
Abstract
Objective
This narrative review examines the impact of the United States on the war against HIV/AIDS and thus the impact of political ideologies on the financing of the medical sector.
Discussion
Initially marked by stigma, particularly in the early years of the epidemic, the US response was transformed with the launch of the Presidential Emergency Plan for AIDS Relief (PEPFAR) in 2003. PEPFAR has partnered with entities such as the Global Fund and the Joint United Nations Programme on HIV/AIDS (UNAIDS), retranslating global health governance. Despite this success, the global response remains dependent on the support of the United States. Political changes under the leadership of the conservatives have limited funding. Therefore, political polarization in the US is undermining long-term progress on HIV/AIDS prevention and treatment, particularly in low- and middle-income countries.
Conclusion
By tracing historical developments and analysing current funding trends, the article highlights the urgent need for sustainable and depoliticized investments in global health systems. Without renewed bipartisan commitment and greater local ownership, the vision of eliminating AIDS as a public health threat by 2030 is seriously threatened.
Keywords
Introduction
The global response to the HIV/AIDS epidemic has always been deeply influenced by political will and socio-cultural dynamics. Despite resistance from the conservative camp in the U.S., the Presidential Emergency Plan for AIDS Relief (PEPFAR) emerged as a transformative force in the global fight against HIV/AIDS. Led by the U.S., PEPFAR partnered with the Global Fund and UNAIDS to forge a coordinated international response. However, American political volatility has repeatedly undermined this leadership, creating instability and threatening long-term gains. Recent U.S. presidential decisions have placed these hard-won achievements at risk, further destabilizing a global health system that remains precariously reliant on external funding rather than grounded in sustainable local investment.
The early years: Stigma and political inaction
The United States, a global leader in health policy, has taken the helm since 2003 in combating HIV/AIDS through multiple initiatives such as the PEPFAR, the Global Fund and the UNAIDS. In the early years, intense stigmatization and politicization marked global and U.S responses. As the crisis intensified, the intervention was inevitable. In the U.S, during the early to mid-80s, HIV/AIDS was linked not only to specific populations, but also to certain behaviors, and the cultural and political response emphasized “abstinence” over medical intervention. The more conservative the political culture, the lower the state expenditures were on AIDS. 1 The Stigma contributed to significant delays in allocating federal funds, developing treatments and providing care, especially among marginalized populations. 2 Roy Schwartz of the American Medical Association once said: “AIDS is a political disease, a social, religious and moral disease it’s more complex to manage. It’s also a civil-rights disease, and the fascination and damnation of the disease. 1 ” The politicisation of the HIV/AIDS continued with the slow response of the Reagan administration. Grassroots advocacy, particularly from organizations like ACT UP, played a pivotal role in prompting action from the government, the medical sector, and insurance companies. It pushed for increased funding for research-based medications that prioritized people’s needs, changes to insurance policies to expand coverage, and reduced medical and treatment costs, among other reforms. 3 Outside the U.S., politicization also occurred, with some nations underreporting cases to avoid stigma. 4 Since the beginning of the HIV/AIDS epidemic, it was viewed as an immoral disease and treatment was often aimed at changing behavior rather than addressing the disease itself. Nevertheless, the humanitarian urgency of the U.S. intervention managed to overcome these value-based barriers and allowed for the establishment of effective interventions, particularly in low- and middle-income countries. By the early 2000s, U.S. global health policy shifted from inaction to leadership, driven in part by the redefinition of health as a security issue, especially post-9/11.
The launch of PEPFAR and U.S. Global health leadership
The U.S. global health leadership brought on board other countries and entities to build a global system in the fight against HIV/AIDS through multilateral and bilateral interventions. Most international funding went to the PEPFAR that was created by the U.S, in 2003 as a bilateral initiative providing direct support to over 55 countries with $110 billion in the global HIV/AIDS response, the largest commitment by any nation to address a single disease in history. 5 On the multilateral level two entities joined forces with PEPFAR in the fight against HIV/AIDS, namely UNAIDS, created in 1996, and the Global Fund, established in 2002. Even though many countries and organizations came on board, the vast majority of funding for the mentioned initiatives and entities came directly from the US. The U.S. continued to be the largest donor to HIV efforts, providing US$5.71 billion and accounting for 73% of total donor government funding in 2023 6
Comparison of U.S. HIV/AIDS contributions with those of other major donor countries in 2023: KFF (2024).
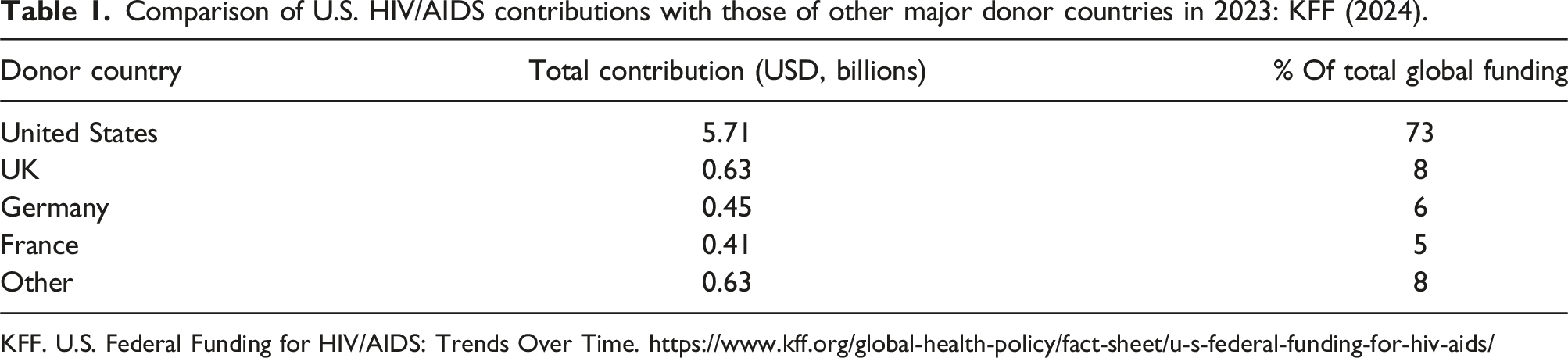
KFF. U.S. Federal Funding for HIV/AIDS: Trends Over Time. https://www.kff.org/global-health-policy/fact-sheet/u-s-federal-funding-for-hiv-aids/
The US, as main funder of the initiative to fight against HIV/AIDS made both bilateral and multilateral contributions, though these were not equally distributed, with bilateral contributions making up 92% of the total, while most other countries focused on multilateral efforts. Having said that, the impact of the US contributions went directly to target countries and programs to initiatives and to countries which made the recipients fully reliant on the U.S. and its funding. 6
The U.S. implementation of PEPFAR was deemed one of the most successful health funding initiatives in modern history, with impacts not only on HIV/AIDS but also on global health systems and economic strategies. PEPFAR focused on training medical teams, upgrading laboratories, and enhancing data and health system management, which also supported responses to other diseases and improved general healthcare for local populations. It also contributed to economic development by lowering unemployment and encouraging growth in other sectors. These initiatives helped reshape the global approach to health and development and encouraged the engagement of multiple sectors. 7
Impact and global partnerships
The PEPFAR is the largest commitment by any nation to address a single disease in history. It saved more than 26 million of lives across more than 50 countries through bilateral collaboration. This program laid the foundation for global health governance and encouraged other countries to contribute more to Global Health. PEPFAR not only focused on direct combat against HIV/AIDS but on improving health systems in the partnering countries which came with improvement in the economy and education which helped achieve political and security stability. PEPFAR worked closely with international partners to create a unified global governance framework against HIV/AIDS and other emerging infectious diseases. In 2020, UNAIDS launched a new strategy called ‘95-95-95’ by 2030 to build on the progress of the previously achieved ‘90-90-90’ target. The new goals aim for:
At least 95% of people living with HIV to know their HIV status,
At least 95% of those diagnosed to receive treatment,
At least 95% of those on treatment to achieve a suppressed viral load. 8
Although the 2025 target has not yet been met, significant progress has been made in the global fight against HIV/AIDS.
Global progress toward the 95-95-95 HIV targets (as of end 2023).
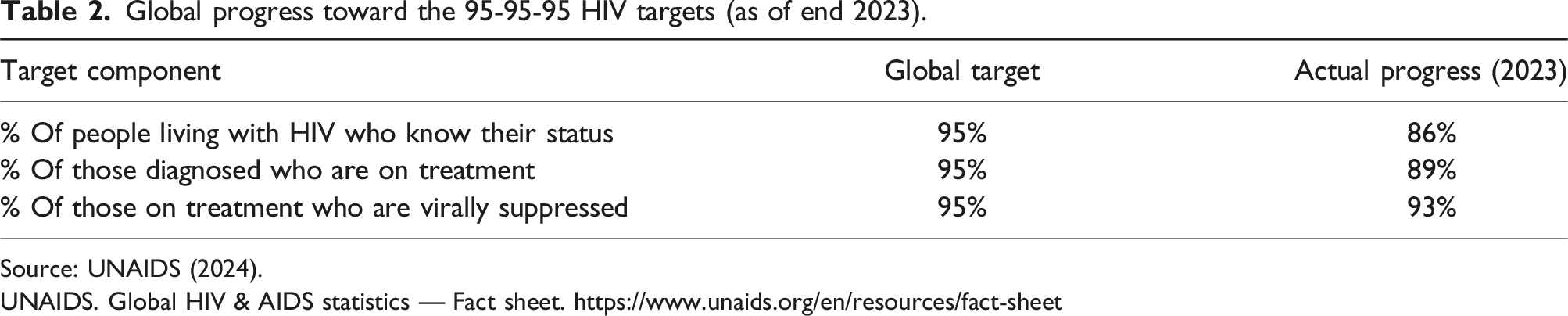
Source: UNAIDS (2024).
UNAIDS. Global HIV & AIDS statistics — Fact sheet. https://www.unaids.org/en/resources/fact-sheet
These advances come after years of successful strategies that saved millions of lives. According to UNAIDS, AIDS-related deaths have dropped by 64% since their peak in 2004, and new infections have declined by 42%. Additionally, 73% of people living with HIV are now accessing antiretroviral therapy. Services offered by these initiatives focus on treatment, prevention, education, and care, particularly for the most vulnerable populations. 9
According to the U.S. Department of State: - Between FY 2020 and FY 2024, PEPFAR increased its support to PrEP initiations by 500%, to reach 2.5 million people protected from HIV infection in FY 2024. - PEPFAR is behind over 90% of global PrEP (pre-exposure prophylaxis) initiations and has started offering long-acting injectable PrEP in five countries, with plans to roll it out in six more by the end of 2024. - In 2023, countries supported by PEPFAR saw 52% fewer new HIV infections compared to 2010, which represents a stronger drop than the 39% global average. AIDS-related deaths also fell by 59% in PEPFAR countries, compared to a 51% global decline. - In fiscal year 2024, PEPFAR delivered HIV testing services to 83.8 million people — an increase of 12 million from the previous year. - As of September 30, 2024, PEPFAR is supporting antiretroviral treatment (ART) for 20.6 million people in 55 countries, including 566,000 children living with HIV. - In FY 2024 alone, PEPFAR reached 2.3 million adolescent girls and young women with HIV prevention services tailored to their needs. - By September 2024, the program helped ensure 7.8 million babies were born HIV-free to mothers living with HIV, and provided care and support to 6.6 million orphans, vulnerable children, and their caregivers. - Since 2007, PEPFAR has supported 35.1 million voluntary medical male circumcisions in East and Southern Africa to reduce HIV transmission, including 2.7 million procedures in 2024 alone. - PEPFAR alone is directly supporting more than 327,000 health workers in combatting HIV/AIDS and other health areas which provided better health services and a sustainable health system in the participating countries.
10
The PEPFAR, UNAIDS and Global Fund made significant progress in addressing the HIV/AIDS epidemic, however significant challenges remain. According to UNAIDS report “The urgency of now, AIDS at a crossroad” published in 2024, HIV/AIDS can be ended as a public threat by 2030, but this is unlikely due to political and financial reasons. The report highlights several key issues notably urging political leaders around the world to increase national and international funding for HIV programs, to increase treatment accessibility, and to implement stronger policies promoting equity and gender-related rights.
U.S. Government funding for global HIV/AIDS by year (2003–20240): KFF (2024), white house OMB (2024).
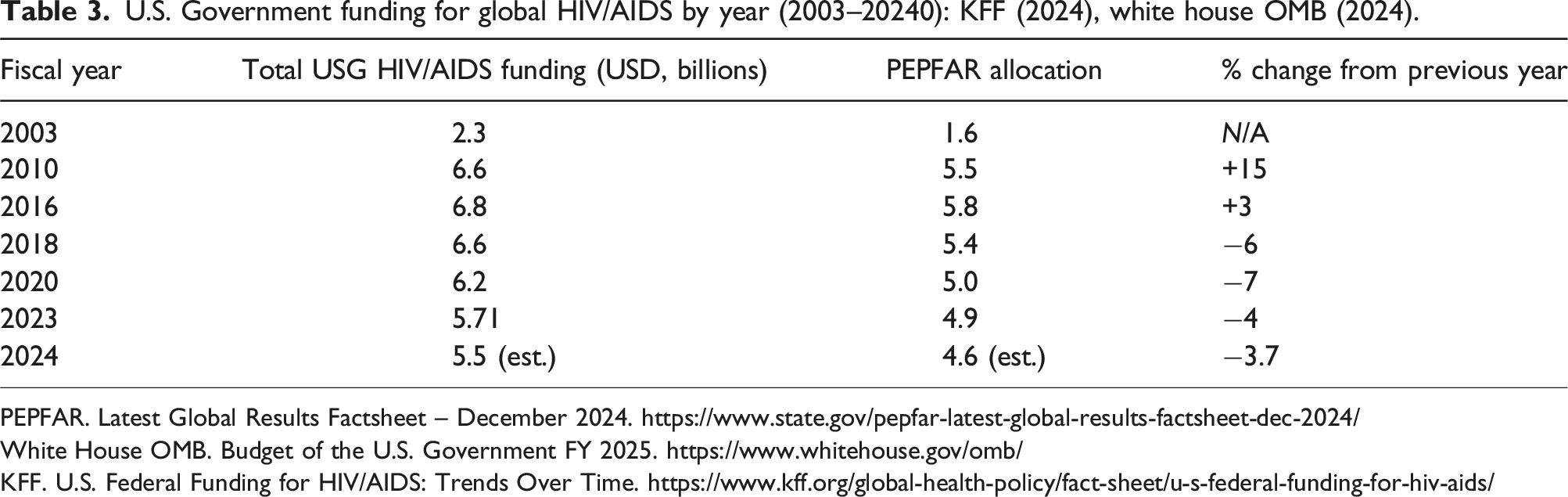
PEPFAR. Latest Global Results Factsheet – December 2024. https://www.state.gov/pepfar-latest-global-results-factsheet-dec-2024/
White House OMB. Budget of the U.S. Government FY 2025. https://www.whitehouse.gov/omb/
KFF. U.S. Federal Funding for HIV/AIDS: Trends Over Time. https://www.kff.org/global-health-policy/fact-sheet/u-s-federal-funding-for-hiv-aids/
From leadership to isolation: How U.S. Conservatism is reshaping global health
This polarization of global health issues is not new. A notable example is the Helms Amendment of 1974, which prohibited U.S. foreign aid from supporting abortion as a method of family planning. In recent decades, however, an increasing number of health issues have become politically polarized between democrats and republicans. Global health has become subject to shifting priorities with changes in U.S. administrations, often influenced by internal politics and differing interpretations of American values. This trend intensified in recent years due to rising tensions between liberal and conservative ideologies. The conservative movement, particularly under Donald Trump’s “Make America Great Again” agenda, emphasized national sovereignty and self-reliance, often leading to isolationist policies. This was reflected in decisions such as withdrawing from the World Health Organization and the Paris Climate Agreement, as well as reducing funding to the United Nations. International treaties and organizations were framed as threats to U.S. sovereignty and interests. Consequently, global health was deprioritized in favor of a domestic conservative agenda that emphasized traditional family values, “protecting life,” and promoting so-called “moral behaviors”. 11
The rise of political conservatism was reflected in Trump’s administration, particularly through the executive orders taken at the beginning of his second mandate. Global health was struck with a strong hit, fundamentally altering the entire U.S. foreign health policy—from leadership to isolationism. 12 This isolationism was accompanied by restraints and pressure on medical research within the U.S. as well, targeting specific populations and issues. One of the most affected areas was HIV/AIDS-related activities, where a 90-day pause was announced on all U.S. foreign assistance, including activities supported by the PEPFAR and UNAIDS. Additionally, an order was sent to the Centers for Disease Control and Prevention (CDC) and the National Institutes of Health (NIH) to suspend research into key populations. 13 For example, multiple resources disappeared from the CDC website, including materials related to HIV, sexually transmitted infections, contraception, women’s reproductive health, and gender-affirming care. 14
On January 28, 2025, the U.S. Secretary of State approved an “Emergency Humanitarian Waiver” to allow specific activities to continue during the 90-day pause. The waiver was later communicated to PEPFAR on February 1, 2025. It permitted certain HIV-related services, such as treatment, life-saving care, counseling, and prevention of mother-to-child transmission, while restricting others. 15
This funding freeze and limited waiver are linked to far-right conservative views that label HIV/AIDS as a “lifestyle” disease, claiming that abstinence and education are the most effective forms of prevention. 16 According to Senator Marco Rubio, “This waiver does not apply to activities that involve abortions, family planning conferences, administrative costs… Gender or DEI (diversity, equity, and inclusion) ideology programs, transgender surgeries, or other non-life-saving assistance.”
The fragile future of global health equity and emerging opportunities
After the 90-day pause was announced on all U.S. foreign assistance on January 20, 2025, international, regional, and local entities and governments started working towards finding solutions and advancing strategies to respond to the pause and towards estimating the impact of the funding cut. UNAIDS put together a detailed weekly report to assess the impact of the funding cut as well as reports by countries. In April 2025, UNAIDS estimated an additional 6.6 million new HIV infections between 2025 and 2029, in addition to over 4.2 million AIDS-related deaths in the same period, in the event the programmes supported by PEPFAR are fully and permanently discontinued. 17 Knowing the difficulty of estimating the short- and long-term impact of funding disturbance, UNAIDS considered the worst scenarios, and its reports presented multiple prediction models such as the GOALS model from Avenir Health, the Optima model from Burnet Institute, as well as other models. They didn’t all present the same estimations, but they all showcased the urgency of the situation and the finding of alternatives.
The HIV/AIDS statistics show that low- and middle-income countries still have the highest numbers, and these countries heavily rely on external funding, especially that provided by the U.S. The reliance on external funding as the primary source of support in this epidemic has been a subject of much debate in these countries. Many governments, particularly after the funding cuts under the Trump administration, have made efforts to launch local initiatives to compensate for the loss of funding. In sub-Saharan African countries, where the highest rates of HIV/AIDS and external funding are concentrated, the average expenditure on health is 5.1% of GDP, which is one of the lowest worldwide. Only 6% of total public health spending is directed toward developing health infrastructure. This low level of public health spending has created a gap, increasing reliance on external funding, especially since this funding is typically focused on specific diseases rather than the entire health system. 18 The lack of sustainable strategies and responses from local governments is not only linked to low spending but also to the path dependency phenomenon. 19 This dependency is shaped by the historical legacies of colonialism, which left African nations with fragile institutions and governance structures.
HIV/AIDS burden and health system financing in selected LMICs. UNAIDS (2024), World Bank (2024).

World Bank. Global Health Expenditure Database. https://databank.worldbank.org/source/world-development-indicators
UNAIDS. Global HIV & AIDS statistics — Fact sheet. https://www.unaids.org/en/resources/fact-sheet
To break through path dependency, countries heavily reliant on external funding for HIV/AIDS must adopt several measures, including increased financing to the health sector, which can reduce this reliance and enable governments to respond effectively to epidemics and diseases. The financing can come directly from government spending, as seen in Malawi and the Philippines, which plan to increase their HIV/AIDS funding in the 2025/2026 government budget. 20 It can also come through partnerships between the government and the private sector, such as the 2015 health service provision partnership between the Kenyan government and GE Healthcare. 18 Financing can also come through direct investment in the health sector by financial institutions and investors. For example, Nigeria has put a plan in place to locally produce drugs and test kits by 2025 as part of a larger plan focused on local initiatives and funding. 21 Countries can also create regional partnerships to join efforts and share resources. For example, in Nigeria, government agencies held the first-ever conference on HIV prevention in May 2024 to advance strategies in the fight against HIV/AIDS. The Chairman of the House Committee on HIV/AIDS, Tuberculosis, and Malaria (ATM), Amobi Ogah, focused on reducing reliance on external donors. 22 At the institutional governance level, governments must dismantle colonial-era institutions and create local governance methods and institutions within the local context.
Conclusion
Tremendous global progress has been achieved in the fight against HIV/AIDS. Lives have been saved, care delivered, and science advanced. Yet, as international funding recedes, particularly from the U.S., the future hangs in the balance. The path forward requires locally anchored, financially sustainable, and politically independent health systems. As decisions on U.S. funding cuts are postponed once more, the global health community must act decisively. The risk is real and growing.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.