
Abstract
Background
The antimicrobial resistance of Neisseria gonorrhoeae and the high prevalence of asymptomatic extragenital infections are a worldwide concern. This research investigated whether gonorrhea can be transmitted from the oral cavity to the anorectal tract among men who have sex with men.
Purpose
The aim of this research is to find plausible relationships regarding the probability of gonococcal transmission from the oral cavity to the anorectal tract among MSM.
Research Design
A research question was defined using the P.I.C.O. strategy (population, intervention or exposure, comparison and outcome), where the target population is MSM, the intervention is exposure to contaminated oral cavity/saliva, the control is the absence of exposure, and the outcome is the acquisition of GC. The eligibility criteria included observational studies involving men who have sex with men, regardless of sexual orientation, aged 16 or older, screened for oropharyngeal and rectal gonorrhea, and examining the role of oral fluids in transmission. Studies involving partners previously diagnosed with urogenital gonorrhea or reporting consistent condom use during receptive penoanal sex were excluded to avoid urethral-to-anorectal transmission bias.
Study Sample
The databases employed were PubMed, Scopus, Web of Science, EBSCO, SciELO, and the Virtual Health Library (VHL). A total of 383 studies were identified, however, only 6 were included.
Data Collection and/or Analysis
According to the Newcastle-Ottawa Scale (NOS), two studies were “very good,” two “good,” and two “satisfactory”. Most studies described a complete methodology according to Strengthening the Reporting of Observational studies in Epidemiology (STROBE).
Results
Differences in diagnostic methods, methodologies, and variables limited the findings. While the results do not confirm transmission from the oral cavity to the anorectal tract, they suggest its possibility. Further research is needed to better understand this transmission route.
Conclusions
Transmissibility of gonorrhea from oropharyngeal via to the anorectal tract cannot be totally establish. However, evidence suggested the existence of this gonorrhea transmission. The fact that men with rectal gonorrhea continue to appear, even in contexts of condom use or the absence of receptive penoanal sex, brings the importance of cases monitoring and the establishment of preventive strategies.
Introduction
Gonorrhea (GC) is a sexually transmitted infection (STI) of worldwide concern, commonly reported and affecting individuals of all sexes. 1 The prevalence of gonorrhea is disproportionate among men who have sex with men (MSM).2,3 In fact, oropharyngeal (OPG), anorectal (ARG) and urogenital gonorrhea (UGG) among MSM was reported to be 8.5%, 15.0% and 6.81% respectively.4,5 Young individuals aged 24 years or younger and those with multiple casual sexual partners are most affected in this population.2,6–8
Gonococcal transmission occurs through direct inoculation of infected secretions during sexual intercourse between three anatomical sites in individuals with penises: the urethra, oropharynx, and rectum. 1 Extragenital infections of GC are generally asymptomatic and potential transmitters9,10 with high viable gonococcal loads11–14 with the duration of untreated infections until spontaneous elimination being approximately four to 12 months.15,16 Urethral infection, in turn, is generally symptomatic, with an incubation period of two to 8 days.1,17–19
Among authors and international clinical protocols, there are various considerations regarding the modes of transmission (e.g., urethra - anus, anus - oropharynx, oropharynx - oropharynx). Current public health strategies in countries such as Brazil and the United States are based on the traditional paradigm that the urethra performs a central role in the transmission of gonorrhea, primarily through sexual practices.20–22 Australia follows a different approach, proposing that the high prevalence of this infection is explained by the oropharynx as the primary source of transmission, that is, through saliva in situations such as French kissing and sexual practices (oral, orogenital, use of saliva as a lubricant, etc.). 23
The oropharynx may perform a crucial role in understanding the transmission of gonorrhea among MSM and its multiple antimicrobial resistances. 23 Most of these infections are asymptomatic, drug action at this site is less effective, and there is genetic material exchange of Neisseria gonorrhoeae (NG) with various commensal species of the same genus, including antibiotic resistance genes. 24 Genomic analyses have demonstrated that resistant strains are transmitted between sexual partners. 25 Discoveries indicate that NG can be cultured from rectal swabs, oropharyngeal swabs, and expectorated saliva in a significant proportion of patients positive for the infection at these sites, and that there is a substantial bacterial DNA load in these samples.11,12,26 However, it is uncertain to what extent kissing and saliva contribute to the transmission of gonorrhea.18,27
Little is known and discussed regarding the contributions of sexual practices involving the oral cavity and saliva in the transmission of NG,13,28 which leads to the belief that they are safe and would not pose health risks, 28 except in the condition of visible and obvious lesions. 29 The effectiveness of interventions against transmission at each specific site is highly uncertain given the possibility of additional transmission routes. 30 This understanding is crucial for predicting the effectiveness of interventions.12,30 Given the discovery of a considerable load of gonococci in saliva,12,13 it is presumed that any sexual activities involving it, which are frequent among MSM,28,29,31 may carry the infection. The aim of this research is to find plausible relationships regarding the probability of gonococcal transmission from the oral cavity to the anorectal tract among MSM.
Methodology
The present study constitutes a systematic review. A research question was defined using the P.I.C.O. strategy (population, intervention or exposure, comparison and outcome), where the target population is MSM, the intervention is exposure to contaminated oral cavity/saliva, the control is the absence of exposure, and the outcome is the acquisition of GC. The research question defined was: “Among men who have sex with men, can gonorrhea be transmitted from the oral cavity to the anorectal tract?”
The databases employed were PubMed, Scopus, Web of Science, EBSCO, SciELO, and the Virtual Health Library (VHL). Initially, a search pattern was established using Mesh terms, synonyms, and terms commonly used by authors, linked with Boolean connectors: (“neisseria gonorrhoeae” OR gonorrhoea OR gonococcal) AND (transmission OR sexual OR risk) AND (pharyngeal OR oropharyngeal OR pharynx OR oropharynx OR mouth OR saliva OR throat OR rimming OR anilingus OR “receptive anal practices”) AND (anal OR anorectal OR rectal OR anus) AND (“men who have sex with men” OR msm OR homosexual OR bisexual OR “gay men”). This pattern was employed and modified according to the specificities of each database, without limitations on date or language.
The search engines were organized according to a logical sequence: presenting results from studies on gonorrhea (1st group), its transmission or sexual risk factors associated with transmission (2nd group), infection in the oropharynx (3rd group), to the anorectal tract (4th group), among “men who have sex with men” (5th group). The expressions “rimming”, “anilingus”, and “receptive anal practices” were included to encompass studies relating these sexual risk practices to transmission. The term “men who have sex with men” (MSM) in the fifth group is the most recent, utilized, and appropriate for defining the sexual interest group of the research, given that sexual orientation (homosexual, bisexual, etc.) is subjective, although used in search engines as it was more commonly employed in the 20th century.
The eligibility criteria encompassed observational studies whose target population consisted of men from the group “men who have sex with men,” regardless of sexual orientation, aged 16 years or older, screened for oropharyngeal and rectal gonorrhea, and which investigated the involvement of oral cavity fluids in the transmission process. To exclude the possibility of infection from the urethra to the anorectal tract, studies that included groups of partners previously diagnosed with urogenital gonorrhea or with reports of consistent condom use for receptive penoanal sex were excluded.
Two reviewers conducted independent searches in the databases and determined the final sample based on an analysis of titles, abstracts, and full texts that met the eligibility criteria.
The quality of the studies included in the final sample was assessed using the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) instrument and the Newcastle-Ottawa Scale (NOS). For data analysis, prevalence and incidence ratios of anorectal gonorrhea, oropharyngeal gonorrhea, and urogenital gonorrhea reported in the studies and the risk factors for the acquisition of GC were collected: partners diagnosed with oropharyngeal gonorrhea and practices including receptive anal sex, digital-anal or fisting, and oroanal activities, as well as the use of saliva as a lubricant. Additionally, confounding factors such as the number of sexual partners, HIV status, and condom use were collected. The data were organized, categorized, and analyzed using Excel spreadsheets and presented in tables and figures.
Results
The search results are detailed in Figure 1. A total of 1011 articles were found in the databases: Web of Science (174), Scopus (252), PubMed (269), EBSCO (95), and VHL (221). No results were obtained from searches in the SciELO database. After the removal of 628 duplicate studies, 383 remained. These were analyzed according to the eligibility criteria, resulting in a final analytic sample composed of six studies18,32–36 with data reported in English language. Detailed search result.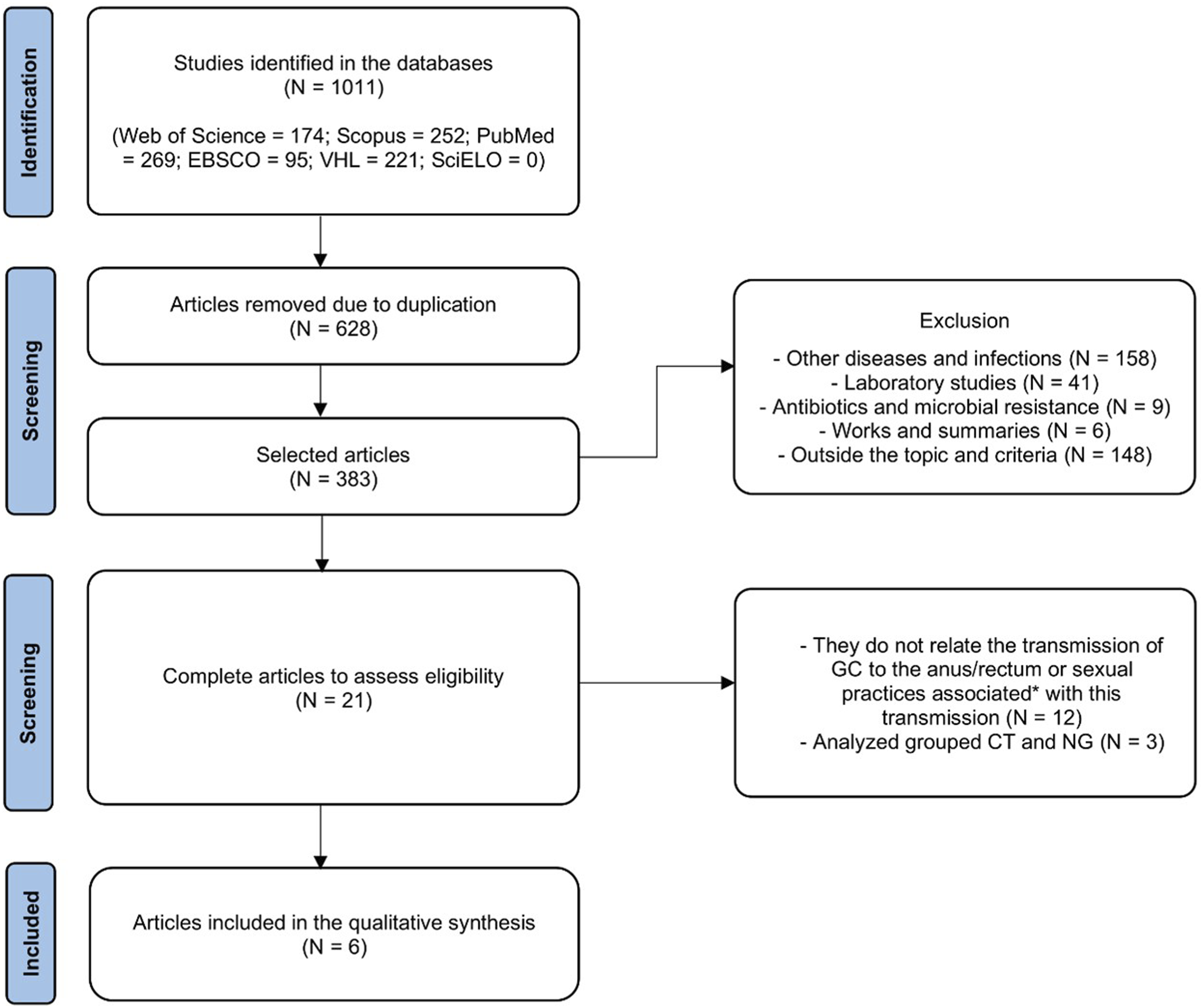
Quality analysis of studies according to STROBE and NOS criteria (score) for observational studies.
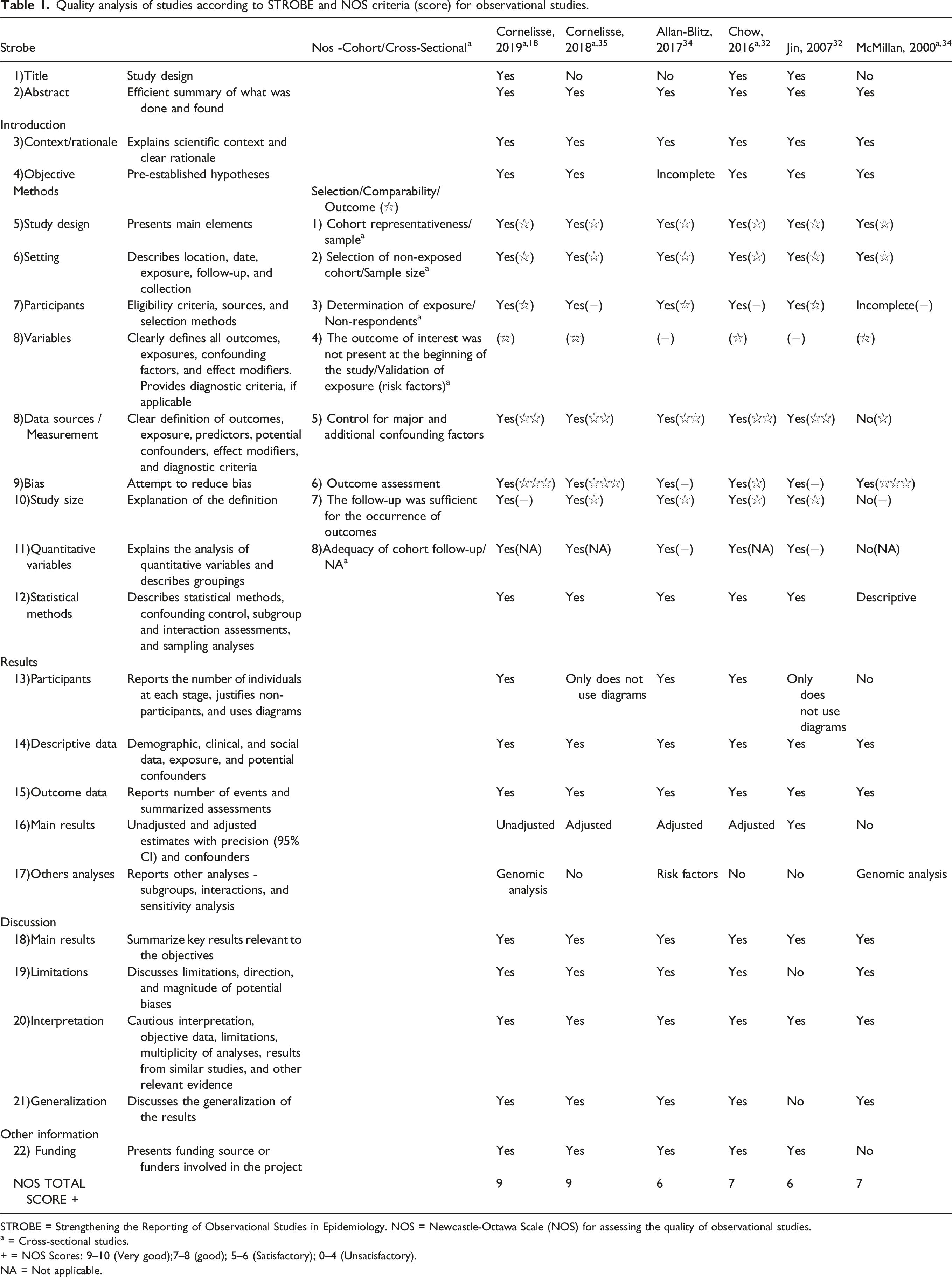
STROBE = Strengthening the Reporting of Observational Studies in Epidemiology. NOS = Newcastle-Ottawa Scale (NOS) for assessing the quality of observational studies.
a = Cross-sectional studies.
+ = NOS Scores: 9–10 (Very good);7–8 (good); 5–6 (Satisfactory); 0–4 (Unsatisfactory).
NA = Not applicable.
Description of methodological characteristics and results of the final sample.

OPG = Oropharyngeal gonorrhea, ARG = Anorectal gonorrhea, UGG = Urogenital gonorrhea, UC = Urethral chlamydia, RC = Rectal Chlamydia, NAAT = Nucleic acid amplification test, CI = Confidence interval, OR = Odds Ratio, aOR = Adjusted Odds ratio, aIRR = Adjusted incidence rate, aHR = Adjusted risk ratio.
In this sample, the prevalences found for anorectal gonorrhea ranged from 2.9% to 4.8%, for oropharyngeal gonorrhea from 1.7% to 6.2%, and for urogenital gonorrhea was 3.3%. Meanwhile, the incidences for anorectal gonorrhea ranged from 3.0 to 28.1 cases per 100 person-years, for oropharyngeal gonorrhea was 21.3 cases per 100 person-years, and for urogenital gonorrhea was 3.5 cases per 100 person-years. In two studies,32,35 the presence of anorectal gonorrhea was associated with HIV in the same individual.
Four studies18,32,34,36 analyzed sexual risk practices for gonorrhea. One study 32 found an association with the use of saliva during penoanal sexual practice conducted in the 3 months prior to testing, and another 33 with digital-anal, fisting, and oroanal practices in the 6 months prior. In two articles,32,33 gonorrhea was significantly associated with unprotected penoanal sexual practice.
Three studies32,33,35 sought evidence regarding the transmission of gonorrhea from the oral cavity to the anus (oropharyngeal gonorrhea to anorectal gonorrhea). In these studies, three sites (anorectal tract, oropharynx, and urethra) were screened in couples to detect extragenital infections that could not have been caused by urethral infection, and to determine if among these partners there would be the presence of anorectal gonorrhea and oropharyngeal gonorrhea, but without urogenital gonorrhea. It was demonstrated in all three studies that in the absence of urethral infection, men with anorectal gonorrhea commonly had partners with oropharyngeal gonorrhea; however, the studies did not indicate the direction of transmission. Two studies32,35 conducted phylogenetic analyses of strains isolated from sexual partners positive for oropharyngeal gonorrhea and anorectal gonorrhea and found a high concordance between the pairs.
Discussion
In the current study, half of the investigations demonstrate that men with anorectal gonorrhea had steady partners with oropharyngeal gonorrhea, excluding the involvement of urogenital gonorrhea.18,34,36 These studies did not seek to identify the origin of the infection; however, it was assumed that the direction of transmission is from mouth to anorectal tract. This hypothesis is supported by a previous study by Cornelisse et al.,, 27 in which no association was found between active oroanal sex as a risk factor for oropharyngeal gonorrhea, and other evidence of detection and cultivation of NG in saliva samples,12,13 a frequent element in practices among MSM.28,29,31,37,38
In our sample, two studies identified an association between anorectal gonorrhea and the use of saliva 32 or the oral cavity during sexual practices. 33 Jin et al., 33 did not include saliva in their analysis, whereas Chow et al., 32 when including saliva, did not detect a significant association value for oroanal sex. Studies discussed that the volume of infected saliva introduced into the anorectal tract by the tongue during oroanal sexual practice or by penile or digital penetration with saliva lubrication could be responsible for this transmission.28,32,37,38
The involvement of saliva in sexual practices is an important factor for discussions on sexual health, as it contains various microorganisms, including NG, and its presence is particularly notable in relationships among men, whether due to kissing, the use of saliva as an anal lubricant, oroanal sex, or other sexual fetishes such as spitting during the sexual act (knowing as “sialophilia”). Studies have discussed the role of saliva in the rectal transmission of the disease, commonly active in sex among MSM, which can come into direct contact with the anus in large quantities.28,37,38 Fairley et al., 23 proposed that the incidence of anorectal gonorrhea among MSM could occur due to the involvement of saliva in ororectal sex or as a lubricant, practices common among MSM.28,29,31,37
In our study, prevalences reported for anorectal gonorrhea, oropharyngeal gonorrhea and urogenital gonorrhea were low. Studies that focus in oral transmission of gonorrhea reported similar results. For instance, pharyngeal, urethral, and anal gonorrhea was reported to be 1.7%, 2.3%, and 2.9%, respectively 39 and 3.8%, 2.3% and 0% at oropharynx , anorectum and urethra. 40 These results could be related to the relatively short lived of the bacteria in oropharyngeal sites reported to be clear in approximately 6 weeks to 12 weeks. Thus, lower prevalences by oral transmission, for example by kissing, were expected. 40
On the other hand, studies have identified higher prevalences of asymptomatic gonorrhea at extragenital sites3,9,41,42 compared to urogenital gonorrhea. Furthermore, the acquisition of anorectal gonorrhea still occurs in a scenario of frequent condom use for anal sex, 43 and studies have reported these findings. According to the authors, the increase in disease cases cannot be explained solely by urethral transmission, and most infections would not be identified if screening were conducted only for urogenital gonorrhea or based on symptoms or sexual history.41,44–46 Ong et al., 17 found in their research that 11% of urethral infections would be missed if only symptomatic cases were diagnosed. Marcus et al., 46 reported that with exclusive urethral screening, the loss of gonorrhea cases was high (95.2%). All this reinforces the paradigm proposed by Fairley et al.,, 23 in which oropharyngeal gonorrhea would be the main culprit for the transmission of GC at the three sites, including the oropharynx.
Biopsychosocial factors, such as the culture in each country or region, can influence outcomes. For instance, in the metropolitan region of Australia 32 and in San Francisco, United States, 28 studies indicate that oroanal sex and the use of saliva as a lubricant are common practices among MSM. Additionally, a younger age, below 35 years, can also be a risk factor associated with GC.47,48
There remains a limited number of studies with research samples that constitute a small analysis pool. The discussion regarding the origin of anorectal gonorrhea began in 1991 with Tomlinson et al.,, 49 but it was not until 2000 34 that the first article based on this inquiry was published. The second study was released in 2007, 33 but it took another 9 years for a new investigation to emerge. From 2016 to 2019, a study was published each year18,32,35,36; however, no further studies have been conducted since then.
Studies found that having more than one partner in the last 3 months and among seropositive HIV patients increased the risk of gonorrhea. 50 On the other hand, studies50,51 showed that the use of condom during intercourse reduced the risk of having gonorrhea by almost 61%. 50 In our study, these confounding factors were collected to reduce bias. However, considering the nature of such information, there exists the possibility of inaccurate responses.
Several limitations can be noted. There is a need for standardization in diagnostic methods and methodologies used across studies. Some used culture methods, while others utilized NAAT techniques. Compared to culture, NAAT techniques have higher sensitivity in detection, which could lead to differences in the value of the associations found.52–54 Most studies include various variables, with no reports of standardized instruments being used. Another limitation is the exposure time employed in the sexual history of participants. Anorectal gonococcal infections are commonly asymptomatic, lasting approximately 12 months until complete resolution by the immune system, 16 thus making it impossible to estimate the duration of the infection until diagnosis. Therefore, data collection in cross-sectional studies over a shorter interval could be subject to variations.
Given the higher prevalence of extragenital gonorrhea among MSM,3,9,41,42 there is a public health concern, particularly in countries where these cases are not routinely identified or where detection relies solely on self-reported sexual behaviors. To confirm oral-to-anal transmission, future research should prioritize well-designed longitudinal studies that incorporate microbiological typing methods, such as whole-genome sequencing, to establish transmission pathways. Additionally, studies should systematically collect behavioral data, including detailed sexual practices, partner networks, and frequency of exposures, alongside biological sampling from multiple anatomical sites over time. Standard methods that include more specific and validated tools, to collect data such as risk variables, are recommended to achieve more precise results and a better comprehension of disease in that risk population.
Conclusion
Transmissibility of gonorrhea from oropharyngeal via to the anorectal tract cannot be totally establish. However, evidence suggested the existence of this gonorrhea transmission. The fact that men with rectal gonorrhea continue to appear, even in contexts of condom use or the absence of receptive penoanal sex, brings the importance of cases monitoring and the establishment of preventive strategies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.