
Abstract
Background
In the context of People Living with HIV (PLWH), poor health literacy (HL) seems to be linked to poorer health outcomes and reduced engagement in care. Additionally, the level of HL can affect HIV knowledge and may impact adherence to antiretroviral therapy (ART). This research explored the connection between ART adherence, HL, and engagement in care in a cohort of 250 PLWH receiving ART in Italy.
Methods
A questionnaire was given to PLWH at Policlinico Gemelli in Rome to assess their health literacy and adherence to therapy. The Brief Health Literacy Screening (BHLS) and the Newest Vital Sign (NVS) were used to evaluate subjective and objective HL. Adherence levels were self-reported as poor, good, or excellent, and the assessment included the Patient Health Engagement Scale (PHE-S).
Results
Notably, the majority of the sample comprised male individuals (67.9%), with 69.2% reporting a 10-years or longer duration between their HIV diagnosis and their initiation of ART. It was found that PLWH with poor adherence had low schooling, had been living with HIV for 1–5 years, were HCV co-infected, had a viremia >50 copies/mL, poor health status, poor engagement in care, and poor HL (p = <0.001). They exhibited lower mean scores on the subjective HL scale and lower CD4 T-cell counts and nadir CD4 T-cell counts (p < .001).
Conclusion
Our study demonstrated a positive correlation between higher HL levels and improved disease management, treatment adherence, and overall physical and mental well-being. Enhanced HL capabilities are paramount in bolstering health management and treatment adherence.
Introduction
Health literacy (HL) encompasses the capacity to comprehend and implement health-related information to adopt suitable health behaviors for physical and psychological well-being. 1 HL facilitates enhanced communication between healthcare providers and is integral to a patient-centered model of care. 2 The definition of HL comprises both objective and subjective dimensions. The objective dimension encompasses specific skills, including comprehending medical terminology and interpreting health information presented in numerical or graphical formats. 3 The subjective dimension pertains to the ability to self-assess competency and make informed decisions regarding personal health status. 4
HL is a pivotal consideration for patients battling chronic diseases, including People Living with HIV (PLWH), as research indicates a correlation between low HL and adverse health outcomes.5,6 In the context of PLWH, low HL may engender significant challenges, such as diminished self-esteem, difficulties in health management, 7 a sense of exclusion from the treatment process, 8 and frequent hospitalizations. 9 It is essential to develop HL skills among PLWH to maintain a high quality of life. 10 Patients with low levels of HL tend to struggle with using healthcare services and communicating with healthcare providers, which can result in low engagement with their care.11–14 On the other hand, patients with high levels of HL are more engaged with health service providers and can adopt positive health behaviors to prevent illness or manage their medical condition better.12,13,15
Encouraging PLWH to be actively involved in their care and knowledgeable about HIV is crucial for improving HIV management and ensuring adherence to antiretroviral therapy (ART).16–18 Studies have shown that HL level affects HIV knowledge and is linked to treatment adherence. 19 While some research has provided mixed results, a study by Rodkjaer et al. demonstrated a strong association between health literacy and adherence to antiretroviral therapy. 20 In a study conducted by Kalichman et al., 21 it was observed that fewer than half of the patients with low HL achieved an optimal level of therapeutic adherence. This inadequate adherence may lead to an increased susceptibility to therapeutic failure and the potential development of treatment-resistant strains. Conversely, both Wawrzyniak et al. and Colbert et al. found no significant association between health literacy and therapeutic adherence.22,23
Furthermore, Rebeiro et al. discovered that low HL was correlated with inadequate viral suppression, although not with suboptimal adherence to ART. 24 Current literature indicates that compromised cognitive performance, both overall and in specific domains, is associated with poorer adherence. 25 Specifically affected domains include information processing speed, verbal fluency, attention and working memory, learning, and executive functions.26,27 Adherence to ART stands as the most dependable predictor of achieving virologic suppression. 28 Inadequate adherence to ART correlates with virologic failure, heightened risk of HIV transmission, and diminished survival rates.29,30
In light of the available literature, it is evident that the correlation between HL and adherence to treatment in PLWH remains the subject of ongoing scrutiny, as numerous studies have presented conflicting findings. As such, our study sought to examine the nexus between adherence to ART, HL, and engagement in care within a cohort of PLWH in Italy.
Material and methods
Participants
In the period from January to February 2024, a total of 250 individuals diagnosed as people living with HIV (PLWH) were consecutively enrolled at the Infectious Disease Institute, Fondazione Policlinico Universitario A. Gemelli IRCCS in Rome. As part of their routine outpatient visits, these individuals were requested to complete a questionnaire after an explanation of the research’s purpose and objectives by the attending infectious disease physician. Exclusion criteria comprised individuals below 18 years of age and those encountering challenges in comprehending the Italian language. It is imperative to note that participation in this study was entirely voluntary, and no form of remuneration was provided. Furthermore, all procedures conducted were consistent with the ethical standards of both the institutional and national research committee, as well as in compliance with the 1964 Helsinki Declaration including its subsequent revisions or equivalent ethical benchmarks.
Procedure
Each participant completed a 21-item questionnaire, providing demographic and clinical data. This included age categories (24–45, 46–60, >60 years), levels of education (lower secondary school, upper secondary school, bachelor’s degree), employment status (unemployed, employed, retired), duration since HIV diagnosis (<5 years, 5–10 years, >10 years), time elapsed since commencing the initial ART regimen (<5 years, 5–10 years, >10 years), awareness of personal viremia (yes or no), HIV-RNA <50 copies/mL (yes or no), CD4 T-cell counts, nadir CD4 T-cell counts, and self-assessment of health status (i.e., poor, good, excellent). Additionally, patients were requested to assess their own adherence to therapy over the preceding month. They were required to specify whether, in their judgment, their adherence had been poor, good, or excellent. Based on a post-hoc power analysis conducted in G-Power (for one-sample Wilcoxon signed-rank test, 0.05 significance level, a sample size of 250, a small effect size (d = 0.2), and two tails), the power achieved is adequate (0.86).
HL measure
Two instruments were employed to assess health literacy (HL): the Brief Health Literacy Screening (BHLS) and the Newest Vital Sign (NVS). The validated three-item BHLS is a self-report questionnaire designed to evaluate subjective HL. It encompasses three domains: understanding one’s medical condition through written information, proficiency with medical forms, and reliance on others to comprehend hospital materials. Within each domain, respondents are presented with a selection of five responses, varying from “never” to “always” (never, occasionally, sometimes, often, always). The questions are: “How often do you have someone (like a family member, friend, hospital/clinic worker or caregiver) help you read hospital materials?”; “How often do you have problems learning about your medical condition because of difficulty understanding written information?”; and “How confident are you filling out forms by yourself?”. In order to administer it to our PLWH, the questions were translated into Italian. 31 In each domain, the subject has the potential to achieve a score ranging from 1 to 5, which is subsequently aggregated across all areas to yield a comprehensive score between 3 and 5. A higher cumulative score is indicative of superior health literacy. 32
The Newest Vital Sign (NVS) is a performance-based assessment of HL, gauging patients’ capacity to read and comprehend health-related information and apply it to varying scenarios. The abbreviated form, derived from a larger 21-item test, comprises 6 items designed to evaluate the aptitude to interpret, comprehend, and utilize data gleaned from an ice cream label. Each accurate response garners 1 point, while erroneous answers yield 0 points, resulting in a total score ranging from 0 to 6. 33 The NVS evaluates pivotal elements of HL, encompassing literacy and numeracy competencies. 34 In our case, the Italian rendition of the NVS, validated by Capecchi from the English version, was deployed to assess our patients. 35
Health engagement measure
The Italian iteration of the Patient Health Engagement Scale (PHE-S) was employed to evaluate the level of engagement exhibited by patients in managing their medical condition. The Patient Health Engagement Scale PHE-S is designed to be on the principles articulated in the Patient Health Engagement Model (PHE-Model). The stages encompassed in the PHE-Model are blackout, arousal, adhesion, and eudaimonic project. During the blackout phase, patients experience a state of physical and psychological vulnerability. In the arousal phase, patients begin to acquaint themselves with their health condition, albeit their comprehension of the disease remains superficial. In the adhesion phase, patients are no longer in a state of physical and psychological vulnerability, yet they have not achieved autonomy in dealing with health issues. Finally, in the eudaimonic project phase, patients comprehend and accept their illness and can attain a satisfactory quality of life. 36
The Patient Health Engagement Scale (PHE-S) is comprised of 5 ordinal items, each featuring 7 potential responses: 4 of which reflect distinct engagement positions, while 3 represent intermediate responses between engagement positions. The intermediate responses serve to facilitate the emotional expression of patients and prevent responses based solely on social expectations. Opting for an intermediate response is deemed to correspond to the preceding engagement position. The sum of the scores for each chosen response is calculated, and the median score is determined to ascertain the patient’s engagement position. A median score of 1 corresponds to the blackout position, 2 to arousal, 3 to adhesion, and 4 to the eudaimonic project. 37 Patients with low PHE levels are positioned within the blackout and arousal stages, while those with high PHE levels are in the adhesion and eudaimonic project stages.38,39
Statistical analysis
Descriptive statistical analysis was employed to summarize the sociodemographic characteristics and HIV-related clinical variables of the study population. Qualitative variables were presented as absolute frequencies and percentages, while quantitative variables were described using median and interquartile ranges (IQR) or means and standard deviations (SD). Subsequently, the Kolmogorov-Smirnov test was utilized to assess the normality of the data distribution. Given the non-normal distribution, the nonparametric Kruskal-Wallis test was applied to compare the mean values obtained on the BHLS scale, CD4 cell count, and CD4 cell count nadir in adherence to ART. Furthermore, the Chi-square test was utilized to compare the varied frequencies of adherence to ART and PHE positions with the NVS scale, demographic, and clinical-HIV-related variables. Statistical significance was set at a two-tailed p-value of <0.05. All analyses were performed using the SPSS version 21.0 software package (SPSS Inc., Chicago, IL).
Results
Demographic and clinical characteristics
We conducted a study involving 250 PLWH who were receiving ART. Among the participants, the majority were male (67.6%, n = 169), aged between 46 and 60 years (42.0%, n = 105), possessed an upper secondary school degree (50.0%, n = 125), and were employed (61.6%, n = 154).
Additionally, 173 (69.2%) PLWH had received an HIV diagnosis over 10 years prior, while 64.0% (n = 160) had initiated ART therapy more than 10 years before. Moreover, 92.8% (n = 231) reported HIV-RNA levels lower than 50 copies/mL, and 86.8% (n = 217) did not exhibit co-infection with the hepatitis C virus.
Demographic and clinical characteristics of People Living with HIV (n = 250).
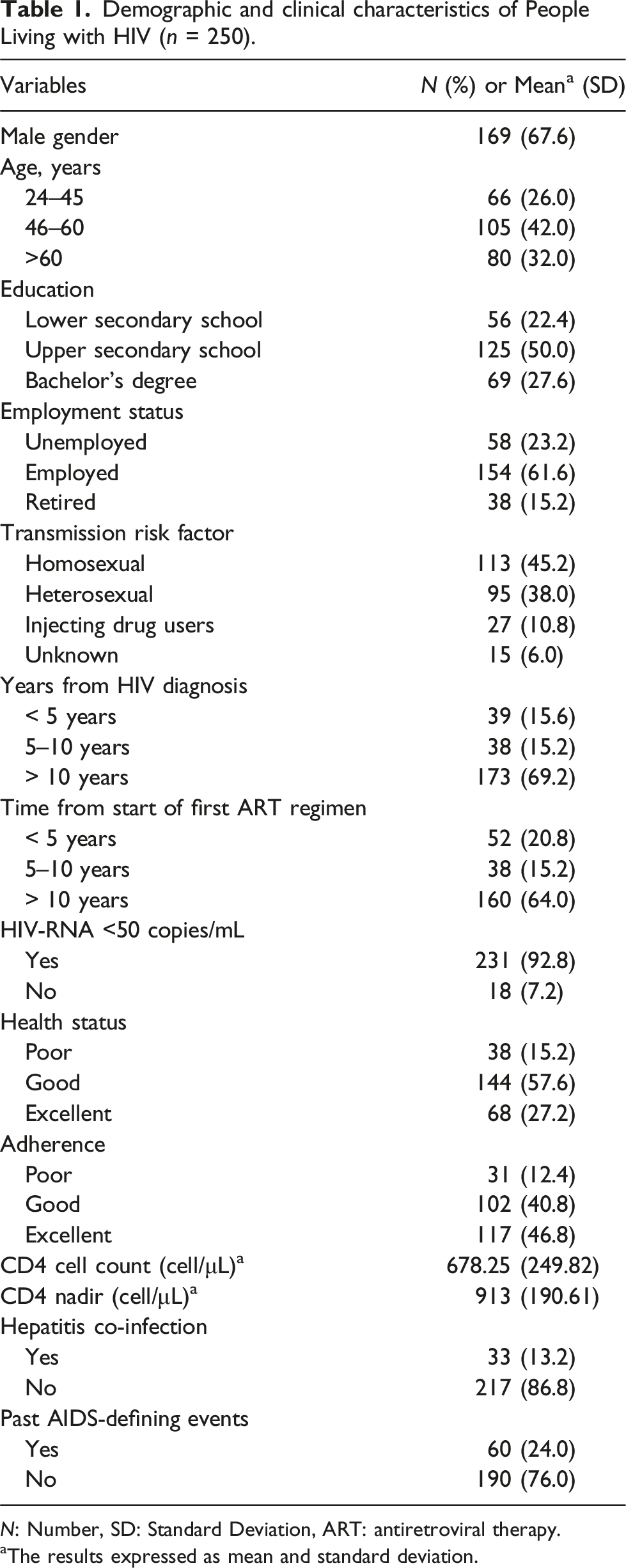
N: Number, SD: Standard Deviation, ART: antiretroviral therapy.
aThe results expressed as mean and standard deviation.
Adherence evaluation
Most PLWH with poor adherence had low schooling [p = <0.001; 38.7% (n = 12/31)] compared with those with good adherence (25.5%; n = 26/102) and those with excellent adherence (15.4%; n = 18/117) who have higher levels of schooling. A good part of the participants with poor adherence had been living with HIV for 1–5 years [p = <0.001; 32.3% (n = 10/31)] compared with those with good adherence (8.8%; n = 9/102) and those with excellent adherence (17.1%; n = 20/117), who had been diagnosed with HIV for more than 10 years. A large proportion of PLWH without HCV co-infection had excellent adherence [p = <0.001; 53% (n = 115/217)], compared to almost all HCV co-infected PLWH with poor adherence (91%, n = 30/33). In addition, nearly all participants with a viral load of >50 copies/mL exhibited poor adherence [p = <0.001; 88.9%, (n = 16/18)], in contrast to the majority of PLWH with a viral load of <50 copies/mL who demonstrated good adherence (80%, n = 185/231). The study revealed that most participants with poor treatment adherence also reported poor health status [p = <0.001; 90.3%, (n = 28/31)], while the majority of PLWH with good adherence reported excellent health status (80%, n = 82/102). Moreover, a significant number of PLWH with poor adherence reported low objective HL [p = <0.001; 41.9%, (n = 13/31)] compared to the majority of participants with excellent adherence who reported optimal objective HL (70%, n = 82/117).
PLWH with excellent adherence scored higher on the subjective HL than those demonstrating good and poor adherence [p = <0.001; 170.26 versus 101.95 versus 34.06, respectively], indicating notable differences. Additionally, participants with excellent adherence displayed higher mean CD4 T-cell counts than those with good and poor adherence [p = .065 - significant trend - 117.44 VS 129.66 VS 96.43]. Furthermore, PLWH with excellent adherence exhibited an elevated mean nadir CD4 T-cell count compared to those with good and poor adherence [p = .019; 136.23 VS 110.56 VS 110.98].
Health engagement evaluation
People Living with HIV in the four positions of the engagement model (n = 250).

N: Number.
In the last phase of the PHE model, most of the participants were 60 years old [p = .002; 41.3%, (n = 19/46)], while in the arousal phase, 60% (n = 30/50) of the participants were between 25 and 45 years old.
In addition, the adherence phase of the model was characterized by the presence of employed patients [p = <0.001; 68.4% (n = 93/136)] compared to the blackout phase in which only unemployed patients were distributed (100%, n = 18/18). Furthermore, the adherence phase included PLWH who had been living with HIV for more than 10 years [p = .003; 71.3% (n = 97/136)], compared to the arousal phase in which half of the participants were diagnosed less than 5 years (50%, n = 25/50). Moreover, PLWH with undetectable viremia were concentrated in the adherence phase [p = <0.001; 97.8% (n = 133/136) compared to almost all PLWH with detectable viremia who were focused on the blackout phase (90%, n = 16/18). Finally, in the adherence phase, more than half of the participants reported good health status [p = <0.001; 65.4%, (n = 89/136)] compared to more than half of the PLWH with poor health status in the arousal phase (65%, n = 33/50).
A high percentage of PLWH in the blackout phase had been on therapy for less than 5 years [p = <0.001; 72.2%, (n = 13/18)] compared to those on treatment for more than 10 years who were more present in the last phase of the model (65%, 30/46).
Most patients in the lowest phase of the engagement pattern had poor adherence [p = <0.001; 66.7% (n = 12/18)], compared to those with poor adherence in the second phase (32.0%, n = 16/50), those with poor adherence in the third phase (2.2%, n = 3/136), and those with poor adherence in the phase with higher engagement of the pattern (0%, n = 0/46).
Discussion
Our research explores the correlation between adherence to ART, HL, and engagement in care within the context of PLWH undergoing ART treatment in an Italian medical facility.
Our results showed that our patients with poor adherence have the following socio-demographic and clinical characteristics: low schooling, fewer years living with HIV, HCV co-infected, with a viremia >50 copies/mL, with poor health status and the lowest mean CD4 and nadir CD4. Furthermore, it was found that patients with poor objective and subjective HL were in the early phase of the PHE model, the phase of low therapeutic involvement and maximum physical and psychological vulnerability.
Based on our findings, Kordwski’s study concludes that performance on the objective HL scale significantly predicts plasma viral load, the ability to self-manage treatment, and the quality of the relationship established with healthcare providers. 40 The NVS evaluates numerical skills, which are essential for medication management and consequently, for maintaining optimal medication adherence. 41 The capacity to adhere to prescribed therapy is closely linked to viral load. 42 Even minimal levels of subjective health literacy show a significant correlation with the inability to achieve sustained viral suppression. Importantly, enhancing the subjective HL score is shown to increase patients’ likelihood of achieving sustainable viral suppression, particularly among people living with HIV over the age of 50. 43
In the work of Rivero-Méndez et al., it was discovered that individuals living with HIV (PLWH) with low HL often exhibited lower levels of education, poor adherence to ART, and inadequate understanding of key HIV-related health concepts such as CD4 + T cell count and viral load. 44 This lack of comprehension was particularly notable among PLWH who were recently diagnosed or had limited experience in managing their health and HIV-related symptoms as compared to those with extensive experience.
Similarly, Dear et al. observed that patients who were recently diagnosed and younger were more inclined to miss regular clinic visits, exhibit suboptimal treatment adherence, and experience challenges in achieving viral suppression. 45 This underscores the imperative for the provision of patient-centered care services tailored to individual needs. 45
In the realm of HIV care, healthcare professionals often underestimate the low HL levels of their patients. 46 As highlighted by Ohl et al., 47 healthcare workers may misidentify more than half of PLWH with low HL as having adequate HL. 48 However, it is paramount for individuals with chronic ailments to possess adequate HL for successful self-management. 49 Those with low HL are more susceptible to adverse health outcomes due to difficulties in disease management and accessing vital support from healthcare and social services. 50
In a study conducted by Shuper et al., it was emphasized that individuals with HIV and HCV co-infection may encounter additional obstacles in adhering to ART compared to those with HIV infection alone. The authors highlighted that while co-infected patients may face challenges, optimal adherence levels are attainable if behavioral barriers related to adherence, such as the adoption of consistent health management behaviors, are effectively addressed. 51
We have identified a correlation between low levels of HL and suboptimal engagement in care. Specifically, PLWH in the blackout phase, characterized by being the most passive phase of psychological vulnerability, exhibited lower subjective and objective HL compared to PLWH in other phases. Prior data substantiate the association between HL and patient engagement, accentuating the necessity for interventions aimed at enhancing patients’ HL skills, encompassing their capacity to utilize and disseminate health-related information for informed decision-making.52,53 Additionally, other studies propose that refining patients’ comprehension of information may be achievable through the simplification of medical materials or the dissemination of strictly essential information only. 54 These interventions stand as pivotal measures not solely for augmenting patients’ HL, but also for fostering their participation in their healthcare journey. 55 Mitigating barriers linked to HL holds the potential to afford patients increased access to information and heightened engagement in their care. 56
Our patients with a high level of engagement were 60 years old, employed, living with HIV, and undergoing treatment for more than 10 years, with undetectable viremia and excellent self-reported health and adhesion. These findings are consistent with our previous study, wherein we observed that many PLWH were in the adhesion phase of the PHE Model. Moreover, individuals with a high level of engagement in eudaimonic projects exhibited better physical health status than those in the lower phase. 57 The results underscore the significance of engagement in eudaimonic activities for enhancing the physical well-being of people living with HIV. We also found that low CD4 count, high viremia, AIDS events, and early ART failure could result in disengagement from the course of treatment. 58
Our study findings demonstrate a positive correlation between higher HL and enhanced disease management, treatment adherence, and overall physical and mental well-being. Elevating HL levels has the potential to significantly improve health management and treatment adherence. In the context of ART adherence, it is notable that adherence is influenced by and influences various contributing factors, including stigma, challenges associated with HIV status disclosure, limited familial and social support, coexisting medical conditions, suboptimal engagement in care, and obstacles related to medication adherence.59,60 Consequently, it is imperative to establish consistent and comprehensive social support structures for these patient populations. Furthermore, healthcare providers must diligently assess and leverage the available resources and support systems to aid patients in effectively managing their condition. By fostering the development of appropriate coping strategies, healthcare professionals can facilitate improved pharmaceutical adherence among patients. 61
It is important to note the following points from our study. Firstly, the cross-sectional nature of our study renders it vulnerable to interference from uncontrolled biases inherent in routine clinical practice. Therefore, longitudinal studies will be necessary to validate the emerging data and to monitor changes in the relationship among adherence, HL, and engagement in care. Secondly, future research endeavors should incorporate a control group of patients with other chronic diseases to investigate potential variances from those living with HIV. Thirdly, it is imperative to involve physicians in forthcoming investigations to obtain their insights regarding patients’ HL and level of engagement in care.
In summary, our findings, which reveal a correlation between adherence, low subjective and objective HL, and inadequate care engagement, can be instrumental in devising interventions aimed at enhancing these proficiencies.
The introduction of ART has fundamentally altered the management of HIV, shifting it from a life-threatening condition to a manageable chronic ailment. 62 Adherence to ART yields a reduction in a patient’s viral load, effectively curbing viral replication, mitigating the risk of treatment failure and the emergence of drug-resistant viral strains, and preventing further transmission of HIV to uninfected individuals.63,64 Notwithstanding, impediments to optimal ART adherence may arise from various factors encompassing healthcare provider-related concerns, stigma, fear of disclosure, as well as mental health, interpersonal, and cognitive barriers. 65 Limited HL, signifying a lack of comprehension regarding HIV and its management, as well as the beneficial impact of ART, serves as a barrier to adhering to prescribed treatment regimens. Enhancing HL can dismantle social obstacles that deter self-care, including internalized stigma experienced by PLWH upon disclosing their illness,66,67 thereby fostering a willingness to seek external support. 68 By addressing HL, potentially through collaborative efforts between physicians and psychologists, it is plausible to alleviate the negative emotions experienced by PLWH and guide them in utilizing healthcare services effectively, thereby enabling them to access the requisite support they necessitate.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Footnotes
Acknowledgements
We thank VA and DPRC for their advice during the drafting of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.