
Abstract
Introduction
Cystic echinococcosis, or hydatidosis, is a parasite infection that can occur in humans. It can affect all organs, mostly the liver and the lungs. The number, size and evolution of those cysts is mediated by the immune system. Herein we report an unusual presentation of hydatidosis in an immunocompromised woman who lives with HIV.
Case presentation
Our patient was a 40-year-old female with a 2-decade history of HIV and echinococcal infection. She was in AIDS stage due to poor medical adherence. She presented a medullar toxicity to Albendazole, a medication she had been taking for years to control the echinococcal cysts, which were stable then. Upon stopping the Albendazole, she presented an enlargement of those cysts. Surgery was mandatory, and revealed five liver cysts, a 12cm-large kidney cyst, and a gigantic 20 cm-large retroperitoneal cyst. They were treated successfully, and the patient has been asymptomatic during the last 4 years since surgery, along with maintained HIV suppression.
Conclusion
Hydatidosis can be negatively affected by immunosuppression such as HIV infection. However, the scarcity of the cases studying this association makes it difficult to fully grasp the possible interactions between those two diseases.
Introduction
Cystic echinococcosis, also known as hydatidosis, is a worldwide anthropozoonosis parasite infection due to Echinococcus granulosus.1,2 All organs can be infected by Echinococcus granulosus. Hydatidosis most commonly affects the liver (60%–70%) then the lungs (20%–30%).1,3
Tunisia is one of the most endemic countries with a human surgical incidence rate (SI) averaging 12.6/100000 inhabitants. Some regions are hyper-endemic (SI >22,6). 4 However its route of transmission is not well-known among the people, especially the rural population. 5 It is believed that the size, number and evolution of the cysts depend on the immune status of the host. 6 Yet, there are few reports of cystic echinococcosis in people living with human immunodeficiency virus (HIV). Herein we report the case of a patient who had both infections, with unusual, gigantic echinococcal cysts.
Case report
Our patient was a 40-year-old woman who was diagnosed with HIV at the age of 22. She was from a rural area where hydatidosis is endemic. The HIV infection was then at its early stage as the CD4 count was still high, over 500/mm3. She was diagnosed with disseminated hydatidosis involving the spleen, the liver and the right kidney at the same period. Initially, she couldn’t undergo surgical treatment because of important operative risks and received Albendazole daily along with the highly active antiretroviral treatment (HAART) combination of lamuvidine, zidovidine and lopinavir/ritonavir. Immunological success was initially achieved. She then progressively had had poor adherence to medication due to social pressure. She later developed ocular toxoplasmosis and her nadir CD4 count was 29 cells/mm3. Her HAART regimen was switched to tenofovir disoproxil fumarate, etravirine, and atazanavir/ritonavir. The evolution of cysts was monitored through computed tomography scans (CT-scans), which didn’t reveal any modification. The patient sought us out in early 2019 because of asthenia. Physical examination revealed extreme paleness, cachexia and multiple abdominal masses. Explorations disclosed a pancytopenia, and a pharmacovigilance study incriminated Albendazole. The role of this drug was later confirmed since the blood cells count went back to normal 1 month after she stopped taking it. A full-body CT-scan and an abdominal magnetic resonance imaging (MRI) were performed 4 months after the interruption of the anti-parasitic treatment and showed the extension of the hydatid cysts (Figures 1 and 2). There was a multivesicular cyst in the spleen of 21 ×11.5 ×10.8 cm. There were five hepatic cysts, and a cyst in the right kidney. Her viral load was 7000 copies/mL and CD4 count 127 cells/mm3 at that time. Axial contrast enhanced CT scan (a and b) and coronal reformatted contrast enhanced CT scan (c) show multiple hepatic cysts with peripheral wall calcification ( Axial (a and b) and coronal (c and d) T2-weighted MR images show multi-vesicular large cyst occupying the inter spleno-renal space ( ). Note the peripheral daughter cysts within the lesion of the left lobe of liver (
). Note the peripheral daughter cysts within the lesion of the left lobe of liver ( ). Large cysts are also noted at the right kidney and the inter spleno-renal space. Multiple round daughter cysts are seen peripherally within the inter spleno-renal space lesion (
). Large cysts are also noted at the right kidney and the inter spleno-renal space. Multiple round daughter cysts are seen peripherally within the inter spleno-renal space lesion ( ). The peripheral curvilinear wall calcification within renal cyst (
). The peripheral curvilinear wall calcification within renal cyst ( ).
). ) and a smaller hepatic one (
) and a smaller hepatic one ( ). The daughter cysts have varying sizes and are seen predominantly in the periphery of the giant mother cyst. Detached endocyst is seen within renal cyst , appears as twisted-linear structure as the serpent-sign or snake-sign (
). The daughter cysts have varying sizes and are seen predominantly in the periphery of the giant mother cyst. Detached endocyst is seen within renal cyst , appears as twisted-linear structure as the serpent-sign or snake-sign ( ). Note the characteristic hypointense rim on T2-weighted images representing the pericyst (
). Note the characteristic hypointense rim on T2-weighted images representing the pericyst ( ). Axial T1-weighted MR image (e) and axial contrast enhaced T1-weighted MR image (f) show a unenhanced low signal intensity on T1 weighted imaging within all hydatic cyst.
). Axial T1-weighted MR image (e) and axial contrast enhaced T1-weighted MR image (f) show a unenhanced low signal intensity on T1 weighted imaging within all hydatic cyst.
The patient underwent surgery two months later. Midline laparotomy incision was performed. There were five liver cysts. Four of them were exophytic: one located in segment 3 type IV, measuring 6 cm, two located in segment six on the falciform ligament of 3 cm type IV each, another one in segment VI measuring 9 cm type IV and the last one was an intraparenchymal 4cm-large, type V cyst in segment VIII seen through intraoperative ultrasound. There was also an inferior polar cyst in the right kidney measuring 12 cm. A retroperitoneal cyst measuring 20 cm was found on the left hemiabdomen, from the left kidney to the left diaphragmatic cupola. It was pushing the spleen and the kidney away. The pericystic area and the operative fields were covered with pads soaked with hypertonic saline solution. Partial cystectomy was performed for the four exophytic liver cysts, the right renal cyst and the left retroperitoneal cyst.
There were two visible biliary fistulas in the segment III and the segment IV cysts, that were sutured. After cholecystectomy, trans-cholecystic methylene blue was injected. There were no other biliary fistulas. Epiploplasy was performed for the cysts of the segment III and IV, and all residual cavities were drained through five tubes. Urine was found in the renal drainage tube 4 days postoperatively, revealing a cysto-urinary fistula. A ureteral stent was placed.
The patient evolved favorably. The urinary fistula dried up and tubes were removed. The patient was discharged on the 20th post-operative day. Now at 6-year follow-up, the patient is asymptomatic. She takes HAART daily, achieving HIV suppression with an undetectable viral load and a CD4 count of 456 cells/mm3. No new cysts have developed since her operation.
Discussion
Cases of HIV-Hydatidosis coinfection through literature.
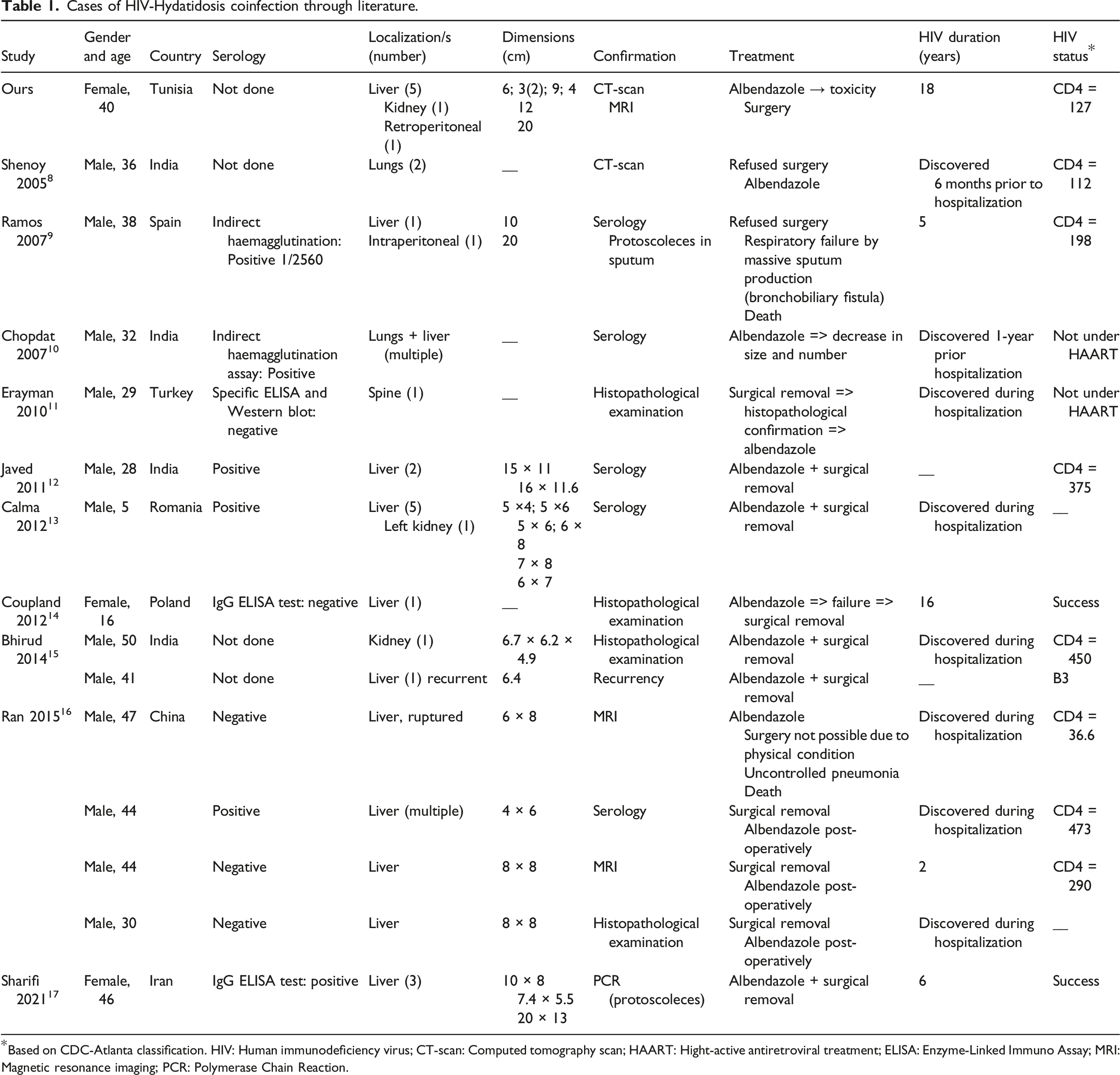
Based on CDC-Atlanta classification. HIV: Human immunodeficiency virus; CT-scan: Computed tomography scan; HAART: Hight-active antiretroviral treatment; ELISA: Enzyme-Linked Immuno Assay; MRI: Magnetic resonance imaging; PCR: Polymerase Chain Reaction.
Conclusion
Hydatidosis, when associated with HIV, can present in a more severe, disseminated form. It can also be more difficult to treat as there are few effective treatments and as the overall condition of the patient can be worsened due to the HIV infection. There are no clear guidelines regarding the management of those two diseases when associated, and the overall number of cases is probably underestimated. The lack of published cases is probably why this association is rather unknown. More data are needed regarding this coinfection so the interactions, physiopathology, evolution and particularities can be explored.
Footnotes
Acknowledgements
The authors would like to thank the study participants for consenting to be part of this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data Availability Statement
The data used to support the findings in this study are included within the article.