
Abstract
Background
Quantitative HIV-1 DNA (qDNA) is a biomarker of the viral reservoir. We evaluated whether two-drug regimens (2DRs) maintain qDNA values comparable to those of three-drug therapies (3DRs).
Materials and methods
We collected data from people living with HIV (PLWH) undergoing qDNA testing. Total HIV-1 DNA was measured using the HIV-1 DNA Test PRO (Diatheva) on InGenius (ELITech) platform. Descriptive analyses and non-parametric tests were performed. Bivariate logistic regression was applied to identify predictors of qDNA levels ≥2.3 log copies/106 in peripheral blood mononuclear cells (PBMC).
Results
263 PLWH receiving antiretroviral therapy (ART) were included; 118 (44.9%) had qDNA ≥2.3 log copies/106 PBMC. Age (OR: 1.44 per 10-years increase, p = 0.008) and prior CDC C stage events (OR: 2.26, p = 0.025) were associated with qDNA >2.3 log copies/106 PBMC. Years of treatment (OR: 0.71 per 5-years increase, p = 0.018) was associated to lower probability of qDNA >2.3 log copies/106 PBMC. No association was found between ART type (2DR vs 3DR) and qDNA levels (p = 0.441).
Conclusion
The impact of 2DRs on the viral reservoir assessed by mean of qDNA is not different from what observed with 3DRs and may be a viable option for PLWH at risk of disease progression.
Introduction
Early in the HIV lifecycle, reverse transcription converts viral RNA into complementary DNA (cDNA), which can integrate into the host genome or remain unintegrated. Unintegrated cDNA (uDNA), that includes 1-LTR, 2-LTR circles, as well as linear unintegrated DNA, represents the predominant form of HIV-1 cDNA in the nucleus. 1 uDNA can be transiently transcribed, contribute to latency, support limited virus production, and trigger immune responses. 2
Notably, uDNA persists even under suppressive antiretroviral therapy (ART), especially in effector memory CD4 + T cells, indicating ongoing residual viral activity and contributing to chronic immune activation. 3 These forms of uDNA are part of the viral reservoir, that is all the cells and tissues that harbor persistent HIV and play a role in pathogenesis and potential viral reactivation. 4
The persistence of the viral reservoir in people living with HIV (PLWH) on ART is the main reason why, the virus remerges if treatment is interrupted, leading to a rebound in viremia. This persistence makes HIV eradication impossible and necessitates lifelong treatment.
Among the markers used to measure the HIV reservoir, total HIV DNA is the most widely studied and utilized. 5 It quantifies all forms of HIV DNA, including integrated proviruses and unintegrated episomal DNA, providing a broad assessment of HIV persistence. 6
Assessing HIV-DNA has also clinical implications as it can predict disease progression independently of HIV RNA load and CD4 + T cell count in untreated individuals. 7 Higher levels of total HIV DNA correlate with higher plasma viremia and lower CD4 + counts. In addition, early level of HIV DNA during primary infection and increased T-cell activation predict the extent of T-cell proliferation. 8 Additionally, it has been linked to HIV-associated neurological disorders, with higher HIV DNA levels associated with greater disease severity. 9
Evidence suggests that starting ART earlier leads to a greater reduction in total HIV DNA, and that lower baseline HIV DNA levels are associated with a better virological response to ART and lower residual viremia. 10
Lower HIV DNA levels indicate a higher chance of maintaining viral control after stopping ART in both early and chronic infection. It also helps predict the risk of virological failure when simplifying ART or using two-drug regimens (2DR).11,12
Recent studies have evaluated the effects of dual therapies compared with triple regimens on both virological suppression and reservoir dynamics: for example, Saborido-Alconchel et al. aimed to clarify potential differences in viral reservoir, immune activation, and inflammation between dolutegravir/lamivudine and dolutegravir plus TAF/emtricitabine in treatment-naïve individuals 13 ; Bailón et al. measured the impact of a 2DR of dolutegravir plus lamivudine (DTG+ 3 TC) and a 3DR of dolutegravir plus emtricitabile/tenofocir alafenamide (DTG + FTC/TAF) on the HIV-1 reservoir and immune activation biomarkers 14 ; real-word evidence from Alzate-Angel et al. evaluated the clinical, virological, and immunological benefits of first-line integrase strand transfer inhibitor (INSTI)-based ART, including dual-therapy, compared to regimens based on nonnucleoside reverse transcriptase inhibitors (NNRTIs) or protease inhibitors (PIs) 15 ; furthermore Dragoni et al. aimed to evaluate the dynamics of the viral reservoir by quantifying both total HIV-1DNA (tTDNA) and the biological active fraction, intact HIV-1DNA (iDNA), over 48 weeks in virological suppressed individuals who either remained on 3DRs or switched to 2DRs. 16
Total HIV-1 DNA quantification detects all forms of HIV-1 DNA (integrated and unintegrated), as well as defective and replication-competent sequences, in both resting and activated infected cells. While this broad detection capability could be seen as a limitation, all these forms play a role in HIV pathogenesis, making total HIV-1 DNA a valuable biomarker of the viral reservoir and providing many insights into HIV pathogenesis.
Our aim was to evaluate whether 2DRs maintain HIV DNA levels comparable to standard three-drug therapy (3DR), ensuring reservoir suppression while offering a potential alternative treatment strategy.
Methods
Study population
This retrospective, monocentric, cross-sectional analysis, included PLWH tested for quantitative DNA (qDNA) between April and October 2023.
The collected data included demographics (age and sex), risk factors for HIV acquisition, length of infection, length of therapy, presence of resistance associated mutations (RAMs), HIV RNA, CD4 + cell count and CD4/CD8 ratio, previous CDC stage C status, antiretroviral regimen at the time of qDNA measurement and its duration, and viremia copy-years. Demographic and clinical data were retrieved from the hospital’s electronic records.
Previous studies have demonstrated that HIV DNA levels <2.3 log copies/106 PBMC are associated with successful therapeutic de-escalation strategies and are independent predictors of a lower risk of virological failure or viral blips. 17 Based on these findings, we adopted 2.3 log copies/106 PBMC as the cutoff to define low qDNA levels, indicative of better infection control.
Thus, the individuals were stratified according to their qDNA levels (<2.3 vs ≥2.3 log copies/106 PBMC).
qDNA analysis
Total HIV-1 DNA measurements were introduced in our clinic in December 2022. Genotypic resistance testing on DNA could be difficult to perform in cases of low viral load leading to a long turnaround time and delayed clinical decisions. Therefore, when clinicians decide to evaluate the presence of RAMs on DNA for any clinical reason (for instance, the need to switch to a 2DR with an incomplete virologic and therapeutic history, frequent blips, and persistent low-level viremia), we decided to screen the samples by measuring qDNA and undergo genotypic testing if the value was above 2.3 log copies/106 PBMC.
Total HIV-1 DNA was analyzed using the RUO HIV-1 DNA Test PRO (Diatheva S.r.l., Italy), optimized for the ELITe InGenius Platform (ELITechGroup, a Bruker Company, Italy), following the manufacturer’s instructions. DNA was extracted from 200 µL of whole blood (K2-EDTA), followed by fully automated amplification on the same platform. The InGenius system provided enhanced stability for positive and negative controls and calibrators, which were performed every 15 days and every 2 months, respectively, or when reagents were changed. This improved stability ensured greater result comparability compared to that of manual assays. All assays were performed by trained laboratory technicians blinded to the clinical information of the selected individuals and to the assay results.
Statistical analyses
Descriptive analyses were performed to characterize the subjects included in the study. Median values and interquartile ranges (IQR) were used to describe continuous variables, whereas counts and percentages were used for qualitative variables. The association between variables was assessed using Pearson’s chi-square and Mann-Whitney U tests, as appropriate. Unadjusted bivariate regression was used to analyze the strength of the association between having a qDNA above 2.3 log copies/106 PBMC and other variables, calculating the odds ratios (OR) and their 95% confidence intervals (CI). Multivariable binary logistic regression was fitted to variables selecting relevant risk factors based on clinical knowledge.
Two-tailed p-values were calculated and a value of <0.05 was considered statistically significant. Data management and analysis were performed using the STATA package, version 16.1 (College Station, TX, StataCorp 2019).
This study was conducted in accordance with the principles of the Declaration of Helsinki. All individuals participating in this study signed an informed consent form regarding the medical procedure and the use of their data for medical research.
Results
Demographic and clinical features of the study population.
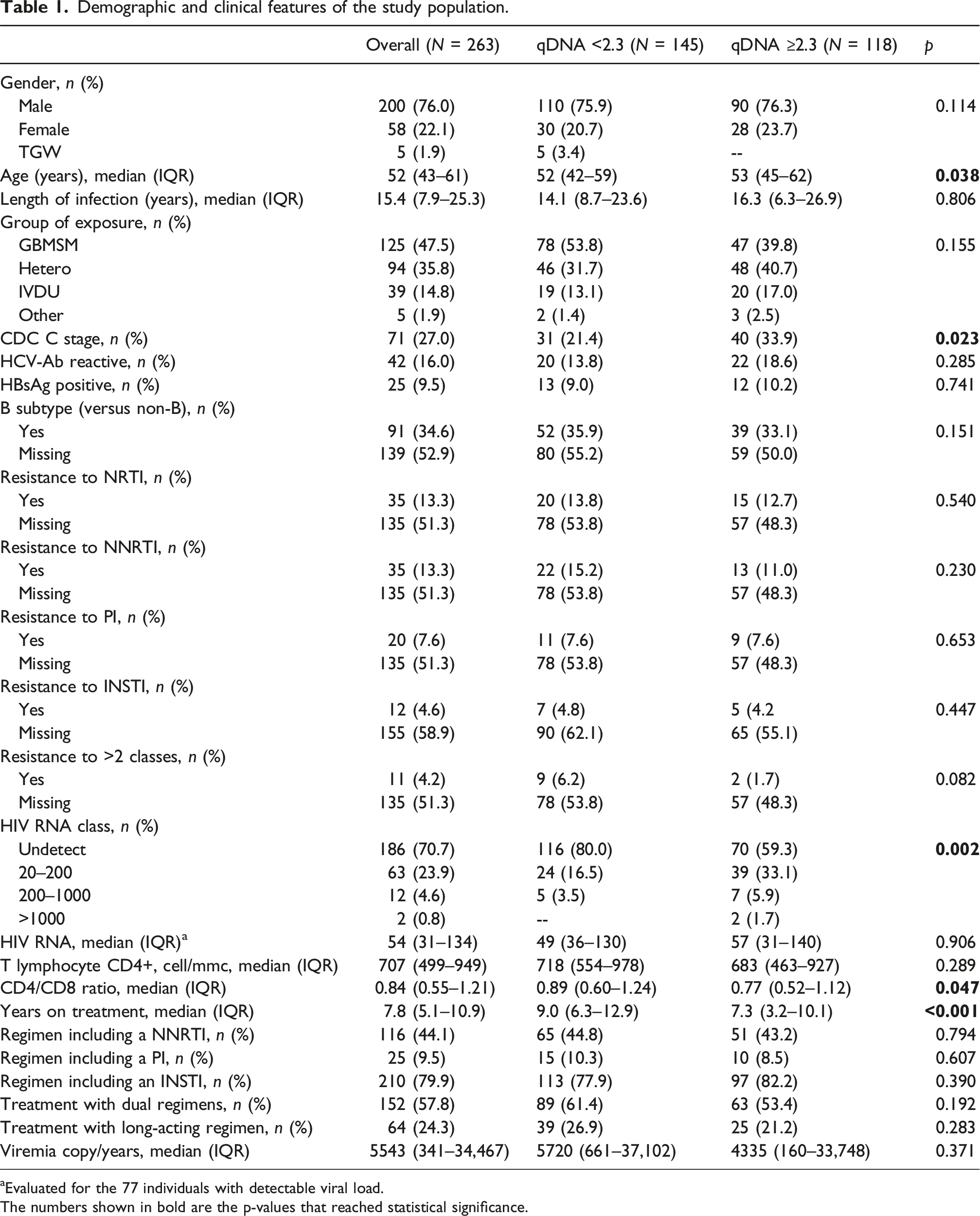
aEvaluated for the 77 individuals with detectable viral load.
The numbers shown in bold are the p-values that reached statistical significance.
After adjusting for the bivariate regression model, older age (per 10 increase) and CDC C events were associated with higher odds of having a qDNA above 2.3 log copies/106 PBMC, with an OR of 1.44 (95% CI: 1.10–1.9, p = 0.008) and of 2.26 (95% CI: 1.11–4.61, p = 0.025), respectively. Additionally, years of treatment (per 5 increase) was associated with a lower probability of having a qDNA >2.3 log copies/106 PBMC (OR: 0.71, 95% CI: 0.54–0.94, p = 0.018).
Adjusted bivariate regression model for factors associated with qDNA >2.3 log copies/106 PBMC.

aAdjusted for all the variables listed.
bAny combination including more than one anchor drug (i.e., INSTI plus NNRTI, INSTI plus PI, NNRTI plus PS).
The numbers shown in bold are the p-values that reached statistical significance.
Discussion
Total HIV DNA is a crucial marker of viral persistence that is linked to disease progression and immune activation. 18 However, the impact of 2DR on HIV DNA is unclear.
To address this knowledge gap, we analyzed 263 PLWH, of whom 55.1% had qDNA <2.3 log copies/106 PBMC. Those with lower qDNA were younger, had fewer CDC stage C diagnoses, more often had undetectable HIV RNA, higher CD4/CD8 ratios, and longer ART duration. Although individuals receiving 2DRs had lower qDNA value, this is the result of a channeling bias since the adjusted bivariate regression analysis found that, as expected, age and CDC C stage were associated with a higher probability of qDNA >2.3 log copies/106 PBMC. Conversely, years of treatment were associated with a lower probability of qDNA >2.3 log copies/106 PBMC (OR: 0.71, 95% CI: 0.54–0.94, p = 0.018).
Our data confirm that sustained viral suppression reduces HIV viral burden over time, as demonstrated also by Hocqueloux L et al. 19
When comparing our findings to recent literature, the results align with other studies showing that simplification to dual therapy does not lead to an expansion of the viral reservoir. In particular, the decay of the HIV-1 reservoir, the immune recovery asses by the CD4/CD8 ratio and the inflammation were demonstrated to be independent of whether antiretroviral therapy was initiated with the three-drug regimen DTG + TAF/F or the two-drug regimen DTG/3 TC. 13 Similarly, a comparable reductions in reservoirs size, markers of inflammation, and T-cell exhaustion was seen in patients receiving DTG/3 TC compared to 3DR. 14 Alzate-Angel et al. also confirmed that INSTI-based regimens, including dual combinations, maintain both virological suppression and reservoir stability. 15 Furthermore, it was demonstrated that total HIV-1DNA tDNA and iDNA did not show a statistically significant change in the the 2DRs (dolutegravir- or atazanavir-based dual therapy) compared with the 3DRs group. 16
Notably, in our study the type of ART regimen (2DR vs 3DR) did not significantly affect HIV-1 DNA levels. This observation, together with the above evidence, supports the growing body of evidence that two-drug regimens (2DRs) are virologically non-inferior to three-drug regimens (3DRs) in both naïve and treatment-experienced individuals. Several clinical trials, including GEMINI, TANGO, and SWORD, have consistently shown comparable rates of virological suppression between 2DR and 3DR, leading to the inclusion of 2DRs as valid options in various clinical scenarios. 20
The current study had several limitations that should be acknowledged. First, the retrospective and cross-sectional nature of the study and the monocentric analysis design could have generated selection bias that might misrepresent the outcomes.
Second, viremia copy/years could not be calculated for a large proportion of individuals who moved to our clinical site at any time after the diagnosis; thus, full virologic data were missing and could not be used to determine this parameter. Moreover, qDNA measurement has flaws. It captures both integrated and unintegrated HIV DNA and could not distinguish between replication-competent and defective viral sequences. Additionally, the standardization of qDNA assays remains a challenge, with variability between manual and automated methods. Our use of the HIV-1 DNA Test PRO on the fully automated InGenius platform represents an advancement in improving reproducibility and reducing assay-related variability. Molecular assays for total HIV-1 DNA are simpler, faster, and more cost-effective than quantitative viral outgrowth assay (QVOA). 21 Although various in-house and a few commercial manual assays exist for HIV-1 DNA quantification, the differences between methods make direct comparisons challenging. 22
All the qDNA analyses were conducted using a fully automated and commercially available assay on the ELITe InGenius ® platform. Unlike previous studies, this approach minimized variability in DNA measurement and enhanced result reproducibility. 23
Conclusion
Our study demonstrates that 2DRs do not result in significantly different qDNA levels than 3DRs, supporting their role as a viable and effective option for long-term HIV management. These findings provide further reassurance that modern 2DRs do not negatively affect the HIV reservoir.
Furthermore, qDNA is an important marker for evaluating disease progression, treatment efficacy, and potential ART simplification strategies. While it offers valuable insights into viral persistence, it could be to guide clinical decision-making. 24
Finally, total HIV DNA quantification has the potential to play a key role in evaluating innovative therapeutic strategies, including intensification/simplification approaches, immune-based therapies, latency-reversing agents, and potential curative interventions, such as stem cell transplantation. 5 Future research should continue to explore the role of qDNA in assessing novel ART strategies and optimizing the care of PLWH.
Footnotes
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Comitato Etico Territoriale Lombardia 3 (no. 5370_16.10.2024_N bis) on November 20, 2024, with the need for written informed consent waived.
Consent to participate
All subjects starting PrEP at Milano Checkpoint provided written informed consent allowing the analysis of their anonymized aggregated data for scientific purposes.
Consent for publication
All participants provided written informed consent for participation and publication of anonymized data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.