
Abstract
Background
This study investigates drug-drug interactions (DDIs) in people with HIV (PWH) receiving antiretroviral therapy (ART) with comorbidities. We focus on pharmacological factors and evaluate DDI notifications from online databases, emphasizing the clinical relevance of pharmacokinetic, pharmacodynamic, and pharmacogenomic variations.
Methods
A comprehensive literature search was conducted using PubMed, ScienceDirect, Google Scholar, and the Cochrane Library for studies published between January 2019 and September 2024. Newly identified DDI evidence was analyzed by comparing DrugBank, Drugs.com, and the Liverpool HIV databases.
Results
Eleven studies met the inclusion criteria. The findings of these studies showed the critical importance of considering DDIs in PWH with tuberculosis (TB), malaria, and pulmonary hypertension. Severe adverse drug reactions associated with ARTs, including efavirenz, darunavir, nevirapine, and atazanavir-ritonavir, especially when combined with treatments for TB and malaria. Key interactions included reduced drug levels from rifampicin and QT prolongation from artemether-lumefantrine. Pharmacogenomic factors, such as CYP2B6 slow metabolism during pregnancy, influenced outcomes. Database discrepancies were noted, especially for riociguat interactions and ritonavir through inhibition of P-gp or OATP1B1 functions.
Conclusions
DDIs in PWH receiving ART with comorbidities have highlighted the crucial need for personalized treatment. Incorporating pharmacokinetic, pharmacodynamic, and pharmacogenomic factors is essential for optimizing therapy outcomes.
Introduction
The management of human immunodeficiency virus (HIV) has significantly improved with the introduction of antiretroviral therapy (ART), leading to better long-term outcomes and quality of life for people with HIV (PWH).1,2 However, as ART regimens become increasingly complex, particularly in individuals with comorbid conditions such as tuberculosis (TB), malaria, cardiovascular disease, and mental health disorders, the risk of severe drug–drug interactions (DDIs) also increases.3–6 Epidemiological evidence suggests that coadministration of ART with other medications may heighten the risk of toxicity, therapeutic failure, and adverse drug reactions (ADRs).3,6–9 For instance, efavirenz has been shown to reduce plasma concentrations of atovaquone/proguanil by 43%–75%, potentially compromising malaria prophylaxis. 8 Protease inhibitors such as atazanavir/cobicistat and darunavir/cobicistat have been reported to significantly increase rosuvastatin levels, with corresponding risks of rhabdomyolysis and severe myopathy. 9 DDIs are particularly prevalent among vulnerable populations, including older adults, pregnant individuals, and those with multiple comorbidities,7,10,11 further complicating HIV treatment strategies.
Many ART-related DDIs involve pharmacokinetic and pharmacodynamic mechanisms, particularly cytochrome P450 enzymes such as CYP3A4 and CYP2C9. 6 DDIs contribute to various ADRs.3,6,10–12 A deeper understanding of the mechanistic pathways of ART-related DDIs is essential for optimizing treatment outcomes and minimizing harm. Despite an expanding body of literature on ART-associated DDIs, most prior reviews (1995–2022) had focused narrowly on food interactions, herbal products, and single-drug analyses. 9 There remains a lack of comprehensive evaluation of the full spectrum of ART-related DDIs, particularly in PWH with co-existing medical conditions.9,12–14 Moreover, mechanistic factors such as drug metabolizing enzyme induction/inhibition, and transporter modulation are frequently underexplored. Another underrepresented area is the role of pharmacogenomic variability in determining individual DDI outcomes. 15 Considering these factors in HIV management, including disease burden, polypharmacy, and genetic variability, can improve treatment safety and efficacy, highlighting the need for a comprehensive approach to HIV treatment. In addition, clinical guidelines and recommendations for HIV treatment have been recently updated. 16
This study aims to synthesize and evaluate recent evidence on DDI involving ART, focusing on clinical studies published between January 2019 and September 2024 in the four high-impact databases (the Cochrane Library, PubMed, Google Scholar, and ScienceDirect). This literature review followed systematic review principles based on PRISMA 2020 guidelines. This timeframe reflects recent advancements in ART and evolving drug interaction patterns associated with emerging treatment regimens. In addition to summarizing findings related to pharmacokinetics, pharmacodynamics, and pharmacogenomics, we compared the included studies with three widely used drug interaction resources: DrugBank, Drugs.com, and the Liverpool HIV interaction database to note new information on DDI evidence. These platforms are strengths: DrugBank for detailed pharmacological insights, Drugs.com for broad clinical accessibility, and Liverpool HIV for HIV-specific expertise. The database comparison was used to assess the consistency and coverage of DDI. With its comprehensive approach, this study identified discrepancies in DDI classifications, underlying mechanisms, and severity ratings by integrating data from peer-reviewed literature with curated interaction databases. Our finding has practical implications for managing DDIs in HIV care, equipping healthcare providers with the knowledge to inform personalized strategies and improve patient safety and therapeutic outcomes, thereby instilling confidence in their practice.
Methods
PRISMA compliance
The PRISMA 2020 guidelines were used to conduct this systematic review. 17 The completed PRISMA checklist is available in Supplemental Table S1.
Review protocol
The protocol was not registered in PROSPERO or any other database due to the retrospective nature of the review process. This decision was made to avoid potential bias in the selection of studies, as the review was based on existing literature and did not involve any prospective data collection.
Data searching strategy
Our comprehensive literature search, conducted on 12 September 2024 across four databases (PubMed, Cochrane Library, Google Scholar, and ScienceDirect), was meticulously planned and executed. We used Medical Subject Headings (MeSH) and relevant keywords, including HIV/AIDS, anti-HIV, drug interaction, antiretroviral therapy, treatment, and clinical pharmacology. The search was limited to English-language studies published between 1 January 2019 and 12 September 2024. The search strategy for each database is shown in Supplemental Table S2.
Study selection and data extraction
Six reviewers (PB, LR, PT, PR, NC, CB) were involved in the study selection and data extraction process. Titles and abstracts were independently screened for eligibility by reviewers based on predefined criteria. Full-text screening was conducted for studies deemed potentially relevant. Any disagreements were resolved through discussion and consensus among the reviewers, ensuring the reliability of our process.
Inclusion criteria were: Peer-reviewed clinical studies involving HIV-positive individuals with comorbidities Studies reporting DDIs involving ART Studies reporting data on: sample size, follow-up duration, pharmacokinetic profiles (Cmax, Tmax, AUC), therapeutic efficacy, and/or ADRs
Exclusion criteria included: Studies not involving HIV-positive populations Review articles (conference abstracts, systematic, narrative, or meta-analyses) Preclinical studies (in vitro or in vivo animal models) Articles with incomplete, unclear, or insufficient data
Data from included studies were extracted using a standardized form in Microsoft Excel (Microsoft Corporation, Redmond, WA, USA). Extracted data fields included: ART regimen design, population characteristics, co-medications, reported DDIs, pharmacokinetic/pharmacodynamic/pharmacogenetic findings, ADRs, and drug resistance.
Research questions
The following research questions were addressed: What is the frequency of drug–ART interactions in PWH, with or without comorbidities, and how are these interactions classified as mild, moderate, or severe according to the Common Terminology Criteria for Adverse Events (CTCAE)? Which drugs interact with ART, resulting in pharmacokinetic, pharmacodynamic, or pharmacogenomic changes that impact clinical outcomes? What are the mechanisms of worsened ADRs due to drug-ART interactions, as outlined in DrugBank, Drugs.com, and Liverpool HIV interactions?
Quality assessment and risk of bias
The quality of included studies was assessed using the Cochrane Collaboration’s Risk of Bias Tool, as described in the Cochrane Handbook for Systematic Reviews of Interventions. 18 The following domains were evaluated: sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other sources of bias. Each domain was classified as having low, high, or unclear risk of bias. A summary of risk assessments is provided in Supplemental Table S3.
Outcome analysis
Outcomes were categorized based on the frequency and severity of DDIs (mild, moderate, or severe) from clinical data, with visualization via a Sankey diagram to illustrate the relationship between drug classes and interaction severity. Clinical outcomes were evaluated regarding pharmacokinetic and pharmacodynamic changes, pharmacogenomic associations, ADRs, and instances of drug resistance.
Drug interaction database comparison
To strengthen the clinical relevance of the findings, DDIs identified in the literature were cross-referenced with three widely used drug interaction databases as follows: DrugBank - detailed pharmacological data (accessed 15 October 2024) Drugs.com - user-friendly clinical interface (accessed 15 October 2024) Liverpool HIV Interaction Database - HIV-specific interactions (accessed 20 February 2025)
These resources were chosen for their currency, comprehensiveness, and clinical utility. The comparison allowed identification of discrepancies in interaction severity, mechanistic classification, and notification systems. Findings from this cross-comparison informed a more robust pharmacovigilance framework and clinical interpretation of DDIs in HIV care.
Results
Article selection, screening process, and risk of bias
PRISMA flow diagram shown in Figure 1. We identified 70 articles across the four databases. After removing 20 duplicates, 50 titles and abstracts were screened. Of these, 32 articles were selected for full-text review, but six were unavailable despite repeated attempts. Of the 26 reviewed, 15 articles were excluded due to a lack of HIV-positive populations, pharmacokinetic/pharmacodynamic data, ADR reporting, or data clarity. Ultimately, 11 high-quality studies met the inclusion criteria for data extraction and synthesis. Risk of bias was assessed using the Cochrane Collaboration’s tool. Studies varied significantly in blinding, allocation concealment, and outcome reporting (Supplemental Table S3), with some rated high risk and others low, indicating a need for improved methodological rigor in future research. The PRISMA flow diagram depicted the process of selecting articles for the systematic review.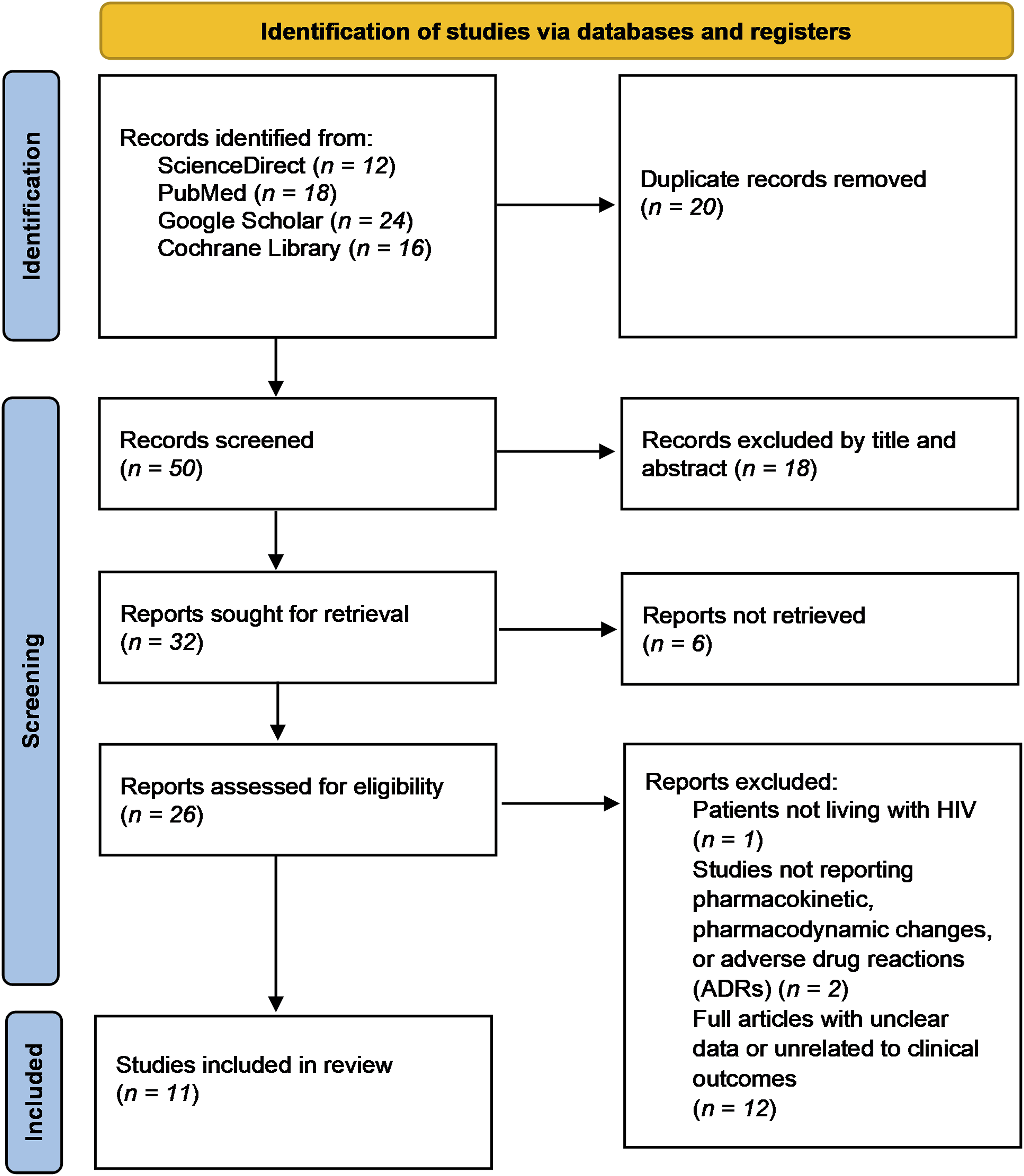
Frequency and severity of drug–ART interactions in PWH
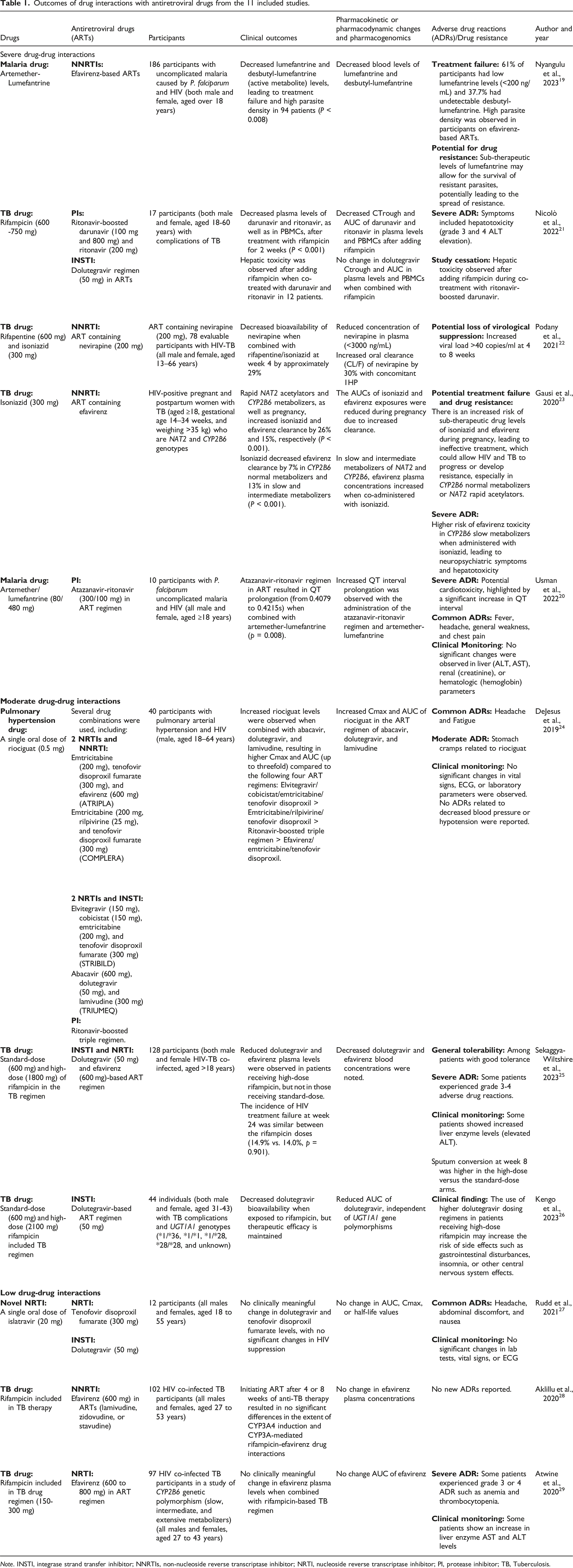
Based on a synthesis of 11 studies, the review identified frequent DDIs involving ART as visualized in a Sankey diagram (Figure 2) and summarized in Table 1. Twelve ART agents were associated with varying degrees of interaction severity. Efavirenz exhibited moderate to severe DDIs when administered with tuberculosis treatments such as rifampicin and isoniazid, as well as with the antimalarial combination artemether-lumefantrine. Riociguat demonstrated moderate interactions with abacavir, lamivudine, and dolutegravir, while weaker interactions were observed between riociguat and other agents, including ritonavir, emtricitabine, tenofovir disoproxil fumarate, rilpivirine, and elvitegravir. Clinically significant adverse effects were noted in particular combinations, such as atazanavir-ritonavir with artemether-lumefantrine, and nevirapine with either rifapentine or isoniazid. In contrast, the combination of tenofovir disoproxil fumarate and dolutegravir with islatravir was well tolerated, with no substantial adverse effects reported. The frequency and severity of drug-ART interactions observed in PWH. Outcomes of drug interactions with antiretroviral drugs from the 11 included studies. Note. INSTI, integrase strand transfer inhibitor; NNRTIs, non-nucleoside reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; PI, protease inhibitor; TB, Tuberculosis.
Impact on pharmacokinetics, pharmacodynamics, and pharmacogenomics
As shown in Table 1, the reviewed literature demonstrated DDIs between ARTs and antimalarial or antituberculosis medications, with important implications for efficacy and safety in HIV co-infected individuals. The efavirenz-based regimen was found to significantly reduce plasma lumefantrine levels, resulting in subtherapeutic concentrations and treatment failure in 61% of patients with malaria co-infection, potentially increasing parasitemia and the risk of resistance development. 19 Atazanavir-ritonavir administered with artemether-lumefantrine was associated with QT interval prolongation, elevating the risk of cardiotoxicity. 20 Rifampicin, when combined with ritonavir-boosted darunavir, reduced ritonavir-boosted darunavir exposure. 21 Similarly, rifapentine and isoniazid coadministration decreased nevirapine bioavailability and increased its clearance, reducing virologic control. 22 In pregnant women with the CYP2B6 slow metabolizer genotype, efavirenz plasma concentrations increased when combined with isoniazid, raising the risk of neuropsychiatric and hepatic toxicity. 23 Conversely, women with rapid NAT2 and normal CYP2B6 genotypes showed lower isoniazid and efavirenz plasma levels, potentially leading to subtherapeutic drug exposure during pregnancy. 23
Integrase inhibitors also showed notable interactions. Coadministration of abacavir, dolutegravir, and lamivudine with riociguat increased riociguat plasma levels in patients with HIV-associated pulmonary hypertension, resulting in moderate ADRs such as abdominal discomfort. 24 While high-dose rifampicin reduced dolutegravir and efavirenz plasma concentrations, virologic suppression was maintained. 25 The decrease of AUC in dolutegravir appeared independent of UGT1A1 polymorphisms; however, higher dolutegravir doses may lead to insomnia and gastrointestinal side effects. 26
In contrast, islatravir, a novel nucleoside reverse transcriptase inhibitor, did not significantly alter the pharmacokinetics of dolutegravir or tenofovir disoproxil fumarate and preserved HIV suppression. 27 Furthermore, low to moderate doses of rifampicin (150–300 mg) showed minimal interaction with efavirenz, supporting the continued use of current dosing regimens in co-infected populations.28,29
Mechanistic insights from literature reviews compared with drug interaction databases
Possible mechanisms of drug interactions with antiretroviral drugs in a clinical setting: A comparison of drug interaction mechanisms based on evidence from DrugBank, Drugs.com and Liverpool HIV notifications regarding safe combinations.

In addition, pharmacogenetic variability and physiological changes during pregnancy were shown to alter ART metabolism significantly. Increased activity of CYP2B6 and NAT2 in normal metabolizers and rapid acetylators was associated with faster clearance of efavirenz and isoniazid, potentially leading to subtherapeutic drug exposure. 23 Conversely, in CYP2B6 intermediate and slow metabolizers, isoniazid inhibited efavirenz metabolism, resulting in elevated plasma levels and an increased risk of neurotoxicity. This genotype-dependent mechanism was not documented in any of the databases reviewed, highlighting the limited integration of pharmacogenomic data in current clinical decision support tools.
Discussion
ART remains essential for improving long-term health outcomes in PWH.29–34 This study offers a novel contribution to understanding the complexities of DDIs between ART and treatments for comorbidities such as TB, malaria, and pulmonary hypertension. This study identified frequent and severe DDIs by including pharmacokinetic, pharmacodynamic, and pharmacogenomic mechanisms, emphasizing the need for more personalized treatment strategies. We evaluated three online drug-interaction databases (DrugBank, Drugs.com, and the Liverpool HIV database), finding that they inadequately represent key interactions, particularly those influenced by genetic factors.
A key finding is the significant interaction between commonly used ART agents, including dolutegravir and efavirenz, and treatments for comorbid conditions. These drugs are standard components of HIV therapy globally.1,2 High-dose rifampicin has been shown to reduce plasma concentrations of both dolutegravir and efavirenz.25,26 However, the effect on dolutegravir was less pronounced, 21 suggesting that ART regimens containing dolutegravir may require fewer adjustments in HIV/TB co-infected patients. Doubling the dolutegravir dose showed that it could counteract this interaction and maintain adequate drug levels. 26 The combination of nevirapine with rifapentine and isoniazid has also been associated with increased viral load and HIV resistance, 22 further emphasizing the need for vigilant clinical monitoring to prevent treatment failure. Similarly, efavirenz combined with artemether-lumefantrine significantly lowers lumefantrine and its active metabolite levels, raising concerns about malaria treatment failure and drug resistance in Plasmodium falciparum. 19 Furthermore, coadministration of atazanavir-ritonavir with artemether-lumefantrine has been linked to QT interval prolongation, 20 a serious concern in HIV patients with malaria comorbidity. These risks necessitate regular monitoring of liver function, neuropsychiatric status, and electrocardiograms, in cooperation with WHO and U.S. Department of Health and Human Services (HHS) guidelines.35,36 Additionally, the discovery of interactions between riociguat and ART drugs with dolutegravir, abacavir, or lamivudine in patients with pulmonary hypertension presents further clinical challenges. This combination may lead to stomach cramps, requiring close supervision. 24 This study noted how administered drugs alter the pharmacokinetics of ART agents. Rifampicin significantly reduced the AUC for dolutegravir and efavirenz.25,26 Conversely, combinations such as tenofovir disoproxil fumarate and dolutegravir with islatravir showed no meaningful pharmacokinetic interactions, 27 indicating their potential suitability for dual therapy regimens. Islatravir does not inhibit major metabolic enzymes or transporters (e.g., CYP1A2, 2B6, 2C9, UGT1A1), making it a promising candidate for future treatment, though it remains under clinical investigation.27,37
Pharmacodynamic interactions were also notable. Efavirenz reduced plasma concentrations of lumefantrine, potentially compromising malaria treatment in HIV-malaria co-infection. 19 Similarly, the interaction between atazanavir-ritonavir and artemether-lumefantrine elevated cardiotoxic risks due to QT prolongation. 20 These studies showed the critical importance of evaluating both pharmacokinetic and pharmacodynamic factors when managing HIV in patients with concurrent infections.
Our study revealed evidence pointing to the role of pharmacogenomics in modulating ART-related drug interactions. Genetic polymorphisms (i.e., CYP2B6 and NAT2) affect the metabolism of efavirenz and isoniazid, increasing the risk of ADRs. 23 It is particularly crucial in pregnant women, where normal metabolizers of CYP2B6 and rapid acetylators of NAT2 may experience subtherapeutic levels of these drugs. In contrast, CYP2B6 slow metabolizers are at risk of severe ADRs such as neurotoxicity and hepatotoxicity. Genotyping patients before treatment could support safer, more effective ART dosing, especially during pregnancy, when hormonal changes further alter drug metabolism. The effect of rifampicin on dolutegravir bioavailability, despite dose adjustments, was not associated with UGT1A1 polymorphisms but rather with the induction of intestinal enzymes or transport proteins. 26 Although no significant pharmacogenetic influence was observed on the rifampicin-efavirenz interaction, 29 the findings emphasize the need to incorporate pharmacogenomic testing into HIV treatment, especially in complex clinical scenarios.
This study evaluated drug interaction mechanisms involving ART and compared interaction data across DrugBank, Drugs.com, and the Liverpool HIV interaction database to assess their consistency and completeness. While three databases support clinicians, pharmacists, and researchers in ensuring the safe and effective use of medications, particularly in managing complex ART regimens for PWH, notable discrepancies were identified. For instance, abacavir, lamivudine, dolutegravir, and riociguat inhibited CYP1A1 and P-gp/BCRP, which was not uniformly reported across the databases. 24 While abacavir was listed in Drugs.com as a CYP1A1 inhibitor, and dolutegravir was shown in DrugBank to inhibit P-gp, the Liverpool HIV database only identified riociguat as a substrate of CYP1A1, CYP3A4, CYP2C8, CYP2J2, and P-gp/BCRP, without acknowledging interactions with the ART agents. This discrepancy showed a lack of harmonization between mechanistic predictions and clinical documentation. Another key example involves ritonavir, which is known to inhibit P-gp and OATP1B1, thereby increasing plasma concentrations of rifampicin and resulting in a risk of hepatotoxicity. 21 Surprisingly, this interaction was not documented in any of the three databases. However, all three did acknowledge that rifampicin induces CYP3A4, leading to decreased plasma levels of ritonavir-boosted darunavir and enhanced ritonavir metabolism. Despite the availability of DDIs from databases, these tools do not always account for genetic variability or physiological changes in pregnancy. 23 During pregnancy, increasing hepatic blood flow and plasma volume accelerated the clearance of isoniazid and efavirenz, possibly compromising therapeutic efficacy. Genetic polymorphisms of slow or intermediate metabolizer variants in CYP2B6 can also impair efavirenz metabolism. Coadministration of isoniazid, which inhibits efavirenz metabolism, can further elevate plasma concentrations and increase the risk of toxicity. 23 Prospective studies would be needed to evaluate the real-world impact of ART-related DDIs across diverse populations, considering genetic variability, physiological changes, and comorbidities. This study has several limitations. The review protocol was not registered in PROSPERO. Only 11 clinical studies were included, and they varied in design, sample size, and reporting quality, resulting in some heterogeneity. Some studies also had a high risk of bias in blinding and outcome reporting, which may affect the robustness of certain conclusions. We excluded observational studies, which may have omitted additional relevant evidence. Our analysis was restricted to DrugBank, Drugs.com, and the Liverpool HIV database; other resources such as Micromedex, Lexicomp, and DIDB® were not included due to limited access. The exclusion of DIDB®, in particular, may have limited our ability to capture more detailed mechanistic insights into transporter- and metabolism-based interactions. Nevertheless, the databases used are widely accessible and provide clinically relevant information for ART-related drug interactions. Most included trials involved small populations, limiting the applicability of results to broader populations. Despite these limitations, our study provided an overview of clinically important DDIs and highlights the need for further research and improved database integration. In addition, although 11 high-quality studies were included, our review did not perform a formal meta-analysis due to differences in outcomes, populations, and pharmacokinetic parameters. As a result, quantitative estimates of ART-related DDIs could not be provided. Future research incorporating individual participant data meta-analysis may strengthen the precision and clinical relevance of these findings.
Conclusion
This study demonstrated critical gaps in current drug interaction databases when managing ART with comorbidities such as TB, malaria, and pulmonary hypertension in PWH. Our findings indicate that DDIs occur across all classes of ART regimens. Non-nucleoside reverse transcriptase inhibitors (efavirenz, nevirapine) frequently interact with tuberculosis drugs (rifampicin, rifapentine, isoniazid) and antimalarials (artemether-lumefantrine), which may reduce efficacy and increase toxicity. Similar to evidence, protease inhibitors (atazanavir-ritonavir, darunavir-ritonavir) interact with rifampicin or artemether-lumefantrine. Integrase inhibitor (dolutegravir) had generally manageable interactions with high-dose rifampicin. In contrast, nucleoside/nucleotide reverse transcriptase inhibitors (tenofovir disoproxil fumarate, islatravir) exhibit minimal interactions and maintain effective HIV suppression. Discrepancies among DrugBank, Drugs.com, and the Liverpool HIV database may hinder optimal clinical decision-making, particularly in settings of polypharmacy. The influence of pharmacogenetic factors, including CYP2B6 and NAT2 polymorphisms, is important for personalized approaches to ART, especially in pregnant individuals. Ongoing updates to interaction databases and integration of pharmacogenomic data are essential to support safer, more effective, and individualized HIV care globally. Future studies should include larger, multicenter trials, broader populations, and expanded database evaluations to optimize real-world outcomes and improve evidence-based ART management.
Supplemental Material
Supplemental Material - Insights from systematic reviews (2019–2024) and drug interaction database analysis in people with HIV and comorbidities
Supplemental Material for Insights from systematic reviews (2019–2024) and drug interaction database analysis in people with HIV and comorbidities by Cherdsak Boonyong, Phattarapon Boonsing, Laphatsanan Ruangritpassorn, Phasapon Thayutichayaton, Phomin Rattanamungkun, Nattharika Chaiboonrueang, Pannapa Powthong in International Journal of STD & AIDS
Supplemental Material
Supplemental Material - Insights from systematic reviews (2019–2024) and drug interaction database analysis in people with HIV and comorbidities
Supplemental Material for Insights from systematic reviews (2019–2024) and drug interaction database analysis in people with HIV and comorbidities by Cherdsak Boonyong, Phattarapon Boonsing, Laphatsanan Ruangritpassorn, Phasapon Thayutichayaton, Phomin Rattanamungkun, Nattharika Chaiboonrueang, Pannapa Powthong in International Journal of STD & AIDS
Supplemental Material
Supplemental Material - Insights from systematic reviews (2019–2024) and drug interaction database analysis in people with HIV and comorbidities
Supplemental Material for Insights from systematic reviews (2019–2024) and drug interaction database analysis in people with HIV and comorbidities by Cherdsak Boonyong, Phattarapon Boonsing, Laphatsanan Ruangritpassorn, Phasapon Thayutichayaton, Phomin Rattanamungkun, Nattharika Chaiboonrueang, Pannapa Powthong in International Journal of STD & AIDS
Footnotes
Author contributions
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.