
Abstract
Cytomegalovirus (CMV) pneumonia is an uncommon presentation of CMV among patients with HIV/AIDS, particularly in co-infection with Pneumocystis jirovecii pneumonia (PCP). A case was reported with a literature review, and a comprehensive literature search was performed using the PubMed/MEDLINE and Scopus databases. We report a 52-year-old male with AIDS presenting with progressively worsening dyspnea over 1 week. One month earlier, he had completed a 21-day course of PCP treatment, showed improvement and was discharged. Two weeks before presentation, he started antiretroviral therapy (ART), but his dyspnea worsened significantly 1 week later. Chest radiography showed bilateral ground glass opacities. Bronchoscopy and lung biopsy revealed nuclear enlargement with prominent intranuclear inclusions and marginated chromatin of alveolar cells on H&E staining, along with positive immunohistochemistry for CMV. Grocott’s methenamine silver staining identified 3–5 μm irregular yeast-like organisms resembling crushed ping-pong balls, consistent with P. jirovecii. He was treated with intravenous ganciclovir for a total of 21 days, and his clinical and radiologic findings completely resolved. CMV pneumonia co-infection with PCP is extremely rare and should be considered among patients with severely immunocompromise with interstitial pneumonitis unresponsive to PCP treatment or recurring after treatment.
Introduction
Cytomegalovirus (CMV) is a double-stranded DNA virus belonging to the Herpesviridae family. Primary CMV infection is typically asymptomatic, as a competent immune system effectively limits active viral replication. However, in advanced HIV stages, T-helper cell function is compromised, leading to a decline in the adaptive immune response crucial for CMV control. Before the widespread use of highly active antiretroviral therapy (HAART), the prevalence of CMV opportunistic infection (OI) in AIDS was high. Autopsy studies revealed evidence of disseminated CMV in up to 90% of patients with AIDS. CMV OI typically manifests among individuals presenting AIDS-defining illnesses and CD4 lymphocyte counts below 100 cells/µL. CMV pneumonia is an uncommon manifestation of CMV in HIV/AIDS. A large epidemiologic study of AIDS-defining opportunistic infections among 18,733 people living with HIV receiving a diagnosis between 1993 and 2008 found that only 0.6% presented CMV as their initial OI, with no reported cases of CMV pneumonia. Co-infection with CMV and PCP can occur and was mostly reported during the pre-ART era.1,2 However, a few cases have been reported in the post-ART era.3–9 Additionally, rather than being solely due to severe CD4 T-cell depletion from AIDS, CMV re-activation and subsequent pneumonia may be promoted by the steroid therapy used in PCP treatment. Here, we report an unusual case of CMV co-infection with PCP in a patient receiving a new diagnosis of AIDS, accompanied by a literature review. A comprehensive literature search was performed using the keywords “Pneumocystis pneumonia” or “Pneumocystis jirovecii pneumonia” and “Cytomegalovirus pneumonia” combined with terms such as “human immunodeficiency virus” “acquired immunodeficiency syndrome” and “HIV/AIDS” across PubMed/MEDLINE and Scopus databases from their inception to November 2024.
Case presentation
A 52-year-old man presented progressive dyspnea for 1 week. One month prior, he presented worsening dry cough, disturbing daily life activities. He experienced exertional dyspnea and fever. Physical examination revealed a body temperature of 38.1°C, a respiratory rate of 38 breaths/min with rapid and shallow breathing, an SpO2 of 77% on ambient air, a heart rate of 138/min, and a blood pressure of 120/60 mmHg. However, pulmonary auscultation was normal. A rash was observed on the arms and legs, characterized by generalized multiple hyperpigmented papules, compatible with pruritic papular eruption. A chest X-ray showed ground-glass opacity in both lungs. The patient was intubated. Laboratory investigations were performed, confirming HIV with a CD4+ T cell count of 19 cells/µL (1.6%). Other laboratory results revealed that the serum cryptococcal antigen was negative, HBsAg was nonreactive, anti-HBs was positive, anti-HCV was negative, and the syphilis chemiluminescence microparticle immunoassay was negative. Empirical treatment for PCP was initiated due to the severe interstitial pneumonitis in AIDS, with TMP/SMX at 15 mg/kg/day, along with dexamethasone at an equivalent dose of prednisolone (80 mg/day for 5 days, then tapering to 40 mg/day for 5 days, and then reducing to 20 mg/day for 11 days). Tracheal suction for sputum AFB was negative, Xpert MTB/RIF was not detected, bacterial culture isolated normal flora, and the immunofluorescence assay for P. jirovecii was negative. However, after 3 days of TMP/SMX and dexamethasone, he showed dramatic improvement and was extubated. Thus, we clinically diagnosed severe PCP in AIDS and considered the treatment course for PCP to be complete. After 8 days of treatment, the patient’s condition improved significantly, allowing oxygen therapy to be discontinued. He continued to recover clinically and radiologically and was discharged within 12 days. Two weeks before this hospital visit, after being discharged, the patient experienced improvement in exertional dyspnea but continued to experience dry cough. The patient was scheduled for a follow-up appointment at the infectious disease outpatient clinic, where ART with a regimen of TDF/FTC/EFV was initiated.
One week before this hospital admission, after taking ART for 1 week, the patient developed worsening exertional dyspnea accompanied by a high-grade fever. He took antipyretics but experienced no improvement, prompting hospital evaluation. Physical examination revealed a body temperature of 39.4°C, pulse rate of 90/min, respiratory rate of 18/min, blood pressure of 106/64 mmHg and SpO2 of 93% on ambient air. Pulmonary auscultation was normal, and fundoscopic examination showed no abnormalities. A chest X-ray demonstrated worsening findings, with bilateral ground-glass opacities in both lungs as shown in Figure 1. The patient was admitted to an intensive care unit. (a) Chest X-ray on the day of the initial PCP diagnosis; (b) chest X-ray on the day after completing PCP treatment; (c) chest X-ray on the day of CMV pneumonia diagnosis; (d) chest X-ray on the day of completed CMV pneumonia treatment; (e) coronal view and (f) axial view of chest computed tomography showing ground-glass opacities with interlobular and intralobular septal thickening scattered throughout both lungs, predominantly involving the bilateral lower lobes while sparing the subpleural regions.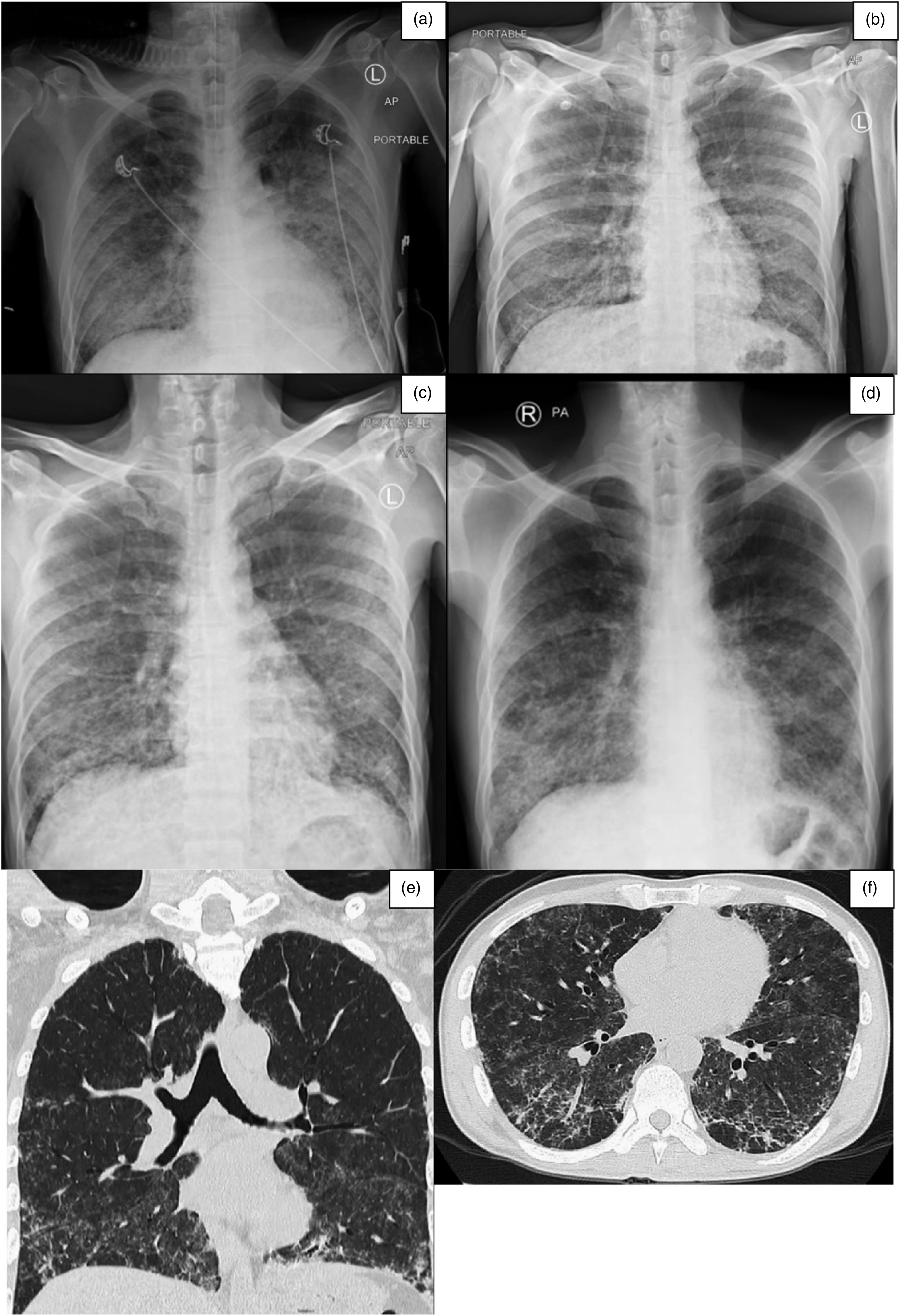
Laboratory investigations revealed mild anemia (Hb: 12.6 g/dL), mild hyponatremia (sodium: 133 mEq/L) and hypoalbuminemia (albumin: 2.5 g/dL). His blood CMV viral load was 7430 (log; 3.87) copies/mL. Chest computed tomography showed ground-glass opacities with interlobular and intralobular septal thickening scattered throughout both lungs, predominantly involving the bilateral lower lobes while sparing the subpleural regions. Additionally, several subcentimeter perivascular, aortopulmonary window, right lower paratracheal and subcarinal lymph nodes were identified, as shown in Figure 1.
A bronchoscopy and lung tissue biopsy were performed at the RB9a segment. Histopathologic examination demonstrated cytopathic changes, with H&E staining showing nuclear enlargement with prominent intranuclear inclusions and marginated chromatin of alveolar cells. Immunohistochemistry confirmed positivity for CMV. Additionally, lung tissue biopsy stained with Grocott’s methenamine silver stain revealed multiple yeast-like organisms with irregular shapes, resembling crushed ping pong balls, measuring approximately 3–5 μm, compatible with P. jirovecii as shown in Figure 2. Bronchoalveolar lavage fluid for Xpert MTB/RIF was not detected, bacterial culture isolated 103 Viridans streptococci, and Neisseria spp.; fungal and nocardia culture revealed no growth. Lung tissue biopsy with staining revealed the following: (a) hematoxylin and eosin (H&E) staining showed nuclear enlargement with prominent intranuclear inclusions and marginated chromatin in alveolar cells. (b) Immunohistochemistry staining was positive for CMV. (c) Grocott’s methenamine silver stain revealed multiple irregularly shaped yeast-like organisms resembling crushed ping pong balls, measuring 3–5 μm.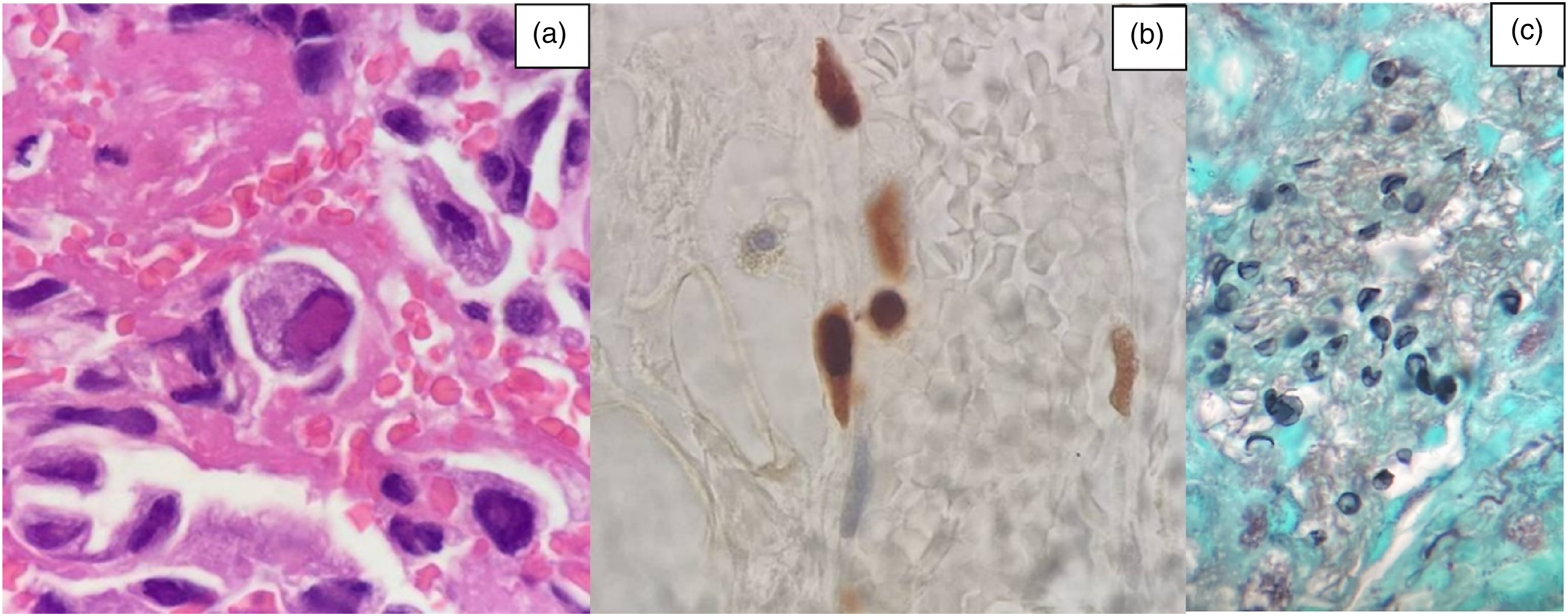
The patient received a definitive diagnosis of PCP co-infection and CMV pneumonia. He was treated with intravenous ganciclovir for a total duration of 21 days. Following treatment, his condition improved, with noticeably reduced dyspnea, significantly improved radiologic findings, and suppressed blood CMV viral load (<150 copies/mL). After completing the full course of treatment, he was discharged home in stable condition and received TMP/SMX prophylaxis. After 6 months of follow-up his HIV-1 viral load was suppressed (HIV-1 VL; 39 copies/mL), and CD4+ T cell was 110 cells/µL (9.4%).
Discussion
Reported cases of PCP co-infection with CMV pneumonia among people living with HIV/AIDS.

Abbreviation: BAL: bronchoalveolar lavage; CMV: cytomegalovirus; IHC: immunohistochemistry; IV: intravenous; mNGS: metagenomic next generation sequencing; NGS: next generation sequencing; PCP: pneumocystis pneumonia; PCR: polymerase chain reaction; PLWHA: people living with HIV/AIDS; TMP/SMX: trimethoprim/sulfamethoxazole; VV ECMO: venovenous extracorporeal membrane oxygenation.
Diagnosis is based on clinical symptoms including cough, fever, and shortness of breath, accompanied by radiographic findings that typically reveal diffuse interstitial infiltrates. The gold standard for diagnosing CMV pneumonia and PCP is tissue biopsy, which identifies infection-specific cytopathic changes such as enlarged cells with viral nuclear inclusion bodies. 10 BAL CMV viral load has become a widely accepted alternative to lung biopsy for evaluating lung disease. Using a cutoff value of 1258 IU/mL of CMV in BAL, pneumonia can be diagnosed with a sensitivity of 76%, specificity of 100%, positive predictive value of 100%, and negative predictive value of 98%. CMV was isolated in 100% of BAL cultures. Among patients with HIV or those immunocompromised, CMV DNA detection in BAL has been suggested to provide valuable diagnostic information, particularly when performed in clinically suspected cases.13,14 Several studies have investigated the utility of CMV viral load in blood for diagnosing pneumonitis and determining a cutoff value for clinically significant lung replication. However, the conclusions are not unanimous.15–17 Some studies suggest a high predictive value for lung disease, while others indicate that a negative blood CMV viral load does not exclude pneumonitis caused by local lung replication. 14 Thus, to perform the diagnosis, the clinician should integrate clinical, radiologic, and microbiological findings. Early diagnosis and prompt treatment significantly improve patient outcomes.
Treatment guidelines recommend the use of ganciclovir at a dosage of 5 mg/kg every 12 h intravenously or foscarnet at 60 mg/kg intravenously for 14–21 days. Literature reviews suggest that patients with HIV and CMV pneumonia can be effectively treated with ganciclovir or valganciclovir, typically for 21 days. 10 Shorter treatment durations may lead to treatment failure. Most patients respond well to treatment, with approximately 60% showing improvement. ART can be initiated one to 2 weeks after completing CMV pneumonia treatment. 18 Once the acute CMV syndrome resolves and effective ART is started, chronic maintenance therapy for CMV pneumonia is generally not recommended. 10
Drug-resistant P. jirovecii has been rarely reported. Most cases have shown only genotypic resistance, commonly found among patients receiving long term TMP/SMX prophylaxis, and its clinical significance remains controversial.19,20 PCP is the most common cause of interstitial pneumonia among patients with HIV/AIDS. A definitive diagnosis of PCP requires bronchoscopy or bronchoalveolar lavage to obtain an adequate specimen. However, in clinical practice, PCP is often diagnosed clinically and treated empirically. Given the rarity of drug-resistant P. jirovecii, a dramatic improvement is typically expected after TMP/SMX treatment, particularly within 1 week. Therefore, when no response occurs, alternative diagnoses should be considered. CMV pneumonia should be suspected, especially among patients with PCP, treated with TMP/SMX for at least 1 week without improvement or developing recurrent interstitial pneumonitis shortly after PCP treatment. 7 Paradoxical immune reconstitution inflammatory syndrome of PCP (PCP-IRIS) should be included in the differential diagnosis, particularly in the era of rapid initiation of high potency ART, especially integrase strand transfer inhibitors. The incidence of PCP-IRIS has been reported to range from 5 to 40% among people living with HIV/AIDS, with a median onset of 9.5 days after initiating ART. Notably, PCP-IRIS is not associated with increased mortality or respiratory failure. 21 However, a rigorous evaluation is essential to exclude concurrent co-infections and underlying malignancies before establishing a diagnosis of PCP-IRIS.
This case highlights the histopathologic diagnosis of co-infection with PCP and CMV pneumonia in a patient with AIDS, emphasizing the need for clinicians to consider co-infection in similar scenarios. However, this case has certain limitations. Firstly, genotypic resistance testing of P. jirovecii was not performed to confirm the possibility of drug resistance. Nonetheless, given the patient’s excellent response to TMP/SMX during the initial occurrence of interstitial pneumonia and the absence of prior TMP/SMX exposure, the likelihood of drug-resistant P. jirovecii is considered very low. Secondly, pre-ART HIV-1 viral load was not assessed in this case. Measuring HIV-1 viral load could have been valuable in supporting the possibility of PCP-IRIS following ART initiation.
Conclusion
Cytomegalovirus pneumonia is a rare manifestation of CMV among people living with HIV. It should be considered among patients with AIDS presenting interstitial pneumonitis, particularly among those with PCP failing to improve after TMP/SMX treatment or developing recurrent interstitial pneumonitis shortly after completing PCP therapy.
Footnotes
Author contributions
All authors meet the ICMJE authorship criteria. All authors participated in the diagnosis, management and/or care of the patient. T.T. and W.N. wrote the draft and revised the manuscript for important intellectual content. W.N. cared for the patient and supervised the writing of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.