
Abstract
Introduction
Azithromycin is first-line for uncomplicated Mycoplasma genitalium (Mgen) treatment in UK and European guidelines, however the rates of azithromycin resistance have increased significantly in recent years leading to higher rates of treatment failure. This study aims to review the disease epidemiology to guide service improvement.
Methods
We undertook a retrospective case note review of 1036 persons treated for Mgen over 1067 Mgen-related attendances. We obtained data on demographics, site(s) of infection, antibiotic resistance, treatment regimen received and results of test of cure.
Results
71.1% (n = 759) patients received the recommended first-line regimen of doxycycline and azithromycin. Moxifloxacin is the recommended first-line management for macrolide-resistant or complicated infection. 15% (n = 155) patients received moxifloxacin alone as first-line treatment, and 6.9% (n = 72) patients received doxycycline and moxifloxacin dual therapy. 72.9% (n = 753) samples were successfully tested for macrolide resistance. Of these, 55.5% (n = 418) showed macrolide resistance. 20.6% (n = 7) showed fluoroquinolone resistance.
Conclusions
Resistance data show a macrolide resistance rate of 55.5% across our region, and at least 1 in 10 persons were inappropriately screened for Mgen. We propose a multi-pronged approach which includes strict adherence to testing criteria, local resistance testing, resistance-guided management as well as innovative approaches to improve test of cure rates.
Introduction
Mycoplasma genitalium (Mgen) is a sexually transmitted bacterium that predominantly affects the genitourinary tract, causing non-gonococcal urethritis (NGU) or cervicitis, as well as complicated urogenital infections such as epididymo-orchitis in men and pelvic inflammatory disease (PID) in women. It has also been linked to preterm birth and miscarriage. 1 The prevalence of Mgen in the general UK population is 1–2%, rising to 38% in individuals attending sexual health clinics. 2
The management of Mgen is challenging for several reasons. Firstly, the absence of a cell wall makes penicillins and cephalosporins ineffective treatment against Mgen. Only a few antibiotic classes retain therapeutic activity against mycoplasmas, including tetracyclines, macrolides, fluoroquinolones, and streptogramins (e.g., pristinamycin). Of these, macrolides are the first-line treatment for uncomplicated Mgen in UK and European guidelines.1,3
Due to limited effective treatment options available, current UK guidelines recommend testing based on symptoms, or for current sexual partners of people infected with Mgen. 1 Guidelines advise that all Mgen positive specimens should be tested for macrolide resistance associated mutations (MRAMs), but this is logistically challenging as results are often not received in a timely manner to allow for prompt and definitive treatment decision making. In this audit, we describe the epidemiology of Mgen, MRAMs and fluoroquinolone resistance associated mutations (QFRAMs) in our region and review our current management against UK guidelines to aid service improvement.
Methods
Thirteen sexual health clinics across Cheshire, Manchester, and Merseyside participated in this audit. We undertook a retrospective case note review of all attendees with a positive Mgen NAAT from September 2022 to December 2023. Patients were identified using the Genitourinary Medicine Clinical Activity Dataset (GUMCAD), a mandatory STI surveillance system in the UK, with Mgen coded as C16. Data abstracted from electronic patient records included demographics, reason for testing, site(s) of infection, antimicrobial resistance reports, treatment regimen received, and test of cure results.
For all clinics, Mgen NAAT was performed on the Roche Cobas 8800 and samples for antibiotic resistance testing were sent to the United Kingdom Health Security Agency (UKHSA) sexually transmitted infections reference laboratory where inhouse real time polymerase chain reaction (RT-PCR) was undertaken (targets Mgen adhesin P1 (MgPa) and glyceraldehyde-3-phosphate dehydrogrenase (gap)). 2 Sanger sequencing was then performed for region V of the 23S rRNA gene (MRAM) and in some samples the QRDR of the parC gene or gyrA gene (FRAMs).
All data were anonymized, and identifiable individual-level data were removed. We performed descriptive analysis of the collated data using Microsoft Excel. We also used the Statistical Package for the Social Sciences (SPSS version 29) utilising chi square testing to assess association between antimicrobial regimen received and TOC rates.
Results
We reviewed 1067 samples from 1036 patients. A total of 528 persons were seen in Liverpool and Cheshire, and 508 were seen in Manchester.
Population characteristics
Half of patients identified as male (n = 524, 50.6%), with 49.1% (n = 509) identifying as female and 0.3% (n = 3) being non-binary. The mean age was 28 years (range 15–80) with 39.3% (n = 407) patients aged under 25 years. The majority (n = 702, 67.8%) were of white ethnicity, and heterosexual (n = 848, 81.9%).
Screening indications
A total of 812 persons with symptoms (76.1%) were appropriately tested for Mgen, and 160 (15%) were appropriately tested as contacts of Mgen infection with 76.9% (n = 123) of these being asymptomatic. Ninety-five persons (8.9%) had Mgen testing performed for reasons outside UK guidelines, such as asymptomatic testing. 1
Site(s) of infection
The majority had genital infection (n = 1,025, 96.1%). Forty-one (3.8%) had rectal infection, and one person had dual site infection.
Macrolide and fluoroquinolone resistance
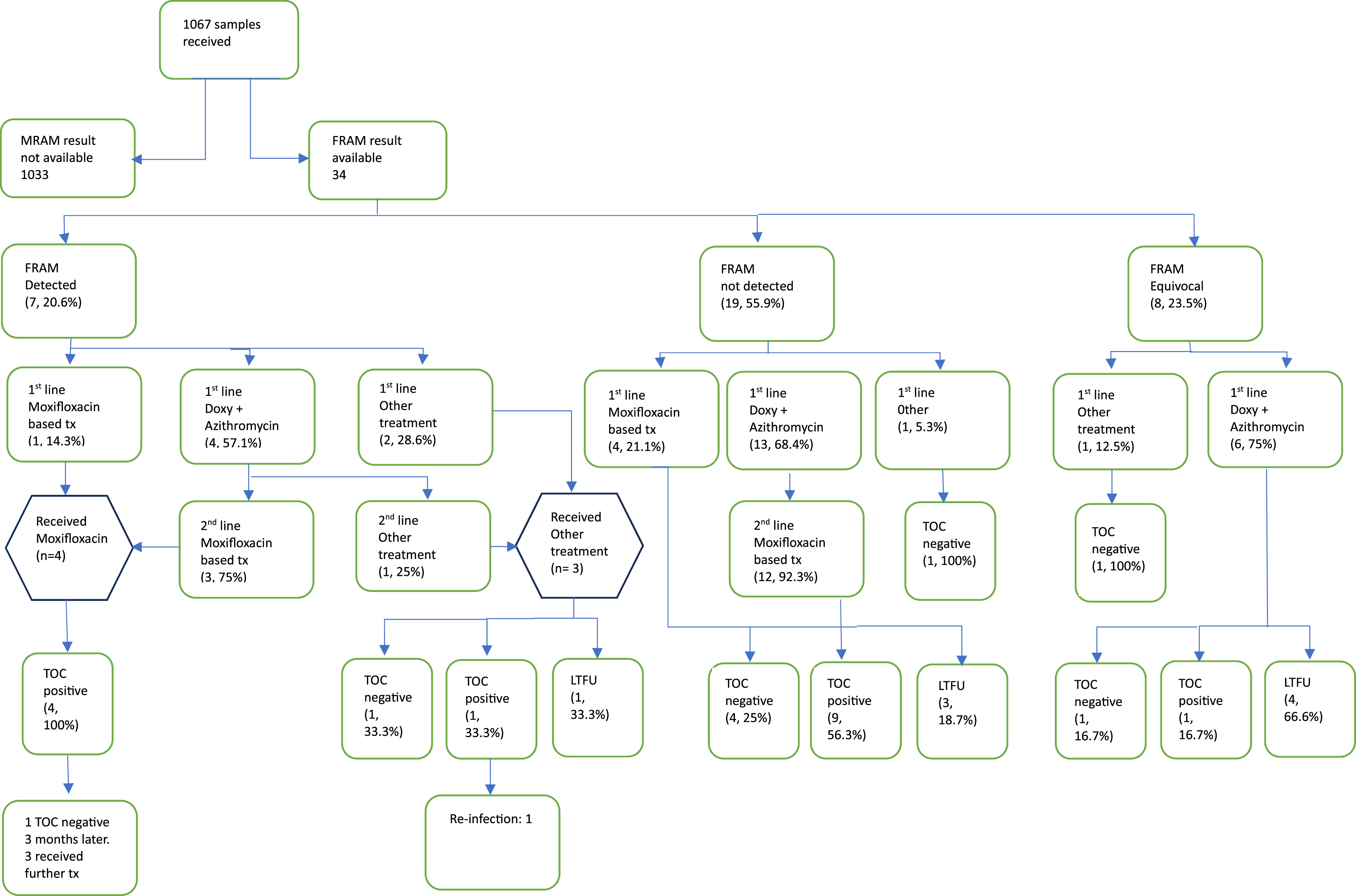
As summarised in Figure 1: Flow chart of clinical outcomes of MRAM-determined samples, 753 samples (72.9%) were successfully tested of which 418 (55.5%) had MRAMs detected. It was not possible to test 27.1% (n = 280) of samples due to factors such as low DNA titres. Routine fluoroquinolone resistance testing was available for a brief period at the start of the audit but was subsequently discontinued by UKHSA. Results were available for 3.3% (n = 34) of samples, as summarised in Figure 2: Flow chart of clinical outcomes of FRAM-determined samples. All 7 patients with FRAMs also had MRAMs. FRAMs included S83I (5 samples), D87 N (1 sample) D87Y (1 sample). One sample with a S83I mutation also had a G93 C mutation (of unknown significance). Flow chart of clinical outcomes of MRAM-determined samples. Flow chart of clinical outcomes of FRAM-determined samples.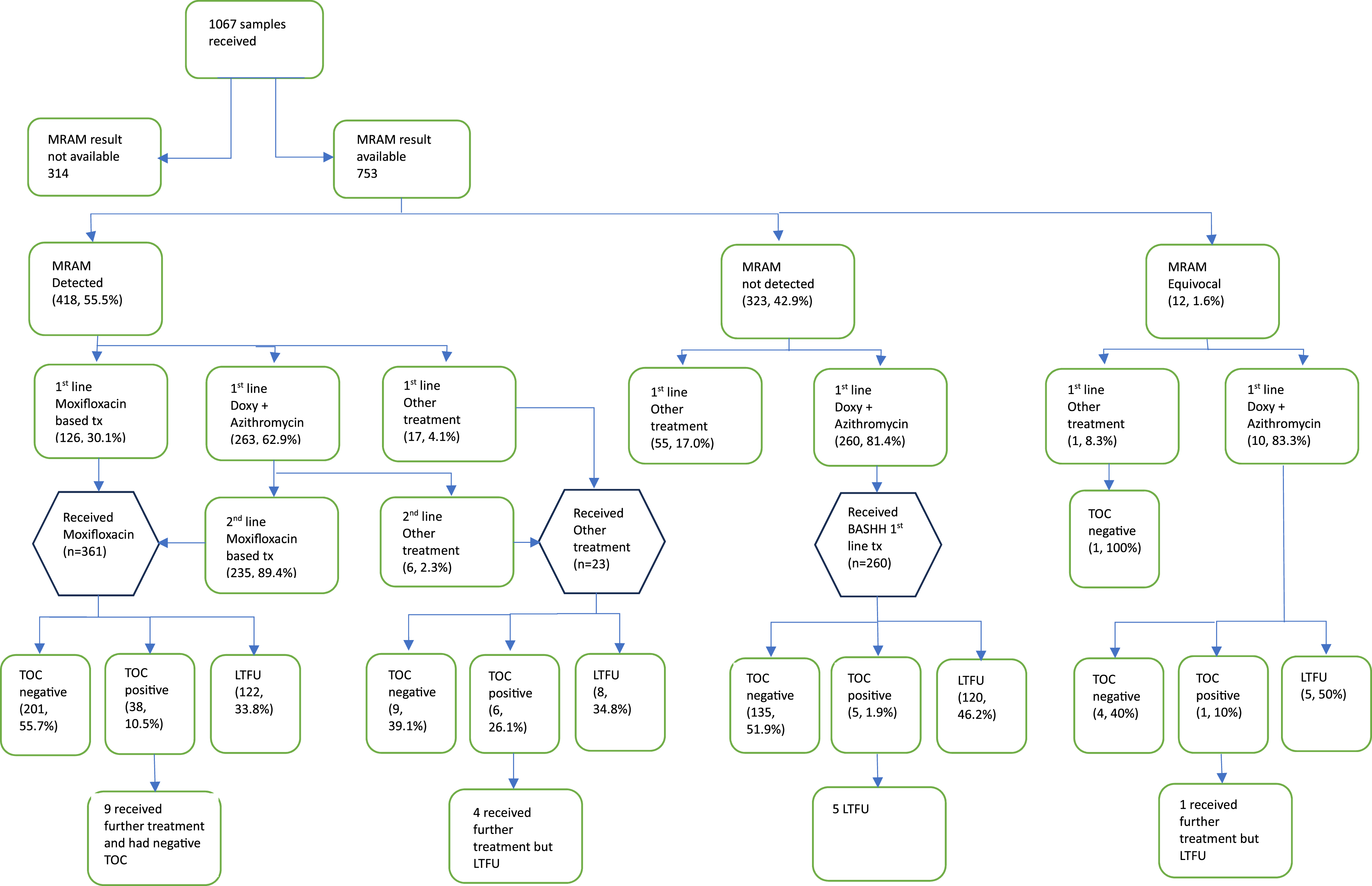
First line treatment regimen
Local guidelines in Merseyside and Cheshire clinics followed UK national guidelines (doxycycline plus azithromycin, or moxifloxacin), and clinics in Manchester followed USA national guidelines (doxycycline plus azithromycin, or doxycycline plus moxifloxacin).1,4 The Manchester clinics had consulted with the members of the UK guidelines writing group and were advised that doxycycline plus moxifloxacin was a reasonable strategy to try to preserve moxifloxacin effectivity.
The majority (n = 759, 71.1%) of patients received the recommended first-line regimen of doxycycline and azithromycin for uncomplicated infection. Fifteen percent (n = 155) of patients received moxifloxacin alone as first-line treatment for complicated infection, and 6.9% (n = 72) of patients received doxycycline and moxifloxacin dual therapy. Other regimens received included non-standard monotherapy regimens: doxycycline (n = 21), azithromycin (n = 14), minocycline (n = 7), doxycycline and pristinamycin (n = 3), and doxycycline and minocycline (n = 1). Thirty-four patients (3.2%) received no treatment.
Test of cure
A total of 599 patients (56.1%) had an available initial test of cure performed within 3 months of completing treatment. Of these, 86.6% (n = 519) were negative, and 13.4% (n = 80) were positive. Those with a positive TOC were demographically like the general population sample: 56.8% (n = 42) male, 73% (n = 54) heterosexual, and 70.3% (n = 52) white.
On subgroup analysis of TOC rates between those who received dual treatment (n = 36) versus moxifloxacin monotherapy (n = 84), there was no statistically significant difference between the groups on chi square testing (p = .75).
Second-line treatment regimen
Three hundred and six persons (28.7%) required second-line treatment due to macrolide resistance, antimicrobial intolerance, or treatment failure. Of these, 90.5% (n = 277) received moxifloxacin either as monotherapy (n = 159) or following pre-treatment with doxycycline (n = 118). Other regimens for second-line treatment included doxycycline & azithromycin (n = 18), minocycline (n = 7), doxycycline and pristinamycin (n = 2), pristinamycin monotherapy (n = 1), and azithromycin monotherapy (n = 1).
Third-line and fourth-line treatment regimens
Twenty-two patients (2%) required third-line treatment. Twelve (54.6%) received moxifloxacin, and five (22.7%) received minocycline. Other regimens included doxycycline & azithromycin (n = 2), and pristinamycin both as monotherapy (n = 2) and in combination with doxycycline (n = 1).
One patient required fourth-line treatment. Their treatment regimen consisted of doxycycline and azithromycin, followed by moxifloxacin, then pristinamycin, which was switched to minocycline after 3 days due to adverse effects.
Discussion
Our resistance data show a macrolide resistance rate of 55.5% across our region. Although this is lower than the national average of 62.2% reported by the Mgen Antimicrobial Resistance Surveillance, it remains high. 2 High rates of macrolide-resistant Mgen infection have been reported globally. For instance, rates of up to 66% have been reported in the Netherlands, and all 31 Mgen-positive samples in a study in Greenland demonstrated macrolide resistance.5,6
In our setting, 28.7% people diagnosed with Mgen required second-line treatment due to macrolide resistance, antimicrobial intolerance, or treatment failure. The implications of this are significant, potentially leading to increased costs due to extra prescribing and multiple patient reattendances, greater strain on sexual health services, risk of loss to follow-up, and higher patient dissatisfaction rates. We propose local resistance testing as a solution to this challenge for two reasons. Firstly, local testing ensures results are available to the clinician more quickly compared to the current arrangement of testing at a central reference laboratory with a turnover of 2–3 weeks. If results are available sooner, then patients can be counselled to wait for resistance results before commencing treatment. Unnecessary exposure to macrolides may contribute to further antimicrobial resistance and lead to adverse effects, such as gastrointestinal discomfort, which could be avoided if treatment were delayed until resistance reports were available. Available evidence shows that resistance-guided management can be cost-effective, reduces rates of treatment failure, and prevents overuse of fluoroquinolones.7,8
Equally worryingly, the rate of fluoroquinolone resistance in our cohort is 20.6%. Fluoroquinolone resistance testing is not routinely available, and therefore our data should be interpreted with caution due to our small sample size (n = 37). Fluoroquinolone resistance rates of 12.1% were reported in the latest MARS report, where all samples from reporting clinics were tested over a 2-month period. 2 Fluoroquinolone-resistant Mgen already presents a management dilemma for clinicians, and some opt for a trial of fluoroquinolone regardless of resistance status. More research is needed to determine the optimal management strategy for this patient cohort.
The 2018 guideline, current at the time of this project, recommends that all patients have a test of cure performed 5 weeks post-treatment to confirm microbiological clearance of infection and identify treatment failures, with a duty to report confirmed treatment failures to the UKHSA for surveillance purposes. 1 Our data show that only 56% of patients had a test of cure performed. The reasons for this high rate of nonattendance are unclear. However, it is possible that a home test kit, if available, may be a better testing option, as it does not require clinic attendance.
The 2025 UK guideline (currently in draft) is no longer recommending routine TOC, only advising TOC in individuals who remain symptomatic and where there is suspicion of persistent infection. 9 Given that microbiological cure can be challenging, especially in the presence of resistance associated mutations, the more pragmatic approach taken by the new UK guidelines seems sensible, despite the potential risk of the presence of ongoing antibiotic-resistant infection in some patients.
UK guidelines recommend moxifloxacin monotherapy where a fluoroquinolone is required, and this recommendation is supported by our findings of comparable microbiological cure rates among those who received moxifloxacin alone and those who received doxcycline and moxifloxacin. USA guidelines however continue to recommend doxycycline pre-treatment to preserve moxifloxacin effectiveness.1,4
At least 1 in 10 individuals in our cohort were inappropriately screened for Mgen. This is comparable with a UK national audit in 2022 where 8.6% of individuals did not have a guideline recommended or suggested reason for Mgen testing. 10 While Mgen screening is increasingly available, it is paramount that screening is reserved only for those meeting BASHH criteria. 1 We recommend strict screening criteria that discourages asymptomatic screening. This will help avoid unnecessary exposure to antibiotics, with the concomitant risk of driving further antimicrobial resistance.
Limitations
Our audit was geographically restricted to the Northwest of England and may not be generalizable to the rest of the UK or internationally. Resistance reports were not available for a small proportion of patients, due to the transfer of patient records from paper to electronic.
Conclusions
The high and rising rates of macrolide-resistant Mgen are an issue of public health concern, and clinicians are increasingly faced with challenges on how to address this. Reported fluoroquinolone resistance is currently low; however, we would not recommend fluoroquinolones as first-line treatment due to their side effect profile and the risk of disabling musculoskeletal and neuropsychiatric toxicity. In January 2024, the UK Medicines Regulator (MHRA) further limited fluoroquinolone use only to situations where other classes of antibiotics are inappropriate. 11 There are also wider issues to consider regarding the lack of large-scale data on baseline fluoroquinolone resistance, as well as expected increases in fluoroquinolone resistance with more prevalent use. We propose a multifaceted approach that includes strict adherence to testing criteria, local resistance testing, resistance-guided management, as well as innovative approaches to improve test-of-cure rates, such as home testing kits.
Footnotes
Acknowledgements
The authors wish to thank the technical teams at all sites for their help in extracting the required data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.