
Abstract
Syphilis, known for its capacity to mimic various diseases, has seen rising incidence, particularly in adolescents, men who have sex with men (MSM), and individuals with HIV. Palmoplantar keratoderma (PPK), a rare manifestation of secondary syphilis, poses diagnostic challenges due to its resemblance to other conditions. We report the case of a 42-year-old man living with HIV presenting with acquired PPK, characterized by hyperkeratotic plaques on the palms and soles, alongside syphilitic roseola. Histopathology confirmed psoriasiform dermatitis with spirochetes. The patient received weekly intramuscular benzathine penicillin G, leading to significant clinical improvement without relapse. This case underscores the importance of recognizing atypical infectious presentations in individuals living with HIV and highlights the need for careful differential diagnosis in acquired PPK cases.
Introduction
Syphilis is known for its ability to mimic other diseases. Over the past decade its incidence has increased, particularly among adolescents, MSM, and individuals with HIV. 1
The earliest skin manifestations of secondary syphilis include well-defined, small erythematous, brown, or hyperpigmented macules.1,2 Atypical presentations may mimic tinea, psoriasis, impetigo, vasculitis, lupus vulgaris, or lichen planus. Palmoplantar keratoderma (PPK) is a rare occurrence in secondary syphilis. 2
Discerning between keratodermic presentations is clinically challenging and often requires histopathology for accurate diagnosis. 3 PPKs represent a heterogeneous group with overlapping clinical features. Differential diagnoses include hereditary PPK, keratoderma climactericum, and paraneoplastic syndromes (e.g., Sézary, Bazex, and hereditary Howel-Evans syndromes). Conditions such as verruciform epidermodysplasia, psoriasis, keratoderma blennorrhagica, pityriasis rubra pilaris, atopic or chronic hand dermatitis, lichen planus, and lupus erythematosus can mimic PPK. Infectious causes like HPV, syphilis, scabies, trichophytosis, leprosy, and tuberculosis should also be considered. PPK can arise from drugs (e.g., beta-glucans, lithium, chemotherapeutics), chemicals (arsenic, chlorinated hydrocarbons), malnutrition, pregnancy, menopause, or hypothyroidism.4,5
We present a case of acquired PPK, highlighting the importance of recognizing atypical infectious disease presentations in HIV-positive individuals.
Case report
A 42-year-old male with a history of cerebellar stroke and basilar artery dissection in 2020, along with chronic use of alcohol, marijuana, and cocaine, presented with a month-long history of moderate headache and altered mental status. Upon referral to the Infectology Clinic, HIV infection was confirmed through a positive ELISA test. At the time of diagnosis, the patient had a viral load of 90,000 copies and a CD4 count of 14 cells/mm3. He was hospitalized for treatment, and our service was consulted for a disseminated dermatosis. Examination revealed hyperkeratotic plaques with perilesional erythema on the palms and soles. (Figure 1(a) and (c)). A second dermatosis was noted on the extremities and trunk, characterized by confluent pink macules and scratch marks (Figure 1(e)). A presumptive diagnosis of acquired keratoderma (secondary syphilis vs verruciform epidermodysplasia) was made, while syphilitic roseola was suspected for the second dermatosis. The VDRL test was positive with a titer of 1:32, and punch biopsies were taken from the palms, soles, and anterior trunk. (a)–(d). Palmoplantar keratoderma before and after treatment. B (e)-(f). Syphilitic roseola before and after 3 weeks after treatment.
Histopathology of the palms and soles revealed psoriasiform dermatitis with spirochetes highlighted by Warthin-Starry stain (Figure 2). The anterior trunk biopsy showed papillary and reticular dermal edema with superficial perivascular lymphoplasmacytic infiltrate. These findings confirmed diagnoses of acquired PPK secondary to syphilis and syphilitic roseola. The patient began a weekly regimen of 2.4 million units of IM benzathine penicillin G for 3 weeks, along with topical 30% urea for the palms and soles. After 3 weeks, both skin conditions significantly improved. (Figure 1(b), (d) and (f)). He then started triple antiretroviral therapy (ART) with a daily regimen of bictegravir/emtricitabine/tenofovir (50/200/25 mg). Punch biopsy of the left sole with Warthin-Starry stain showing the presence of spirochetes.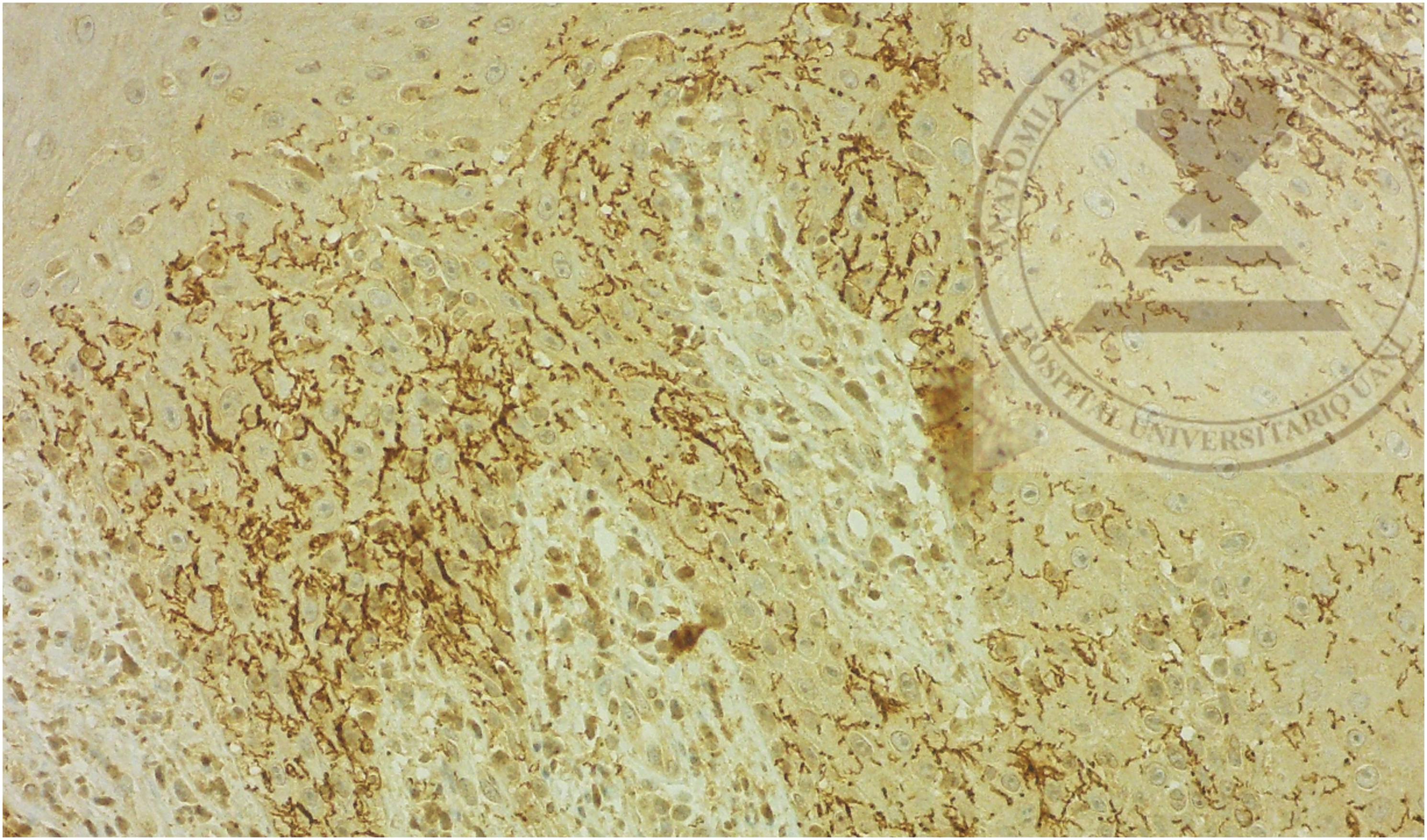
Discussion
Three primary categories of palmoplantar keratoderma include: hereditary PPK, genodermatoses featuring PPK, and acquired PPK. Acquired PPK in adults pose a diagnostic challenge for dermatologists. The clinical distinction between different keratodermas is generally difficult, often requiring histopathology to achieve precise diagnosis. 3
Various factors contribute to acquired PPK, including chemical exposures, medications, nutritional deficiencies, hypothyroidism, and inflammatory dermatoses. 4 Differential diagnoses to consider include hereditary PPK, keratoderma climactericum in peri-menopausal women, infections, and paraneoplastic manifestations.
The patient had never been tested for HIV prior to our encounter and he had spent multiple years living in the streets due to substance abuse and reported a history of frequent sexual intercourse with multiple partners. Considering this background, an infectious etiology was suspected, however, he was unable to specify when he might have acquired HIV or syphilis. Infectious diseases represent the least frequent etiologies of acquired keratoderma, and secondary syphilis is an uncommon cause of this dermatological presentation.2,3 After receiving treatment with benzathine penicillin, our patient showed a great clinical response and additionally no relapse was observed during the first 2 months. Unfortunately, no further VDRL testing was performed after treatment and the patient did not attend follow-up appointments, so we were unable to confirm whether he achieved viral suppression or maintained adherence to ART.
This clinical vignette serves as a poignant reminder of the propensity for individuals living with HIV to manifest atypical presentations of common infectious diseases, such as syphilis. In the right clinical setting, it is imperative to prioritize consideration of infectious etiologies with uncommon manifestations over less prevalent dermatoses in this demographic population.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.