
Abstract
Intravesical Bacillus Calmette–Guérin (BCG) therapy is a mainstay for non-muscle invasive bladder cancer, but may rarely cause disseminated infection. We describe a 71-year-old man who developed fever, respiratory failure, and hepatomegaly 1 week after completing maintenance intravesical BCG instillations. Examination revealed multiple erythematous-violaceous papules on the glans penis. Biopsies of both skin and liver showed granulomatous inflammation with focal necrosis; Ziehl-Neelsen, PAS, and Grocott stains, culture, and PCR for Mycobacterium tuberculosis complex were negative. These findings supported a diagnosis of disseminated BCGitis with cutaneous penile involvement. Anti-tuberculous therapy with rifampicin, isoniazid, and ethambutol led to full systemic and cutaneous improvement. Penile involvement in BCGitis is exceedingly uncommon, and microbiologic confirmation is often lacking due to low sensitivity. Awareness of this entity is essential, as early recognition and prompt therapy can prevent severe systemic complications and improve outcomes in patients recently exposed to intravesical BCG.
Intravesical Bacillus Calmette–Guérin (BCG) therapy is a cornerstone in the management of non-muscle invasive bladder cancer (NMIBC). While generally well-tolerated, rare systemic complications, such as disseminated BCGitis, can be life-threatening. Cutaneous manifestations, particularly involving the genitalia, are uncommon and may serve as critical diagnostic clues in complex systemic presentations.
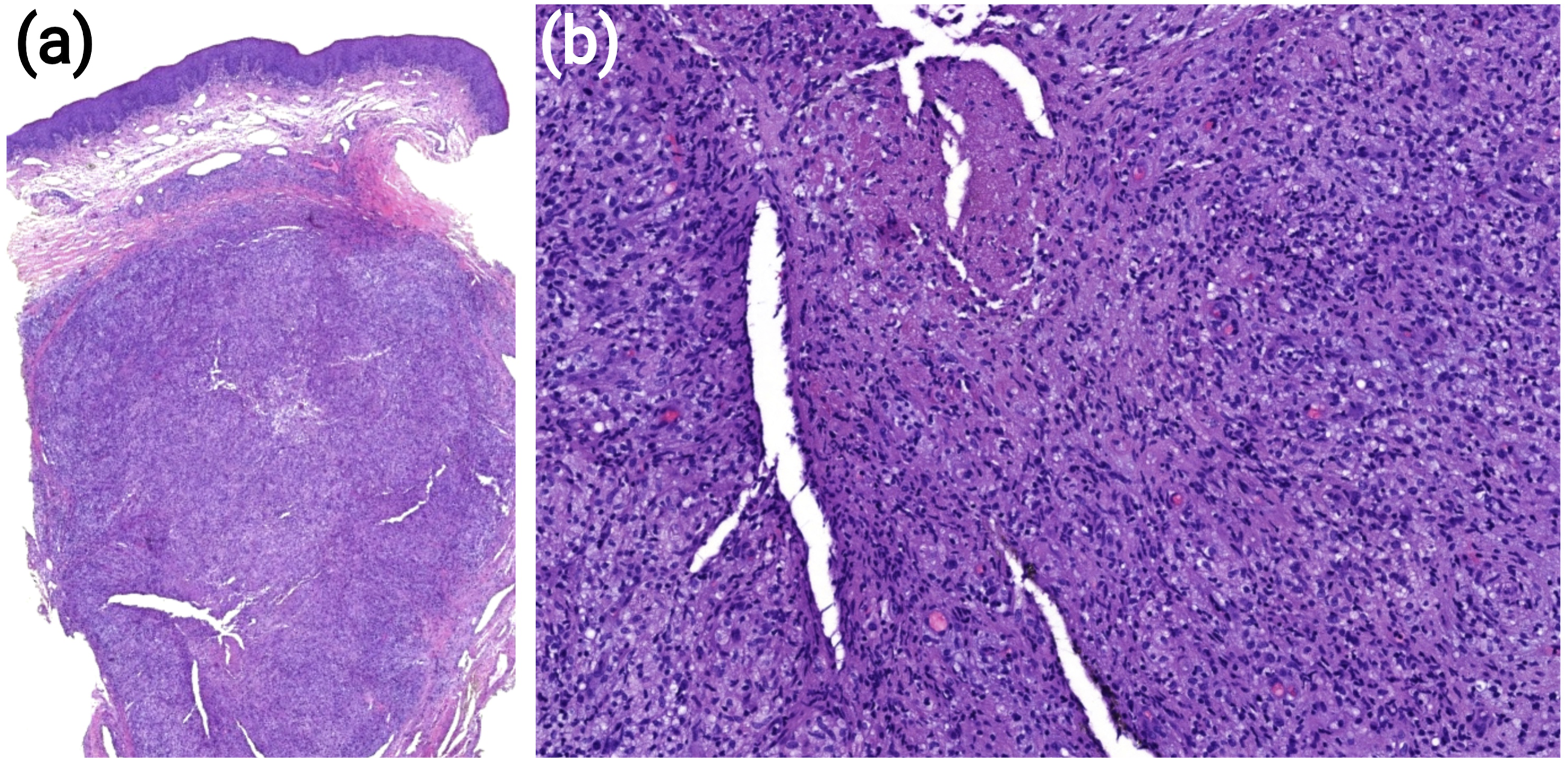
We report the case of a 71-year-old male with a history of high-grade papillary urothelial carcinoma (pT1HG), managed with transurethral resection followed by induction and maintenance intravesical BCG instillations. One week after his final BCG instillation, the patient presented with fever and disorientation. Due to clinical deterioration, including respiratory insufficiency, he was admitted to the intensive care unit (ICU). Imaging revealed bilateral pneumonia with diffuse pulmonary micronodules and hepatomegaly. During hospitalization, multiple erythematous-to-violaceous infiltrated papules on the glans penis were also observed (Figure 1). Based on clinical and analytical findings, a provisional diagnosis of disseminated BCGitis was made. Histopathological examination of a penile skin biopsy revealed granulomatous inflammation with focal necrosis in the reticular dermis (Figure 2). A liver biopsy performed to evaluate hepatic dysfunction revealed similar granulomatous changes. Ziehl-Neelsen staining was negative for acid-fast bacilli in both specimens, and no microorganisms were identified on PAS and Grocott stains. Cultures and PCR for Mycobacterium tuberculosis complex were also negative. The penile lesions were interpreted as a cutaneous manifestation of systemic BCGitis. Causes of immunossupression, including HIV infection, were excluded. Triple anti-tuberculous therapy with rifampicin, isoniazid, and ethambutol was initiated, leading to gradual clinical improvement of systemic symptoms and regression of the penile papules over several weeks. Clinical image showing multiple erythematous-to-violaceous infiltrated papules on the glans penis. Histopathological image of glans biopsy revealing an epidermis without significant alterations, in the presence of granulomatous inflammation with focal necrosis in the reticular dermis - hematoxylin and eosin stain, 12.5× on panel (a) and 79× on panel (b).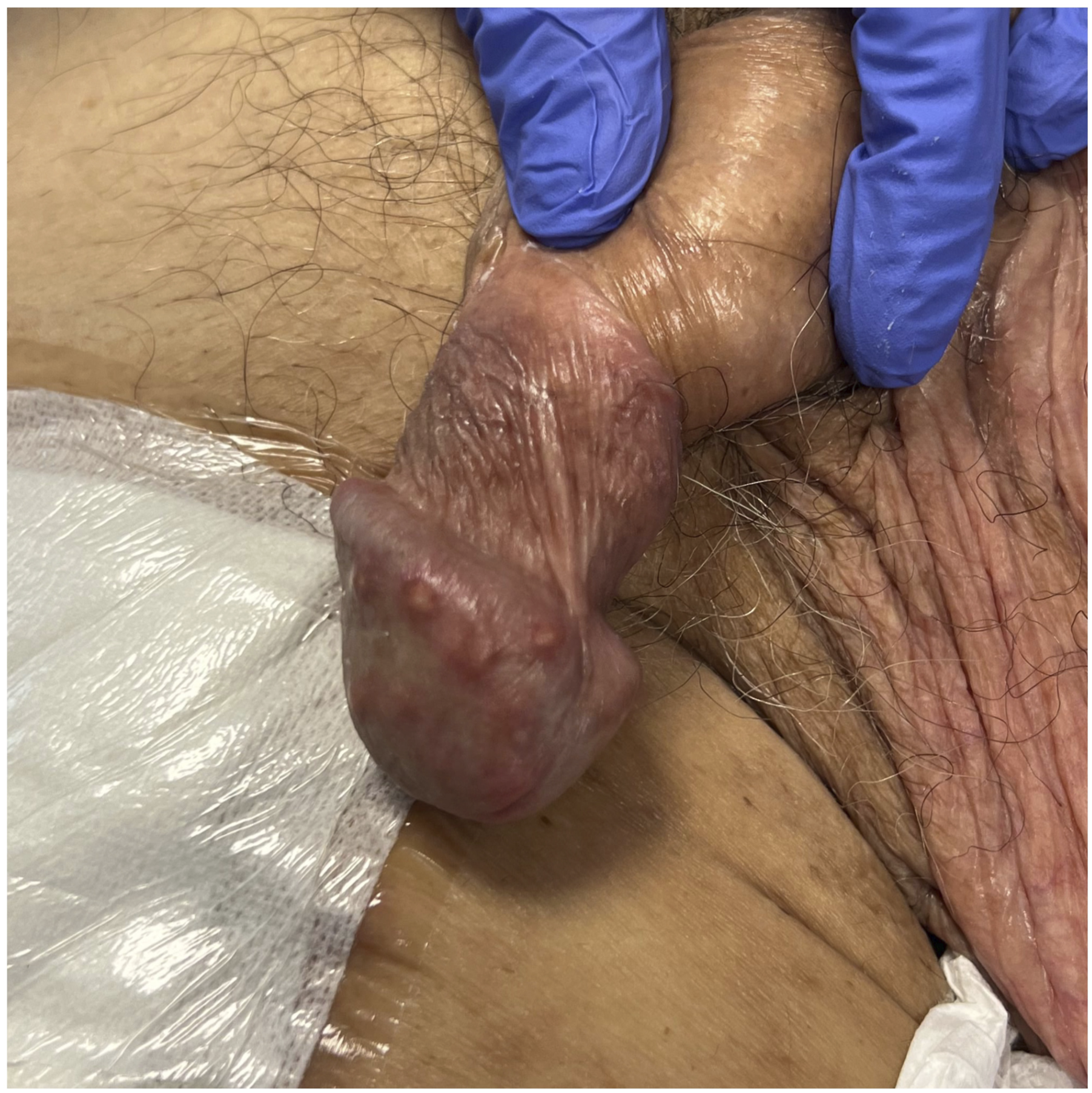
BCG infection is an uncommon complication of intravesical BCG immunotherapy. A recent meta-analysis showed a pooled incidence of BCG infection after intravesical immunotherapy of 2% (95% CI 1–2%), with over half of cases presenting a disseminated pattern, and localized genitourinary involvment being less common. 1
Penile involvement in disseminated BCGitis is exceedingly rare. A review of the literature reveals limited reports detailing such presentations, with variable clinical presentations, including erosions, pustules, ulcers, edema and firm papules, with some cases showcasing associated systemic symptoms, as in our patient.2–9 In general, the diagnostic workup always included skin biopsies which revealed granulomatous inflammation. Ziehl-Neelsen staining, culture and PCR were also commonly performed and may aid in the diagnosis. However, Ziehl-Neelsen staining was positive in only one of nine reviewed cases 2 and only one case reported a positive culture from a penile lesion biopsy. 3 PCR testing was inconsistently performed and positive in only one case. 4 The negative microbiological findings in most cases underscore the diagnostic challenges, as cultures and PCR assays often yield low sensitivity in detecting M. bovis. Favorable response to treatment remains another valuable clue for the diagnosis.
The pathogenesis of cutaneous manifestations in disseminated BCGitis remains unclear. It is hypothesized that hematogenous or lymphatic dissemination of M. bovis may lead to granulomatous lesions in the skin, with traumatic inoculation possibly playing a role in penile lesions. 5 It seems that both direct infectious processes and hypersensitivity reactions may play a role in the clinical manifestations of BCGitis, 6 as supported by the frequent negativity of microbiologic tests.
This case underscores the importance of considering BCGitis in the differential diagnosis of penile lesions, especially in patients with recent intravesical BCG exposure. Dermatologists and Sexual Health physicians play a pivotal role in recognizing such atypical presentations, facilitating timely diagnosis and management. Additionally, other frontline clinicians may also encounter these lesions and contribute to their early identification. This case underscores the need for a comprehensive physical examination that includes the genitoanal region, which is frequently neglected both by clinicians and by patients, who may refrain from reporting changes due to embarrassment or unawareness of small, asymptomatic lesions. Furthermore, it reinforces that, in the post–intravesical BCG setting, granulomatous cutaneous changes — particularly in the genital area — should be regarded as a potential sign of BCGitis. Early initiation of anti-tuberculous therapy is crucial in mitigating systemic complications and improving patient outcomes and should not be delayed based on the absence of microbiologic confirmation, specially in the presence of systemic symptons.
Footnotes
Ethical considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.