
Abstract
Background
This study aimed to assess HIV prevalence and associated sexual behaviors among immigrant men who have sex with men (MSM) in Brazil and Portugal, recognizing the elevated vulnerability of this population due to sociocultural and structural barriers.
Methods
A cross-sectional online survey was conducted between January 2020 and May 2021 with 2033 immigrant MSM. Participants were recruited using snowball sampling through dating applications. Data were self-reported and analyzed to identify associations between sexual behaviors and HIV status.
Results
The overall HIV prevalence was 11.7%. Higher-risk sexual practices were frequent, including receptive anal intercourse and having multiple sexual partners. Conversely, low adoption of preventive behaviors such as sexual abstinence and non-penetrative sex was observed. Condomless sex was commonly justified by trust in partners or recent negative HIV test results. Factors independently associated with unprotected sex included being versatile or receptive in anal sex and not disclosing HIV status on dating apps. Gaps in HIV prevention knowledge and engagement were also identified.
Conclusions
Immigrant MSM in Brazil and Portugal experience a high burden of HIV and engage in behaviors that increase their risk of infection. Cultural and structural barriers—such as language difficulties, limited healthcare access, and stigma—contribute to inadequate prevention practices. These findings highlight the urgent need for targeted, culturally competent public health interventions to expand access to HIV prevention strategies and reduce transmission risk in this underserved population.
Keywords
Introduction
A decade ago, the Joint United Nations Programme on HIV and AIDS (UNAIDS) released a Fast-Track strategy, including the 90-90-90 targets, which aimed to accelerate global efforts to end the AIDS epidemic by 2030, 1 however, none of these targets were achieved. On the other hand, the number of new infections has declined from 2.1 million in 2010 to 1.5 million in 2020. 2 Despite considerable improvements since the peak of infections in 1998, there is still much to be done as the world renews its commitment for the next targets by 2030, i.e. fewer than 200,000 new infections and 95-95-95 targets. 3
HIV prevention continues to be a critical concern in global public health, necessitating specific focus on populations at a disproportionate risk of infection. 4 As of the end of 2022, approximately 39 million people globally were living with HIV, with an estimated prevalence of 0.7% among adults aged 15–49 years. 5 The disparity in the epidemic’s impact is pronounced, with the WHO African Region experiencing the most severe challenges. 6 Yet, vulnerability to HIV transcends geographic boundaries, affecting various demographic groups, particularly men who have sex with men (MSM), who have HIV prevalence rates surpassing those of the general population. 7
Immigrant MSM face unique challenges, including significant barriers to accessing healthcare and preventive services, exacerbated by stigma, discrimination, and linguistic or cultural differences. Therefore, it is essential to understand the risk behaviors and factors associated with HIV transmission in this population to design more effective and tailored health interventions and policies.
Geographic mobility has been identified as a factor that influences sexual behaviors and access to healthcare, subsequently impacting HIV transmission rates. 8 Despite this, there is a notable gap in research on immigrant MSM, particularly in recent major migration destinations such as Portugal and Brazil. 9 The high HIV prevalence observed among these groups, coupled with behaviors like unprotected sex, the use of sexualized drugs, and insufficient prevention knowledge, highlights a pressing public health issue that warrants urgent attention.7,10
In Portugal and Brazil, the rates of HIV prevalence among MSM, and especially among immigrant MSM, reflect not just public health challenges but also intricate socioeconomic and cultural dilemmas. In 2021, MSM in Portugal had an HIV prevalence of 19.9%, representing 38.8% of the country’s new HIV diagnoses. 11 Significantly, immigrant MSM accounted for the majority of these new cases, underscoring the particular challenges this community faces. 11
In Brazil, the situation has proven even more alarming, with an estimated HIV prevalence among MSM of 25.4%. Within this group, migrant MSM exhibited a prevalence of 17.8%, representing 14% of all new HIV cases among MSM in the country in 2020.1–5 The high prevalence rates in both countries can be attributed to complex factors, including unprotected sex and obstacles to accessing information and prevention services, further intensified in contexts of migration. Furthermore, a lack of awareness about prevention strategies, such as pre-exposure prophylaxis (PrEP) and post-exposure prophylaxis (PEP), exacerbates the situation, underscoring the need for comprehensive research and tailored, sensitive interventions.
Hence, this study aims to explore the prevalence of HIV and the factors associated with unprotected sex practices and the lack of knowledge regarding preventive strategies among immigrant MSM in Portugal and Brazil. By doing so, we intend to establish a robust basis for developing prevention and treatment strategies that meet the unique needs of this population, thereby contributing to the global fight against the HIV epidemic.
Methods
Study design
This study is a cross-sectional online survey that included MSM in Portugal and Brazil, aged 18 years and older, from January 2020 to May 2021.
Population and sample
A sample size calculation was conducted using G*Power software (version 3.1.9.7) to determine the necessary sample size for the study. The calculation considered the population of men, an allowable standard error of 3%, a confidence level of 95%, and an assumed prevalence of 50%.
It is noted that when it is not feasible to determine the true prevalence of the phenomenon of interest from local or national literature, an assumed prevalence of 50% is utilized. This value maximizes the sample size, and its use is not problematic. 12
Participants were those who identified as men (cisgender or transgender), had engaged in sexual relations with another man in the previous 12 months, were 18 years or older, and were immigrants residing in Portugal or Brazil. For the purposes of this study, an immigrant was defined as any individual who self-reported being born outside of Portugal or Brazil, regardless of their current nationality or length of residence in the country.
Data collection procedures
To recruit research participants, we employed the “snowball” sampling method, adapting it to the virtual environment, a technique previously validated for the MSM population.13,14
In this approach, participants help in recruiting other individuals with similar characteristics through their social networks and contacts, by sending an invitation to participate. Considering that our study was carried out in two countries across different continents, we intentionally selected the first 30 participants with varied social and demographic characteristics. This included age range, region or district of residence within the country, race/skin color (white/non-white), income, and education level, to facilitate data generalization.13–15
To reach the initial 30 participants without necessitating travel by researchers, two of our researchers—cisgender men who identify as MSM, properly trained and calibrated with each other—created a public profile on two geolocation-based dating apps (Grindr and Hornet) to identify the “seeds.”
The choice to use Grindr and Hornet to identify the initial study participants stems from these apps’ widespread recognition as popular platforms within the MSM community, offering a large user base. The researchers approached the first individuals who were available online on each of the two apps, ensuring they met the predefined inclusion criteria for the study and conformed to the seed generalization criteria as recommended by previous studies.16,17 After contacting each seed, we sent them a link to the survey and instructed them to invite other MSM from their social networks until the required sample size was achieved through a strategy of dissemination.
Study outcomes
This study focuses on three self-reported primary outcomes: the prevalence of HIV among immigrants MSM residing in Portugal and Brazil; unprotected sex in the past 30 days, which was considered the sexual intercourse without condom use; and a lack of awareness regarding two or more HIV prevention strategies (pre-exposure prophylaxis - PrEP, post-exposure prophylaxis - PEP, and undetectable equals untransmittable - U = U).
The selection of lack of awareness regarding two or more HIV prevention strategies (PrEP, PEP, and U = U) as the study outcome is based on the relevance of these tools for HIV epidemic control. Limited knowledge of these strategies impairs HIV prevention, particularly among vulnerable and immigrant populations, who may face greater barriers to access and information. Assessing this outcome helps to identify gaps in the reach of combination prevention policies and guides more appropriate educational and public health interventions. Awareness of these strategies supports the adoption of preventive measures and reduces the risk of HIV infection.
Data collection instruments
The survey was hosted on the SurveyMonkey platform, which includes security features to ensure only one response per Internet Protocol (IP) address. To validate the survey form, a face-content validation process was conducted with 10 subject matter expert judges. A pre-test with 10 participants was also carried out to evaluate the clarity of the form.
The survey collected sociodemographic data, such as age, education, place of residence, gender identity, and relationship status. Questions about participants’ practices regarding the disclosure of HIV status on dating apps, previous STI diagnoses, and history of HIV testing, either lifelong or in the last 12 months, were included. Subsequent sections of the survey explored sexual practices, covering HIV prevention measures used during sex, sexual activities with partners living with HIV, participation in group sex (three or more people simultaneously), preferred sexual positions, recent engagement in unprotected sex, drug use during sexual encounters or sex under the influence of drugs, participation in sexual activities in public places, and specific practices such as bareback sex, double penetration, or fisting, as well as the frequency of seeking health services. We provided clear and understandable explanations for less common or potentially unfamiliar terms, such as “cruising,” 18 “double penetration (DP),”14,19 “chemsex,” 16 and “gouinage”,19,20 to ensure participants’ comprehension. To define “chemsex,” participants were asked if they had used illicit drugs immediately before and/or during sexual activities in the last 12 months. Those who answered affirmatively were presented with a multiple-choice list to specify the drugs they used. 16
Data analysis
Statistical analyses were conducted using IBM SPSS software, version 27.0 (SPSS Inc., Chicago, IL, USA). Pearson Chi-square test with the Monte Carlo Permutation method (999 simulations with a 95% confidence level) was utilized to select variables for inclusion in the multivariate models for the outcomes of unprotected sex in the last 30 days and unawareness of at least two HIV prevention strategies. A p-value <.20 served as the statistical criterion for inclusion.
The analysis’ final stage involved multivariate modeling to identify factors independently associated with unprotected sex in the last 30 days and unawareness of at least two HIV prevention strategies. The selected regression model was the generalized linear Poisson model with a log-linear link function, chosen because the prevalence of both outcomes exceeded 10%. Adherence to the Poisson distribution was confirmed using the Kolmogorov-Smirnov test (p-value >.05), and the assumption of equidispersion was verified.
Adjusted prevalence ratios (aPRs) and their 95% confidence intervals (CI95%) were calculated using a hybrid method of parameter estimation, a robust variance estimator, and type III analysis for testing model effects. An omnibus test determined whether the final multivariate model more effectively explained the outcomes compared to a model including only the intercept, with statistical significance set at 5% (p-value <.05). The Akaike Information Criterion (AIC), deviance, and log-likelihood were used to determine the best-fitting model, with lower values indicating a better fit. The significance of the aPRs for variables in the final model was analyzed using the Wald Chi-square test. Variables with a p-value <.05 in the final model were considered significant.
Ethical aspects
The project was approved by the Ethics Committee of the Ribeirão Preto School of Nursing, Brazil, under opinion number 4,163,084, and by the Research Ethics Board of the Institute of Hygiene and Tropical Medicine of the University of Lisbon, Portugal, with opinion number 12.19. Free and informed consent was obtained online.
Results
Baseline characteristics of participants, Brazil and Portugal, 2020-2021.

Most participants were cisgender men (n = 1986; 97.7%), young adults under 25 years old (n = 1174; 57.7%), and had at least 12 years of schooling (n = 1493; 73.4%). Regarding relationship status, 70.7% were single (n = 1438), and 94.6% reported having casual sexual partners (n = 1924). In terms of sexual position, 47.5% identified as versatile (n = 965), 36.4% as receptive (n = 741), and 11.4% as insertive (n = 232).
Concerning the use of dating apps, 61.0% (n = 1241) reported meeting four or more partners through these apps in the last 6 months. The majority did not disclose their HIV serostatus on apps (n = 1491; 73.3%), and 73.5% (n = 1495) had two or more sexual partners in the last 30 days. Regarding prevention, 85.1% (n = 1731) knew at least two HIV combination prevention strategies, while 14.9% (n = 302) were unaware of two or more strategies. Unprotected sexual behavior (sex without a condom in the last 30 days) was reported by 41.0% (n = 833) of participants.
The prevalence of previous diagnoses of chlamydia, gonorrhea, and syphilis was 11.4% (n = 232), 13.7% (n = 279), and 15.8% (n = 321), respectively. Sexual practices such as double penetration (n = 552; 27.2%), group sex (n = 822; 40.4%), chemsex (n = 643; 31.6%), and cruising (n = 238; 11.7%) were also reported. Only 2.3% (n = 46) of participants reported that their last sexual partner was HIV positive.
Multivariate analysis of factors independently associated with unprotected sex in the last 30 Days and unawareness of at least two HIV prevention strategies, Brazil and Portugal, 2020-2021.
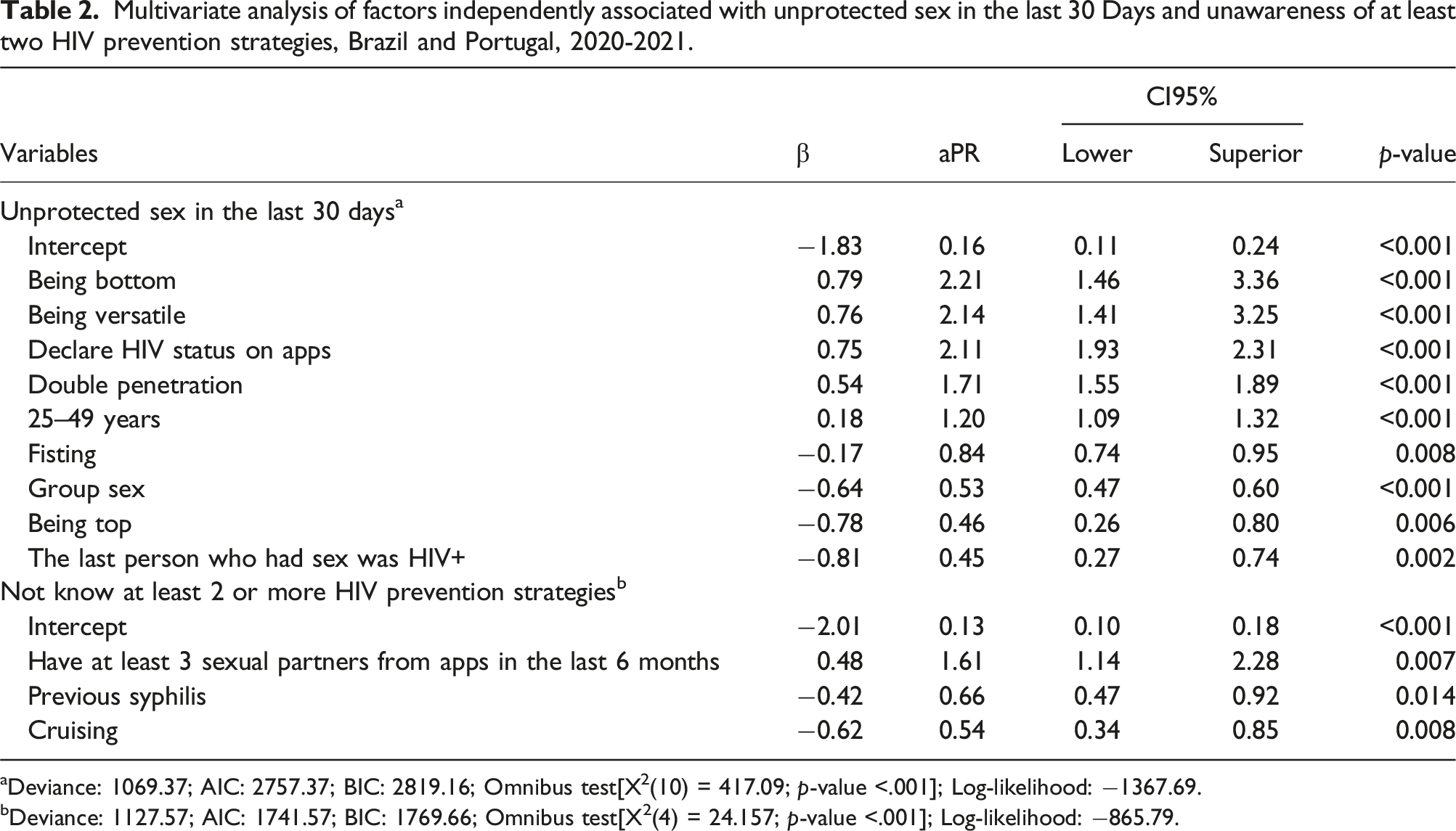
aDeviance: 1069.37; AIC: 2757.37; BIC: 2819.16; Omnibus test[X2(10) = 417.09; p-value <.001]; Log-likelihood: −1367.69.
bDeviance: 1127.57; AIC: 1741.57; BIC: 1769.66; Omnibus test[X2(4) = 24.157; p-value <.001]; Log-likelihood: −865.79.
Seven variables were included in the final model for unprotected sex [X2(10) = 417.09; p-value <.001]. Key associations included higher prevalence with being receptive or versatile, disclosing HIV status on apps, and double penetration. Lower prevalence was linked to having an HIV-positive partner, being insertive, and group sex. For unawareness of HIV prevention strategies [X2(4) = 24.157; p-value <.001], having four or more sexual partners from apps was linked to higher prevalence, while prior syphilis diagnosis and cruising were linked to lower prevalence.
Discussion
The findings of this study highlight an HIV prevalence of 11.7% among immigrant men who have sex with men (MSM), a significantly high figure, especially when compared to previous studies conducted within the general population.21–24 This elevated prevalence can be attributed to a variety of factors, including the complexities inherent in the migratory scenario, such as linguistic, cultural, and socioeconomic barriers, which may hinder access to essential health information and services. Additionally, the stigma associated with HIV and sexual orientation can lead to marginalization within the healthcare system, thereby decreasing the likelihood that these individuals will seek or receive appropriate preventive and therapeutic care.25,26
The high HIV prevalence among immigrant MSM carries significant implications for this group, highlighting the urgent need for inclusive public health policies and intervention programs that are tailored to the specific needs of migrants and sexual minorities. 4
An analysis of sexual behaviors and prevention strategies among immigrant MSM uncovers several critical factors contributing to HIV vulnerability within this population. 27 The prevalence of practices such as receptive anal sex and having multiple sexual partners underscores the urgent need for targeted sexual education interventions. These interventions should not only promote the consistent use of condoms but also address negotiating safe sexual practices within this community. These behaviors, widely recognized as posing a higher risk for HIV transmission, reflect challenges in the effective implementation of prevention measures. 28
Furthermore, the low utilization of traditional preventive methods and the excessive reliance on known partners or those who have recently been tested for HIV point to a concerning lack of knowledge about HIV transmission methods and risk perception.29,30 This gap in knowledge suggests that existing public health campaigns may not be reaching the immigrant MSM population, potentially due to linguistic, cultural, or access barriers. Research supports this, indicating that immigrants, especially those from marginalized communities, may lack access to sexual health information.21,23,24
The findings reveal critical aspects of sexual health and HIV prevention behaviors among immigrant MSM in Brazil and Portugal. The prevalence of unprotected sexual relations in the last 30 days among these individuals was 41.0%, while the unawareness of two or more HIV prevention strategies was 14.9%. These data highlight significant vulnerabilities associated with the immigration environment and emphasize the need for specific interventions targeted at this population.
The high prevalence of unprotected sex can be understood within the context of various dimensions. Firstly, factors such as being receptive or versatile in anal sex were linked to a higher prevalence of unprotected sexual practices.31–33 This may reflect dynamics of vulnerability and power negotiation within sexual relationships, where communication about safe practices and the use of condoms can be especially challenging. The disclosure of HIV serostatus on dating apps, along with a higher prevalence of unprotected sex, highlights how risk perception can be influenced by the digital environment, where a sense of anonymity or trust in shared information can lead to risky behaviors.
The findings of this study, in which sexual practices such as group sex and fisting were associated with a lower prevalence of unprotected sex, contrast with a study that identifies these practices as risk factors for STIs and HIV. 34 One possible explanation for this result is social desirability bias, which is common in research on sexual behavior, where participants tend to underreport behaviors considered stigmatized due to embarrassment or fear of judgment. 35 This phenomenon can lead to intentional concealment of these practices, resulting in an apparent inverse association between higher-risk practices and unprotected sex in self-reported data. Therefore, it is important to consider that the actual prevalence of unprotected sex during these practices may be underestimated due to respondents’ reluctance to report behaviors perceived as socially undesirable. On the other hand, practices such as group sex and fisting may indicate a greater awareness of risks and adherence to prevention strategies in these specific contexts.9,23
To mitigate these vulnerabilities, developing inclusive, accessible, and tailored sexual education and HIV prevention programs that meet the needs of these populations is crucial.36–38 This includes promoting condom use, disseminating information about PrEP and PEP, and fostering an environment that encourages open communication and the negotiation of safe sexual practices. 39
Overall, these findings underscore the need for a holistic and multifaceted approach to HIV prevention among immigrant MSM, taking into account the cultural, social, and individual aspects that influence sexual behavior and access to healthcare. The literature suggests that successful interventions must provide not only information and resources but also address the deep-seated stigma, discrimination, and isolation that many immigrant MSM experience. Therefore, for HIV prevention strategies to be effective, they must be tailored to the specific needs of this population, ensuring they are inclusive, accessible, and culturally sensitive.
Limitations
The cross-sectional nature of the study means that the associations identified between sexual behaviors, knowledge about HIV prevention, and other factors cannot be interpreted as causal relationships. Additionally, the use of the “snowball sampling” technique, especially in a virtual environment, may have led to a biased selection of participants, thus limiting the generalizability of the findings to all MSM immigrants in Portugal and Brazil. Although this technique allows for reaching a hard-to-access population, the participants recruited may not fully represent the diversity of this community.
Furthermore, the self-reporting of sexual and health behaviors may have introduced a social desirability bias, with participants potentially underreporting or inaccurately reporting risky behaviors or STI diagnoses.
Conclusions
The prevalence of HIV among MSM immigrants residing in Portugal and Brazil, as well as the practice of unprotected sex, was found to be high. The factors associated with the outcomes of unprotected sex and unawareness of HIV prevention methods were significant. Practices posing a higher risk of exposure to HIV and other STIs, such as receptive anal sex and double penetration, were associated with a greater prevalence of unprotected sex.
Supplemental Material
Supplemental Material - HIV prevalence and prevention behaviors among immigrant men who have sex with men in Brazil and Portugal
Supplemental Material for HIV prevalence and prevention behaviors among immigrant men who have sex with men in Brazil and Portugal by Alvaro Francisco Lopes de Sousa, Caíque Jordan Nunes Ribeiro, Guilherme Reis de Santana Santos, Matheus Vinícius Cardoso Santos, José Flávio Cerqueira dos Santos Júnior, Emerson Lucas Silva Camargo, Ana Paula Morais Fernandes, Talita Morais Fernandes, Liliane Moretti Carneiro, and Isabel Amélia Costa Mendes in International Journal of STD & AIDS
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) – Funding Code 001. The funders had no role in the design, analysis, or conclusions of the study.
ORCID iDs
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.