
Abstract
Leishmaniasis is a tropical disease caused by protozoa belonging to the group of Leishmania species. Visceral leishmaniasis, diffuse cutaneous leishmaniasis, and atypical forms of cutaneous leishmaniasis are common in acquiring HIV. We report a case of atypical cutaneous leishmaniasis (CL) in a person living with HIV.
Introduction
The protozoan parasite Leishmania is highly prevalent in many areas of the world. 1 Leishmaniasis is transmitted to humans by the bite of a sandfly, and disease progression can be influenced by host immunity. 2 In Morocco, both acquired immunodeficiency syndrome (AIDS) and leishmaniasis are prevalent, posing significant public health concerns. 3 Co-infection results from the geographical overlap between cases of these two infections. 3 Co-infection can manifest as atypical clinical forms, which may occur before or after treatment, potentially resembling postkala-azar dermal leishmaniasis lesions. 4 Visceral leishmaniasis, diffuse cutaneous leishmaniasis, and atypical forms of cutaneous leishmaniasis are common in people living with HIV. 5 We report a case of atypical cutaneous leishmaniasis (CL) in a person living with HIV.
Case presentation
A 23-year-old man was diagnosed with HIV in 2024 following the discovery of neuromyelitis optica. His initial viral load was 134,000 copies/ml (5.13 Log), and his CD4 count was 8/mm3. He was classified as stage B3 according to the CDC classification and was started on antiretroviral therapy (ART) consisting of two nucleoside reverse transcriptase inhibitors (lamivudine and tenofovir) and an integrase inhibitor (dolutegravir).
One month after initiating ART, his condition worsened, with the appearance of disseminated skin lesions spreading across the entire body. Dermatological examination revealed multiple papules and papulonodules, some umbilicated and others covered with hemorrhagic crusts, predominantly on the trunk, back, and arms (Figure 1(a)). Additional lesions were observed in the retroauricular region and scrotum. Dermoscopy showed whitish streaks and follicular plugs (Figure 1(b)). Despite the skin involvement, the patient remained in good general condition, with no fever or weight loss, and he reported no history of insect bites. (a) Clinical examination: multiple papules and papulonodules, some umbilicated and others covered with hemorrhagic crusts, predominantly on the trunk, back, and arms. (b) Dermoscopy: whitish streaks ( blue arrow), follicular plugs (yellow arrow) on erythematous background.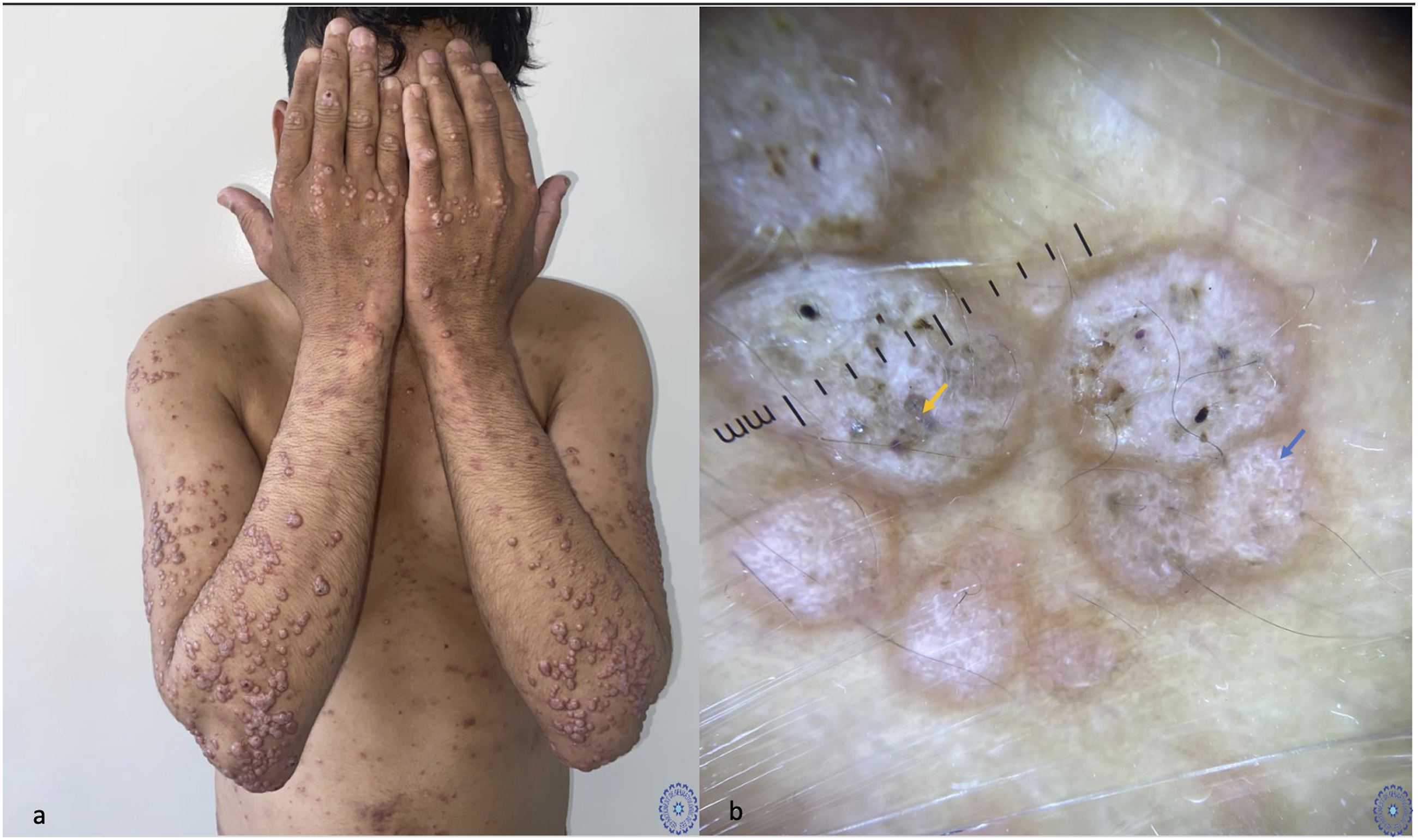
A skin biopsy and smear confirmed the diagnosis of cutaneous leishmaniasis (Figure 2). A sternal puncture was performed, revealing multiple Leishmania bodies along with 6% blasts. The radiological assessment revealed mild, homogeneous splenomegaly, with a splenic longitudinal axis measuring 14.5 cm and no focal lesions. Complete blood count, liver function tests, and renal function tests were within normal limits. The controlled viral load was measured at 40 copies/ml. A diagnosis of cutaneous leishmaniasis with probable expansion to the bone marrow was established, and the patient was started on meglumine antimoniate. After 4 weeks without clinical improvement, treatment with amphotericin B is planned. (a) Skin biopsy: HES G x 630. A dense and polymorphic inflammatory infiltrate consisting of diffuse lymphoplasmacytic and histiocytic components is observed. These histiocytes contain small oval-shaped bodies within their cytoplasm corresponding to “Leishmania” bodies (Giemsa + staining). There is an absence of epithelioid granulomas and giant cells. (b) Skin smear showing Leishmania bodies.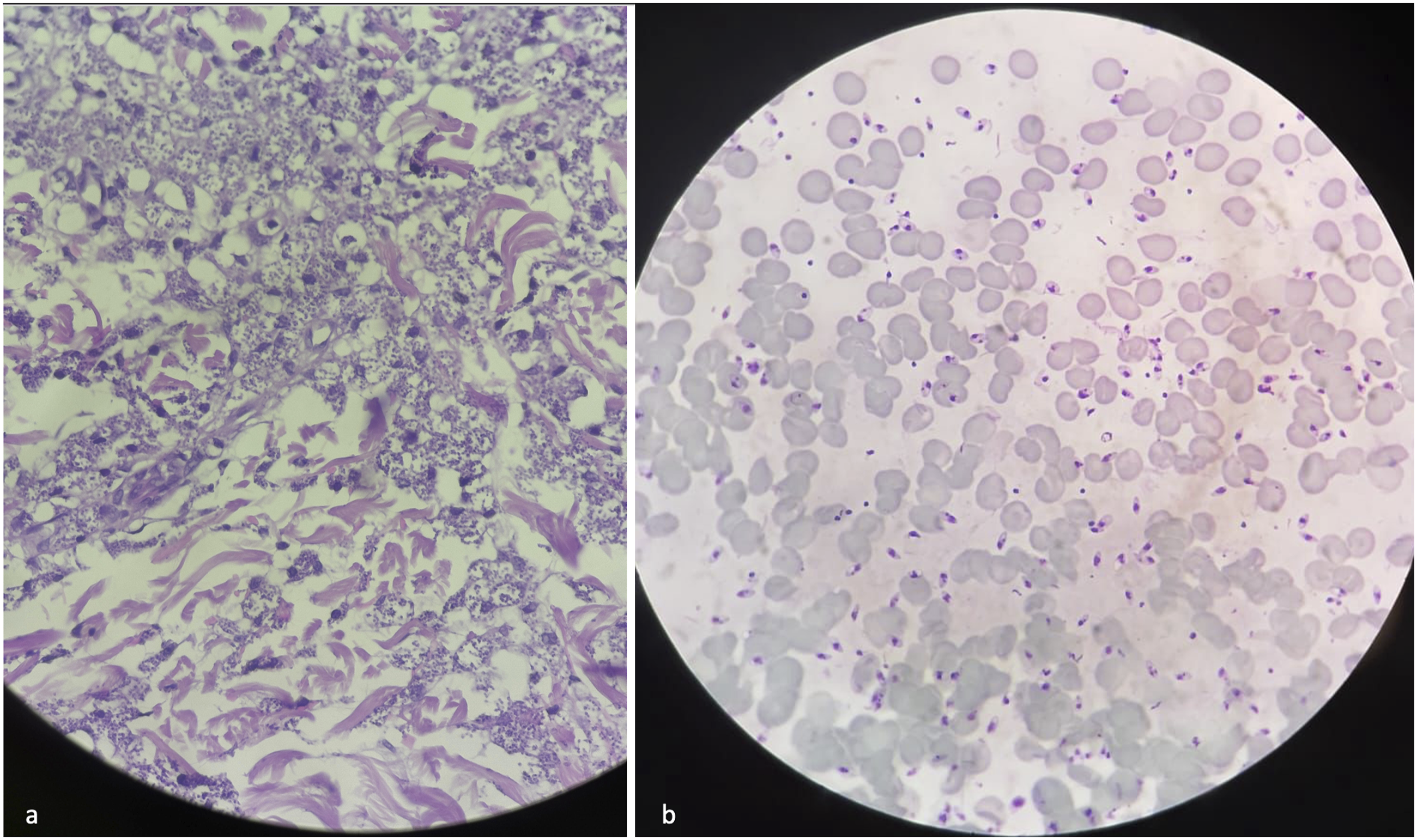
Discussion
Leishmaniasis is a tropical infection caused by an intracellular parasite of the genus Leishmania, transmitted to humans by sandflies. 6 In an immunocompetent host, CL classically presents as a solitary nodule at the inoculation site, which ulcerates and heals with scarring 5 Leishmania and human immunodeficiency virus coinfection is an emerging global issue. Leishmaniasis is the third most common parasitic infection in people living with HIV after Toxoplasma gondii and Cryptosporidium parvum. 7 In Brazil and Morocco, approximately 9% and between 3% and 25% of patients with visceral leishmaniasis (VL), respectively, have been reported to be living with HIV and leishmaniasis. 8 This co-infection results from the geographical overlap between cases of these two infections.3,9 Leishmania species can cause a wide range of cutaneous lesions in persons living with HIV, including localized cutaneous, mucosal, and mucocutaneous forms, post-kala-azar dermal leishmaniasis (PKDL), and diffuse cutaneous forms, 10 as observed in our patient. These atypical cutaneous manifestations may result from a shift from a predominantly T-helper 1 response to a T-helper 2 response or as a hyperinflammatory reaction associated with immune reconstitution inflammatory syndrome (IRIS).11–13 A 2015 review of 34 cases reported a mean interval of 4 months between the initiation of ART and the onset of leishmaniasis, with a range from 6 days to 9 years. 14 In our case, IRIS was considered a possible etiology of diffuse CL due to the worsening of the patient’s skin condition 1 month after initiating ART and the reduction in viral load. Clinical studies have shown that leishmaniasis accelerates the progression to AIDS by increasing the viral load, thereby reducing the life expectancy of persons living with HIV-1. This synergistic interaction between the two pathogens weakens the immune response by targeting similar host immune cells. In co-infected patients, the exhaustion of cellular and humoral responses to Leishmania increases the risk of disease progression following infection. 1 Based on these data, two hypotheses can be proposed to explain the diffuse cutaneous form with medullary involvement in our patient. The skin involvement could be due to parasitic dissemination from a quiescent visceral localization, given the patient’s severe immunosuppression, or it could represent the primary site with cutaneous and medullary dissemination as part of IRIS. The diagnosis of leishmaniasis in our patient was a significant challenge, as several differential diagnoses were considered, including cryptococcosis, diffuse molluscum contagiosum, and even lepromatous leprosy. This observation highlights the atypical clinical presentation of leishmaniasis in persons living with HIV and stresses the importance of considering this diagnosis in any unusual cases in endemic areas. Furthermore, atypical forms of cutaneous leishmaniasis should warrant HIV testing.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.