
Abstract
Background
Female sex workers (FSWs) are at high risk for sexually transmitted infections (STIs). This study estimated the prevalence of STIs caused by Neisseria gonorrhoeae (NG), Chlamydia trachomatis (CT), Mycoplasma genitalium (MG), and Trichomonas vaginalis (TV) and identified factors related to oral, vaginal, or anal intercourse among FSWs in informal settings in Tshwane, South Africa.
Methods
Samples were collected from 200 FSWs aged 18 and older in Pretoria who engaged in transactional sex. Participants completed a questionnaire on demographics, sexual history, and HIV testing. Three swabs (rectal, oral, and endocervical) from each participant were tested for NG, CT, MG, and TV.
Results
Of the 200 participants, 53 (26.5%) had at least one infection. Of these infections, the most common site of infection was genital (100 %), followed by the rectum (45.3 %), and pharynx (20.8 %). CT and TV were detected in 24 (12.0%) participants, while NG and MG were found in 20 (10.0%) participants. Most of the infected FSWs (32/53) had one sexually transmitted pathogen, while 21 (40%) had multiple STIs. Substance use was significantly associated with the presence of an STI.
Conclusion
This study reveals a high burden of STIs among FSWs, highlighting pathogen prevalence at genital and extragenital sites. These findings underscore the need for targeted STI control interventions for high-risk groups like FSWs in South Africa.
Background
The World Health Organization (WHO) estimates that over 374 million people acquire new Sexually Transmitted Infections (STIs) annually, with 96 million in Africa. 1 Sub-Saharan Africa has the highest prevalence, 2 with South Africa (SA) carrying the highest burdens of both HIV and STIs. 3 The majority of cases are attributed to sexually transmitted pathogens (STPs), such as (Chlamydia trachomatis (CT), Neisseria gonorrhoeae (NG), Mycoplasma genitalium (MG), Trichomonas vaginalis (TV), and Treponema pallidum (TP)]. 4 Controlling STIs remains a priority, especially in groups at risk, as untreated STIs increase the risk of acquiring and transmitting HIV by at least 5-fold.2,4,5 Female sex workers (FSW) experience at least a 10-fold higher chance of contracting STIs, and have a 6-fold higher prevalence of chlamydia than the general population. 2
Despite the lack of consolidated data, it is estimated that between 0.76 and 1 % (131,000 and 182,000) of the adult female population in SA is involved in commercial sex work. 6 Sex work in SA operates across a spectrum, from formal settings (e.g., regulated brothels) to informal contexts (e.g., street-based or ad hoc arrangements).7,8 Informal sex workers, often lack institutional protections and face greater barriers to healthcare, safety, and legal recourse compared to their formal counterparts. The unlawful classification of sex work exacerbates their exposure to violence, 9 with 71 % of FSWs in one Johannesburg study experiencing physical or sexual intimate partner violence (IPV) or violence from police officers or clients in 2016. 9 According to the WHO, FSW is a high-risk group for contracting or transmitting HIV and other STIs. 10 They engage in higher-risk behaviours such as multiple sex partners, inconsistent condom use, anal sex, drugs and alcohol use, and transactional sex.5,11
STIs cause acute conditions such as cervicitis, urethritis, and genital ulceration, and can lead to severe complications including pelvic inflammatory disease amongst others. 2 Beyond clinical burden, STIs result in stigma and shame, 12 particularly among high-risk groups like FSWs. 13
STIs among FSWs in SA are challenging to prevent because of difficulties in reaching specific populations at higher risk of contracting sexually transmitted infections. This study aimed to estimate the prevalence of common STIs caused by NG and CT. MG, and TV, and identified factors related to unprotected oral, vaginal, or anal intercourse in a population of FSWs in informal settings. These pathogens were considered together because of their shared symptomatology and to provide a broader view of the potential public health consequences of risky sexual practices. 14
There is limited data regarding the prevalence of curable sexually transmitted pathogens (NG, MG, CT, TV, and TP) among FSWs in South Africa. This study aimed to estimate the prevalence of common STIs caused by NG, CT, MG, and TV, and identify factors related to sexual practices among FSWs in informal settings, to inform strategic prevention planning, especially in Tshwane where there are no dedicated STI clinics.
Methods
This cross-sectional study was conducted between June and November 2022 at Sefako Makgatho Health Sciences University in Pretoria, South Africa. It received approval from the Research Ethics Committee of Sefako Makgatho Health Sciences University (SMUREC) under the reference SMUREC/M/60/2022: PG. In this study, we included adult women who voluntarily engaged in sexual activities with men in exchange for money, operated in specific places (Soshanguve, Ga-Rankuwa, Mabopane, Marabastad, etc.), and gave their consent to participate. The study found that the workplaces of the FSWs included outdoor areas with vegetation, establishments serving alcoholic beverages, and indoor spaces. A recruitment team consisting of two community liaison officers and two recruiters was established, and snowballing was the primary method of recruitment. Snowball sampling defined as a non-probability method where initial participants refer peers from their social networks, creating a chain of referrals. 15 It is mainly used for hard-to-reach groups, such as FSWs, where traditional sampling is impractical. 16 The participants received an information brochure and a questionnaire at their workstations. After briefing, their consent was obtained, and the recruitment team assisted with questionnaire completion. Data collected included demographics (age, place of residence, and education) and recent sexual behaviours (oral/anal sex, rimming, number of partners, condom usage, and substance use). Unsafe sex was defined as unprotected intercourse and/or multiple sexual partners. Current sex practice refers to sexual within the last 6 months prior enrolment. In order to maintain confidentiality, each participant was given a distinct identifier.
A total of 600 swab samples were collected from three anatomical sites (pharynx, rectum, and cervix) from a cohort of 200 subjects. The specimens were tested for Chlamydia trachomatis (CT), Neisseria gonorrhoeae (NG), Trichomonas vaginalis (TV), and Mycoplasma genitalium (MG) at SMU. The Seegene STI-7 real-time PCR kit (Seegene, Seoul, Korea) was utilized, following manufacturer’s instructions. The CFX96 TM Real-Time PCR Detection system (Bio-Rad, USA) was used for amplification.
The data obtained from the questionnaire as well as the test results were put into a Microsoft Excel® database. Demographic data was summarized using descriptive statistics. Bivariate and multivariate logistic regression models were employed to evaluate the factors that independently predict the occurrence of a sexually transmitted infection (STI) and any concurrent relationship between factors and the presence of a STIs. Bivariate analysis consisted of conducting two-sample tests to determine differences in proportions, χ2 tests of independence to analyse the relationship between variables, and logistic regression to examine the relationships between factors and the presence of occurrence of STIs. Backward elimination was performed using a relaxed p-value of 0.20, based on the Wald test from logistic regression, to select the variables included in the multivariate model. Furthermore, the model incorporated fundamental demographic attributes such as age and education. The study presented variables that showed a significant association (p < .05) with the presence of a STI. Relevant odds ratios (OR) and 95 % confidence intervals were also calculated.17–19
Results
Demographic characteristics
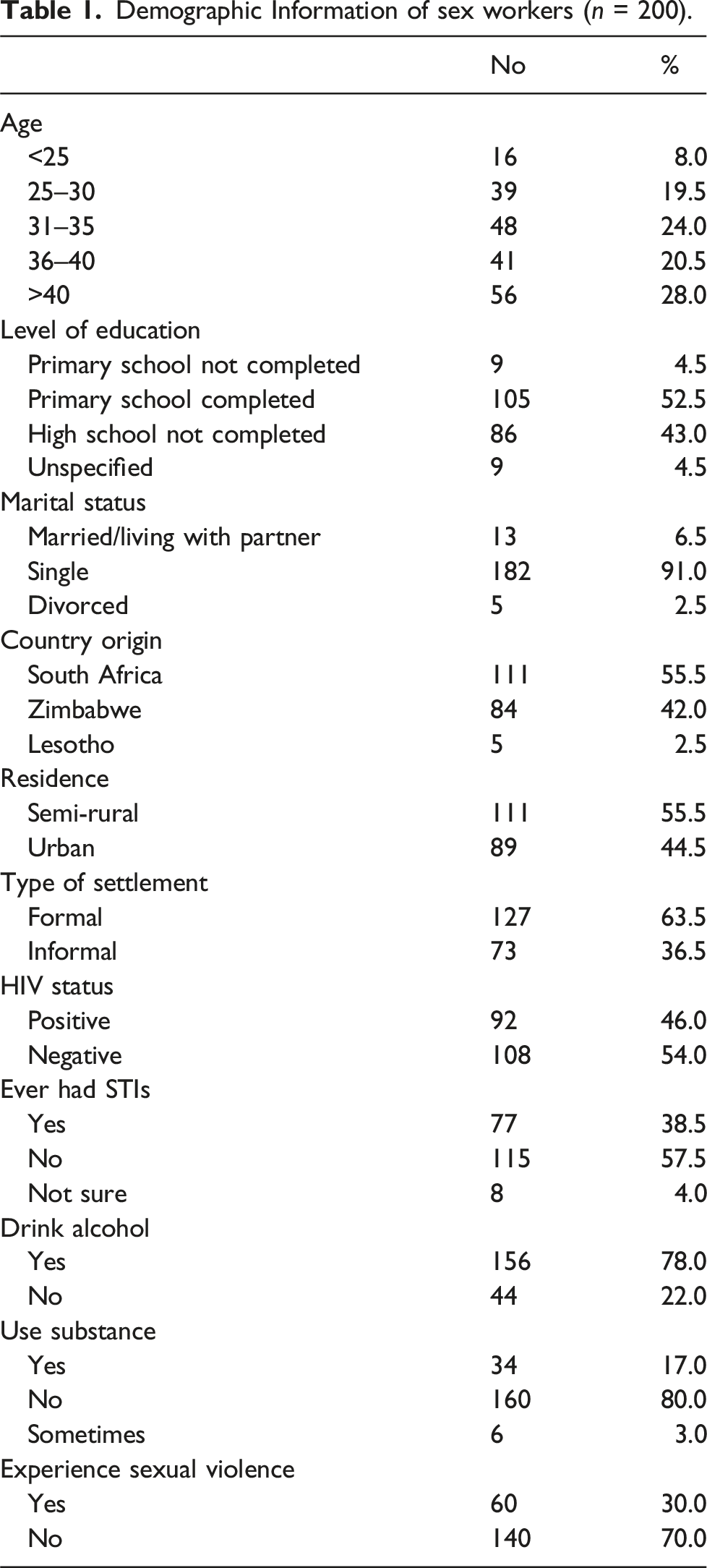
Demographic Information of sex workers (n = 200).
Sexual practices of the informal FSWs
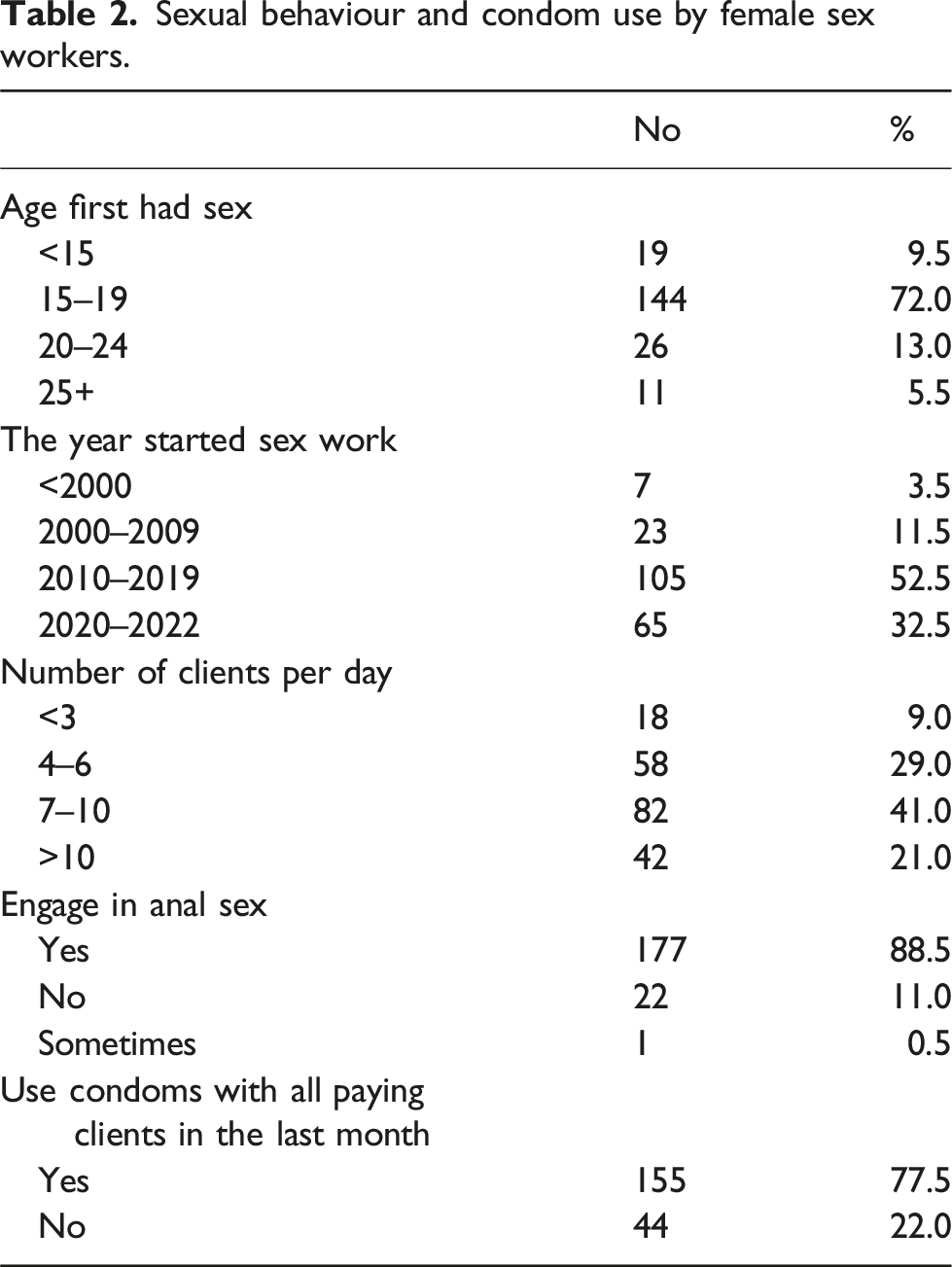
Sexual behaviour and condom use by female sex workers.
Prevalence of sexually transmitted infections among informal FSWs
Of the 200 FSWs included in this study, 53 (26.5 %) were infected with at least one sexually transmitted pathogen. Of these infections, the most common site of infection was genital (53; 100 %), followed by the rectum 24 (45.3 %), and pharynx 11 (20.8 %). Overall, the most prevalent microorganisms were CT and TV (both12 %; 24/200), followed by NG and MG (both 10 %; 20/200), and MG (10 %; 20/200) (Figure 1). Frequency of sexually transmitted infections (%) in 200 FSW participants by anatomical site. NG = N. gonorrhoea, CT = C. trichomatis, MG = M. genitalium, TV = T. vaginalis.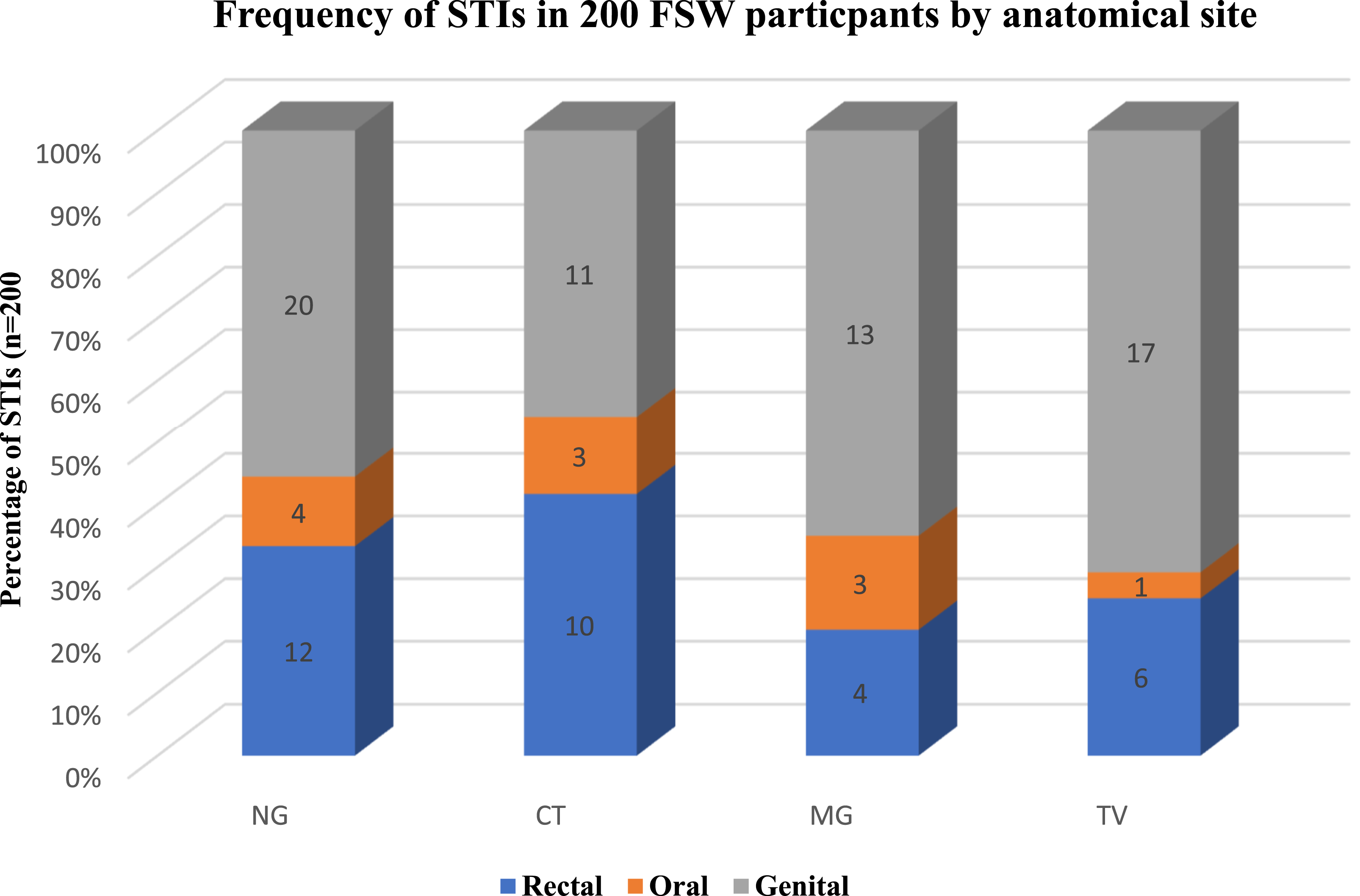
Prevalence of STIs among informal FSWs.
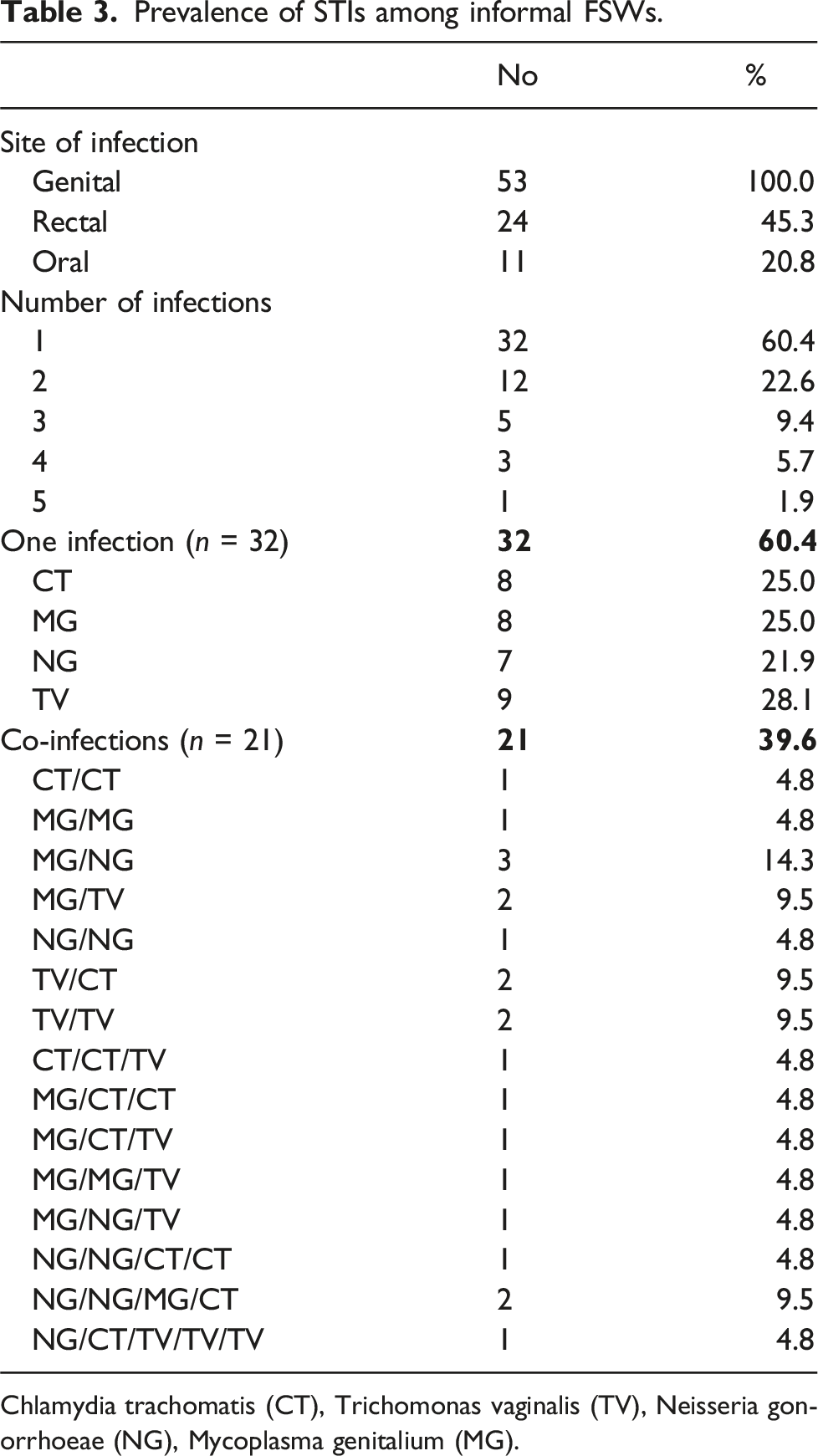
Chlamydia trachomatis (CT), Trichomonas vaginalis (TV), Neisseria gonorrhoeae (NG), Mycoplasma genitalium (MG).
Factors associated with STI among informal FSWs
Bivariate and multivariate analyses of factors associated with infection among FSWs.
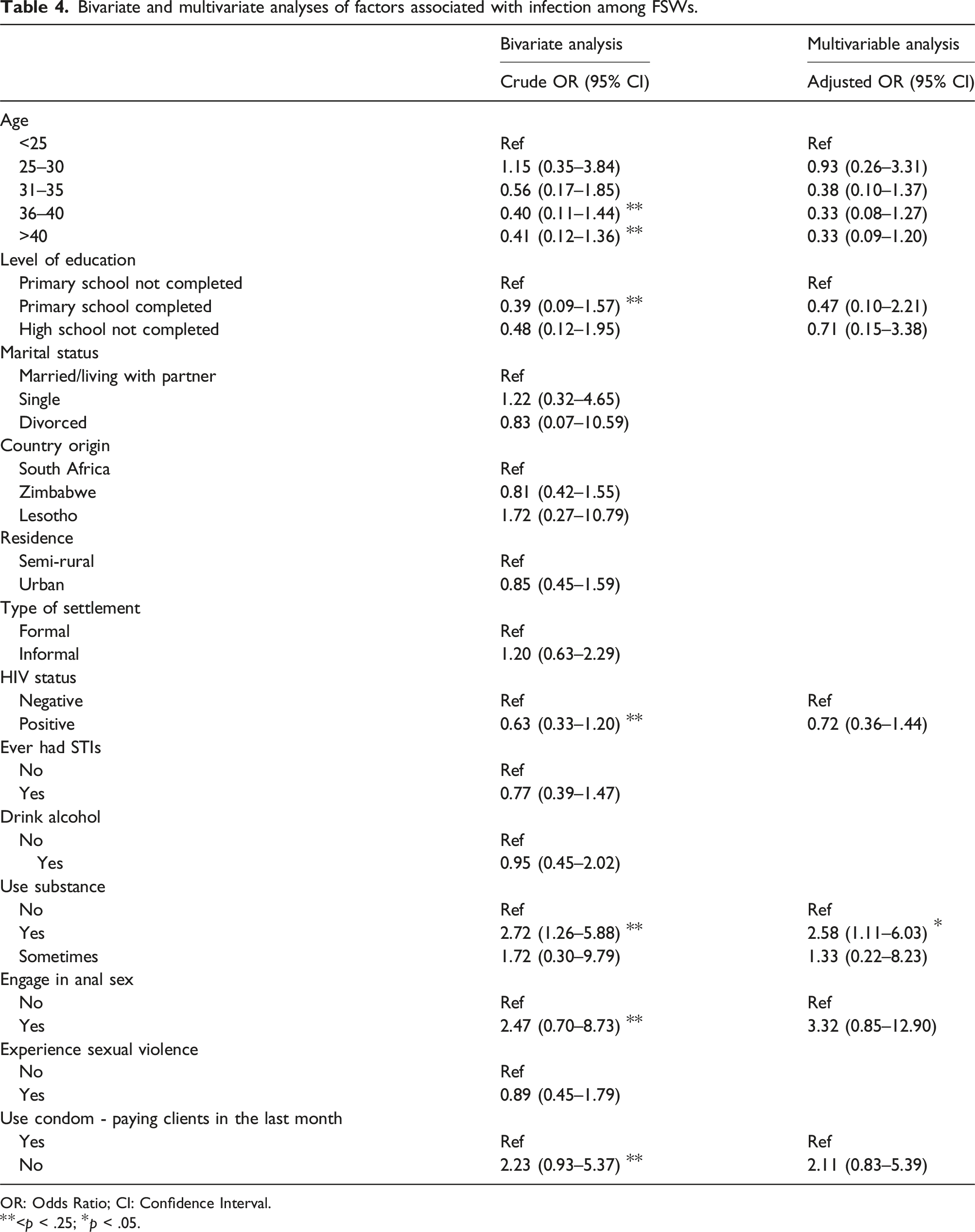
OR: Odds Ratio; CI: Confidence Interval.
**<p < .25; *p < .05.
Discussion
Sexually transmitted infections pose a significant global public health concern, and certain populations such as informal female sex workers are particularly vulnerable to acquiring and transmitting these infections. 20 This study aimed to determine the frequency and factors associated with sexually transmitted pathogens from informal FSWs in an area north of Pretoria, South Africa. The study revealed that more than a quarter (26.5 %) of the participants (FSW) in this area had at least one sexually transmitted infection. The high prevalence of STIs among informal FSWs highlights the urgent need for comprehensively tailor-made STI control and prevention strategies.
Of the 200 FSWs included in this study, a quarter (26.5 %) were infected with at least one sexually transmitted pathogen. This is similar to that reported in a study in Ethiopia in 2023 among the general female population 21 ; however, it was lower than what was reported (30.8%) among FSWs in Burkina Faso. 22 Our study found CT and TV in 12 % of FSWs, and MG and NG in 10 % each. These prevalence rates differ from those of a national surveillance study in Peru, which reported CT in 16.4 % of FSWs, NG in 1.5 %, and TV in 7.9%. 22 A study among FSWs in China, reported similar CT values (12.3%), but lower NG presence (1.3%)23. Among the 349 FSWs recruited in Nairobi, Kenya, the prevalence of MG, CT, NG and TV were 12.9%, 3.7%, 2.3%, and 7.2%, respectively which is with the exception of MG, lower than what was reported in our study. 24 Most of the infections found in the study were genital; however, a high number of anal and pharyngeal infections were seen, which again highlights the urgent need for education and implementation of comprehensive STI screening and treatment programs. Some FSW perceive anal sex as safer or more desirable, and the rates are better than the vaginal intercourse. 25
The findings of our study also revealed that more than two-thirds of the participants were older than 30 years, indicating that a significant proportion of female sex workers in the Tshwane region are in their thirties or older. This demographic insight sheds light on the age distribution of female sex workers in this region, challenging the common misconception that sex work is predominantly undertaken by young women. Moreover, the high proportion of older female sex workers has implications for tailored healthcare services and interventions considering the potential for increased vulnerability to STIs in this age group. These findings are comparable to those of a study conducted in Iran, where the majority (∼70 %) of FSW were above 30. 16 However, this differs from several studies, including data reported from the Mali and Bakomo regions, where most participants were less than 30 years of age. 26 The education level of the participants was relatively low, with over half of the participants having completed at least primary education or higher, which is below the 84.5 % of the FSW participants in Cameroon in 2023, as reported by Gross et al. 27 This suggests that the educational level of the participants in this study was lower than the national average, highlighting the need for increased efforts to enhance access to education and promote lifelong learning opportunities.
This study found that over 22% of the participants engaged in condomless sex with paying clients, consistent with Cameroon data, showing 77.7 % (implying 22.3% did not). 27 However, a Northeast Indian study reported much lower rate (2.1 % non-use) alongside heroin use before sex (52.1 %), and 9.3 % used mobile phones to solicit clients. 28 Alarmingly, our study revealed that 75 % of the FSWs in Tshwane were living with HIV. This, coupled with the finding that over 22 % of individuals engage in condomless sex with clients, raises serious concerns about potential transmission to the general population. These women are at a heightened risk of contracting and transmitting STIs, highlighting the urgent need for targeted interventions that address both their health and the well-being of the wider community.
More than 90 % of the population were single; this data is comparable to the data from Iran, where 77 % were not married. 29 Similarly, in the Iranian study, almost two-thirds of the population were single. 16 A systematic review estimated that 35–65 % of female sex workers in the USA use injection drugs and reported rates of crack use as high as 75 %, 30 which is higher than that reported in the current study with 20 % of the participants.
In this study, factors associated with testing positive for at least one of five STIs among informal FSWs were examined. Univariate and multivariate logistic regression analyses provided insights into the complex web of factors contributing to STI risk in this vulnerable population. When analysing two variables only (crude odds ratio), several factors were associated with an increased STI risk, including younger age, lower educational attainment, HIV infection, substance use, engaging in anal sex, and inconsistent condom use with clients. These findings align with the literature on the heightened vulnerability of sex workers, particularly those in informal settings, to adverse sexual health outcomes. 31
However, the multivariate analysis (adjusted odds ratio) further highlighted the critical role of substance use and inconsistent condom use as key drivers of STIs among this group of informal sex workers. Substance use has been linked to increased risk-taking behaviours and reduced ability to negotiate safer sex practices, contributing to elevated STI risk among this population. 28 Additionally, although not significant, the finding that inconsistent condom uses with paying clients and engaging in anal sex was associated with higher STI prevalence underscores the importance of promoting and enabling consistent condom use within sex work transactions.
These results underscore the need for targeted interventions that address the structural, personal, and socioenvironmental factors that shape the sexual health and well-being of informal female sex workers. Capacity-building efforts to enhance employability and provide alternative livelihood opportunities coupled with comprehensive sexual and reproductive health education and services could help mitigate the vicious cycle of HIV and STI transmission in this vulnerable population ( 32 ,33).
Limitation of the study
Our research possesses several limitations. The cross-sectional design restricts the capacity to show causal links between factors and STI acquisition/outcomes, whereas self-reported behavioural data may be susceptible to social desirability and recollection bias. While our implementation of snowball sampling was appropriate for accessing this elusive demographic, it may have added selection bias, hence constraining the generalisability to the wider FSW community. Moreover, operational limitations hindered longitudinal follow-up to evaluate treatment outcomes or re-infection rates, as those who were infected were referred for further treatments.
Notwithstanding these constraints, our results offer significant insights into STI prevalence and related variables among informal FSWs in Tshwane, hence enhancing the knowledge foundation for public health interventions targeting this vulnerable group.
Conclusion
The prevalence of STIs among FSWs in our study highlights a critical need for widespread screening programs targeting FSWs. Given the high prevalence of asymptomatic and extragenital infections, screening should encompass the endocervix, rectum, and oropharynx. However, further research is needed to determine the most cost-effective balance between empirical treatment and screening for asymptomatic STIs in high-risk populations. These findings underscore the urgent need for policymakers and healthcare providers to prioritize the development and implementation of comprehensive STI screening and treatment programs tailored to the unique needs of FSWs
Footnotes
Acknowledgements
We extend our sincere gratitude to Sister Malebye KC for specimen collection from each participant. We also thank our dedicated field workers and research assistants for their support throughout the study. We are deeply grateful to all the sex workers who generously participated in this research. Finally, we acknowledge the expert guidance provided by the Microbiology Department, Dr Sam Ntuli for data analysis, and last but not least we acknowledge Mr Ramudingana P for proofreading this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Research Foundation (Thuthuka), Sefako Makgatho Health Sciences University (RDG), Vliruos (Project 8-Infectious Diseases).