Abstract
Background
Drug-sparing antiretroviral treatment (ART) regimens are gaining interest in the treatment of HIV-1. Dolutegravir (DTG), a second-generation integrase inhibitor, has been pivotal in this development, allowing treatment with fewer drugs while maintaining virologic control. This study aimed to analyze and compare treatment persistence in people with HIV (PWH) on DTG-based two-drug regimens (2DRs) and three-drug regimens (3DRs) at an HIV center in Munich, Germany.
Methods
Retrospective, observational, longitudinal analysis using electronic patient records at MVZ München am Goetheplatz. All people with HIV-1 receiving DTG-containing ART regimens—combined with rilpivirine (RPV) or lamivudine (3TC) for 2DRs, or with tenofovir (TAF or TDF) and emtricitabine (FTC), or abacavir (ABC) and FTC for 3DRs—were included. Exclusion criteria included HIV-2 infection or concomitant use of other antiretroviral drugs. The primary endpoint was the comparison of time-to-discontinuation between 2DRs and 3DRs. Secondary endpoints included an analysis of reasons for discontinuation. Kaplan-Meier estimates, log-rank tests, and accelerated failure time (AFT) models were used for statistical analysis.
Results
Overall, 854 individuals were included in the study, with 462 (54.1%) on a 2DR. For the primary endpoint, 141 events occurred. In the unadjusted analysis, treatment persistence was significantly longer in the 2DR group compared to the 3DR group (p = .005, log-rank test). Median persistence was not reached in either group. In AFT models, being on a 2DR was associated with a 74.9% (23.0%–126.8%), 85.7% (30.5%–140.8%), and 98.0% (36.7%–159.0%) longer time-to-discontinuation in the unadjusted, partially adjusted (sex, age, route of transmission), and fully adjusted models (additionally adjusted for CD4 nadir and baseline resistance) after multiple imputation, respectively. For the secondary endpoint, 196 events occurred. Persistence on 2DRs and 3DRs was found to be comparable (p = .190). Reasons for discontinuation included cardiovascular risk, unspecified side effects, gastrointestinal side effects, impaired kidney function, weight gain, convenience (switch to a single-tablet regimen), and other factors. Weight gain (p = .018), impaired renal function (p = .008), cardiovascular risk (p = .004), unspecified side effects (p = .003), gastrointestinal side effects (p = .003), and switching to a single-tablet regimen (p < .001) remained significant after adjusting for multiple testing.
Conclusions
This study found significant associations between the type of antiretroviral treatment regimen (2DR or 3DR) and time-to-discontinuation. DTG-based 2DRs were associated with significantly longer treatment persistence compared to 3DRs, as confirmed in parametric and non-parametric time-to-event analyses and after adjusting for baseline differences. Virologic efficacy was comparable between the two regimens, aligning with previous studies. The main drivers of higher discontinuation rates in 3DRs were side effects, supporting the hypothesis that drug-sparing regimens might contribute to better tolerability and lower toxicity. These findings suggest that drug-sparing regimens could lead to improved long-term treatment adherence. However, the study’s retrospective nature and center-specific characteristics may limit generalizability. More real-world data are warranted to confirm these results.
Keywords
Introduction
Drug-sparing antiretroviral treatment (ART) regimens are experiencing increasing interest in the treatment of HIV, being an intuitive approach to reducing toxicity and increasing long-term tolerability of a lifelong treatment. While three (or more) drugs from different classes were previously needed for sustained virologic control of HIV, modern antiretroviral drugs have become more and more potent and robust, allowing for treatment with fewer components. Dolutegravir (DTG), a second-generation integrase inhibitor (INI) with a high barrier to resistance, has played a major role in this development: DTG with rilpivirine (RPV) or lamivudine (3TC) has become the first available single-tablet two-drug regimen (2DR) in the treatment of HIV-1, based on regulatory trials in people with HIV (PWH) on suppressive ART prior to switching1–3 and for the combination of DTG/3TC, even for people without prior ART. 4 In these trials, DTG-containing 2DRs have demonstrated non-inferiority compared to “traditional” treatment regimens with three antiretroviral agents (3DRs) and have therefore been included in major clinical guidelines for the treatment of HIV-1.
The principle of drug-sparing ART has been met with considerable scepticism. The concern about higher rates of virologic failure, particularly with therapy-emergent resistance, might be a major reason for that and is based on experiences from previous attempts with less potent drugs. Additionally, critics point out that most potential benefits of drug-sparing treatment options remain speculative, with very little support from currently available evidence. This study, therefore, aimed to analyse and compare the persistence of PWH on DTG-based two- and three-drug regimens in a large single HIV centre in Munich, Germany, and to investigate the reasons for discontinuations in order to identify trends in efficacy, tolerability, and toxicity.
Methods
A retrospective, observational, longitudinal study was conducted at an HIV research and clinical care center (MVZ München am Goetheplatz) in Munich, Germany, an urban center covering not only Munich but a vast part of the south-west area of Germany with a total number of approximately 3000 people with HIV Data were collected from electronic patient records.
The study included all patients diagnosed with HIV-1 who had been receiving a DTG-containing ART regimen in combination with either RPV or 3TC (2DR group) or with tenofovir (alafenamide [TAF] or disoproxil [TDF]) plus emtricitabine (FTC) or abacavir (ABC) plus FTC (3DR group) as of December 31st, 2019. Patients were followed up until December 31st, 2019, with a minimum follow-up period of 1 year. Thus, individuals who initiated treatment in 2019 were monitored for at least 1 year after switching. People with HIV-2 infection (also if concomitant) were excluded from the analysis.
For those on a 2DR, any available data from a previous DTG-containing 3DR regimen were excluded to ensure that each patient was only included once in the analysis. Exclusion criteria included documented HIV-2 infection or the concomitant use of any other antiretroviral drug together with the previously mentioned regimens. Due to the use of anonymised routine clinical data, this study did not require ethical approval.
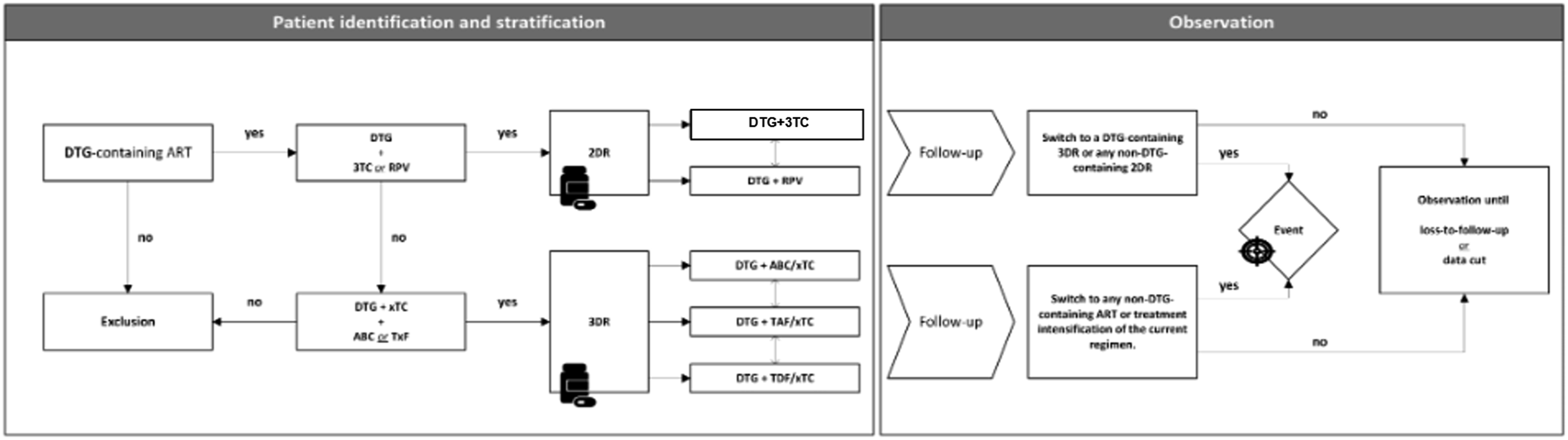
The primary endpoint was the comparison of time to discontinuation between the groups of people on two- and three-drug regimens, with discontinuations excluding switches between one DTG-containing 2DR to another DTG-containing 2DR, or from a DTG-containing 3DR to another DTG-containing 3DR, unless for a lack of efficacy. For the secondary endpoint, the definition of discontinuation included any switch, even if occurring within the same group. Exploratory endpoints included analysis of underlying reasons for discontinuation (as defined for the primary endpoint). A graphical representation of patient identification, stratification, and observation can be found in the appendix.
Time-to-event analyses were used to compare treatment persistence for 2DRs with 3DRs. Kaplan-Meier estimates and curves were used to analsze the persistence on treatment for the entire group. Kaplan-Meier curves were also used for a stratified comparison between the two treatment groups with the log-rank test for an unadjusted, non-parametric comparison. Additionally, accelerated failure time (AFT) models were used to estimate the effect of the treatment (2DR or 3DR) on discontinuation. Three AFTs were fitted: For the first model, only the treatment group was included. The second model was adjusted for baseline imbalances by including all variables with significant group differences at baseline into the model. In order not to lose too much precision, the adjustment was restricted to variables with <10% missing data. For the third model, all variables for which significant differences between the groups were found at baseline were included after multiple imputation. For each of the models, the distribution of time-to-event-times were assumed to belong to one of the following: Weibull, gamma, exponential, log-logistic, or log-normal and chosen based on information criteria (AIC and BIC); log-normal distributions were most supported by the data for all three models.
For the analysis of reasons for discontinuation, proportions of reasons among the entire group were calculated, and the difference between two proportions together with 95% confidence intervals was computed; proportions were compared using a two-sided, two-sample Z-test.
A significance level of
Microsoft Copilot and ChatGPT 4o were used to support copy editing.
Results
Data on demographic and clinical data of the study sample in general, as well as per treatment stratum.

p-values refer to Mann-Whitney tests and χ2 tests for continuous and dichotomised variables, respectively. *W-statistic;#χ2 -statistic (with one degree of freedom). MSM: Men who have sex with men; 2DR: two-drug regimen; 3DR: three-drug regimen.
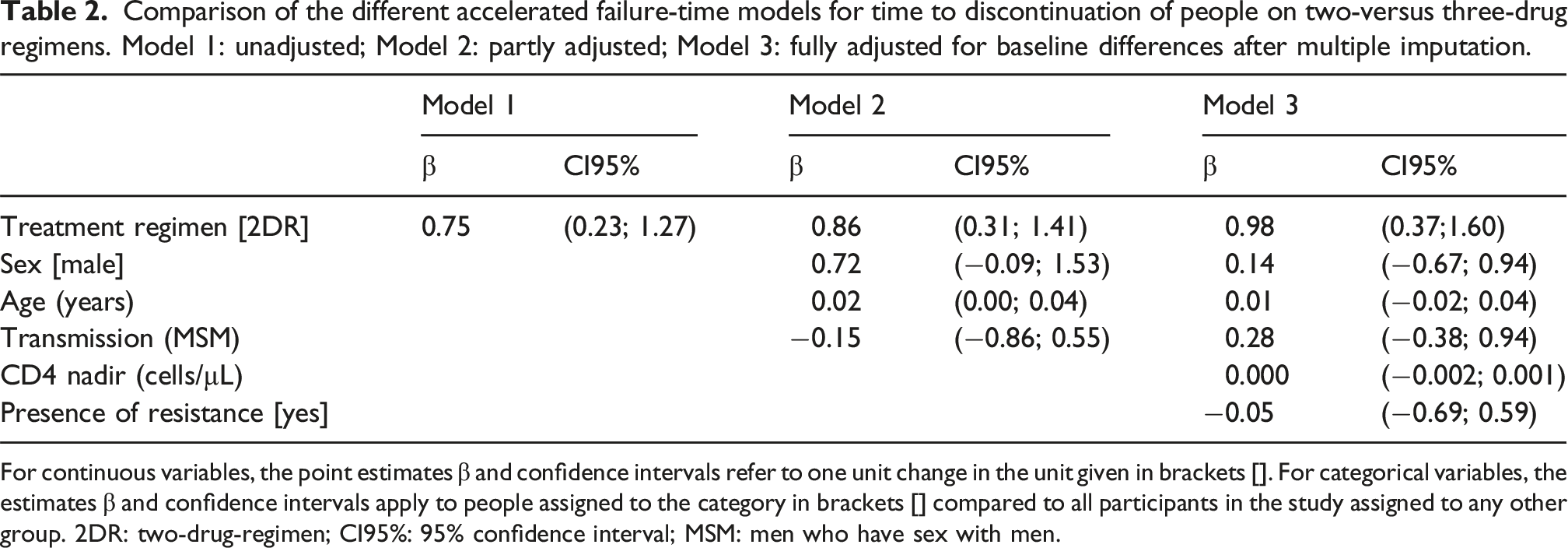
For the primary endpoint, 141 events occurred. Kaplan-Meier curves for persistence on treatment are displayed in Figure 1. Persistence on 2DRs was significantly longer than on 3DRs in unadjusted analysis (p = .005 for log-rank test); median persistence was not reached in either group. Results of the different AFT models can be found in Table 2. Being on a 2DR was associated with a 74.9% (23.0%; 126.8%), 85.7% (30.5%; 140.8%), and 98.0% (36.7%; 159.0%) longer expected time to discontinuation in the unadjusted, partially adjusted, and fully adjusted models after multiple imputation, respectively. Kaplan-Meier curve of persistence on DTG-based two- and three-drug regimens in the study sample for the primary endpoint. 2DR: two-drug regimen; 3DR: three-drug regimen. Comparison of the different accelerated failure-time models for time to discontinuation of people on two-versus three-drug regimens. Model 1: unadjusted; Model 2: partly adjusted; Model 3: fully adjusted for baseline differences after multiple imputation. For continuous variables, the point estimates β and confidence intervals refer to one unit change in the unit given in brackets []. For categorical variables, the estimates β and confidence intervals apply to people assigned to the category in brackets [] compared to all participants in the study assigned to any other group. 2DR: two-drug-regimen; CI95%: 95% confidence interval; MSM: men who have sex with men.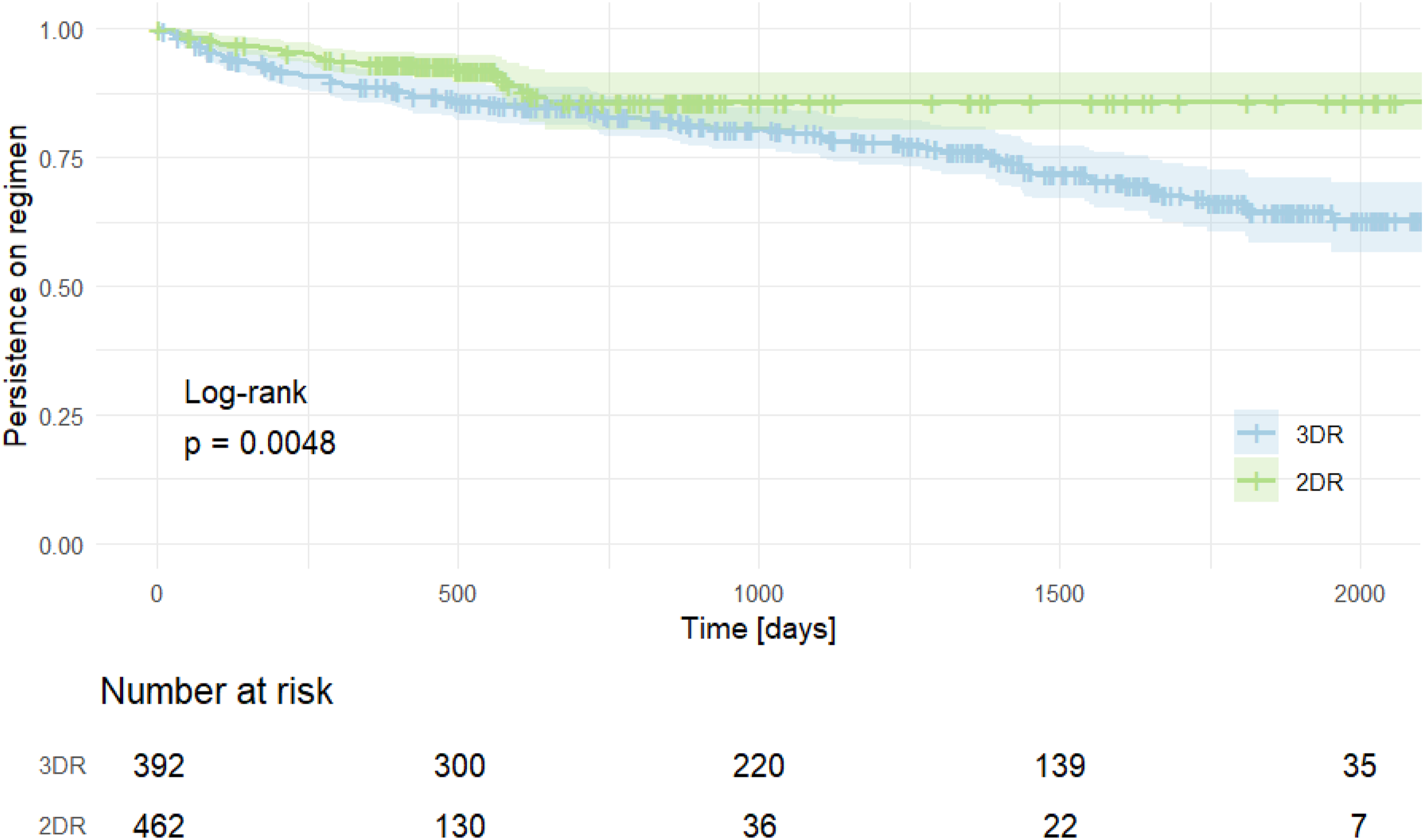
For the secondary endpoint, 196 events occurred. Kaplan-Meier curves for persistence on treatment are displayed in Figure 2. Persistence on 2DRs and 3DRs was found to be comparable (p = .190). Kaplan-Meier curve of persistence on DTG-based two- and three-drug regimens in the study sample for the secondary endpoint. 2DR: two-drug regimen; 3DR: three-drug regimen.
Figure 3 illustrates the reasons for discontinuation, testing them in an exploratory manner, without adjustments for multiple testing. Switches for cardiovascular risk, unspecified side effects, gastrointestinal side effects, impaired kidney function, weight gain, convenience (switch to a single-tablet regimen), and ‘other’ reasons occurred more frequently in the 3DR arm. Weight gain (p = .018), impaired renal function (p = .008), cardiovascular risk (p = .004), unspecified side effects (p = .003), gastrointestinal side effects (p = .003), and single-tablet regimens (p < .001) remained significant after adjusting for multiple testing. Comparison of reasons for discontinuation between the two treatment groups. Bars indicate the frequency of reasons for discontinuation for two-drug regimens (bars to the left) and three-drug regimens (bars to the right). Dots (•) indicate the mean difference between the proportions together with the 95% confidence intervals. Dots on the right side of the 0% threshold indicated higher rates of discontinuation in the three-drug regimen group.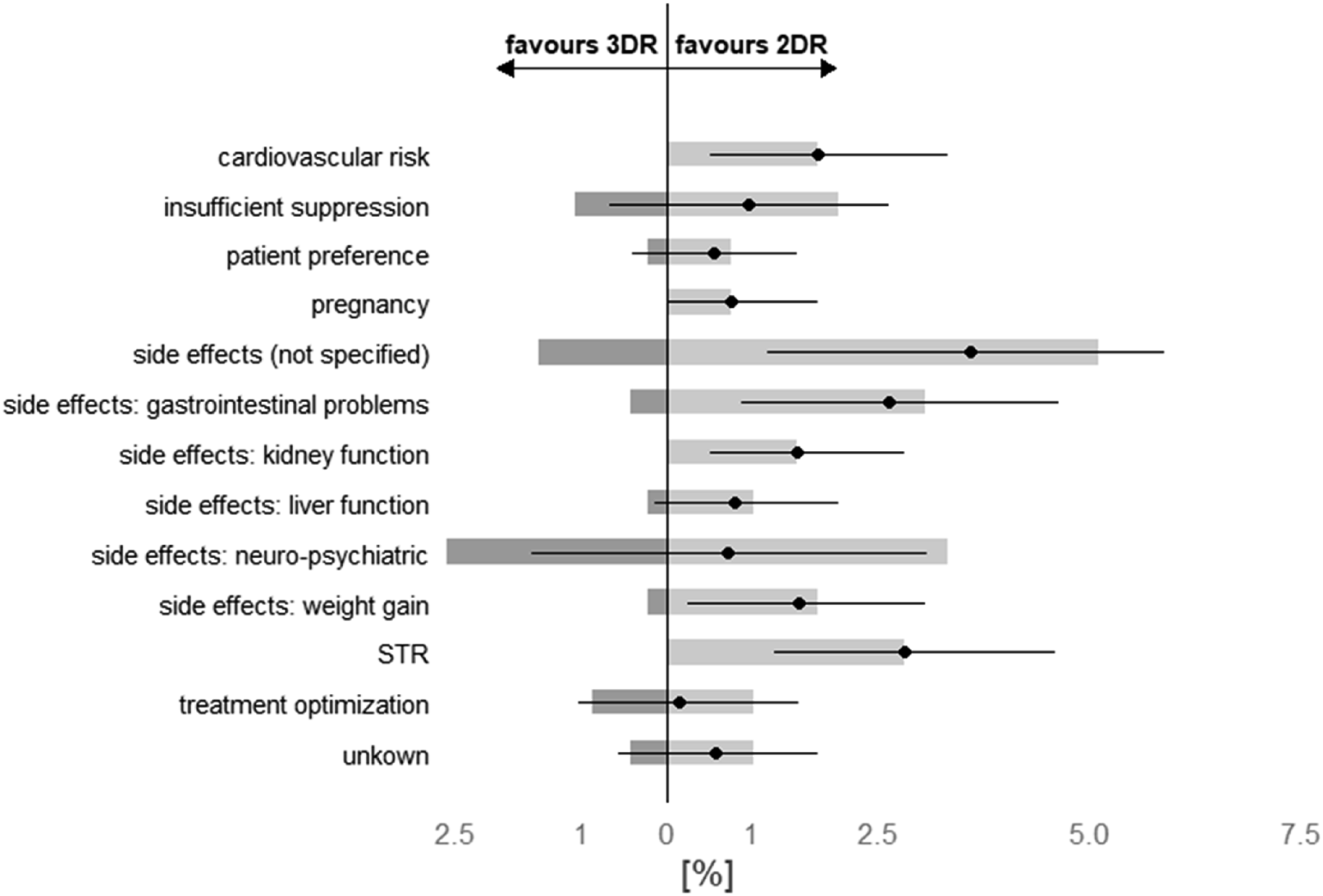
Altogether, 13 patients discontinued treatment for lack of efficacy. Of them, 8 (61.5%) were on a 3DR and had HIV-1 RNA of 57, 164, 173, 191, 218, 241, 301, and 561 copies/mL at discontinuation, while 5 (38.5%) were on a 2DR with HIV-1 RNA levels of 24, 73, 205, 354, and 1280 copies/mL.
Discussion
In our study, we found significant associations between the type of antiretroviral treatment regimen (2DR or 3DR) and the time to discontinuation. Being on a dolutegravir-containing two-drug regimen was associated with significantly longer time-to-discontinuation compared to dolutegravir-containing three-drug regimens. This was confirmed in parametric and non-parametric time-to-event analyses and remained true after adjusting for baseline differences between the two groups. Our findings are therefore in line with real-world evidence from the US, where higher rates of discontinuation were also found in DTG-containing 2DRs versus DTG-containing 3DRs. 5
Before having a look at other reasons for discontinuation, it is worth mentioning that there were no differences in virologic efficacy between the two treatment strategies, in line with what has been published before, in parts including other second-generation INIs,5–7 although some real-world data seem to imply that virologic failure might occur more often on a DTG-containing 2DR.5,6 Comparisons with other cohorts must, however, be done with care as underlying populations, previous therapies, and many other potentially relevant factors might be remarkably different between different sites., For the 13 people in our study sample who discontinued treatment for lack of efficacy, 5 and 8 came from a three- or two-drug regimen, respectively. Being a retrospective observational study, there were no clearly defined criteria of ‘lack of efficacy’ and therefore these discontinuations were rather based on a shared consent between doctors and patients. Of note in this context, only 7/13 people had an HIV-1 RNA >200 copies/mL at discontinuation, a commonly used threshold to define virologic failure in clinical trials.
So, what caused the difference in persistence on two-versus three-drug regimens? After adjusting for multiple testing, management of side effects was one of the main drivers of the higher rates of discontinuation in the 3DR arm. These findings can be seen as support for the hypothesis that drug-sparing regimens might contribute to better tolerability and less toxicity. One might argue that some of the switches we observed might not have happened without the use of TDF- (kidney) or ABC-containing (cardio-vascular risk) regimens. Substituting one drug with another might, however, in turn be associated with other, drug-specific adverse events, which, in the case of TAF, as the most likely alternative, could have been metabolic changes and weight gain. Even though the role of TAF on weight gain remains a matter of scientific debate, the recently published results from the PASO-DOBLE study seem to support TAF as an independent risk factor for weight gain. 7
Our data might be some of the first pieces of real-world evidence to support not only the non-inferior efficacy but also demonstrate a true advantage of 2DRs in terms of (mostly side-effect) associated discontinuation, although positive outcomes in terms of surrogate markers for cardio-metabolic health have been published from real-world data recently.5,8,9 More real-life data is warranted to confirm our results. However, even if results for tolerability and toxicity should turn out to be equivocal throughout different cohorts, it seems increasingly difficult to understand why we should add a (third) drug to a therapeutic regimen that already achieves the goal of virologic suppression with only two active ingredients in the vast majority of people: while not needed for virologic reasons in neither clinical trials5,10 nor under real-life conditions,5–9,11 or better control of residual inflammation,12–14 PWH on 3DRs might experience more side effects than people on a 2DR built on the same but fewer ‘ingredients’. This might also be reflected in the higher degree of treatment satisfaction reported by PWH after treatment simplification to DTG-based 2DRs. 15
Our study has several limitations. Being a retrospective study, the data used for this study have not been captured in a prospective or standardised way. Also, centre-specific features and particularities in terms of patient characteristics might limit the generalizability of our findings to a broader population. It should be noted, however, that our data is highly consistent with other reported real-world data in terms of efficacy, as stated previously. It should also be noted that the design of the study was set up conservatively, as people on a DTG-containing interest in the study were left-censored for the previous use of a DTG-containing 3DRs. This was done to acknowledge the fact that many people were switched ‘only’ based on the increasing literature of equality of the two principles, rather than for reasons of interest, such as tolerability and toxicity. On the other hand, this might have biased the groups in a way that the 3DR subgroups were the more “difficult-to-treat” group. We do, however, not think that this has a major impact on the finding that additional drugs potentially lead to more side effects or other reasons for discontinuation.5,8,9 Among the 13 individuals who discontinued treatment due to a lack of efficacy, 5 were on a three-drug regimen and 8 were on a two-drug regimen. Being a retrospective observational study, there were no clearly defined criteria for ‘lack of efficacy’ and therefore these discontinuations were primarily based on a shared consent between doctors and patients. Of note in this context, only 7/13 people had HIV-1 RNA levels >200 copies/mL at discontinuation, a commonly used threshold to define virologic failure in clinical trials.16,17,18
The strengths of our study include the considerable sample size derived from a diverse population of people with HIV and the ‘adjustment’ for the main agent of each of the antiretroviral regimens under investigation, allowing for a good estimation of the potential benefits of drug-sparing regimens.
Conclusions
In this large cohort of people with HIV on dolutegravir-containing regimens, people on 2DRs demonstrated longer time-to-discontinuation compared to those on 3DRs. Within the limitations of a retrospective study, this data supports the notion of drug-sparing therapies being not only comparable to 3DRs in terms of efficacy but also having a probably more favourable profile when it comes to tolerability and toxicity.
Footnotes
Ethical considerations
The use of anonymized data obtained from clinical routine did not require ethics approval.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SN, EW and CJO report personal fees from services for Gilead Sciences, MSD, and ViiV Healthcare/GSK, as well as educational support from Gilead Sciences and ViiV Healthcare. FS, AK, and CW report educational support from Gilead Sciences and ViiV Healthcare.
AI does not report any conflicts of interest.
Data Availability Statement
Data can be made available by the corresponding author upon reasonable request.
Appendix
Flow chart on patient identification, stratification, and observation for the study sample. ABC: abacavir; ART: antiretroviral treatment; DTG: dolutegravir; RPV: rilpivirine; TAF: tenofovir alafenamide; TDF: tenofovir disoproxil fumarate; TxF: collective term for either TAF or TDF; xTC: collective term for emtricitabine and lamivudine; 2DR: two-drug-regimen; 3DR: three-drug-regimen.