
Abstract
Background
HIV-related stigma, discrimination, and social marginalization undermines optimal HIV care outcomes. More research examining the impact of HIV-related stigma, discrimination, other interlocking forms of oppression, and antiretroviral therapy (ART) adherence is needed to optimize HIV treatment programming. This study uses data from two clinics in the Dominican Republic to examine client and healthcare worker (HCW) perceptions of HIV and intersectional stigmas among people living with HIV.
Methods
Surveys exploring demographics, HIV-related stigma, various dimensions of discrimination (race/ethnicity, HIV status, sexual orientation), healthcare engagement, and medication adherence were collected from 148 clients and 131 HCWs. Analysis of variance was conducted to examine differences in stigma by clinic and logistic regressions were used to determine predictors of optimal client medication adherence.
Results
Perceived discrimination in healthcare facilities due to clients’ sexual orientation retained significance in crude and multivariable logistic regression models and was negatively associated with ART adherence (aOR:0.79; 95% CI:0.66, 0.95).
Discussion
Findings highlight the importance of implementing strategies to address stigma, discrimination, and social marginalization, particularly within healthcare facilities.
Background
The advent of active antiretroviral therapy (ART) and evolution of increasingly effective medication regimens has promise for reducing mortality for people living with HIV, fostering prevention for those at elevated risk, and curbing the global HIV epidemic.1–3 Despite these advances, various social factors undermine the public health community’s ability to optimize biomedical intervention strategies that could significantly reduce HIV threat. Among these factors, HIV-related stigma (a process wherein a person is socially discredited 4 due to their HIV status through labeling, stereotyping, status loss, and discrimination by a dominant force) 5 is a priority barrier to reaching UNAIDS 95-95-95 (diagnosis of 95% of all people living with HIV, ART initiation for 95% of people diagnosed with HIV, and viral suppression among 95% of people living with HIV who are receiving treatment) goals. 6 The stigma of HIV undermines all facets of the HIV care continuum7–10 and experiencing stigma increases the risk of having an elevated viral load.11,12 Stigma also adversely impacts mental health for people living with HIV, which is in itself harmful and inhibits medication adherence and subsequent viral suppression.7,9,13 Thus, reducing HIV incidence, reducing HIV mortality, and enhancing the quality of life for people living with HIV may depend greatly on reducing HIV-related and other intersectional forms of stigma.
Stigma is exceptionally pernicious when it stems from actors within the healthcare sector. 14 Stigmatizing actions reported by people living with HIV in healthcare settings include HIV status disclosure and privacy violations by healthcare professionals, assumptions of moral degeneracy, undermined autonomy in health decision-making, and unreasonable fear of HIV transmission that manifests as othering behavior (e.g. double gloving) and poor healthcare delivery (i.e. distancing from client, treatment refusal).15,16 Consequently, clients reporting stigma in healthcare settings are less likely to remain engaged in HIV care, adhere to ART, or obtain and maintain viral suppression.15,17,18 HIV-related stigma in health facilities can also impact the quality of care provided to clients. 19 These phenomena are concerning given the importance of consistent HIV continuum of care participation in accessing appropriate ART regimens, monitoring HIV disease, addressing comorbidities, and optimizing prevention. Clearly, understanding and addressing HIV-related stigma in healthcare settings is critical for meaningfully addressing HIV.
Beyond HIV-related stigma, people living with HIV can experience stigma and social marginalization related to other identity characteristics such as race, gender, or sexual orientation.20,21 This concept, intersectional stigma, provides a framework for examining how interlocking systems of oppression (i.e., racism, sexism, transphobia, heterosexism) shape experiences of people with intersecting, marginalized identities.22,23 For sexual and gender minorities living with HIV, this may be a particularly pronounced impediment to optimized care use and engagement. For example, both HIV-related stigma and homophobia are associated with inhibited continuum of care participation among men who have sex with men (MSM).24,25 Among African American gay men in the US, HIV-related stigma and homophobia have been linked to inhibited testing and medication adherence specifically. 26 These stigmas may interact in dynamic and complicated ways to reduce care uptake among people living with HIV and impair optimized care delivery by healthcare workers (HCWs).
Interlocking systems of oppression may be particularly deleterious in contexts such as the Dominican Republic. The country’s history of colonialism and development of group-based, skin color influenced social hierarchy fosters social marginalization.27,28 Anti-LGBT sentiment may be particularly challenging in the Dominican Republic. 29 In terms of sexual behavior stigma, research in the Dominican Republic has found that female sex workers living with HIV are more likely to experience harassment because of their HIV status compared to non-sex workers. 30 Further, the social and economic marginalization of migrants, (exclusion from political representation and citizenship rights [including birthright citizenship], access to education, access to tailored HIV prevention programming) represents a social stigma produced by power structures.30,31 This is particularly concerning as many migrants are from communities disproportionately affected by HIV.30,31 This socioenvironmental context may place people living with HIV at high vulnerability to stigma and adverse outcomes.
Understanding the impact of stigma on people living with HIV and care outcomes is crucial for directing stigma-reduction programming in healthcare settings. Thus, this study examines client and HCW perceptions of HIV and intersectional stigma and seeks to illuminate the impact of stigma, social marginalization, and various health care factors on client outcomes. To address this inquiry, this study employs the conceptual model for HIV and intersectional stigma developed by Turan and colleagues (2017), which is grounded in minority stress theory. 32 This framework posits that various forms of HIV-related stigma (enacted, perceived community, anticipated, internalized) and intersecting stigmas at the macro, meso, and micro levels can both directly and indirectly impact care engagement, mental health, and HIV care outcomes for people living with HIV. 32 For the current study, the investigators apply this framework to examine client and HCWs perceptions of the manifestations of HIV and other intersectional stigmas in two HIV care clinics in the Dominican Republic. In addition, we examined the associations of stigma, other forms of social marginalization, and psychosocial healthcare attitudes (i.e. client satisfaction, healthcare empowerment) on ART adherence among clients at these clinics.
Methods
This study uses wave one baseline survey data from the Finding Respect and Ending Stigma around HIV (FRESH) Study in the Dominican Republic. Details can be found elsewhere,33–35 but briefly FRESH is a program that employs workshops involving interpersonal contact between HCWs and clients to reduce HIV-related and intersectional stigma enacted by HCWs and internalized by their clients with HIV. This program has been implemented in multiple countries and settings33,34 and has most recently been adapted for use in the Dominican Republic, with a special focus on MSM and transgender women living with HIV.
Data for the current analyses were collected from two clinics in the Dominican Republic prior to introduction of the FRESH intervention. A convenience sample was recruited through study flyers and a clinic staff member who promoted the study through word-of-mouth. These baseline surveys were completed during the first wave of a four-step stepped wedge cluster randomized controlled trial, by HCWs (n = 131) and clients (n = 148) in 2021. Clients were eligible to participate if they were (1) 16 years of age or older, (2) living with HIV, (3) in established HIV primary care at one of the two clinics, and (4) able and willing to provide informed consent. Clients were excluded if they had a cognitive or developmental impairment that limited their ability to provide informed consent. HCWs were included if they were (1) currently employed at one of the participating HIV clinics in a role that included four or more weekly hours of client contact, and (2) able and willing to provide informed consent. Participants were compensated a $10 USD equivalent grocery store voucher for survey completion. Study approval was provided by the Institutional Review Boards of Universidad Iberoamericana (UNIBE, CEI2020-32), University of Alabama at Birmingham (IRB-300005657), and Florida State University (STUDY00003459).
Measures
Demographics
Sociodemographic variables for client and HCW surveys included age, race, gender, sexual orientation, education, religion, religiosity, and migrant status. Variables were selected based on previous theoretical and empirical associations with ART adherence and HIV vulnerability.36–43 Prior exposure to clinic-based anti-stigma programming was also assessed. Clients were exclusively asked about sex work involvement and years living with HIV. HCWs were exclusively asked about HIV status and their employment role in the clinic.
Stigma and other measures
Stigma and social marginalization measures for clients include, (1) Bogart, et al’s (2013) perceived discrimination scales due to HIV status (alpha = 0.84), race/ethnicity (alpha = 0.89), and sexual orientation (alpha = 0.86), 44 (higher scores indicate more discrimination) and (2) Wright et al’s (2007) HIV stigma scale (alpha = 0.71), which includes subscales related to enacted stigma experienced by people living with HIV (personalized stigma; alpha = 0.81), disclosure stigma (alpha = 0.64), concern with public attitudes (public stigma; alpha = 0.81), and internalized stigma (alpha = 0.84) with higher scores indicate more stigma. 45 Measures of healthcare attitudes for clients included the Healthcare Empowerment Inventory (alpha = 0.73) 46 (higher scores means greater healthcare empowerment) and a single item assessing satisfaction with healthcare (response options: [1] Very satisfied – [5] Very unsatisfied) that was dichotomized into “very satisfied” and “less than very satisfied.” Clients were also asked about prior experience with stigma reduction programming (yes/no).
Clients and HCWs also completed a measure of enacted stigma in healthcare settings in the past 3 months. 47 For clients, the assessment included perceived HCWs’ willingness to provide care, quality of care administered, and stigmatizing discourse by HCWs (alpha = 0.72) (higher scores indicating more stigma). HCWs were asked questions regarding stigma around delivery of healthcare services (observing stigma in delivering services) (alpha = .84) (higher scores indicate more stigma), experiences with secondary stigma among health facility staff (alpha = .42) (higher scores indicate more stigma), opinions about people living with HIV (moralizing about perceived behavior) (alpha = .67) (higher scores indicate more stigma), and willingness to provide services to marginalized groups (men who have sex with men, transgender individuals, sex workers, migrants) (alpha = .99) (higher scores indicate less willingness). 47
Medication adherence
The main outcome of interest for client surveys was ART medication adherence. Medication adherence was assessed using Wilson et al’s (2020) three-item measure of medication adherence. 48 Items were; 1) “In the last 30 days, on how many days did you miss at least one dose of any of your HIV medicines?” (response options range from 0 to 30); 2) “In the last 30 days, how often did you take your HIV medicines in the way you were supposed to?” (response options: six-point Likert between never to always); and 3) “In the last 30 days, how well did you comply with how to take your HIV medication?” (response options: six-point Likert between poor – excellent). Responses for items were linearly transformed to a 0–100 scale. Summary scores were calculated as a mean of the three items. As measures of ART adherence typically have a positive skew, responses were dichotomized as 0 = ≤99% adherence and 1 = >99% adherence.
Data analysis
Descriptive statistics were ascertained for all variables of interest. Analysis of variance (ANOVA) was conducted separately for clients and providers to examine differences in the study variables (i.e., stigma, discrimination, and empowerment) between clinics. Crude logistic regression was conducted to determine predictors of client ART adherence. For each predictor variable, a model adjusted for control variables (age, gender, and clinic) was employed (minimally adjusted model). A final multivariable logistic regression analysis included discrimination measures, control variables, and other variables significant at a p < 0.05 level in all previous models. The data were analyzed using STATA and SPSS (version 29).
Results
Demographics.
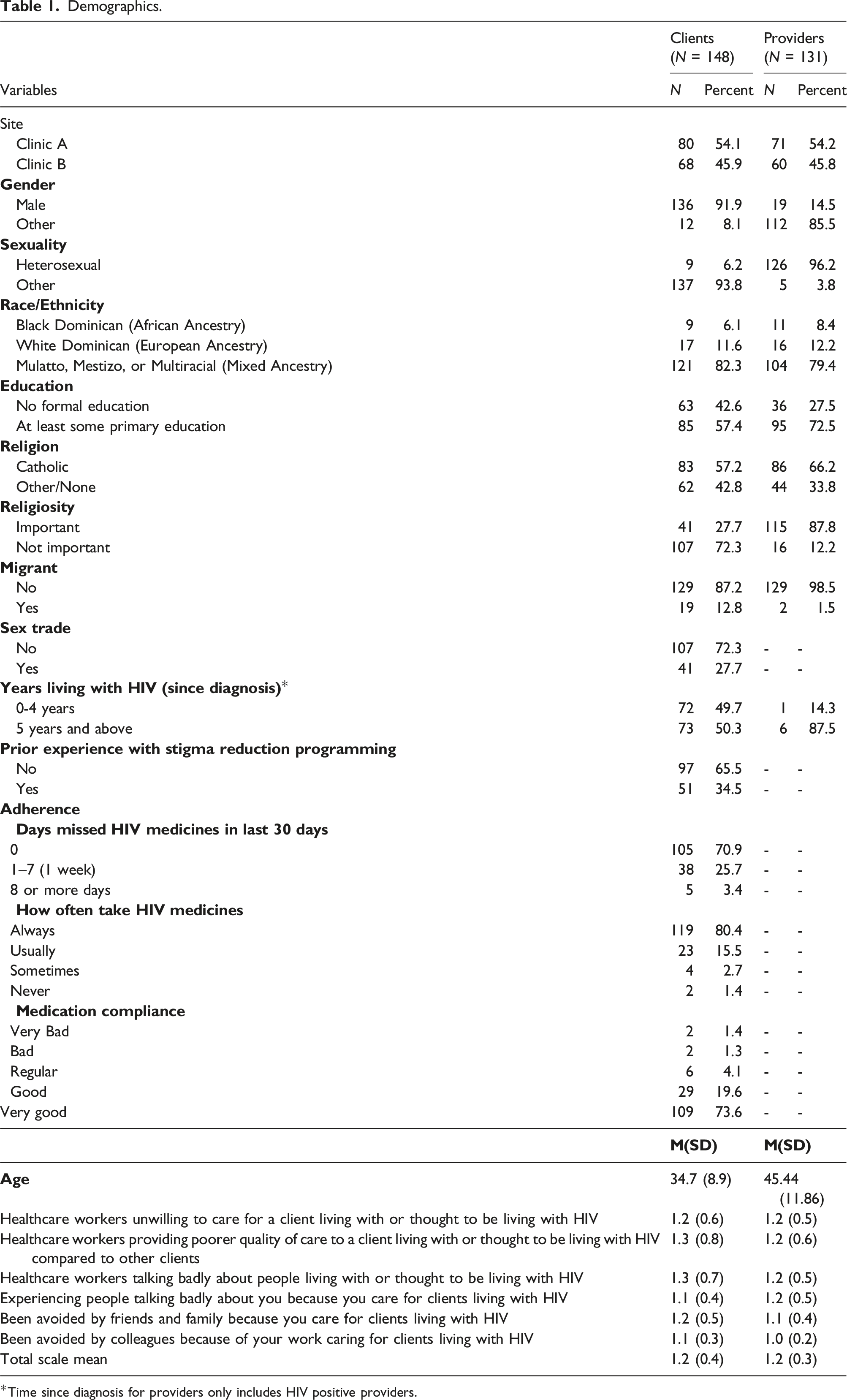
*Time since diagnosis for providers only includes HIV positive providers.
ANOVA – Differences in study variables by clinic.

Logistic Regression for associations with optimal ART adherence among PLWH.

*p
Discussion
This study examined perceptions of stigma and discrimination from the perspectives of clients and HCWs in two HIV clinics in the Dominican Republic. We also examined the impact of healthcare experiences, stigma, and social marginalization on ART adherence among clients. Although various factors, including clinic of care, length of diagnosis, experiencing sexual orientation discrimination, and healthcare empowerment were associated with client ART adherence in crude models, these effects eroded in the final multivariable model with only experiencing sexual orientation discrimination retaining a significant independent association with suboptimal ART adherence. Findings highlight the need for additional investigation to understand complex relationships between healthcare utilization, social marginalization, and ART adherence.
Clients reporting greater discrimination due to sexual orientation were less likely to be adherent to medication. These findings align with other research highlighting the impact of anti-LGBTQ animus on healthcare utilization and medication adherence.26,49 Social marginalization factors in general have been implicated in undermining medication adherence and this has often been mediated through mental health challenges (such as depression), diminished self-efficacy, and other obstacles (concern about inadvertent disclosure, maladaptive coping), that inhibit optimal HIV management.13,17,50,51 Clearly more work is needed to address social marginalization in the interest of improving HIV care outcomes. Efforts to improve resilience, self-efficacy, and discriminatory social environments are critical in this endeavor. However, the selection of approaches that are most effective and efficient in advancing these goals both within and outside of healthcare settings is less apparent. One potential approach for healthcare settings is the FRESH intervention, which uses interpersonal contact and empowerment approaches to reduce HIV-related and intersectional stigmas, and which our team is testing in the Dominican Republic with a focus on promoting health outcomes of sexual and gender minority persons living with HIV.34,35 Additionally, a total facility approach (an emphasis on multilevel interventions incorporating formative research, staff capacity-building and training, and modification of organizational processes) demonstrates potential for HIV-stigma reduction in healthcare facilities.52,53 Implementing and scaling these approaches has promise for more widespread delivery of less stigmatized care.
Clients reported differing stigma experiences between the two clinics. This indicates potential differences in the backgrounds and experiences of client populations that deserve further exploration. There were corresponding differences in stigma between clinic staff as well. Stigma within healthcare facilities is a considerable concern as it generally undermines medication adherence and viral suppression.15,49,54 Stigma perpetuated by HCWs may have more impact on health outcomes than stigma from other sources. 54 More training and incorporation into medical, nursing, and paraprofessional education is needed to address stigma and social marginalization in all types of clinic environments.
More intervention research is critical for developing, implementing, evaluating, and scaling strategies that address stigma. In order for this to occur, more funding should be allocated towards multilevel interventions (including among HCWs), researchers should partner with communities on intervention design, and more emphasis can be placed on implementation science. 55 These strategies may have beneficial returns in reducing intersectional stigma and improving outcomes.
This study has limitations. First, data are self-report and subject to social desirability bias. Second, participants were recruited through convenience sampling at specific clinics and results may not be generalizable. In line with this, collecting survey data in clinic settings may have resulted in under-reporting of suboptimal adherence. Data are also cross-sectional and causality cannot be established. Finally, findings represent experiences of clients who are in care and may not represent the experiences of those who have not been linked or maintained into care.
This study highlights the necessity of HIV and intersectional stigma-reduction strategies, particularly within healthcare facilities. Our results suggest that effective programs with a specific focus on reducing stigma in healthcare settings and reducing social marginalization for sexual and gender minorities in particular are needed to optimize medication adherence and realize subsequent benefits of viral suppression. Future studies should further explore the mechanisms by which stigma reduction programs may improve adherence and employ implementation science approaches to optimize their use.
Footnotes
Acknowledgements
We thank Katelin Adams, Ingrid Ruiz De León, and Analía Henríquez Cross for their early work supporting this project. We acknowledge the contributions of our intervention facilitators, data collectors, and community advocates: Dr Rosa Mayra Rodriguez-Lauzurique, Mr Elias Ramos, and Ms Nairovi Castillo. We also want to express our gratitude to our partner SGM community-based organizations in the Dominican Republic for all their support. Our team recognizes the valuable insights provided through their participation. We also acknowledge the political support and encouragement of the Servicio Nacional de Salud (SNS) authorities.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Mental Health; (K01MH119942, R21MH124083), Fogarty International Center; (R21TW011761).