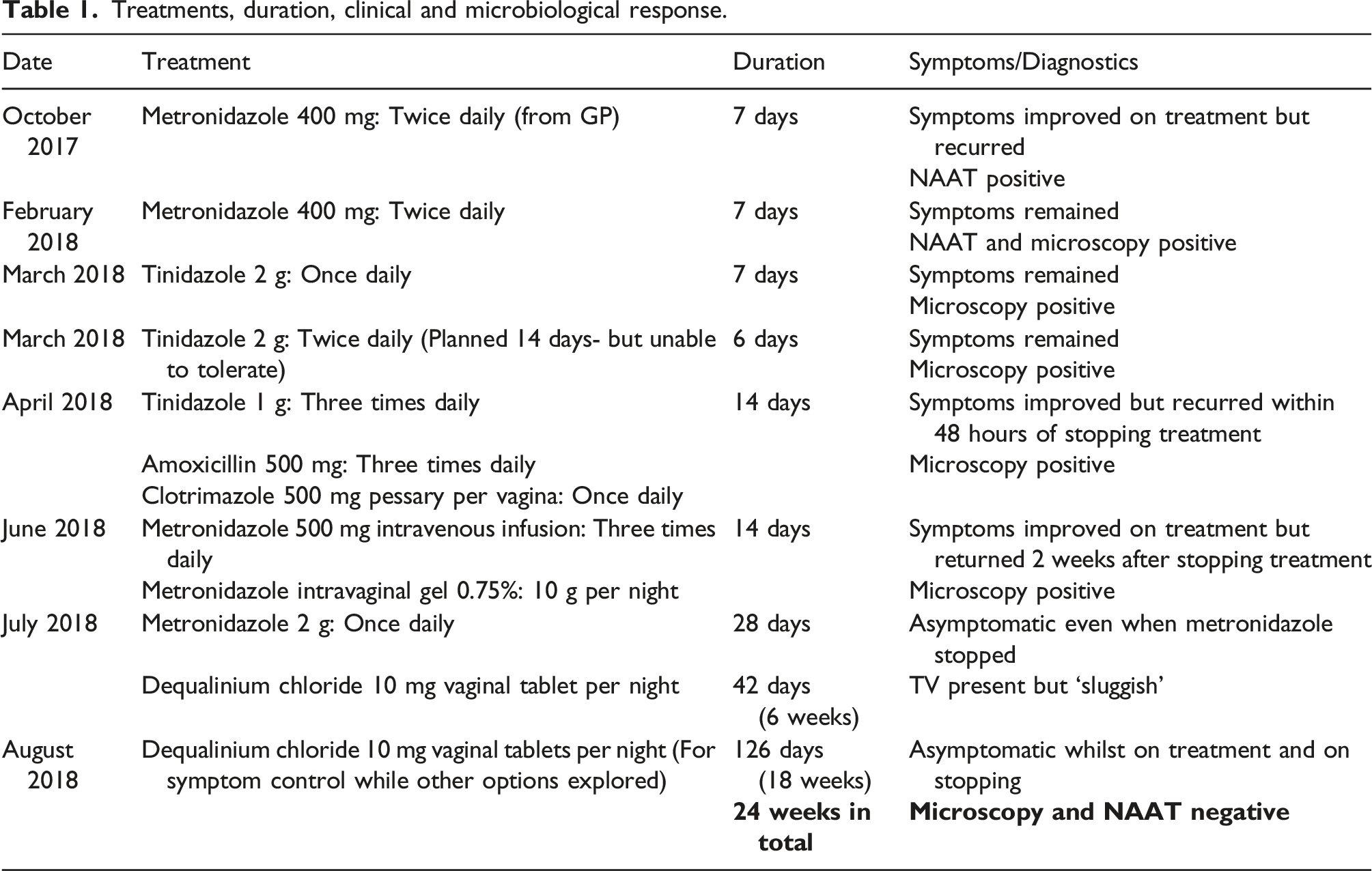
She had difficulty completing some oral courses due to side-effects, so intravenous metronidazole was given for 14 days to ensure adequate systemic levels were achieved but this also failed to clear the infection. TV resistance testing is unavailable in the UK, so the presumed resistance was unconfirmed microbiologically.
Following discussion amongst senior doctors, dequalinium chloride 10 mg vaginal tablets daily were suggested as an adjunct to further oral metronidazole for 4 weeks. Dequalinium was used daily for 6 weeks and at completion, ‘sluggish’ TV were still visible on microscopy, but her symptoms remained controlled by dequalinium alone, with no reported side effects. Daily dequalinium was continued for symptomatic relief pending alternative treatment options which needed to be imported from outside the UK. Having continued dequalinium monotherapy for a further 18 weeks (i.e., 24 weeks in total) she remained symptom free and microscopy and TV NAAT were negative. To ensure the infection really had cleared, the dequalinium was continued for a further 4 weeks and repeat microscopy and TV NAAT remained negative so it was stopped. She was still asymptomatic 4 weeks after stopping treatment and TV NAAT was negative.
Discussion
Current treatment options of recalcitrant TV, when very high dose systemic 5-nitroimidazole plus intravaginal therapy has failed, are very limited. 3 Case reports of successful treatment with intravaginal paromomycin, furazolidone, acetarsol pessaries or 6% nonoxynol–9 pessaries have been reported but these preparations are difficult and expensive to obtain in the UK. Also, their side effects can be very unpleasant. Monotherapy with intravaginal boric acid pessaries for 1 to 5 months has cleared TV in two women. 4 Boric acid is described as well tolerated but is also difficult and expensive to import into the UK.
Dequalinium chloride is a quaternary ammonium compound that is licensed in Europe for treatment of bacterial vaginosis. It increases permeability of cell walls and impairs enzyme activity, resulting in cell death.5,6 It has activity against many bacteria, fungi and protozoa, and no resistance has been reported in laboratory or clinical studies. It is well tolerated with few side effects.
Several small studies have shown in-vivo efficacy of dequalinium against TV. 6 The average treatment lasted 6-week with cure rates of 17%–50%. 6 Vaginal treatments inevitably have lower cure rates than oral treatments as TV also infects the urethra and peri-urethral glands. 7 A 6-weeks course, with 4-week of high-dose oral metronidazole, was chosen using this evidence. Clearly 6-week dequalinium was inadequate for TV clearance in this case but by prolonging the course to 24 weeks, for symptomatic relief pending an alternative treatment, we were able to clear the infection. Dequalinium is easy to acquire in Europe. It offers a safe, pragmatic and relatively cheap alternative to current recommended treatments.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: State: Dr Janet Wilson is the Chief Investigator of an NIHR funded trial ‘Dequalinium versus usual care antibiotics for the treatment of bacterial vaginosis (DEVA): a multicentre, randomised, open label, non-inferiority trial’.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.