
Abstract
The British Association for Sexual Health and HIV UK guideline on the management of scabies has been updated in 2025. It provides details on the pathology and clinical features of scabies, with evidence-informed, practical recommendations on diagnosis, treatment and follow-up of adults and children aged 13 or above attending sexual health services. Key updates are detailed at the start of the article.
What is new in the 2025 guideline?
• Updated description of the biology of the mite and the host response. • The following diagnostic tests are included: adhesive tape test for microscopy, dermoscopy and histology. • The 2020 International Alliance for the Control of Scabies (IACS) consensus criteria for the diagnosis of scabies are summarised. • Two first-line treatments are recommended: topical permethrin 5% cream, or ivermectin (200 μg/kg) by mouth. Whichever treatment is used, a second dose should be administered 7–14 days after the first dose. Co-ordinated fomite decontamination and treatment of contacts are recommended to prevent re-infestation. • The evidence base for recommended first-line treatments has been expanded in light of systematic reviews published since the last version of this guideline. Both treatments have similar effectiveness in clinical trials, and decision should be based on individual clinical circumstances. Cost and resource implications of using oral ivermectin versus permethrin cream require consideration. • The evidence base and specific recommendations for non-pharmacological management (e.g. decontamination of fomites) are included. • Malathion lotion is now listed as an alternative, rather than recommended, regimen. • Other alternative regimens (benzyl benzoate [BB], topical ivermectin, sulphur ointment, spinosad and tea tree oil) are briefly considered, and the evidence summarised. • New section on follow-up including evaluation and management of post-scabetic itch and suspected treatment failure is included.
Introduction and methodology
Objectives
The objective of this guideline is to provide updated, evidence-informed, practical recommendations on the clinical management of people with scabies who are aged 13 and above.
This guideline offers recommendations on 1) diagnostic approach, treatment and follow-up of individuals presenting with scabies, and 2) management of sexual and other close contacts and hygiene measures to prevent re-infestation.
The guideline is aimed primarily at adults with scabies aged 18 years or older presenting to healthcare professionals working in departments offering specialist level 3 care in sexually transmitted infections (STIs) management within the United Kingdom (UK). However, the principles of the recommendations are applicable across all levels of STI care providers, and non-specialist services may need to develop, where appropriate, local referral pathways. Children aged 13 to 17 can attend sexual health clinics in the UK; unless otherwise stated, the recommendations for this age group are the same as for adults.
Search strategy
This guideline was produced according to specifications set out in the British Association for Sexual Health and HIV (BASHH) Clinical Effectiveness Group (CEG) document ‘framework for guideline development and assessment’ (2015, updated 2020) accessed at https://www.bashh.org/_userfiles/pages/files/resources/2020_guidelines_framework.pdf.
This guideline has been updated by reviewing the previous 2016 UK Guideline on the Management of Scabies
1
and conducting a comprehensive literature search of publications. Four databases (Medline, Embase, Cochrane Central Register of Controlled Trials and Cochrane Database of Systematic Reviews) were searched for articles published from 1 January 2015 to 7 June 2023 with the search terms ‘scabies’ or ‘sarcoptic mange’ or ‘sarcoptes scabei’ combined with at least one of the following set of terms: • Etiology or cases or diagnosis or treatment or therapy or interventions; • Specific drugs such as permethrin or ivermectin or malathion or spinosad or crotamiton or hexachlorocyclohexane or lindane or benzyl benzoate or sulphur ointment; • Terms related to side effects or sexual transmission or contract tracing, pregnancy, breast feeding or epidemiology.
The search was limited to systematic reviews and randomised controlled trials (RCTs) using specialist filters designed by the Scottish Intercollegiate Guidelines Network 2 relating to humans. Articles relating to children (<16 years old), mass-treatment strategies or without a focus on scabies were excluded. For the complete list of search terms used for each database, refer to Appendix 1.
Methods
In total, 366 unique articles were retrieved from the four databases following deduplication. One author (AST) reviewed the titles of these articles and excluded 105 articles as irrelevant. Another author (LH) reviewed the titles of the excluded articles and agreed that they were irrelevant. The remaining 261 articles were randomly assigned to four of the authors (AST, LH, GM and PNS) for screening. The authors excluded 197 articles on the basis of the abstract and/or full-text. The findings of the remaining 64 articles were summarised by the four authors who had conducted the screening. Additional articles, not retrieved from the initial comprehensive literature search, and book chapters were considered when appropriate. The guideline recommendations were made and graded based on the available evidence, using the Grading of Recommendations, Assessment, Development and Evaluations1–6 (GRADE, refer to Appendix 2) system to assign quality of evidence (grade 1–4) and strength of recommendation (grade A or B). Where there was a paucity of high-quality evidence, expert judgement was considered. The guideline was revised by all authors (AST, CB, GM, HM, LH, PNS, SLW and SS).
Equality impact assessment
An assessment of the guideline and its recommendations was undertaken to ensure the principles of equality and diversity were adhered to and is available in Appendix 3.
BASHH has adopted an anatomical approach without assuming gender in the majority of guidelines and uses gender terminology in line with BASHH ‘sexual health standards for trans, including non-binary, people’.
Stakeholder involvement, piloting and feedback
The writing group consisted of Specialist Physicians in genitourinary medicine (GM, LH, PNS and SS) with experience in managing scabies, a physician training within general medicine (AST) with experience in managing scabies as a Clinical Fellow in genitourinary medicine, a Clinical Academic and Consultant Dermatologist with UK and international expertise in scabies (SLW), a Specialist Pharmacist working in a large sexual health service (HM) and a consultant in health protection at UK Health Security Agency (UKHSA) (CB). The first draft was produced by the writing group and then circulated to the BASHH CEG for review using the Appraisal of Guidelines, Research and Evaluation (AGREE) 7 appraisal tool Appendix 4. The second draft of the guideline was posted on the BASHH website for wider consultation (2 months) and any comments received during the consultation period were reviewed by the authors and acted on appropriately. The document was also reviewed by members of the BASHH Sexual Health Advisors and Nurses (SHAN) Special Interest Group, a patient representative, target users and the public panel of BASHH, and their feedback was considered by the authors and used to inform the guideline. The final draft was presented to the CEG for review and piloting in sexual health clinics.
Once the guideline is published, the CEG will keep it under review should critical new evidence become available that affects the current recommendations. The guideline will be formally reviewed and updated, if necessary, every 5 years.
Aetiology
Introduction
Scabies is a common disease that can affect people of any age or socioeconomic status worldwide. Estimates of its prevalence range from 0.2 to 71%, with the highest rates found in the Pacific region and Latin America. 3 Risk of acquiring scabies is increased in crowded conditions such as in care homes, schools and prisons.
Causative pathogens
Scabies is caused by the human mite Sarcoptes scabiei var hominis. Female mites measure 0.3–0.4 mm and are about twice the size of males. 4 Mites burrow into human skin and lay their eggs, which later hatch and grow into adults.
The life cycle begins after mating following which the male dies and the female mite begins to dig burrows with help of proteolytic enzymes. The burrows are seen in the superficial layers of epidermis, primarily the stratum corneum, and typically persist for 4–6 weeks. Mites live in the host by ingesting intercellular fluid at the interface of stratum lucidum and stratum granulosum.5,6 They are able to penetrate the skin within 30 minutes of contact with the host. 7 Mites burrow at a rate of 0.5 to 5 mm per day throughout their adult lifetime, which typically spans 4–6 weeks. The female lays one to three eggs per day, totalling about 25 eggs in her lifetime, before dying. The eggs hatch after 3–4 days, developing into larvae that mature into adults after 10–15 days. Less than 10% of the eggs develop into mature adults. The possible reasons for this include removal by scratching and the host immune response. 8 The average number of mites in a person with an initial infestation is 10 to 15 and about half this number with a subsequent infestation.9,10 The newly hatched adult mites can reinfest the host at a different site or infest another host.11,12
Transmission
Transmission occurs from person to person through skin-to-skin contact. Scabies mites are attracted by both heat and body odour. 13 In young adults, scabies is frequently sexually acquired. Other factors for transmission include living in crowded conditions and malnutrition. 7 Transmission through casual contact such as a hand shake is unlikely. 14 Transmission of scabies is more common during the first 4–6 weeks, when patients are asymptomatic. 15 Fomite transmission is uncommon but can occur in those wearing contaminated clothing or using a bed recently occupied by a person with scabies, for example. 10 Transmission is more likely to occur with crusted scabies due to the greater number of mites present16–18 and because mites can survive longer for up to 7 days in the shed skin. 19 The survival of mites outside the human body depends on the room temperature and humidity. At 21⁰C 20 with a relative humidity of 40–80%, mites survive outside the body for 24–36 hours.11,21–25 In contrast, fasting female mites have been shown to survive for up to 19 days at 10⁰C and relative humidity of 97%. 22
Scabies mites are resistant to alcohol and to other antiseptics such as povidone iodine and soap.11,26 Chloramine 5% has been used to disinfect rooms of individuals with scabies. 27
Risk factors for scabies
Risk factors for scabies include: young age; old age; living in crowded homes, care homes or prisons; low income level and sharing clothes and towels. 28
The epidemiology of scabies is complex and varies between different global regions, but crowded living conditions and immunodeficiency are frequently encountered as risk factors. In the UK, most cases are through sporadic transmission with occasional outbreaks in closed institutions such as nursing homes.7,28
Clinical features
Clinical history
A history of pruritus that worsens at night and concurrent history of itching among family members and/or sexual or household contacts is suggestive of scabies.
Symptoms and signs
Classical scabies
The main symptom of scabies is intense pruritus that is usually worse at night. The pruritus is caused by the direct effects of the host-mite interaction, 29 as well as a delayed type-IV hypersensitivity reaction to the mite and its products (faeces and eggs).9,30 The exact mechanism of itch in scabies is still to be determined. Recent studies have shown that non-histaminergic receptors may play a role in causing pruritus. 31 This results in excoriations that provide a point of entry to bacteria such as Staphylococcus aureus and Group B streptococci.
Symptoms begin 3–6 weeks after the primary infestation but can occur as early as 1–3 days, in a person with prior infection, probably due to sensitisation to the mite and mite products. Scabies is infectious before the rash develops.32–34 A lack of a history of itching does not exclude scabies.
The most common lesions are erythematous papules, often excoriated, seen in a characteristic distribution over the interdigital web spaces, sides of fingers, flexor aspects of wrists, extensor aspects of elbows, anterior and posterior axillary folds, around nipples, penis and scrotum, around the umbilicus, medial aspect of thighs, buttocks, sides and back of feet. Vesicles, nodules and wheals may also be seen. 21 The back is usually not affected, and the head is spared except in children. The mites tend to avoid areas with a high density of pilosebaceous follicles, such as the scalp and beard in men. 35
Palms are frequently affected in all age groups. The soles are also affected in infants and in people who are non-ambulatory. Despite the predilection for certain sites, lesions are roughly symmetrical across the body. 36
The pathognomonic lesion is the burrow, which is a linear intra-epidermal tunnel produced by the moving mite and appears as short wavy greyish/white threadlike elevations of 2 to 10 mm in length. Burrows are difficult to find if there is excoriation or secondary eczematisation. Nodular lesions may also be seen especially on the penis and scrotum, the areola, the buttocks, groin and the axillary regions. These lesions are intensely pruritic and tend to persist after treatment, suggesting they result from a hypersensitivity reaction to dead mites8,37,38 and do not indicate active infection. Urticarial lesions may rarely occur.39,40 It has been proposed that the more severe inflammatory response seen in nodular lesions may be due to deeper penetration of the mite from the epidermis to dermis. 41
Crusted scabies
Risk factors for crusted scabies (Scabies crustosa) include: immunocompromise for example people living with advanced human immunodeficiency virus (HIV) infection , leprosy, lymphoma, organ transplant recipients, those receiving systemic or potent topical steroids 42 ; older age; learning disability (e.g. people with Down syndrome); neurological disease causing reduced sensation; and physical disability with decreased capacity to respond to itch by scratching.43,44 In about 40% of cases, no risk factors can be identified. 45 There is some evidence that crusted scabies may be associated with immunogenetic susceptibility.46,47
Crusted scabies is characterised by generalised erythematous scaly crusted plaques, which can be malodorous and associated with fissuring and can affect any part of the body including the face and scalp. The plaques can become verrucous over bony prominences. It may also occur as a diffuse non crusted form with involvement of the back. 21 However, itching may be mild or absent. Crusts contain large numbers of mites and eggs, and hence crusted scabies is considerably more infectious than classical scabies.
Generalised lymphadenopathy is usually present. 23 Sepsis is a frequent complication of crusted scabies as fissures associated with this condition provide an entry point for bacteria. 48
Scabies contracted by a healthy person from a patient with crusted scabies is no different from classical scabies. 43
Nail scabies
This is usually seen in people with crusted scabies. It has rarely been reported in children and healthy adults. 49 Affected nails become thick, dystrophic and discoloured. Subungual hyperkeratosis may be seen. 49 This may be an important reservoir of mites resulting in repeat re-infestation. 50
Bullous scabies
Bullous scabies is a rare variant seen in the elderly which presents with extremely itchy bullae with or without concomitant classical scabies lesions. 50 The trunk and extremities are commonly affected, and the differential diagnosis would involve other bullous disorders such as bullous pemphigoid. 50
Scabies in the elderly
Atypical manifestations of scabies may occur in older adults, with involvement of scalp and face, reduced inflammatory response and persistence of pruritus. 51 Elderly people are more likely to develop crusted scabies.
Scabies in people living with Human immunodeficiency virus
People living with HIV who are immunosuppressed (usually those with CD4 counts <200) may present with crusted scabies52–55 and atypical papular lesions on the face and scalp, psoriasiform lesions, and generalised pruritus with few lesions. Pruritus may be mild due to an impaired immune response. 56 Individuals not taking antiretrovirals may initially present with classical scabies and, as their CD4 cell count falls, may develop crusted scabies with little or absent pruritus. In most people living with HIV, however, the symptoms and signs of scabies are no different from people without HIV. Crusted scabies presenting as a manifestation of immune reconstitution inflammatory syndrome following initiation of antiretroviral therapy has been reported. 57
Atypical scabies
Animal scabies
Humans can rarely contract scabies from pet dogs (caused by S. scabiei var canis) and cats (caused by Notoedres cati). Zoonotic scabies differs from classical scabies in that the incubation period is shorter, the distribution of lesions is confined to sites of contact with the animal, and burrows are not seen. It does not cause extensive infestations in humans unless the animal remains untreated. The lesions are self-limiting, as these mites do not reproduce in human hosts and rarely survive for more than a few days. 17 Consequently, human to human transmission does not occur, 58 and no treatment other than that of the infested animal is required.
Scabies Incognito
This refers to the altered clinical picture seen following use of topical steroids and consists of widespread atypical papular lesions that may mimic other generalized forms of eczema. Symptoms are masked but the patient remains infectious. 9
Complications
Secondary bacterial infections due to Staphylococcus aureus, group A β-haemolytic streptococci, or peptostreptococci 59 may result in skin conditions such as impetigo, folliculitis, furunculosis, ecthyma and abscesses. Secondary eczematisation due to constant scratching, and/or irritant effects of topical medication can occur. Other reported complications include glomerulonephritis 60 and leukocytoclastic vasculitis.61,62 Scabies associated pruritus can be distressing and cause significant problems with sleep.11,63 Secondary infection can also aggravate itch in scabies.64,65
Diagnosis
Scabies is a clinical diagnosis that should be suspected on the basis of symptoms, signs and risk factors as described above. Diagnosis is usually made clinically from the appearance of excoriated papules, burrows and nodules at sites of predilection.
Summary of 2020 IACS criteria for the diagnosis of scabies.
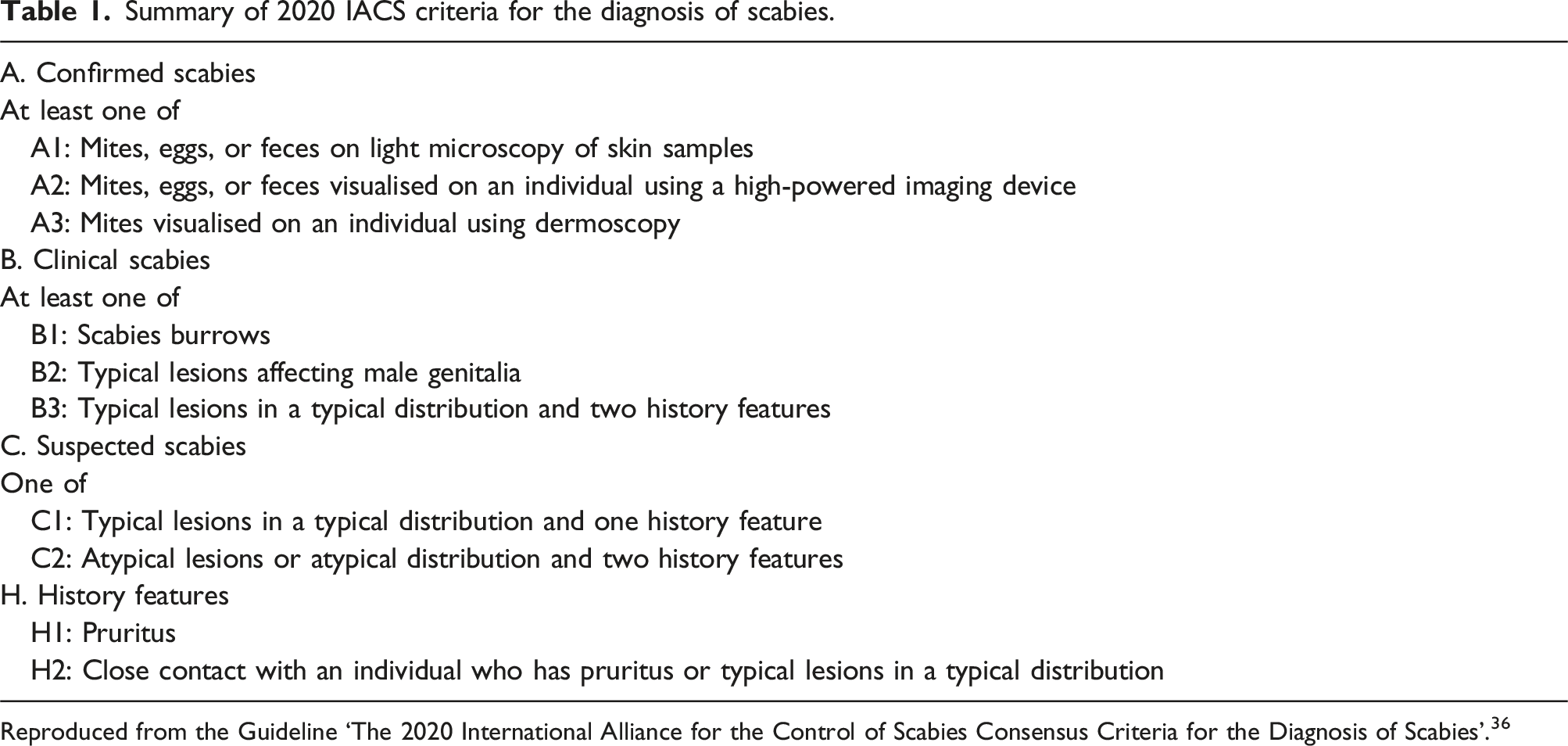
Reproduced from the Guideline ‘The 2020 International Alliance for the Control of Scabies Consensus Criteria for the Diagnosis of Scabies’. 36
Identification of mites and mite products
Microscopy
Definitive diagnosis relies on microscopic identification of the mites, eggs or faecal pellets (scybala) obtained by scraping skin burrows with a scalpel blade and placing the specimen on a glass slide with 10% potassium hydroxide. 8 Scrapings should be taken from multiple sites. Potassium hydroxide dissolves excess keratin (particularly seen in crusted scabies) and thereby permits better visualisation of the mite and mite products.
Alternatively, a drop of mineral oil is applied to the selected lesion or on the scalpel blade. The entire lesion is scraped away with the scalpel blade. The oil and the skin scrapings are then transferred to the microscopic slide and examined under the microscope. 66
In another useful technique, which can be combined with scraping using a scalpel blade, the adhesive side of a transparent tape is firmly applied on to an appropriate skin lesion (e.g. burrow), the tape is pulled off after a few seconds and transferred directly onto a slide for microscopy. 67
A negative microscopic result does not exclude scabies. Microscopy is highly operator dependant. 16 The sensitivity of microscopy in diagnosing scabies varies from 46% to 90% but the specificity is 100%. 68
Identification of burrow: burrow ink test
The burrow ink test (BIT) allows identification of burrows. To perform the BIT, black or blue ink is applied to the suspected papule and then wiped off with alcohol to remove surface ink. A positive BIT is indicated by the presence of a characteristic dark, zigzagged line running across and away from the lesion due to ink tracking down the mite’s burrow.69,70
Other methods
Using a standard magnifying lens with 10 x magnification is useful for the identification of mites/burrows.
Other methods used for diagnosis of scabies include in vivo techniques such as dermoscopy, optical coherence tomography and detection of S. scabiei DNA from cutaneous scales using polymerase chain reaction (PCR) or enzyme-linked immunosorbent assay (ELISA).71,72
Dermoscopy
Very few clinicians use dermoscopy in Sexual Health Clinics, but it is universally used in dermatology services. The technique helps to locate mites and burrows, and serves as a guide for obtaining skin scrapings for microscopy. 68 The two signs described in scabies are: 1) Delta wing sign or jet with contrail sign that represents the head and anterior legs of the mite that are usually seen at the end of a burrow; 2) The ‘mini triangle sign’ that corresponds to the head of the maturing larva within an egg. 23 In crusted scabies, multiple burrows may be seen. 73 Eggs may also be seen as ovoid structures within the burrows. 23
A disadvantage of dermoscopy, when used on its own, is that its specificity is low 68 and it can be difficult to detect mites on pigmented skin. 70
Histology
Biopsy is rarely performed or required in the context of suspected scabies presenting to a sexual health clinic. However, it can be helpful where diagnosis is uncertain, especially in cases of crusted or nodular scabies. Histological findings include pleomorphic infiltrate of eosinophils, lymphocytes and histiocytes in the dermis. In addition, pink, pig-tail-like structures, denoting egg fragments, may be seen in the epidermis. 74
Differential diagnosis
Classical scabies
Scabies may frequently be mistaken for other skin diseases. It is important to have a high degree of suspicion to recognise symptoms and signs of scabies.
Differential diagnoses for scabies include impetigo, folliculitis, papular urticarial reactions, atopic dermatitis, contact dermatitis, dermatitis herpetiformis, psoriasis, seborrhoeic dermatitis, pytiriasis rosea, secondary syphilis and lymphoma and pseudolymphoma (if scabies presents with nodules).
Crusted scabies
Differential diagnosis includes psoriasis, eczema, Darier’s disease, pityriasis rubra pilaris, palmoplantar keratoderma and cutaneous lymphoma.
Management
General advice
People with scabies should be informed about its transmission through skin-to-skin contact, particularly between sexual partners and people living in the same household, and secondarily by fomite transmission. (Good practice point [GPP])
To avoid recurrence, it is recommended to co-ordinate treatment, where possible, to ensure that both those with scabies and ALL relevant contacts are treated correctly at the same time. (GPP).
People with scabies should be offered screening for other STIs. (GPP)
Failure to decontaminate fomites is a risk factor for treatment failure. 75 Optimal time and temperatures required for effective elimination of viable mites and eggs have varied between different in-vitro studies.76,77 Both mites and eggs are likely to be rendered non-viable by laundering items at 50°C for 35 minutes. 76
Clinicians should advise patients on the correct methods of decontaminating or quarantining potential fomites. (GPP) All clothes, soft slippers, towels and bed linen of the affected case should be machine-washed for at least 35 minutes at a minimum of 50°C and/or tumble dried on a high heat setting (50 to 120°C) for 10-35 minutes (higher-end temperatures may eliminate mites more rapidly) 77 on the day of application of the first treatment. If clothes cannot be laundered at high temperature, they can be sealed in plastic bags for 4 days at room temperature, after which mites are unlikely to survive.77,78
Freezing items below -10°C for at least 5 hours is another option for killing mites and eggs. 77 Case by case advice may be required regarding decontamination or quarantining of other close-contact items e.g. children's toys, furnishings. 75 In cases of crusted scabies thorough cleaning of the person's environment including vaccuming carpets and furniture, and laundering curtains and cushion covers is advised. 78
Clinicians should inform patients about proper application of topical scabicides. (GPP) The ankles, under finger nails, between the toes, and sacral region are body sites often left untreated and where scabies has a predilection. 79 Assistance with topical application may be required (e.g. from a partner, relative or carer) to ensure full coverage.79,80
Written advice in the form of a leaflet or website link should be provided. Availability in different languages and a pictorial guide are recommended.
80
(GPP) • The writing committee recommends the use of the patient information leaflets on scabies produced by the British Association of Dermatologists (BAD) (available at https://www.skinhealthinfo.org.uk/condition/scabies/)
81
and the Primary Care Dermatology Society (PCDS) (available at https://www.pcds.org.uk/patient-info-leaflets/scabies).
82
Clinicians should counsel patients to expect that symptoms may take more than 4 weeks to resolve. 83
Treatments
Recommended scabicide treatment regimens for classical scabies
Two possible treatment regimens are recommended for uncomplicated classical scabies: permethrin cream84–92 and oral ivermectin.84,87,89,90,93–95 Both are licensed for use in scabies92,95,96 and have been shown to have similar effectiveness in a systematic review of RCTs. 84 Prescribing decision should be based on the individual clinical situation. Cost, availability and resource implications also need to be considered.
Permethrin 5% cream (Grade 1A)
• Adults and children should apply a thin layer of cream to the whole body, including the neck, face (avoiding the area around the eyes), ears and scalp.
92
Do not apply the cream to mucous membranes. • Head and neck application is recommended for all but is particularly important for adults aged over 65 years and people who are immunocompromised.
92
• Pay special attention to applying the cream to the hands and wrists, under fingernails, between the fingers and toes, around the nipple area, the soles of the feet and the buttock creases and external genitalia. Clip finger and toenails prior to application (to prevent eggs becoming trapped there) and consider using a soft toothbrush to aid application under nails (GPP). • Remove all clothes and jewellery. If rings cannot be removed, move them and apply cream beneath them. Apply the cream to cool, clean, dry skin. Avoid applying immediately after a hot bath or shower. Wait until the cream has fully dried on the skin before putting any clothing on (GPP). • Applying the cream at night and with the assistance of someone else (to apply to the back and other difficult-to-reach areas and check adequate coverage) may be of benefit where possible. • Leave the cream on for 12 hours, then wash it off. If hands are washed within 12 hours of application, reapply the cream to the hands. The same advice applies if cream is washed off or removed from other body areas. • Most adults require one tube (30 g) to cover their body adequately. However, some adults may need up to two tubes (60 g) for a single application.
92
• Given that one cream application often does not achieve full skin coverage, reapply the cream 1–2 weeks later. (GPP)
Ivermectin tablets (Grade 1A)
• The recommended regimen involves two doses of oral ivermectin,
93
each at a dosage of 200 μg per kg.
96
See Table 2 for suggested doses based on available 3 mg tablets (e.g. 5 x 3 mg tablets [15 mg] for a 70 kg person). We generally advise rounding up to the closest 3 mg tablet based on available efficacy and safety data. • The first dose should be administered on Day 1 of the treatment, followed by a second dose on Day 8, but this can be taken up to Day 15 if necessary. (Grade 1D) • Ivermectin is not ovicidal. Giving a second dose is associated with lower risk of treatment failure than a single dose.
93
• Ivermectin is licensed in individuals (adults and children) weighing over 15 kg.
96
• Although the manufacturer’s Summary of Product Characteristics (SmPC) for ivermectin
95
advises it be taken on an empty stomach, taking ivermectin with food may potentially increase its bioavailability and penetration into the dermis.97,98 Suggested dosing for oral ivermectin. Table derived from Summary of Product Characteristics for Ivermectin use in Strongyloides (based on 200 μg per kg per single dose)
95
with expert opinion used above 80 kg.

There is wide variability in trial protocols regarding dosing for both permethrin84–91 and ivermectin.84,87,89,90,93–95 Permethrin doses ranged from one to five applications of 30 to 60 g of cream, while ivermectin doses ranged from one to two doses of 200 μg per kg.
Our recommendations for ivermectin dosing are based on expert opinion, while recommendations for permethrin are aligned with licensing standards in the UK.
Evidence base is limited in the context of scabies treatment in people with very high body weight requiring ivermectin doses above 18 mg (the upper limit of the SmPC). 99 However, ivermectin appears to follow linear pharmacokinetics and has a high volume of distribution, including within adipose tissue. It has been shown to be safe and well-tolerated in a dose escalation study using single doses up to 120 mg. 98 We advise discussion with pharmacy/microbiology if prescribing ivermectin in the context of very high body weight.
Alternative regimens for classical scabies
There are no data on the use of sequenced treatment with multiple agents, or the management of suspected drug-resistant scabies. 100
In addition to the recommended treatments, several other agents, for which there is less evidence, may be available.
Benzyl benzoate is licensed for treating scabies in the Republic of Ireland, but it is not currently licensed in the UK. It requires sourcing from a special-order manufacturer, so may not be widely available. Several clinical trials have assessed its use, with generally worse response rates of BB (ranging from 60% to 92% effectiveness) in comparison to permethrin or ivermectin (84%–100% effectiveness), and an increased incidence of skin irritation compared with permethrin.88,89,91,94,104 There are no published systematic reviews of these trials. Recently, there has been a single centre Austrian trial, conducted in 2022-23, reporting superior efficacy of BB compared to permethrin, based on dermoscopy-based follow-up at 3 weeks post-treatment. 105 However, it is noted that the primary outcome is not explicitly stated in the manuscript. Both agents were applied daily for three consecutive days, an unusual regimen for permethrin. At least 22% of participants had received treatment with permethrin or ivermectin prior to enrolment, but the distribution of these individuals between the treatment arms is not specified. In addition, household contacts could be enrolled, creating potential for confounding. Hands were the predominant infestation site (87%). Permethrin 5% cream was well-tolerated, with mild itching after application reported by only 6% of users. In contrast, 47% of those in the BB group experienced treatment-related adverse events, including mild or moderate burning or stinging in the application area or on excoriated skin lasting up to 1 hour.
Benzyl benzoate may be used as an alternative treatment for scabies in cases where there have been multiple treatment failures with recommended agents, or these are unavailable (consider discussion with dermatology or infectious diseases colleagues). (Grade 2B)
The
Treatment of crusted scabies
Crusted scabies is characterised by hyperinfestation with mites. There is relatively little evidence to inform treatment, and most published information comes from the treatment of Aboriginal Australians. 112 Treatment regimens comprise a combination of oral and topical antiparasitic agents and a topical keratolytic agent.109,113 A scoring system has been described, with three grades of severity indicating 3, five or seven doses of oral ivermectin 200 μg per kg over 28 days. 109 The topical antiparasitic agent may be permethrin 5% cream, or BB combined with 5% tea tree oil, if available. The keratolytic agent is lactic acid and urea in sorbolene cream. The addition of systemic antibacterials is often required. (Grade 1D)
Admission to hospital is avoided unless there is a clinical necessity (e.g. severe sepsis) to prevent risk of transmission to clinical staff and patients. Because of the high parasite burden and shedding of viable mites, there is a significant risk of transmission to carers, health care staff and family or friends who have had only casual contact with the affected person. 54 Early involvement of a dermatologist is recommended. Some patients will also require input from an infectious disease specialist. (GPP)
Pregnancy and breast/chest-feeding
People who are breast/chest-feeding or pregnant should be treated with permethrin 5% cream. 92 (Grade 1D) Alternatively, use malathion 0.5% aqueous liquid, 114 if permethrin is not available or appropriate (e.g. prior hypersensitivity or suspected permethrin resistance). Systemic exposure from topical application of either of these agents is extremely low and, although study data are limited, and neither is licensed for use in pregnancy or lactation, evidence available from their widespread use does not suggest an increased risk of harm to the foetus. 115
People who are breast/chest-feeding should remove the liquid or cream from the nipples before breast/chest-feeding and reapply treatment afterwards. (GPP)
Benzyl benzoate has not been studied in pregnancy or breast/chest-feeding. The SmPC from the product licensed in the Republic of Ireland states that the ‘drug is for topical use and is unlikely to represent a hazard to the pregnant or lactating patient. After application of treatment, breast-feeding should be suspended, but may be restarted once the emulsion has been washed off the body.’ 103
Oral Ivermectin is not recommended in pregnancy because of the uncertainty about its safety in the foetus or breast/chest-fed infant 95 and the lack of evidence that it is superior in efficacy to permethrin. (Grade 2D)
Refer to specialist pharmacist, dermatologist and/or infectious diseases/microbiology, for advice in context of pregnancy or breast/chest feeding, where there has been an inadequate response to topical treatments. (GPP)
In people living with HIV taking antiretroviral therapy
People who have uncomplicated classical scabies and are also living with HIV should receive the same treatment regimens as those who are HIV negative. Prior to the availability of effective antiretroviral therapy, crusted scabies was recognised as a possible complication of HIV-related immunodeficiency. 56
Reactions to treatment
Skin reactions may occur with any topical treatment. Paraesthesia is a recognised side effect of permethrin 92 and is usually mild and transient. More significant irritation and hypersensitivity can occur, including erythema, oedema, pruritus or dermatitis.
Malathion is generally well tolerated. Mild skin reactions may occur. 114
Benzyl benzoate may cause skin reactions, such as burning/stinging or contact dermatitis, and be irritant to mucous membranes. Systemic symptoms have been reported following excessive topical use of BB.88,89,91,94,103,104
Clinical assessment may be needed to differentiate between contact dermatitis, caused by treatment, and ongoing symptoms of scabies. Treatment of skin reactions may include emollients, antihistamines and/or corticosteroids.
A wide range of adverse drug reactions, particularly neurological syndromes, are reported for oral ivermectin therapy.95,116 Nausea and headache are also thought to be common side effects. The frequency of such side effects is unknown, but in a systematic review of clinical trials of scabies treatment, the overall adverse event rate for oral ivermectin was 5% compared to 4% for topical permethrin. 84 It should be noted that ‘adverse events’ in a clinical trial context do not imply causal association with the intervention under study. It has been suggested that the potential for toxicity or side effects of ivermectin is much lower than once thought. 117
Follow-up
• No clear clinical trial evidence exists regarding optimal follow-up, and routine post-treatment reviews have not been recommended previously for scabies in the UK.
1
• However, a face to face review to evaluate the cure of the patient, prevent re-infestation from untreated contacts or from failure to follow laundry and cleaning advice, and to limit unnecessary repeat self-treatments, may be helpful 4–6 weeks after the last administration of scabicide.
80
• Itch beyond 4 weeks after last (second dose) administration of a primary recommended scabicide treatment can represent a diagnostic challenge, and clinicians should perform careful re-examination, including skin scrapings, BIT and dermoscopy where available. (GPP) • Appearance of new burrows and/or evidence of visible mites at any stage beyond 7 days after completion of anti-scabies treatment is indicative of need for further treatment.
36
(see below) • Itching should progressively improve with treatment. If itching worsens despite receiving adequate treatment, the possibility of re-infection or an alternate diagnosis is to be considered.
118
Post-scabetic itch
In most cases, itch and rash should be expected to improve within 2 to 4 weeks after treatment. 84 However, a recent study found that in a third of individuals, itch persisted between 4 weeks and 3 months (median time to symptom resolution was 52 days) after successful mite and egg eradication 83 and clinicians should advise patients about this. (GPP)
The psychological impact of the diagnosis and the fear of social repercussions may lead to behaviours that can aggravate pruritis and skin irritation. For example, excessive cleaning of their body, furniture or clothing with toxic/irritating products. Non-recommended and unnecessary multiple applications of scabicide creams are often observed. • Treat post-scabies itch with crotamiton 10% cream (2–3 times a day) or emollients. (Grade 1C) • Provide advice regarding use of an emollient soap substitute and avoidance of soaps and shower gels, perfumed products, repeated applications of topical scabicides and other potential irritants. (GPP) • If the scabies mites have been eradicated and eczematous areas are present, then a potent topical corticosteroid ointment (e.g. mometasone furoate 0.1%, triamcinolone acetonide 0.1%, betamethasone valerate 0.1%) may be helpful. Nighttime use of a sedating antihistamine (e.g. chlorpheniramine or hydroxyzine) may assist with sleep and reduce scratching but does not treat the underlying pruritic mechanism. (GPP) • Itchy nodules, including those affecting genital skin, may persist for months as a post-scabies inflammatory reaction (post-scabies prurigo syndrome). If emollients, and topical corticosteroids are not helpful, we would recommend referral to a dermatologist for advice regarding treatment.
119
Secondary bacterial infection
• Superadded bacterial infections should be treated according to local antimicrobial resistance patterns and microbiological advice.
Evaluation of treatment failure
Reasons for an apparent non-successful treatment outcome with an effective anti-scabies treatment include:75,79,80,93,120 • Incorrect diagnosis; • Dermatitis secondary to the mite, topical agent or hygiene practices; • Incorrect application of the topical agent; • Failure to repeat treatment after 7–14 days; • Poor penetration of the agent into hyperkeratotic skin or nails; • Immunosuppressed host (greater disease severity/numbers of mites); • Re-infestation from untreated close contacts or potentially contaminated fomites; • Delusional infestation; • Ivermectin incorrectly prescribed or taken;
True treatment failure does occur, primarily because scabicide drugs are not 100% effective. A meta-analysis of RCTs from 2018 reported 74–93% clearance observed with permethrin and 68–86% with ivermectin. 84
A recent systematic review and meta-analysis, including RCTs and observational studies up to 2021, looked specifically at treatment failure prevalence and associated factors. 93 However, it was noted that there was no clear definition given for treatment failure in most studies and many referred to reinfestation, retreatment, recurrence of scabies, or persistent itching and classed these together as failures or non-successful treatment outcomes. The only clear conclusion was that taking a second dose of ivermectin resulted in significantly lower rates of failure than a single dose. Only three studies included a multivariable risk factor analysis to explore reasons for treatment failure. Most attributed non-successful outcomes to patient behaviour, drug administration compliance, environmental and disease severity related factors. Drug resistance, through mite susceptibility testing, was not assessed in any of the included studies.
Drug resistance
Whilst clinically significant drug resistance is documented in headlice,
121
there is still uncertainty regarding acaricides in human scabies.
122
Reduced clinical susceptibility to permethrin has been reported in Europe80,100 and to ivermectin in scabies-endemic areas.123,124 Molecular pathways have been elucidated for potential resistance in S. scabiei mites for both permethrin125–129 and ivermectin using animal models,123,124,130,131 but there are complexities with isolating and preserving sufficient mites for testing, and to date there is no confirmed evidence of these mutations having emerged in patients who have failed treatment.
122
• After confirmed failure of first-line treatments, combination treatment with oral ivermectin plus either permethrin 5% cream, malathion 0.5% liquid emulsion, or BB 25% liquid emulsion should be considered, ideally with supervised administration.80,83,86,122 (GPP) • Intensive treatment regimens with more frequent administration, such as those used in crusted scabies, might also be considered in conjunction with local dermatology and/or infectious diseases multi-disciplinary teams in recalcitrant cases.80,122 (GPP)
Guideline application
This guideline is designed primarily for use by clinicians working in level 3 sexual health services, for the management of individuals aged 18 years and over. However, persons aged 13–17 years can attend sexual health clinics in the UK independently/without parental consent so are also covered by this guideline. It may also be useful for those working in general practice, military medical centres and dermatology services.
At the time of writing, there have within the past 2 years been interruptions in the supply of all recommended and alterative regimens for the treatment of scabies, at different times and places across the UK. This may, in part, have been caused by a rapid rise in the number of cases of scabies seen in many countries after the relaxation of public health measures that were implemented in 2020-21 to control the spread of Coronavirus disease 2019 (COVID-19). Delays in obtaining treatment may lead to clinically significant delays in treating the index patient and their contacts. There is a substantial cost difference between the two recommended regimens, with ivermectin tablets incurring a higher cost than either permethrin cream or malathion liquid emulsion.
The guideline committee therefore recognises that treatment decisions may need to be made on pragmatic or cost grounds, with variations between different locales changing over time. These guidelines are intended to summarise best practice based on available evidence.
Tracing and treatment of contacts
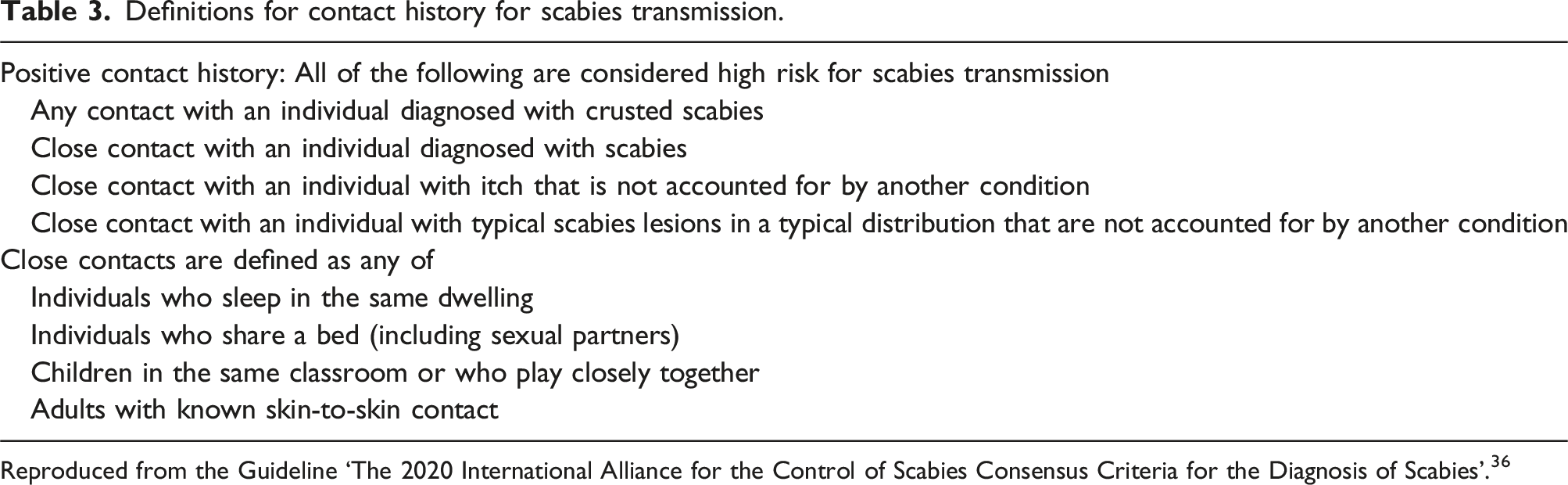
Contact tracing for specific STIs should be performed according to BASHH guidelines (https://www.bashh.org/guidelines), with reference to look back periods. Clinicians should inform patients about the importance of partner notification, and this can be carried out by the patient themselves in most cases. The 2020 IACS
36
definitions for positive contact history and close contact are presented in Table 3. • Contact tracing and notification of partners, household members and other close contacts from the previous 2 months prior to the onset of symptoms should be undertaken.132,133 (GPP) • Where possible, co-ordinate the treatment of index case and ongoing contacts to break cycle of transmission. ‘Ongoing’ contacts may include current sexual partners, household members, carers and other close contacts through skin-to-skin contact or fomite sharing. This may involve referral to general practitioners, community pharmacies and other sexual health services.132,133 If applicable, inform patients that permethrin can be bought over-the-counter. (GPP) • Contact your local health protection team if two or more epidemiologically linked cases occur within an 8 week period involving a closed setting (e.g. a care home, residential facility or prison).
78
(GPP) • Provide advice regarding laundry and other fomite decontamination measures, alongside treatment recommendations.
78
• An individual case-by-case risk assessment is recommended to take into account the severity of infection in the index patient and the likely exposure risk to potential contacts.
78
• Contacts should be treated, even if asymptomatic, given that it can take 6 weeks to develop symptoms. We recommend that they are given first-line treatments and follow laundry and other fomite decontamination advice, as per cases. (GPP). • Clinicians should advise patients to avoid sexual activity and other close skin-to-skin contact until both they and their current contacts have used treatment, followed laundry and other fomite decontamination advice and waited at least 24 hours after completing the first 12-h application of permethrin, or at least 24 hours after taking the first dose of ivermectin.
80
Both index and contacts should complete full treatment with two doses used 7–14 days apart. (GPP) Definitions for contact history for scabies transmission. Reproduced from the Guideline ‘The 2020 International Alliance for the Control of Scabies Consensus Criteria for the Diagnosis of Scabies’.
36
Auditable outcome measures
• All patients with suspected or confirmed scabies should receive an appropriate diagnosis code for audit purposes. (performance standard 95%). • People with suspected or confirmed scabies should be treated with two doses of a recommended first-line treatment regimen (performance standard 95%). • Individuals presenting with scabies should be provided with written information about the condition and its management (performance standard 95%); for example patient information leaflets on scabies from BAD
81
or from PCDS.
82
• Testing for other STIs where scabies is suspected to have been sexually transmitted should be offered (performance standard 95%).
Recommendations for further research
• There is a need to develop sensitive and specific diagnostic tests to support clinical diagnosis of scabies (e.g. a PCR test that could be utilised in clinical settings). • There is a need for a standardised outcome measure for treatment success in scabies that is clinically meaningful, reproducible across a range of clinical and research settings, and shares common criteria with previous RCTs. There is currently no standard definition of treatment failure. • Many recommended interventions for scabies have not been studied in RCTs, and some have never been studied in any controlled observational studies. The following could be considered for future work: o Clinical trials in which malathion lotion is an intervention (vs permethrin and ivermectin); o Trials of second-line treatment regimens, in which participants have recently been treated and experienced treatment failure, relapse or re-infection; o Clinical trials comparing spinosad cream to standard of care (rather than placebo or ‘vehicle’ cream); o Studies estimating the effectiveness of laundry and other fomite decontamination and quarantining methods currently recommended to improve long term cure rates. • Improved surveillance data beyond simple case-finding in outbreaks and sexual health clinic settings. No data are currently collected on rates of persistent symptoms, scabies re-treatment or ivermectin usage. Enhanced surveillance data, including outcomes of repeat treatments for scabies or alternative diagnoses made, would help to identify trends and clarify the situation regarding potential resistance to first-line treatments for scabies. • Research into testing drug susceptibility of mites and developing commercial methods for doing this (e.g. genetic typing of selected multiple targets), which are feasible with smaller numbers of mites than required for current phenotypic testing or can be performed on non-live mites.
Qualifying statement
The recommendations in this guideline may not be appropriate for use in all clinical situations. Decisions to follow these recommendations must be based on professional clinical judgement, consideration of individual patient circumstances and available resources.
All possible care has been undertaken to ensure specification of the correct dosage of medication and route of administration. However, it remains the responsibility of the prescribing clinician to ensure the accuracy and appropriateness of the medication they prescribe.
Review arrangements
An author group will be invited by the BASHH CEG to review and revise the guideline in 2030 using the BASHH framework for guideline development. However, addenda may be issued sooner than 2030, particularly if relevant new data are available relating to testing or treatment options.
Supplemental Material
Supplemental Material - British Association for sexual health and HIV national guideline on the management of scabies in adults 2025
Supplemental Material for British Association for sexual health and HIV national guideline on the management of scabies in adults 2025 by Georgina Morris, Lewis Haddow, Parameswaran N Sashidharan, Amber Savary-Trathen, Suneeta Soni, Charlotte Bigland, Hasan Mirza and Stephen L Walker in International Journal of STD & AIDS
Footnotes
Acknowledgements
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All members of the guideline writing committee completed the BASHH conflict of interest declaration and submitted it to the CEG. No authors had any relevant conflicts of interest to declare, and the content of the guideline is not attributed to any organisation they are associated with.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Editorial independence
This guideline was commissioned, edited, and endorsed by the BASHH CEG without external funding being sought or obtained. All members of the guideline writing committee completed the BASHH conflicts of interest declaration detailed below at the time the guideline’s final draft was submitted to the CEG.
Membership of the clinical effectiveness group
Supplemental Material
Supplemental material for this article is available online.
Notes
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.