
Abstract
This guideline provides details on the pathology and clinical features of Mycoplasma genitalium infection and makes recommendations for diagnostic tests, treatment regimens and the health promotion principles needed for the effective management of infection, in people aged 16 years or older attending sexual health services. The guideline is primarily aimed at level 3 sexual health services in the UK, although it could also serve as a reference guide for sexually transmitted infections services at other levels. It is updated from the previous guideline published in 2018.
What is new in the 2025 guideline?
• An updated description of the complications associated with M. genitalium infection is included. • Indications for M. genitalium testing are now based on specific syndromes (instead of individual symptoms) and/or risk factors. There is reiteration that asymptomatic screening should not be undertaken. • The evidence base for recommended treatments is expanded in light of case reports, clinical series and systematic reviews published since the last version of this guideline. • Clinicians are advised to counsel patients on the risks of damage to tendons, muscles, joints and nerves, as well as significant psychiatric side effects including suicidal intent when moxifloxacin is used. • A test of cure (TOC) is no longer recommended for all patients with confirmed M. genitalium infection. Re-testing can be undertaken in individuals who remain symptomatic after treatment and when there is suspicion of persistent infection.
Introduction and methodology
Objectives
The guideline is primarily aimed at health care professionals seeing people aged 16 years or older in departments offering specialist level 3 care in sexually transmitted infection (STI) management within the United Kingdom. However, the principles of the recommendations can be observed across other levels of STI care providers. Non-specialist services may need to develop local referral pathways.
This guideline provides details on the pathology and clinical features of Mycoplasma genitalium infection, and offers recommendations on the diagnostic tests, treatment regimens and health promotion principles needed for the effective management of infection. Whilst the guideline is intended to summarise recommendations for best practice according to current available evidence, it is acknowledged that not all clinics will have ready access to M. genitalium detection and resistance testing because of logistical and cost issues.
Search strategy and methods
This guideline was produced according to specifications set out in the British Association for Sexual Health and HIV (BASHH) Clinical Effectiveness Group (CEG) ‘framework for guideline development and assessment’ (2015, updated 2020) accessed at https://www.bashh.org/_userfiles/pages/files/resources/2020_guidelines_framework.pdf.
This guideline has been updated by reviewing the previous BASHH national guideline for the management of infection with M. genitalium (2018) 1 and conducting a comprehensive literature search of publications from January 2017 to April 2024. Conference abstracts were updated when the published manuscript became available. The writing group formulated eleven ‘PICO’ questions (see Appendix 1) addressing the patient problem or population (P), intervention (I) (or aetiology/diagnosis/frequency/prognosis), comparison (C) and outcome(s) (O), which formed the basis for the literature search and article identification. The search was conducted using Medline, Embase, Cochrane library and National Health Service (NHS) Evidence databases and the broad search term ‘Mycoplasma genitalium’. All entries in the English language were reviewed, and if relevant the full text obtained. Age, country, and study design limits were included in the PICO criteria. ‘Grey literature’ included conference abstracts from International Union against Sexually Transmitted Infection (IUSTI), BASHH, British HIV Association (BHIVA), Interscience Conference of Antimicrobial Agents and Chemotherapy (ICAAC), Australasian Society for HIV, Viral Hepatitis and Sexual Health Medicine (ASHM) and European Society of Clinical Microbiology and Infectious Diseases (ECCMID) scientific meetings in the last 3 years.
The Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) system was used to assess the evidence and make recommendations (see Appendix 2) and consensus was reached on all recommendations.
Equality impact assessment
An assessment of the guideline and its recommendations was undertaken to ensure the principles of equality and diversity were adhered to and is available in Appendix 3.
BASHH has adopted an anatomical approach without assuming gender in the majority of guidelines and uses gender terminology in line with BASHH ‘Sexual health standards for trans, including non-binary, people’.
The terminology of ‘men’ and ‘women’ has been retained in a few instances relating to other guidelines, e.g., human papillomavirus vaccination and female genital mutilation.
Stakeholder involvement, piloting and feedback
The first draft was produced by the writing group and then circulated to the BASHH Clinical Effectiveness Group (CEG) for review using the the Appraisal of Guidelines, Research and Evaluation (AGREE) appraisal tool Appendix 4. The second draft of the guideline was posted on the BASHH website for wider consultation (2 months) and any comments received during the consultation period were reviewed by the authors and acted on appropriately. The document was also reviewed by a patient representative, target users and the public panel of BASHH, and their feedback was considered by the authors and used to inform the guideline. The final draft was presented to the CEG for review and piloting in sexual health clinics.
Once the guideline is published, the CEG will keep it under review should critical new evidence become available that affects the current recommendations. The guideline will be formally reviewed and updated, if necessary, every 5 years.
Epidemiology
Prevalence in the general population
In England, prevalence estimates of M. genitalium infection range from 1% to 2% in the general population, being slightly higher in women than men. 2 Amongst STI clinic attendees, prevalence ranges are higher, from 4 to 38%.3–6
Risk factors for infection
Similar to C. trachomatis, risk factors for M. genitalium infection include younger age, non
Sexual transmission
Transmission is primarily by genital–genital contact, but transmission by penile–anal contact has also been established following detection of organism in the anorectal compartment.8–11 As carriage in the oro-pharynx is uncommon, the relative contribution of oral sex is likely to be very small.12–14 The risk of transmission per coital act has yet to be determined but is likely to be less than that for Chlamydia trachomatis. 14
Coinfection with other sexually transmitted infections
As M. genitalium is transmitted through sexual contact, co-infections with other bacterial STIs such as C. trachomatis and Neisseria gonorrhoeae are common.15,16
An association between M. genitalium and HIV transmission and acquisition is biologically plausible and supported by some studies in Africa.6,17,18
Clinical features
Asymptomatic infection
The evidence suggests that the majority of people infected with M. genitalium in the genital tract do not develop disease.14,19,20 There are limited data to suggest that infection can be cleared spontaneously within a few months although persistence for up to 2 years is also reported.20,21 Current treatments are imperfect and associated with the development of antimicrobial resistance (AMR).22,23 There is no evidence that screening asymptomatic individuals will be of benefit, and indeed is likely to do harm at a population level. 24
Symptomatic infection
Signs and symptoms
Penile urethral infection
M. genitalium infection is unequivocally and strongly associated with non-gonococcal urethritis (NGU). Typically, the prevalence of M. genitalium in men with NGU is 15%–25% and in men with non-chlamydial nongonococcal urethritis (NCNGU) is 10%–35%. 25 M. genitalium is also associated with persistent and recurrent urethritis, where up to 40% of affected men may have M. genitalium detected. 26
The clinical presentation of M. genitalium urethritis is similar to other causes and thus clinical features of acute symptomatic NGU cannot be used to determine the infective aetiology.14,27–31 The commonest symptoms are discharge and urethral irritation. Although the proportion of infected men that develop symptoms is unknown, this is likely to be <10%. 14
Endocervical infection
Several studies support an association of M. genitalium infection in cisgender women with post-coital bleeding and cervicitis.32–34 Although other genital symptoms including vaginal discharge, odour, itch, dyspareunia and/or bleeding may be apparent during infection, studies have found no association with M. genitalium and their presence alone is not indicative of a testing need. 34
Rectal infection
M. genitalium is commonly found in rectal samples from gay, bisexual and other men who have sex with men (GBMSM).35,36 While some studies show no association with symptoms, 9 a recent systematic review did demonstrate an overall association of M. genitalium infection with proctitis. 37 There appears to be a correlation between organism load and symptoms suggesting causation.8,9,38 To avoid overtreatment, and given that proctitis caused by C. trachomatis or N. gonorrhoeae mono-infection is more likely than proctitis caused by M. genitalium, routinely testing for M. genitalium in proctitis presentations is not recommended, except in specific circumstances (see Indications for Testing).39,40
Pharyngeal infection
A low prevalence of M. genitalium in pharynx is consistently reported, suggesting that this is not an important reservoir in the transmission of infection.36,37
Ocular infection
Ocular infection with M. genitalium can lead to conjunctivitis. 41 There are no reports of neonatal conjunctivitis when born to mothers with M. genitalium infection.
Complications
Pelvic inflammatory disease
M. genitalium is linked aetiologically to pelvic inflammatory disease (PID) and accounts for 9–13% of cases of PID.42–44 A meta-analysis in 2015 demonstrated significant associations between the presence of M. genitalium and cervicitis (pooled OR 1.66) and PID (pooled OR 2.14). 33
The organism has been shown to ascend from the lower to upper female genital tract, has been detected frequently from endometrial biopsies in individuals with PID independent of C. trachomatis and N. gonorrhoeae45,46 and can cause epithelial cilial damage in human fallopian tube culture. However, an association with tubal factor infertility has not yet been demonstrated and conducting studies to determine this will be difficult.25,47,48
It is estimated that 4.9% of individuals with M. genitalium in the female genital tract will progress to PID (compared to 14.4% of those with C. trachomatis infection). 44
Epididymo-orchitis
A small number of studies suggest an association of M. genitalium infection with epididymo-orchitis.49,50 Due to insufficient data, routinely testing for M. genitalium in epididymo-orchitis presentations is not recommended, except in specific circumstances (see Indications for Testing).
Prostatitis
Although M. genitalium has been detected in people with prostatitis and chronic pelvic pain syndrome,51,52 current data are lacking to support a clear association with prostatitis.
Sero-negative reactive arthritis
Case reports and case series indicate a possible association between M. genitalium and sexually acquired reactive arthritis.14,25,53,54
Pregnancy
A small number of studies have examined outcomes of M. genitalium in pregnancy. There is a possible increased risk of preterm birth (OR 1.91) but no association with spontaneous abortion. 55 There are insufficient data for premature rupture of membranes, low birth weight and perinatal death.
Indications for testing
Based on syndromes
• It is recommended to test for M. genitalium infection in people with NGU. (Grade 1B) • It is recommended to test for M. genitalium infection in people with signs and symptoms suggestive of PID. (Grade 1B)
Although M. genitalium may present with a range of symptoms (see Clinical features), it is often non-pathological and not the causative organism. Routine testing in these situations would result in overdiagnosis and overtreatment. Therefore, it is only recommended to test for M. genitalium in the following syndromes if symptoms persist after other infections have been ruled out and the index of suspicion is high: • People with signs or symptoms of mucopurulent cervicitis, particularly post-coital bleeding (Grade 2B); • People with epididymo-orchitis (Grade 2D); • People with sexually-acquired proctitis (Grade 2D).
An alternative strategy is to test for M. genitalium based on persistent symptoms and where C. trachomatis and N. gonorrhoeae screening is negative. However, this is not a preferable approach because it results in delayed identification of infection and treatment.
Based on risk factors
It is recommended to test for M. genitalium infection in current sexual partners of M. genitalium-infected individuals (see Tracing and Treatment of Contacts) (Grade 1D).
Asymptomatic individuals
There are currently insufficient data to recommend routine screening for M. genitalium infection in asymptomatic individuals. Newer multiple pathogen assays which include the detection of M. genitalium are being used by some providers in STI screening of asymptomatic individuals. This is not recommended. 56 Asymptomatic individuals with confirmed C. trachomatis and/or N. gonorrhoeae infection should not routinely be tested for M. genitalium.
Diagnosis
Diagnostic tests
M. genitalium has fastidious nutritional requirements and is extremely slow growing therefore culture is not appropriate for diagnosis. Nucleic acid amplification tests (NAATs) that detect M. genitalium-specific DNA or RNA in clinical specimens are the only useful diagnostic method.
It is recommended to test all M. genitalium-positive specimens for macrolide resistance associated mutations (MRAMs) using the commercial assays available in the UK. Commercial assays available for the detection of fluoroquinolone resistance associated mutations are not widespread but are becoming available. The UK Health Security Agency (UKHSA) STI Reference Laboratory offers a fluoroquinolone susceptibility genotyping assay for cases of treatment failure.
Specimen collection
Penile urethra
Most studies have found that first void urine and urethral swabs have good sensitivity (>90%) for the detection of M. genitalium.57–62 There are conflicting data for self-taken meatal swabs, with sensitivity estimates of 79–88%.62,63
Female genital tract
Vulvovaginal swabs are the most sensitive specimen (sensitivity >98%). Self-taken specimens have comparable diagnostic accuracy to clinician-taken specimens.62,64 The sensitivity of endocervical swabs and urine is lower (74–81% and 58–86.4%, respectively).57,62,65–67
Non-genital sampling
Rectal swabs are suitable for sampling and can be self-taken.
Pharyngeal M. genitalium is not thought to be clinically relevant and sampling is not recommended.
Considerations for people following gender reassignment surgery
There are a paucity of data concerning M. genitalium infection in individuals following gender reassignment surgery. It is therefore difficult to recommend an optimal specimen type, but this should be guided by sexual history and symptoms.
Recommendations
• It is recommended to use first void urine as the specimen of choice in cisgender men (Grade 1C). • It is recommended to use vaginal swabs (clinician- or self-taken) as the specimen of choice in cisgender women (Grade 1C). • It is recommended, where possible, to test all M. genitalium-positive specimens for the presence of MRAMs (Grade 1B).
Window period
There are no data on the incubation period for M. genitalium, or on the likely window period before a laboratory test becomes reliably positive. However, it is likely that sensitive tests will detect early infection.
Management
General advice
Patients should be given a detailed explanation of their condition, reinforced with clear and accurate written information. A patient information leaflet for M. genitalium can be found on the resource page of the BASHH website. 68 This will be updated when new guidance is published or new information becomes available.
Patients should be advised to abstain from sexual intercourse until 14 days after the start of treatment, and until symptoms have resolved. Where azithromycin has been used this is especially important because of its long half-life and is likely to reduce the risk of selecting/inducing macrolide resistance if the patient is re-exposed to M. genitalium.
Treatment
Recommended regimens
Treatment of uncomplicated infection (urethritis, cervicitis)
Azithromycin and macrolide resistance
Eradication rates of M. genitalium following treatment with macrolides have declined globally in recent years, and rates of genotypic resistance range from 30% to 100% regionally. 69 A recent systematic review and meta-analysis of 166 studies, including 22,974 samples across 41 countries demonstrated a global point prevalence of genotypic macrolide resistance of 33%. 70 Data from UK surveillance studies estimate macrolide resistance in the UK to be around 62.2% with the highest proportions of resistance seen in GBMSM. Use of azithromycin 2 g over 3 days in the absence of MRAMS is associated with a high rate of treatment success (94%). 71 Although there is no direct evidence to suggest that this regimen is superior in efficacy to longer courses of azithromycin, the risk of developing macrolide resistance is likely to be lower whilst offering a shorter and well tolerated course.
Access to prompt MRAM testing varies across the UK centres but is a useful tool to guide appropriate antibiotic therapy and improve treatment outcomes where available in a timely manner.
Even where an organism is known to be initially macrolide-sensitive, an azithromycin regimen should not be repeated following treatment failure because it is likely that resistance has developed on treatment.
Doxycycline
Although doxycycline as monotherapy has poor efficacy and eradication rates are low at about 30%–40%, studies suggest AMR-guided therapy, with doxycycline initially followed by azithromycin or moxifloxacin
Moxifloxacin and quinolone resistance
Moxifloxacin still has good efficacy in Europe29,74 although resistance is increasing in the Asia-Pacific region where its use is greater. 75 A recent systematic review and meta-analysis of 139 studies has demonstrated that global fluoroquinolone resistance rose from 10.5% (7.0–14.5%) in 2015–2017 to 17.0% (11.2–23.5%) in 2018–2020 and from 8% to 12% in non-Nordic European countries specifically. 70
Genotypic determinants of quinolone resistance are complex and incompletely understood. Mutations more commonly arise in the parC gene than in the gyrA gene. Mutations in parC gene may confer reduced susceptibility to moxifloxacin, and the occurrence of mutations in both genes is a strong predictor of treatment failure. 76 Recent enhanced surveillance data of M. genitalium samples in the UK detected fluoroquinolone resistance in 12.1% specimens with parC sequencing, and MRAM/parC dual class mutations in 10.1%. 71
Using moxifloxacin first-line in all cases of M. genitalium infections is not recommended because future therapeutic options are limited. Furthermore, the 2024 update on the use of fluoroquinolones published by the Medicines and Healthcare Products Regulation Agency (MHRA) has restricted the systematic use of this class of antibiotics to only situations where no alternative antibiotics are suitable. 77 As treatment options for M. genitalium are restricted in the presence of MRAMs, it remains appropriate to use moxifloxacin as an alternative first-line therapy, though patients require counselling on the risks of damage to tendons, muscles, joints and nerves, as well as significant psychiatric side effects including suicidal intent. The MHRA has produced patient information leaflets to provide to patients commencing quinolone therapy which are accessible via the MHRA website.
A meta-analysis reported no significant difference between moxifloxacin regimens of 7- and 10-days' duration, 78 and considering the MHRA guidance, a 7-day course is recommended in uncomplicated infections.
See Figure 1 a suggested treatment pathway for men presenting with NGU who subsequently test positive for M. genitalium. Suggested treatment pathway for men presenting with non-gonococcal urethritis who subsequently test positive for Mycoplasma genitalium. Azithromycin 3d should be started within 2 weeks of finishing doxycycline. Azithromycin 3d: azithromycin 1 g, then 500 mg od for 2 days; bd: twice daily; d: days; Doxycycline: doxycycline 100 mg bd for 7 days; Mgen: Mycoplasma genitalium; Moxifloxacin 7d: moxifloxacin 400 mg od for 7 days; MRAM: macrolide resistance associated mutation; neg: negative; pos: positive; tds: three times a day.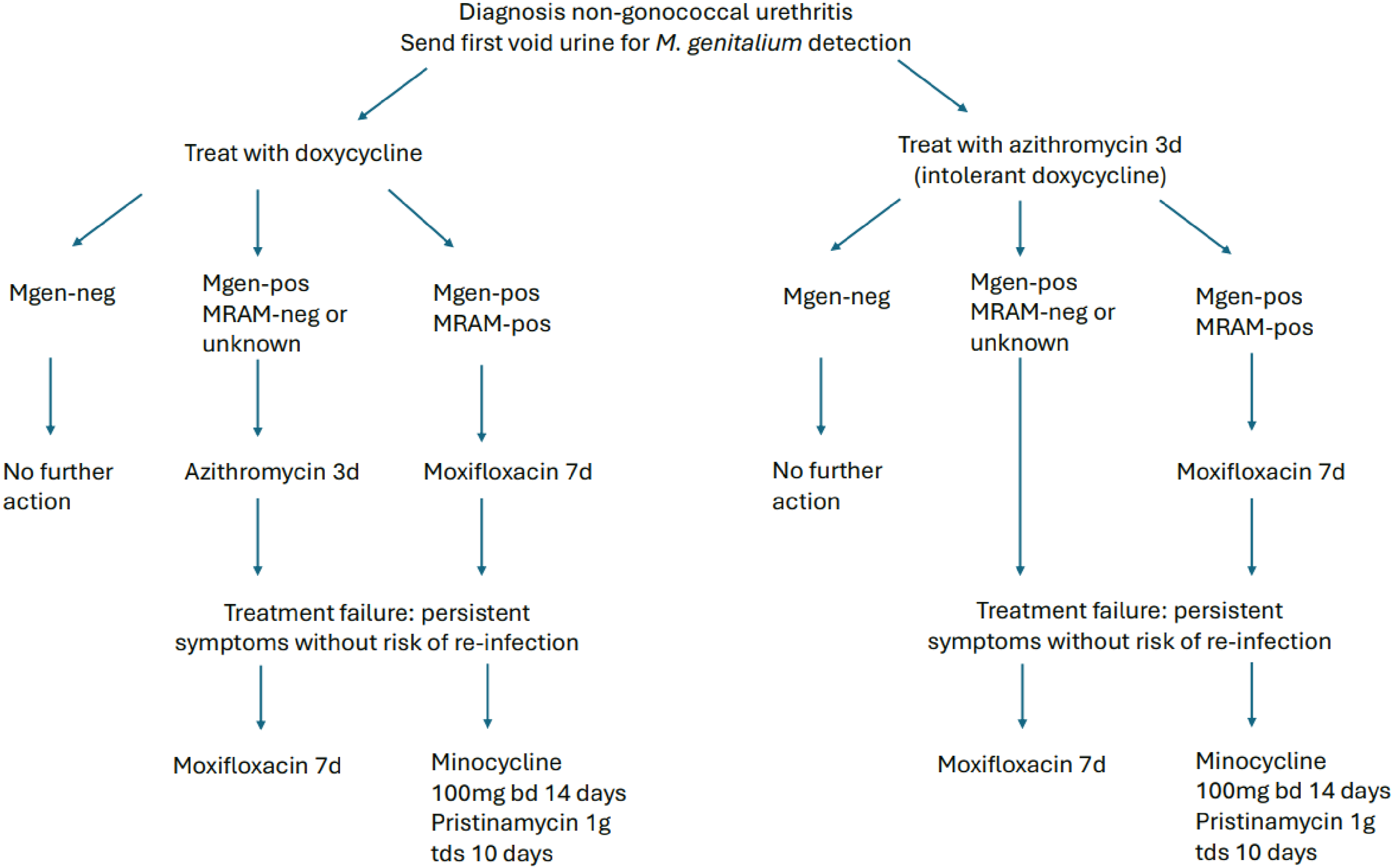
Recommended regimens (uncomplicated infections): • Doxycycline 100 mg twice daily (bd) for 7 days followed by azithromycin 1 g orally as a single dose then 500 mg orally od for 2 days* where the organism is known to be macrolide-sensitive or where resistance status is unknown (Grade 1C). • Doxycycline 100 mg bd for 7 days followed by moxifloxacin 400 mg orally od for 7 days if organism is known to be macrolide-resistant or where treatment with azithromycin has failed** (Grade 1C).
*Given that many individuals will have had doxycycline as first-line therapy for uncomplicated infectious syndromes, a repeat course is unnecessary once the M. genitalium positive result is known. Azithromycin and/or moxifloxacin should be given immediately after doxycycline, and ideally within 2 weeks of completing doxycycline. If this is not possible, the course of doxycycline should be repeated prior to giving azithromycin or moxifloxacin.
**Treatment failure is defined as persistent symptoms following treatment, or a positive test in the presence of symptoms taken 5 weeks post-treatment (if indicated – see Section Follow Up).
In situations where clinical cure is achieved prior to confirmation of a positive M. genitalium result, it may be pragmatic to take a watch and wait approach rather than offering further antimicrobial therapy.
Alternative regimens
In cases of failure or intolerance of recommended regimens, there are some observational data to support alternative regimens.
In one study, treatment with minocycline 100 mg od for 14 days was generally well-tolerated and cured approximately 67% of people who experienced treatment failure with a previous regimen. 79 The minimum inhibitory concentrations (MICs) of minocycline for reference strains of M. genitalium have been shown to be lower than those of doxycycline, thus greater effectiveness might be inferred (but, as with doxycycline, MICs of tetracyclines may not predict treatment outcomes). 80
Pristinamycin is a streptogramin antibiotic. It is available on a named patient basis in England for several indications, including treatment of M. genitalium infection failing recommended regimens.
An observational analysis of 114 people with macrolide-resistant M. genitalium infection showed 75% cure when treated with pristinamycin. 81 For infections with higher pre-treatment bacterial load, treatment was more likely to fail. Hence to improve chances of organism clearance, pre-treatment with doxycycline is advised. Patients should be warned of gastrointestinal side effects.
A recent observational study investigated the tolerability and efficacy of combination therapy of minocycline 100 mg twice daily and metronidazole 400 mg twice daily for 14 days (with or without pre-treatment with doxycycline) in individuals with macrolide-resistant M. genitalium in whom fluroquinolones had failed or were not advised. 82 In patients receiving pre-treatment with doxycycline, the microbiological cure rate was 90.3% (n = 28/31) compared to 76.7% (n = 56/73) in those who had not. Central nervous system and gastrointestinal side effects were commonly reported, however.
In cases of treatment failure with, or intolerance of first- and second-line regimens (including doxycycline, azithromycin, moxifloxacin), it is recommended to use: • Minocycline 100 mg orally bd for 14 days (Grade 1C). • Doxycycline 100 mg bd for 7 days followed by pristinamycin 1000 mg orally three times daily for 10 days (Grade 1C).
Treatment of complicated urogenital infection (PID, epididymo-orchitis)
There are few studies examining the efficacy of extended azithromycin and moxifloxacin regimens in the treatment of PID and epididymo-orchitis caused by M. genitalium. Given the need for prompt and effective treatment in complex STI syndromes, individuals with confirmed M. genitalium infection should be given moxifloxacin as a 14-day regimen. 78 Moxifloxacin is the currently the most efficacious agent against M. genitalium and an extended regimen has the highest chance of eradication. Individuals should be switched to moxifloxacin (if another regimen has been started) as soon as possible after M. genitalium is confirmed; doxycycline pre-treatment is not necessary in this situation. However, if treatment for PID has been completed and symptoms have resolved by the time of the M. genitalium result then it is pragmatic to review symptoms rather than re-treat all with moxifloxacin.
Recommended regimens (complicated infection)
• Moxifloxacin 400 mg orally od for 14 days (Grade 1C).
Alternative regimens
• Azithromycin 1 g orally stat followed by 500 mg orally od for 4 days (Grade 2A).
Pregnancy and breast-/chest-feeding
Pregnancy
Where possible, it is advisable to delay treatment until after pregnancy. 83 Clinicians should have an informed discussion with the pregnant person about the risks associated with treatment during pregnancy and the low risk of adverse pregnancy outcomes associated with M. genitalium infection. Condom use during the remainder of pregnancy is advised to reduce the risk of onward transmission of infection to sexual partners.
Treatment options in pregnancy are constrained by limited available data. There is some evidence that the use of azithromycin during pregnancy is unlikely to increase the risk of birth defects or adverse pregnancy outcomes.84–86 It is recommended a longer course of azithromycin to treat PID in pregnant people. This should be 1 g stat followed by 500 mg od for 4 days (Grade 1A).
Although the BNF recommendation is to avoid tetracyclines at all stages of pregnancy, BASHH supports the use of doxycycline in pregnant people only when the full course of treatment can be completed prior to 15 weeks gestation. 87 (Grade 2D)
The use of moxifloxacin in pregnancy is contraindicated. 88 Minocycline use during pregnancy is contraindicated. 89
Pristinamycin is considered safe in pregnancy, given its widespread use in Europe, but the writing group acknowledges that there are a lack of data supporting this. 81
Breast-/Chest-feeding
The level of antibiotic detected in breast milk of those taking azithromycin is very low and the systemic exposure in infants does not exceed that observed when azithromycin is administered for treatment. 90 Therefore, the risk for the infant is considered to be low. Infants should be monitored for possible side effects on the gastrointestinal flora including diarrhoea and candidiasis. A large cohort study found an association between the maternal use of macrolides during the first 13 days after delivery and an increased risk of pyloric stenosis in breastfed infants. 91 Where possible, exposure of neonates to macrolides should be minimised and precautionary monitoring undertaken with use. Doxycycline is excreted into breast milk in very small amounts and long term use is contraindicated due to the risk of tooth discolouration and effects on bone growth. 92 However, shorter courses (<21 days) are unlikely to cause harm because drug absorption by the infant is inhibited by calcium in breastmilk, and use of 7 days doxycycline as part of dual treatment for M. genitalium is acceptable. 93 Moxifloxacin is contraindicated during breast/chest-feeding. 88 Use of pristinamycin during breast/chest feeding has been associated with side effects in the baby. Due to a lack of data overall, its use is not recommended. 94
People living with HIV taking antiretroviral therapy
Treatment of M. genitalium in people living with HIV is the same as that for people living without HIV.
Adverse effects
Azithromycin, doxycycline, minocycline, moxifloxacin and pristinamycin can all cause gastrointestinal problems including nausea, but symptoms are most frequently reported with doxycycline and azithromycin doses over 1 g. 95
Caution should be taken when prescribing azithromycin or moxifloxacin to patients already on medications which may prolong the QT interval.
Minocycline has been associated with early onset toxicity reactions, hypersensitivity, autoimmune disorders, skin pigmentation and hepatitis. The risk of adverse effects increases with the duration of use and cumulative dose.
The MHRA has strengthened the recommendation on restricting the use of fluoroquinolone antibiotics following a review of their disabling and potentially long-lasting side effects. 77 Healthcare professionals should advise patients to stop treatment with a fluoroquinolone antibiotic at the first sign of side effects including tendonitis or tendon rupture, muscle pain/weakness, joint pain/swelling, peripheral neuropathy and central nervous system/psychiatric effects. Hepatotoxicity has been reported but is very rare (<1/10,000).
Follow-up
Persistence of M. genitalium has been demonstrated in the absence of symptoms in men treated for NGU.96,97 This occurs in about 10%–20% of men treated with doxycycline but is not associated with the development of AMR.14,97 Persistence of M. genitalium following treatment with azithromycin and moxifloxacin is strongly associated with AMR.96,97 Choice in efficacious therapeutic agents subsequent to this is limited and achievement of microbiological cure is not always possible. Thus, a more pragmatic aim for successful treatment should be the resolution of symptoms.
If symptoms persist following treatment with a regimen deemed efficacious, the risk of re-infection should be excluded and compliance with medication should be verified. Re-testing can be considered to determine whether symptoms are specific to M. genitalium and thus whether further treatment is warranted. The optimal time to perform this test after treatment has not been determined, but data suggest that very early testing after treatment when DNA load is low can give false negative results. 98
It is advisable that: • A test of cure (TOC) is not required where there is resolution of symptoms; clinical rather than microbiological cure should be pursued in all people (Grade 1D); • Re-testing can be performed in individuals who remain symptomatic after treatment when there is suspicion of persistent infection (Grade 1D)
Tracing and treatment of contacts
Patients should be informed of the importance of partner notification and supported to do this by appropriately trained professionals.
Among heterosexual contacts, women were twice as likely as men to be infected with M. genitalium, after adjusting for condom use and nature of relationship. 99 Among those patients reporting sexual contact with an M. genitalium-infected individuals, 48.2% of women, 31.0% of men who have sex with women, and 41.7% of GBMSM were infected.99,100
Whilst acknowledging this, the primary purpose of partner notification is to reduce the risk of re-infection to the symptomatic index patient.
Only current partner(s) (including non-regular partners where there is likely to be further sexual contact) should be tested, and treated only if positive. Sampling the rectum in contacts of index patients may be indicated by sexual history; we do not recommend sampling the pharynx. Partners should be given the same antibiotic as the index patient unless there is available resistance information to suggest otherwise (Grade 1D).
Auditable outcome measures
• All cases of M. genitalium infection should prompt a Sexual Health and HIV Activity Property Type (SHHAPT) code ‘C16’ submission to Genitourinary Medicine Clinic Activity Dataset (GUMCAD, performance standard 97%). • Cases of microbiologically confirmed treatment failure with persistent symptoms following moxifloxacin therapy should be reported to UKHSA at: https://www.gov.uk/government/organisations/uk-health-security-agency (performance standard 97%) • Individuals presenting with M. genitalium infection should be provided with written information about their diagnosis and management (performance standard 97%); e.g., patient information leaflets on M. genitalium from BASHH.
68
• Partner notification should be performed according to this guideline and documented according to the BASHH statement on partner notification for STIs (performance standard 97%).
101
Recommendations for further research
Longitudinal data are needed to determine natural history and time to clearance of organism, the longer-term effects of M. genitalium on the genital tract and clearer associations with reproductive health consequences.
Randomised controlled trials in clinical settings examining the efficacy of new antibiotic regimens are urgently needed to increase the therapeutic options available to manage M. genitalium. Whilst RCTs for newer drugs have shown some promise with respect to M. genitalium, approval for these newer agents is not yet available.
Qualifying statement
The recommendations in this guideline may not be appropriate for use in all clinical situations. Decisions to follow these recommendations must be based on professional clinical judgement, consideration of individual patient circumstances and available resources.
All possible care has been undertaken to ensure specification of the correct dosage of medication and route of administration. However, it remains the responsibility of the prescribing clinician to ensure the accuracy and appropriateness of the medication they prescribe.
Review arrangements
An author group will be invited by the BASHH CEG to review and revise the guideline in 2030 using the BASHH framework for guideline development. However, addenda may be issued sooner than 2030, particularly if relevant new data are available relating to testing or treatment options.
Supplemental Material
Supplemental Material - British association of sexual health and HIV national guideline for the management of infection with Mycoplasma genitalium, 2025
Supplemental Material for British association of sexual health and HIV national guideline for the management of infection with Mycoplasma genitalium, 2025 by Suneeta Soni, Helen Fifer, Yaser Al-Shakarchi, Joanne Bassett, Joy Mbaulu, Nicolas Pinto-Sander, Sara Strodtbeck and Michael Rayment in International Journal of STD & AIDS
Footnotes
Acknowledgements
The authors would like to thank the members of the BASHH Clinical Effectiveness Group for their appraisal of the guideline, and to all those that provided feedback during the consultation phase of guideline’s development.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All members of the guideline writing committee completed the BASHH conflict of interest declaration and submitted it to the CEG. No authors had any relevant conflicts of interest to declare, and the content of the guideline is not attributed to any organisation they are associated with.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Correction Nov 2025:
Figure 1 caption, Moxifloxacin prescribing amended from bd to od.
Editorial independence
This guideline was commissioned, edited, and endorsed by the BASHH CEG without external funding being sought or obtained. All members of the guideline writing committee completed the BASHH conflicts of interest declaration detailed below at the time the guideline’s final draft was submitted to the CEG.
Membership of the clinical effectiveness group
Supplemental Material
Supplemental material for this article is available online.