
Abstract
Background
Adherence to HIV care is pivotal for achieving viral suppression, preventing viral transmission, and improving health outcomes. Despite advancements in antiretroviral therapy, many people living with HIV (PLHIV) are disengaged from care, compromising treatment effectiveness.
Methods
A retrospective cohort study was conducted on 81 episodes of care dropout at a Portuguese hospital between 2018 and 2024. A multidisciplinary team (physicians, nurses, social workers, and mental health professionals) implemented a structured program to reengage patients. Demographic, clinical, and socioeconomic data were collected at baseline and after 6 months.
Results
79% percent of the participants returned to care, with 68% resuming antiretroviral therapy. Although most patients achieved improved viral load suppression after returning, 27% were lost to follow-up after 6 months. Foreign-born individuals were associated with a lower likelihood of re-engagement. Common barriers include financial hardship, limited social support, and unaddressed mental health needs.
Conclusions
A multidisciplinary approach effectively reconnected PLHIV to care and achieved enhanced virological outcomes. However, persistent socioeconomic and psychosocial challenges can lead to repeated disengagement. Long-term, targeted interventions, particularly for vulnerable groups, are required to sustain retention and ensure improved HIV management and overall patient well-being.
Keywords
Background
Human immunodeficiency virus (HIV) infection remains a major global health concern. An estimated 39.9 (36.1–44.6) million people were living with HIV worldwide by the end of 2023. 1
Antiretroviral therapy (ART) has transformed HIV from a fatal disease to a manageable chronic condition, greatly improving life expectancy and quality of life for those affected.2–5 ART also prevents ongoing HIV transmission.6–8 However, ART’s success depends on consistent adherence and sustained engagement in care. 9
Despite advancements in HIV care across high-income countries, many people living with HIV (PLHIV) still face difficulties leading to discontinued care or irregular treatment. Disengagement may be seen across the HIV care continuum as many patients struggle to follow their prescribed drug schedules even when they have asymptomatic early stage HIV infection. 10 Treatment interruptions may lead to viral replication, emergence of resistance mutations, increased risk of transmission, and worse health outcomes. 11 Identifying reasons for dropping out and developing strategies to keep people in care are essential for controlling the HIV epidemic. 12
Disengagement from care and subsequent reentry depends on medical, psychological, social, and environmental factors. Multidisciplinary interventions combining medical care, nursing, psychological support, and social assistance is known to be beneficial in addressing these issues. 12
This study aimed to assess the outcomes of ‘Project Drop-Out HIV’, a multidisciplinary initiative to identify and support PLHIV who had disengaged from care, by pursuing three specific objectives: (i) to quantify the proportion of PLHIV who could be successfully re-engaged in care after being classified as lost-to-follow-up (LTFU); (ii) to measure virological and immunological trajectories such as viral-load detectability and CD4 cell count, at three time-points (last visit before disengagement, the re-engagement visit and 6-month follow-up); and (iii) to describe clinical outcomes after re-engagement, namely hospital admissions and recurrent disengagement within 6 months. By specifying these dimensions a priori, we aimed to provide a reproducible evaluation framework for multidisciplinary re-engagement programmes.
Methods
Study design and population
We conducted a retrospective cohort study at the HIV clinic at the Unidade Local de Saúde de Gaia Espinho (ULSGE), a tertiary referral hospital in Portugal. The study included adult patients diagnosed with HIV who had discontinued treatment and were enrolled in the “Project Drop-Out HIV” program from January 2022 to December 2024.
“Project Drop-Out HIV” description
In early 2022, this multidisciplinary program assigned physicians, nurses, pharmacists, social workers, and community-based partners to identify and reengage PLHIV who were LTFU.
Physicians and nurses flagged patients who had missed three consecutive appointments, and pharmacists alerted the team of those who failed to retrieve ART from the hospital pharmacy since January 2018. Nurses verified these lists, triaged the patients, and attempted phone contact. Social workers targeted individuals who remained unreachable and partnered with community resources to encourage re-engagement with treatment. After initial contact and return to care, the social services team provided follow-up support to ensure patient retention and adherence to ART.
Patient identification and inclusion criteria
Patients were included in the program if they: (1) Missed three consecutive medical consultations, and (2) Failed to collect ART as scheduled for a period longer than 3 months beyond the last scheduled date.
This information was gathered from the clinic records and pharmacy logs. Patients who met these criteria were included in the outreach and follow-up program. Patients were excluded from the program if they died, transferred to another institution, or left the country permanently.
Re-engagement and outreach strategy
After the identification, the program used a step-by-step methodology. (1) Initial Screening: Nurses reviewed the flagged records to confirm their eligibility. This team contacted the patients to schedule follow-up appointments and address immediate barriers to care. (2) Community-Outreach: Community-based outreach was coordinated by hospital social workers in close collaboration with local non-governmental organisations (NGOs), homeless shelters and immigrant support services. Trained peer navigators and social workers employed a multimodal strategy that combined (a) venue-based outreach at shelters, harm-reduction centers and migrant associations; (b) field visits to patients’ last known addresses; (c) information-sharing with partner agencies to obtain updated contact details; and (d) mobile-phone contacts to deliver appointment reminders, ART literacy and transport vouchers. This low-threshold, client-centred model facilitated contact with vulnerable individuals, including those experiencing homelessness or social isolation, and is consistent with established strategies for re-engaging PLHIV lost to follow-up.
12
(3) Return to Care: Upon contact, appointments were offered, and individualized interventions targeting mental health, financial, and logistical difficulties were implemented.
Multidisciplinary approach after reengagement
After patients returned to care, four targeted interventions, medical, nursing, social, and mental health, were combined to meet the diverse needs related to adherence and retention.
Recruitment and data collection
For study purposes, patients were identified through the “Project Drop-Out HIV” database, which is updated daily. Data were retrieved on the 1st December, 2024, from medical charts. All personal identifiers (e.g., name, date of birth, address, national health number) were removed and replaced with unique study codes before analysis. The dataset was anonymized and encrypted to ensure confidentiality.
Variables and outcomes
Variables and outcomes were assessed at three time-points. At baseline, the last clinic visit before participants were classified as LTFU, we recorded demographic and clinical characteristics (age, sex, nationality, employment status, education, CDC disease stage, viral load, CD4 cell count), treatment-related data (duration of ART and self-reported adherence), co-morbidities (co-infections, substance use, mental illness) and social context (financial difficulties and available support). At the re-engagement visit we documented the self-reported reason for disengagement and repeated viral-load and CD4 measurements. Six months after returning to care, viral-load and CD4 testing was repeated to characterize short-term immuno-virological outcomes.
The primary outcome was successful re-engagement in care at any point during the audit period. Secondary outcomes were (i) retention in care at 6 months, (ii) virological suppression (<200 copies/mL) and advanced immunosuppression (CD4 count <200 cells/μL) at each time-point, and (iii) hospital admission after re-engagement. Self-reported adherence at baseline was extracted for descriptive purposes but was not analyzed longitudinally because objective adherence metrics (pharmacy refill or electronic pill counts) could not be retrieved reliably during follow-up.
Ethical Considerations
This study was approved by the institutional review board (reference 199/2024-1). The requirement for informed consent was waived.
Statistical analysis
Descriptive statistics were used to summarize participant attributes. Continuous variables were tested for normality (Shapiro-Wilk test) and compared using t-tests or Mann-Whitney U tests. Categorical variables were compared using the Chi-square or Fisher’s exact tests. We performed a longitudinal analysis of the viral load and CD4 count at three time points (baseline, reengagement and 6-month follow-up). Missing data were not imputed. All analyses were conducted using available cases only. The number of participants included in each outcome variable is reported throughout the results to ensure transparency. Paired proportions were compared using McNemar’s test. A binary logistic regression model was used to identify the predictors of successful reengagement. We used IBM SPSS Statistics (version 17.0). The significance level for all inferential tests was set at 0.05.
Results
Of 146 patients identified as LTFU, 65 were excluded (23 left the country, 17 transferred care to another institution, 14 died, and 11 were duplicates), leaving 81 episodes for analysis (Figure 1). Breakdown of the selection of cases.
Baseline characteristics
Characteristics of patients lost to follow-up.

Legend: AIDS – acquired immunodeficiency syndrome; ART – antiretroviral treatment; HBV – hepatitis B virus; HCV – hepatitis C virus; TB – tuberculosis
More than half had socioeconomic challenges; 56.8% reported economic insufficiency, 38.3% were unemployed, 3.7% reported homelessness, and nearly 40% had no recognized social support. Clinically, 39.5% of patients had advanced HIV (AIDS). Common coinfections included Hepatitis C Virus (17.3%), tuberculosis (6.2%), and Hepatitis B Virus (4.9%). Substance abuse was present in over a quarter of people. Anxiety (21.0%), depression (17.3%), and other psychiatric conditions (23.5%) were also identified.
Regarding ART usage, 45.7% had been on treatment for >10 years, 29.6% for 5–9 years, 13.6% for 1–4 years, 6.2% for <1 year, and 4.9% had not yet started treatment. Overall, 79.0% of the participants reported good adherence.
Dropout rates varied between years, with 2023 having the highest rate (28.4%), followed by 2022 (27.2%) and 2021 (14.8%).
Reengagement data and outcomes
A total of 64 (79.0%) patients returned to care after a median 10-month gap, and upon return, 55 (67.9%) patients resumed ART. Two (2.5%) patients required hospitalization.
Statistically significant differences were noted for nationality when comparing the characteristics of those who reengaged and those who did not, as foreign-born individuals had 83.3% lower odds of re-engaging than Portuguese nationals (95% CI for OR 0.049–0.542). No statistically significant differences were noted in the other participants’ characteristics.
At baseline disengagement, 38 (54.3%) participants with available data had detectable viral loads, and 9 (12.3%) had CD4 counts <200/μL. Upon reengagement, 40 (66.7%) patients had detectable viral loads and 12 (20.7%) had CD4 counts <200/μL. Figure 2 shows the comparison of the proportions of patients with detectable viral loads and CD4 counts <200/ul, over time. Immunovirological outcomes along the care cascade. The figure displays the proportion of participants with a detectable viral load (>200 copies/mL) and CD4 counts < 200 cells/μL at three predefined evaluation points: baseline (last clinic visit before classification as lost to follow-up; n = 81), reengagement (n = 64) and six-month follow-up (n = 58). Numbers shown below each bar denote the absolute number of participants with laboratory results available for the respective marker at that visit; percentages were calculated using these denominators.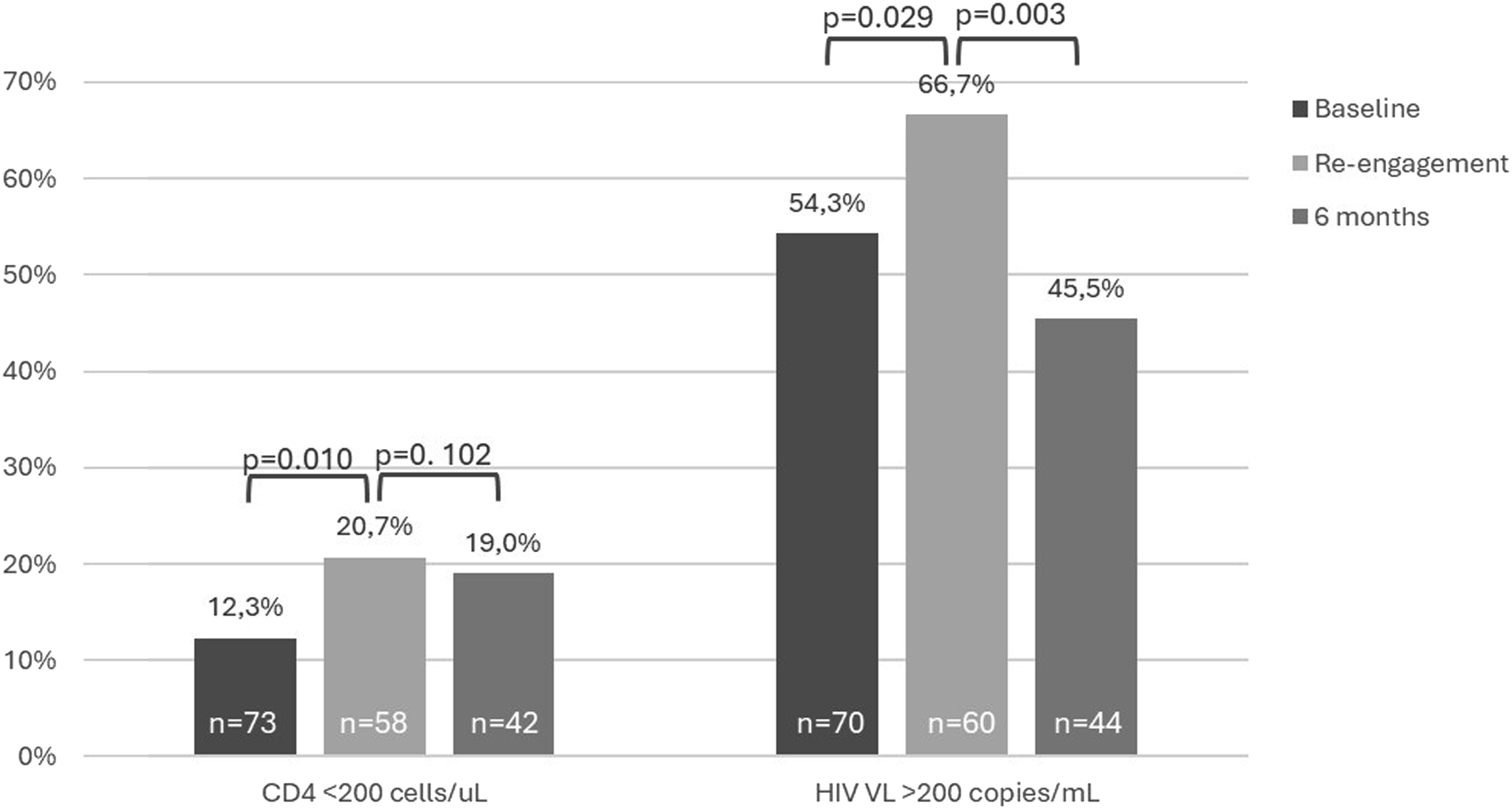
Within 6 months of follow-up, 25 (39.0%) of those who reengaged were LTFU once again. Of these, 19 managed to return to care once again, while six never returned. This means that a total of 23 patients (17 initially and six subsequently) were truly lost to follow-up. Among those whose data were available at 6 months follow-up, only 20 (45.5%) had a detectable viral load and 8 (19.0%) had CD4 counts <200/μL.
Reason for discontinuation and interventions
Patient-reported reasons for disengagement from care.

Summary of clinical and support interventions in patients lost to follow-up.

Discussion
Engagement and retention in HIV care are essential for ensuring optimal HIV-related clinical outcomes. 13 This study highlights the effectiveness of a multidisciplinary strategy in reengaging PLHIV who were LTFU and improving adherence to care. The high rate of return to follow-up (79.0%) underscores the potential of structured, multidisciplinary interventions, The remaining 27.2% of participants who disengaged once again after 6 months reflected the persistent challenges of long-term retention in HIV care and the need for continued, active and assertive support. Similar findings were described in a sampling-based study of 18081 patients which concluded that 26% of PLHIV were LTFU after 2 years of ART. 14
The role of multidisciplinary interventions in Re-engagement
A growing body of evidence supports the importance of multidisciplinary approaches in HIV care. 12 In this study, the collaboration between medical staff, nurses, pharmacists, social workers, and community organizations played a critical role in facilitating patient return. The program addressed key barriers such as stigma, financial insecurity, logistical difficulties, and mental health challenges, all of which are well-documented contributors to loss to follow-up. 14
This study showed that combining data from clinics and pharmacies is a quick and effective way to identify patients with LTFU. However, the lack of a standard definition for “lost to follow-up” was a challenge in this project. Using clear criteria, such as no clinic visits for 180 days instead of three missed consultations, would probably improve reengagement assessments, decrease the gap between LTFU and reengagement, and allow for better comparisons across studies.
Healthcare professionals are key to patient engagement; however, negative attitudes discourage care retention. 15 Medical interventions, such as adjustments to ART regimens, may minimize side effects and better fit into patients’ daily routines. Flexible scheduling, including telephone consultations, may help to accommodate individual needs. Regular medical appointments ensure ongoing clinical monitoring and treatment evaluations. Despite often showing empathy, staff may feel overwhelmed by disengaged patients. Future interventions should provide support for both patients and healthcare providers, helping patients stay in care while equipping healthcare workers with the resources and training needed to manage disengagement and sustain long-term ART adherence. 15
Other studies have demonstrated that provider training enhances engagement. In one study, staff received training in motivational interviewing and patients’ needs assessment. 16 This helped patients navigate health and social services, provided transportation assistance, and addressed other challenges. After 12 months, the number of patient visits increased significantly. Additionally, a retrospective study of 2647 HIV patients found that those receiving multidisciplinary support had higher retention rates and more frequent healthcare visits. Retention increased by 15–18%, reinforcing the effectiveness of team-based HIV care tailored to patient needs. 17 These findings highlight the need for structured, patient-centered support to strengthen long-term retention in HIV care.
Barriers to retention and recurrent dropout
Socioeconomic vulnerability plays a major role in patients’ disengagement. Some patients did not provide a clear reason for disengagement, representing a missed opportunity to understand and address underlying barriers. Financial and travel-related constraints were some of the most commonly reported reasons for dropping out, particularly homelessness and a lack of income. This is consistent with studies showing that transportation costs and distance were major barriers to HIV care. 18
Housing insecurity was identified as a major barrier for some project participants. Programs aimed at stabilizing individuals’ living conditions positively affected treatment compliance. For example, one homeless patient was relocated and rehoused in a stable environment, which greatly enhanced their ability to follow up with care and receive ART. Another patient with severe mobility challenges received regular ambulance transport organized with the aid of a family member. In another case, the local community social support team provided public transport tickets to patients so that they could attend their medical appointments. In addition, visit schedules were adjusted to adapt to public transport timetable.
Reconnecting with patients who had lost touch was challenging, especially those with outdated contact information. Community outreach efforts helped locate and assist vulnerable individuals, such as those experiencing homelessness. Community organizations also helped by distributing prescriptions and providing transportation for medical visits, thus ensuring the continuity of ART. Social workers played a crucial role in addressing complex health-related issues and in guiding patients through social and legal services to remove barriers to care.
Addressing these issues requires a broader policy response beyond the healthcare setting, integrating social services, housing programs, and financial assistance for low-income PLHIV. A non-randomized clinical trial enrolled patients in outreach programs offering appointment support, service coordination, transportation, and HIV education. After 12 months, retention improved, and patients with more than nine contacts in the first 3 months were 50% less likely to have a 4-month care gap than those with fewer contacts. 19
Nationality has emerged as a significant predictor of LTFU, with foreign-born participants facing a higher risk of disengagement. Language barriers, cultural stigma, and lack of familiarity with healthcare rights and services likely contribute to these disparities. 15 A national study on healthcare access among immigrants living with HIV in Portugal found that more than half had already experienced multiple barriers to accessing and using health services. These included administrative complexities, financial instability, social exclusion, lack of information about available services, and discrimination in healthcare settings. 20 Culturally adapted interventions, such as multilingual support, community outreach, and targeted migrant health programs, may help address these challenges. Further research is needed to identify the specific needs of foreign-born PLHIV and to tailor interventions.
Longitudinal outcomes and unmet needs
This study showed that LTFU worsens health outcomes for PLHIV, leading to a higher proportion of patients with detectable viral load and CD4 counts <200/uL. However, the program demonstrated promising clinical results, with participants achieving significant viral load suppression 6 months after re-engagement.
The limited immunological recovery observed at 6 months follow-up underscores the need for enhanced clinical monitoring and additional interventions beyond ART alone. Strategies such as intensive adherence counseling, nutritional support, and mental health care may help improve CD4 recovery, as immune restoration typically requires more time after restarting ART than viral load suppression.
Despite these positive outcomes, 27.2% of participants were lost to follow-up again, emphasizing the persistent challenge of retention in care and the urgent need for sustained, multifaceted interventions. The large proportion of individuals who could not be contacted or who disengaged again after 6 months points to unanswered questions about lived experience. Incorporating qualitative methods, such as in-depth interviews or journey-mapping with patients, peer navigators and clinic staff, could elucidate contextual factors (e.g. stigma, migration stressors, administrative hurdles) that quantitative data alone cannot capture and should be prioritized in future research.
Implications for policy and future directions
The results of this study have important implications for HIV-care programs, particularly in high-income settings with diverse patient populations. First, structured, multidisciplinary, re-engagement should be the standard practice in HIV care facilities. Second, targeted strategies are needed for at-risk groups, particularly for foreign-born citizens and newly diagnosed individuals. Third, addressing the social determinants of health, including housing and financial stability, should be an integral part of HIV retention efforts.
Further investigations should also include qualitative approaches to explore the lived experiences of individuals lost to follow-up, especially those without documented reasons for disengagement. These methods could uncover hidden barriers to care and inform the design of more tailored, patient-centered interventions.
The COVID-19 pandemic accelerated the adoption of telehealth in HIV care, and emerging evidence suggests that it may improve retention. 21 Expanding telemedicine options for follow-up consultations, medication refills, and mental health counseling could help mitigate logistical barriers, particularly for those facing transportation challenges.
Subsequent studies should focus on the long-term sustainability of retention strategies and evaluate how different interventions impact patient outcomes beyond 6 months. Additionally, cost-effectiveness analyses are needed to determine the components of multidisciplinary programs that offer the highest impact relative to resource allocation. Given the high rate of re-disengagement, studies should explore the behavioral and psychosocial factors influencing recurrent LTFU and how personalized adherence interventions can address these challenges.
Study limitations
Several limitations of this study must be considered when interpreting these findings. First, this was a single-center study, limiting the generalizability to broader populations with different healthcare systems or sociocultural dynamics. Second, self-reported adherence data may be subject to recall or social desirability biases. Although self-reported adherence at baseline suggested generally good compliance, we were unable to reassess adherence after re-engagement due to incomplete pharmacy refill records. Future cohorts should integrate objective adherence measures (e.g. electronic refill databases or therapeutic drug monitoring) to clarify how re-engagement affects sustained medication taking. Third, retrospective data collection may have resulted in missing or incomplete information, particularly regarding the socioeconomic factors. The study is also subject to selection bias, as it only includes individuals who could be successfully located and agreed to re-engage with care. Patients who remained unreachable or declined to return may differ in important ways, such as social vulnerability, mental health status, or health literacy. As a result, the findings may not be generalizable to the broader population of PLHIV who are lost to follow-up. Additionally, the follow-up period was limited to 6 months; longer-term retention outcomes remain uncertain. Future multicenter studies with extended follow-up would provide a more comprehensive understanding of the retention dynamics.
Despite these limitations, this study provides strong evidence that a multidisciplinary approach significantly improves reengagement in HIV care.
Conclusion
This study suggests that a multidisciplinary approach can facilitate reengagement of PLHIV who have dropped out of care. While the high reengagement rate is encouraging, the relatively low proportion of participants with follow-up viral load and CD4 data, combined with modest immunologic and virologic outcomes, underscores the need for cautious interpretation. These findings highlight that reengagement is only the first step; sustained retention and clinical improvement remain challenging, particularly in the context of persistent socioeconomic barriers. Future interventions should incorporate structural and social support strategies, culturally adapted services, and integrated mental health care to enhance long-term outcomes. Further research with larger samples and more complete follow-up data is needed to validate and scale these multidisciplinary strategies for HIV retention.
Footnotes
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Unidade Local de Saúde de Gaia Espinho (199/2024-1) on December 17, 2024. The need for written informed consent was waived.
Consent to participate
Informed consent for the information published in this article was not obtained because it was waived by the relevant Ethics Committee.
Declaration of conflicting interests
The authors (s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.