
Abstract
Background
Transgender women (TGW) face a disproportionately high HIV burden, yet real-world evidence on their engagement in the care cascade is scarce. This study analysed HIV care cascade outcomes and associated factors in a large Argentinian cohort to identify key challenges and inform public health strategies.
Methods
This was a retrospective cohort study of TGW with confirmed HIV linked to care at a public hospital in Buenos Aires (2011–2022). We analyzed 12-month retention in care, antiretroviral therapy (ART) use, and virologic suppression using bivariate and multivariate logistic regression.
Results
Of 240 TGW included, 186 completed 12-months follow-up. The cascade outcomes were: 71.5% retained in care; 87.9% on ART among those retained; and 70.7% virologically suppressed among those on ART. In multivariate analysis, ART initiation at linkage was the strongest predictor of retention (aOR: 35.93; 95%CI: 9.72–132.75), while baseline cocaine use was associated with a lower likelihood of being on ART (aOR: 0.17; 95%CI: 0.04–0.68).
Conclusions
Significant gaps persist in the HIV care cascade for TGW in this real-world setting. While immediate ART initiation is a powerful tool for retention, structural barriers like substance use require integrated interventions. This evidence is critical for designing effective public health strategies to improve health equity.
Introduction
Transgender women (TGW) are considered a key population, defined as groups that, due to their practices and structural conditions, face greater exposure to the human immunodeficiency virus (HIV) and other sexually transmitted infections (STIs). 1 A meta-analysis compiling data from 15 countries between 2000 and 2011 estimated a global HIV prevalence of 19.1% in TGW. 2 Additionally, TGW were found to have an odds ratio (OR) of 48.8 for HIV infection compared to the general population. This disproportionate burden is also evident in countries with concentrated HIV epidemics, such as Argentina, where the estimated prevalence of HIV among TGW is 34%, 3 far exceeding not only the prevalences estimated for the general population (0.4%) but also those of other key populations, such as men who have sex with men and sex workers. 3
In many settings worldwide, TGW face stigma, discrimination, and social exclusion, which limits their access to healthcare services.4,5 This marginalization and transphobia are associated with increased prevalence of depression and other serious mental disorders, substance use, and STIs, 6 including HIV. 7 As a result, TGW experience unique vulnerabilities to HIV, facing systematic barriers that impact all stages of the continuum of prevention, diagnosis, and treatment. 7 These barriers include denial of care, harassment, violence, and a lack of adequately trained healthcare providers.8,9 Even after being diagnosed with HIV, many TGW avoid medical care due to fear or prior experiences of discrimination in healthcare settings.10,11
The HIV care cascade is a framework designed to identify programmatic gaps in health services1,12 and to monitor challenges that arise at different stages of HIV care, including prevention, diagnosis, treatment, and viral suppression. Most longitudinal analyses of the care cascade focus on linkage to care, sustained antiretroviral therapy (ART), and virological suppression, both in individuals with newly diagnosed and previously diagnosed HIV.1,12
Despite its programmatic and public health relevance, there is limited published data on the HIV care cascade for TGW in the region. A previous study from our center in Argentina focused on the general adult population living with HIV, 13 but it used a binary sex registry (male or female), and no specific sub-analysis was conducted for TGW.
Given the scarcity of real-world cascade data for TGW, this study aimed to analyze the outcomes from a large cohort in a publicly funded clinic in Buenos Aires, Argentina. The goal is to provide a detailed case study that can inform public health policies and programs in similar urban settings across the global context.
Materials and methods
This retrospective cohort study describes the HIV care cascade outcomes among TGW living with HIV linked to care between February 2011 and November 2022 and identifies factors potentially associated with these outcomes. The outcomes evaluated as dependent variables were retention in care, ART use, and virological suppression at 12 months.
The research was carried out at the Infectious Diseases Division of the Hospital General de Agudos Dr. Juan A. Fernández, a tertiary-level public hospital in Buenos Aires, Argentina, which accounts for 14.5% of all new HIV diagnoses within the city’s public health system annually. 14
Given the descriptive and exploratory nature of the study, no formal sample size calculation was performed and all individuals meeting the selection criteria were included. To establish the cohort a retrospective database search was first conducted. The search strategy identified medical records based on discordance between sex at birth and self-perceived gender, or the presence of the keywords “trans” or “transgender” in the electronic health record (EHR). We included all individuals aged ≥16 years who self-identified as TGW, had a confirmed HIV diagnosis, and were linked to care during the study period. Linkage to care was defined as at least one clinical visit at the center after an HIV diagnosis during the study period. HIV diagnosis was confirmed as per local laboratory algorithms (i.e., a positive screening test followed by a positive confirmatory test), documented through an ART prescription (excluding pre- and post-exposure prophylaxis), or a confirmed diagnosis registered in national surveillance systems. Participants who were regularly monitored at another center and consulted only for non-HIV-related conditions were excluded. Data were collected through a retrospective review of medical records, laboratory reports, pharmacy records, and National Health Surveillance System (NHSS), gathering information at the time of linkage and during the first 12 months of follow-up, and therefore anonymized for analyses.
This study was conducted in accordance with the protocol and Good Clinical Practice guidelines, following applicable local and international regulations, including the Nuremberg Code, Declaration of Helsinki and its amendments, and UNESCO Universal Declaration on the Human Genome and Human Rights (1997). The protocol was approved (number of registry: 7309) by the local Research Ethics Committee (REC), which granted an informed consent waiver in line with Guideline 10 of the CIOMS International Ethical Guidelines.
Dependent variables (outcomes)
The dichotomous dependent variables were evaluated sequentially: retention in care, ART use, and virological suppression at 12 months as per the Framework for Monitoring HIV/STI Services for Key Populations from PAHO. 1
Retention in care was defined as having at least two follow-up visits (clinical visit, laboratory tests, prescription, or medication pickup) after linkage to our center, with one visit occurring at 12 months (±3 months).
To verify vital status and identify care at other centers among those lost to follow-up, records were cross-referenced with the NHSS. This verification was performed at least 1 year post-follow-up to account for administrative reporting lags.
ART use at 12 months was defined as medication dispensing at any point during the 3 months prior to the end of the first year of follow-up. Eligibility for ART initiation was defined according to the clinical recommendations available at the time of linkage. Between 2011 and 2013, ART was recommended for patients with CD4 <350 cells/mm3 or an opportunistic infection. 15 From 2013 to 2015, the threshold increased to CD4 <500 cells/mm3 or an opportunistic infection. 16 Since 2015, universal ART has been recommended, regardless of immune status. 17
Virological suppression at 12 months was defined as a plasma HIV viral load (VL) < 200 copies/ml at 12 months (±3 months) from ART initiation or reinitiation in treatment-naïve participants or previously treated patients, respectively. For those already on ART at the time of linkage to care, virological suppression was defined as VL <200 copies/ml at 12 months (±3 months) from linkage. To account for variations in VL testing availability over time, participants with a VL <200 copies/ml at any point within the 12-month period and documented continuous monthly ART dispensing were also considered virologically suppressed. Additionally, participants who maintained an undetectable VL throughout the 12-months follow-up period, provided that they had regular ART dispensing since treatment initiation, were also classified as virologically suppressed. Participants with no VL records during the defined period, regardless of documented regular medication dispensing, were not considered to be virologically suppressed in the analysis.
Independent variables
The covariates evaluated included age (in years) at the time of linkage to care; CD4 count at linkage to care; viral load at linkage to care; time between presumptive diagnosis (positive screening HIV test) and linkage to care (in days); country of birth; completion of secondary education (equivalent to 12 years); engagement in sex work at the time of linkage to care; reported use of cocaine, alcohol, marijuana, and/or tobacco; prior diagnosis at another center; presence of advanced HIV disease (AHD) at linkage to care (CD4 <200 cells/mm3 and/or a clinical stage 3 or 4 according to the WHO clinical staging of HIV disease) 18 ; prior ART history; reported ART use at linkage to care; and initiation/restart or continuation of ART after linkage to care.
Statistical analysis
Descriptive statistics were used to summarize the sociodemographic and clinical characteristics of the study population. Categorical variables were analyzed using the chi-square or Fisher’s exact test, as appropriate, whereas continuous variables were analyzed using the Mann-Whitney test.
Bivariate and multivariate logistic regression models were used to assess the potential association between study outcomes and covariates. The multivariate model was adjusted for the presence of AHD, age, alcohol use, cocaine use, and ART initiation or continuation after being linked to care. An automatic variable selection procedure was not performed.
Multicollinearity was assessed via Variance Inflation Factor (VIF). Bivariate analyses used pairwise deletion; multivariate models used complete cases. Behavioral variables were defined by affirmative documentation, with absence of record categorized as ‘No’. A Bonferroni correction was applied to bivariate analyses (adjusted p < 0.0033 for retention; p < 0.0036 for ART/suppression). Otherwise, significance was p < 0.05. All analyses were performed using R software version 4.4.1.
Results
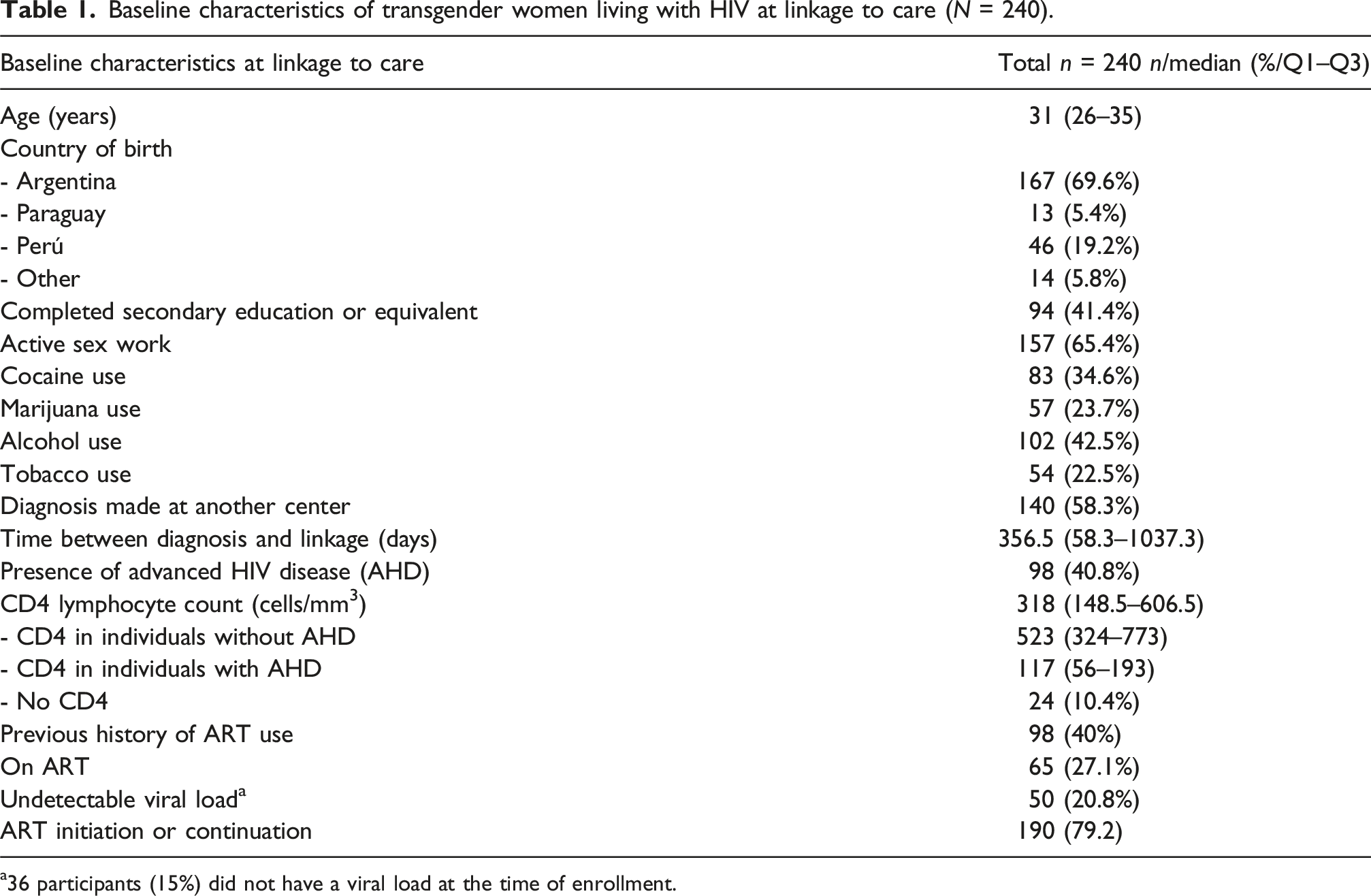
The initial database search identified 438 medical records. After manual review, 198 were excluded. Primary reasons were linkage outside the study period, lack of formal linkage, or receiving care exclusively for non-HIV-related conditions (monitoring elsewhere). Less frequent reasons included administrative-only records, HIV-negative status, unconfirmed HIV diagnosis, duplicate entries, or gender identity mismatch (e.g., cis or transgender men). Consequently, 240 records were included in the final analysis (Figure 1). Baseline characteristics are shown in Table 1. Flow diagram of participant selection and 12-months follow-up outcomes. Baseline characteristics of transgender women living with HIV at linkage to care (N = 240). a36 participants (15%) did not have a viral load at the time of enrollment.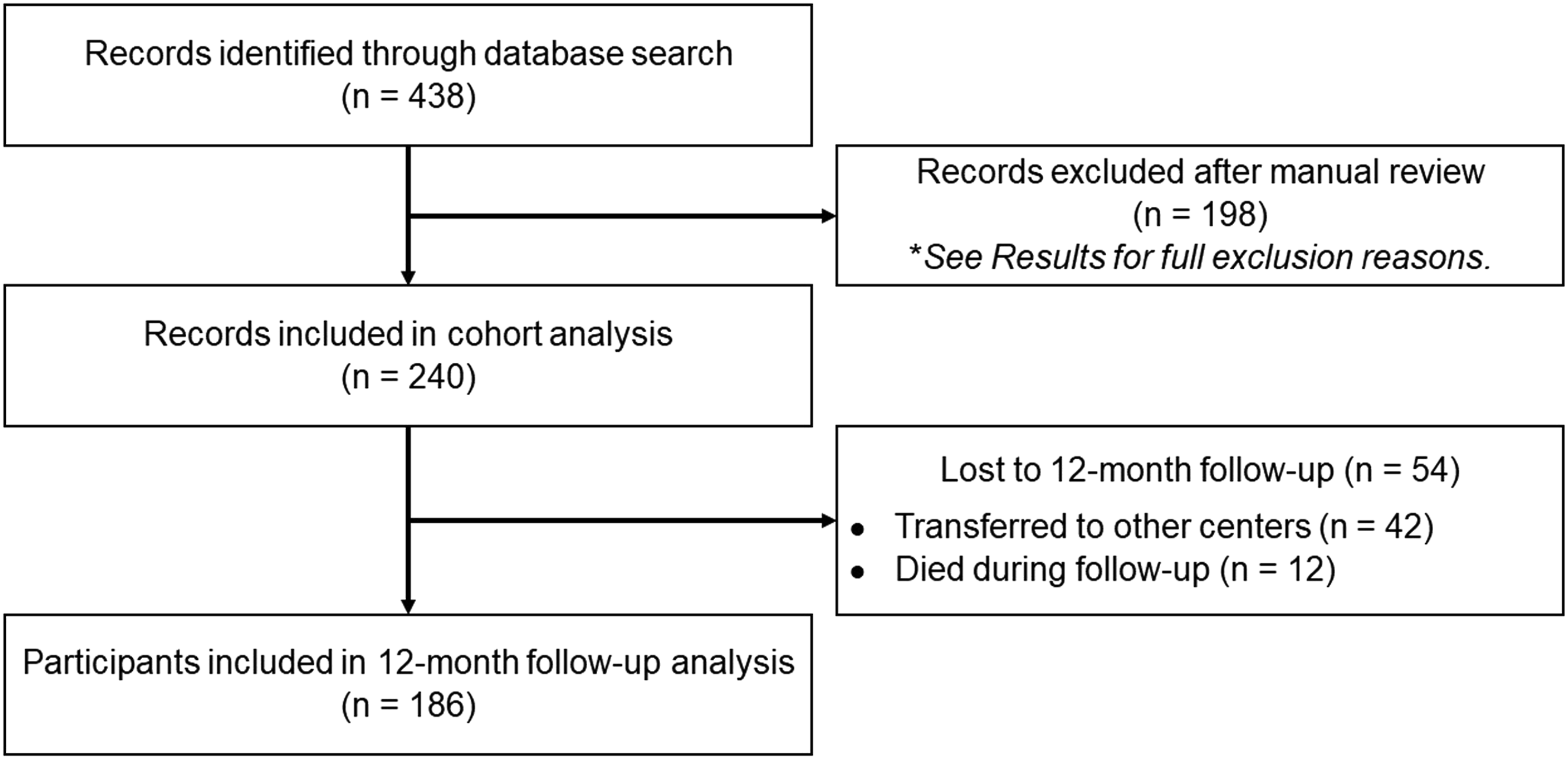
After 12 months of follow-up, 42 participants (17.5%) were transferred to other centers and 12 (5%) died; all deaths occurred in women presenting with AHD at the time of linkage to care. Of the remaining 186 participants, 133 (71.5%) were retained in care at 12 months. Of these, 132 were eligible for ART, and 116 of them (87.9%) were on ART at the end of the follow-up period. Of those receiving ART, 82 (70.7%) had undetectable viral loads (Figure 2). Consequently, the global rate of viral suppression among the participants who completed the follow-up (n = 186) was 44.1%. In a sensitivity analysis using only the strict definition of suppression (VL <200 copies/ml at 12 ± 3 months), the suppression rate among those on ART was 62.9% (73/116). Care cascade of study participants at 12 months of follow-up. It shows the proportion of participants linked to care, retained in care, on antiretroviral therapy (ART), and undetectable viral load. Salmon-colored bars represent participants meeting each stage criterion; orange sections indicate those not meeting the criterion. The brown area in the ‘Retained’ column represents participants who were transferred or died during follow-up.
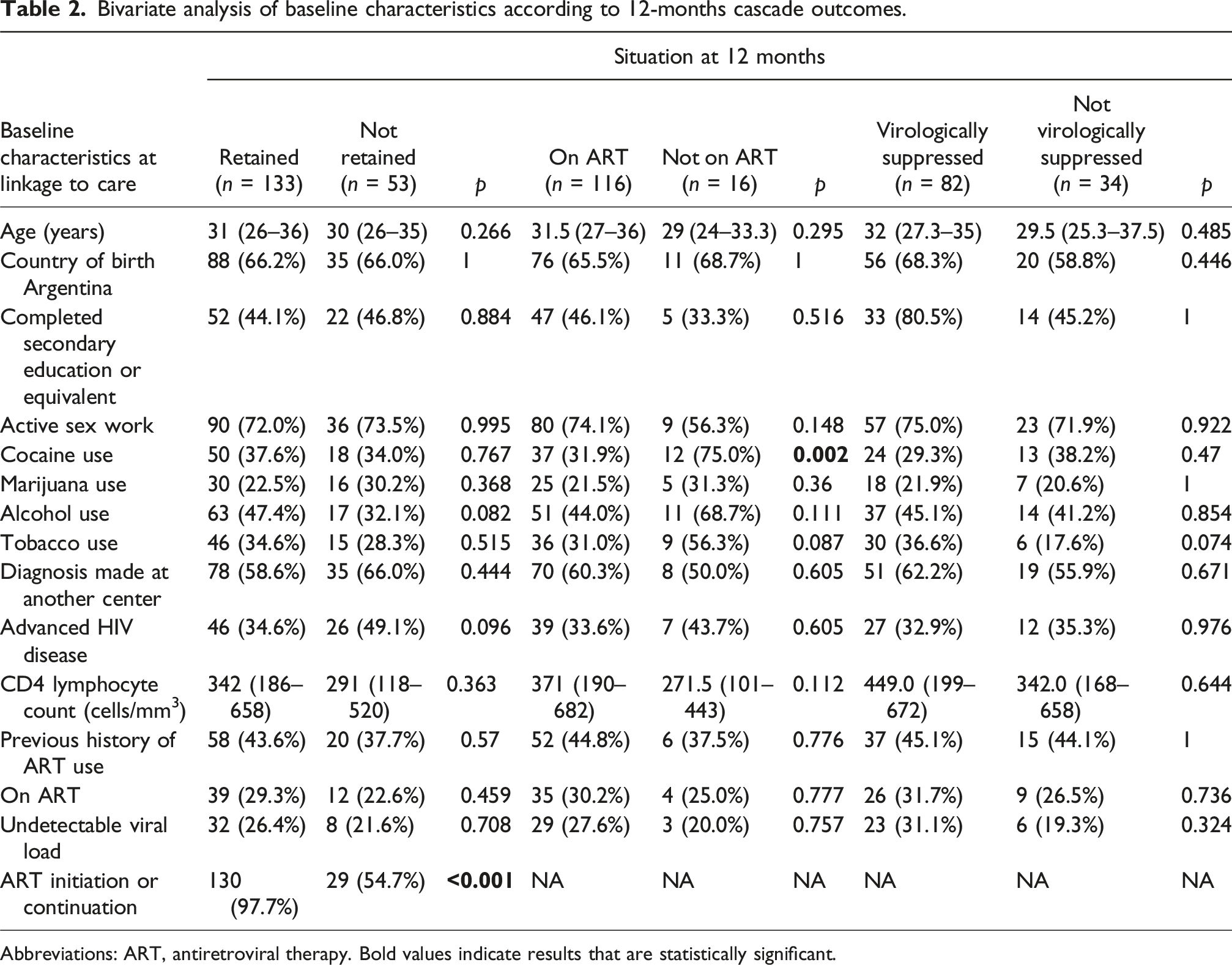
Bivariate analysis of baseline characteristics according to 12-months cascade outcomes.
Abbreviations: ART, antiretroviral therapy. Bold values indicate results that are statistically significant.
Table 2 compares baseline characteristics according to each cascade outcome. Regarding retention in care, participants who initiated or continued ART after linkage were significantly more likely to be retained compared to those who did not (97.0% vs 71.7%, p < 0.001). A difference that remained statistically significant after Bonferroni correction. No other significant differences were observed between retained and non-retained participants.
Regarding ART use, baseline cocaine use was significantly more common among participants not on ART at 12 months compared to those who were on ART (75.0% vs 31.9%, respectively; p = 0.002); this association also remained significant after adjusting for multiple comparisons. No significant differences were observed between those with and without virological suppression in any of the analyzed characteristics.
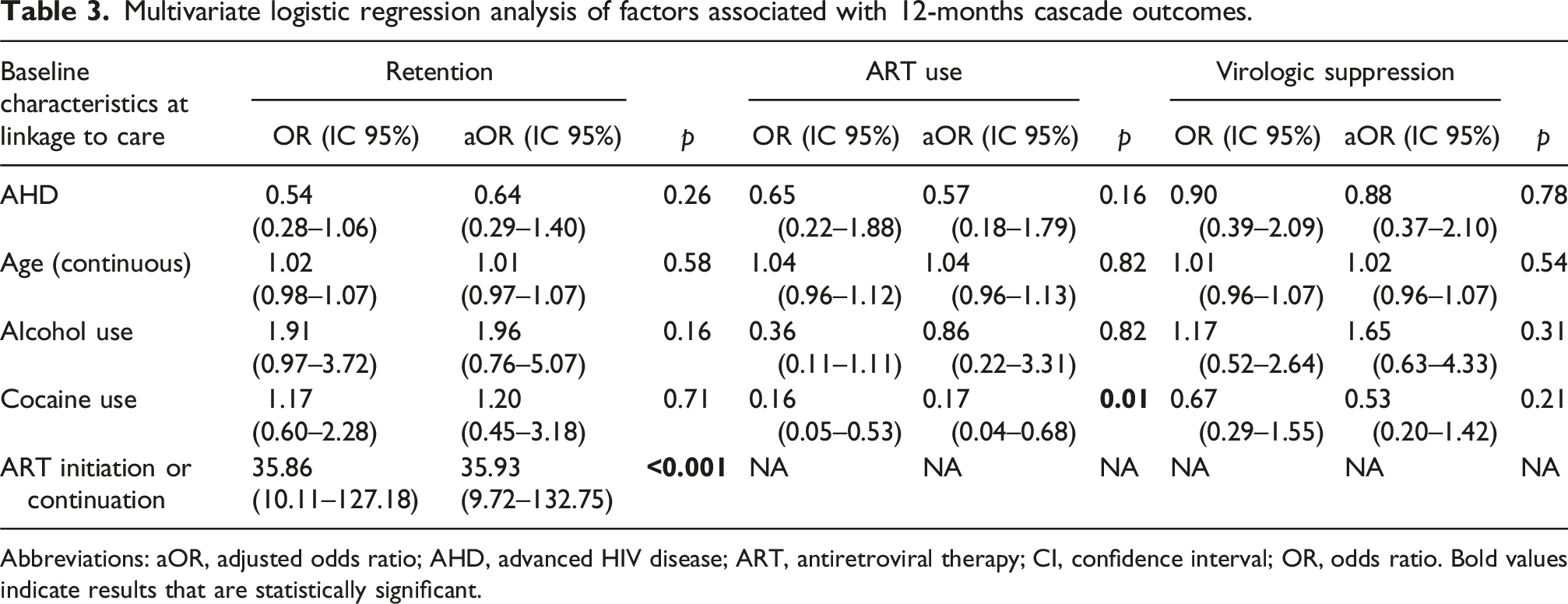
Multivariate logistic regression analysis of factors associated with 12-months cascade outcomes.
Abbreviations: aOR, adjusted odds ratio; AHD, advanced HIV disease; ART, antiretroviral therapy; CI, confidence interval; OR, odds ratio. Bold values indicate results that are statistically significant.
No significant associations were found for other variables, such as AHD, age, or alcohol use, with retention or virological suppression outcomes. The variable “ART initiation or continuation” was not included in the multivariate models for ART use or virological suppression because it is a prerequisite for these outcomes (i.e., a participant must be on ART to be assessed for virological suppression).
Discussion
This is the first study in Argentina to analyze the HIV care cascade for transgender women (TGW) living with HIV in a real-world setting. While conducted in a single urban center, the structural barriers identified—such as substance use and high mobility—and the programmatic successes, like the impact of immediate ART, reflect the challenges and opportunities faced by public health systems throughout low- and middle-income countries. These results not only quantify the gaps in the care cascade for this key population but also identify actionable targets—such as integrated substance use services and immediate ART policies—for public health programs across the world.
The 12-months retention rate in our cohort (71.5%) was lower than the 82% reported in a study conducted in Argentina with the same population. 19 This difference may be attributed to the different methodologies employed. While the previous study, conducted by a non-governmental organization providing free HIV care in Buenos Aires, offered serial monitoring and interventions specifically designed to improve adherence and retention—with a smaller sample size (n = 61)—our study was conducted in a real-world clinical practice setting with a larger sample (n = 186) and may therefore offer a more realistic picture of the challenges in routine public healthcare.
A previous study conducted at our center on the general population of treatment-naïve PLHIV linked to care between January 2011 and December 2013 reported a 1-year retention rate of 65.5%, 13 lower than the 71.5% observed in this study for TGW. These results should be interpreted within the context of temporal changes and evolving clinical guidelines for ART initiation. The increasing availability of simpler and more effective treatment regimens may have positively influenced retention. 20
Additionally, legislative and structural advancements in Argentina, such as the enactment of the Gender Identity Law in 2012, 21 likely contributed to improved access to healthcare for this population. Previous research 22 reported that the law reduced barriers and increased healthcare utilization. By mandating free gender-affirming hormone therapy—known to improve HIV retention 23 — this framework likely served as a key structural facilitator for our observed outcomes.
Compared to studies conducted in the United States 24 and Canada, 25 where retention rates ranged from 85.5% to 92%, our findings were lower. These differences may be explained by methodological and contextual disparities, as both studies were conducted in high-income settings, used cross-sectional designs, and had smaller sample sizes.
Our most notable finding was the significant association between ART initiation or continuation and retention in care, with a 35.9 times higher odds of remaining in care after 1 year. This reinforces the importance of universal treatment, a globally recognized strategy for improving retention in care,26,27 reducing mortality and severe clinical events. 28 However, our results differ from a study in the Democratic Republic of the Congo (DRC), where a “treat-all” strategy was associated with higher rates of attrition and loss to follow-up (LTFU). 29 One possible explanation is that unlike that study, our 12-months assessment did not rely solely on local EHR. As described in our methods, we complemented this information by searching the NHSS to verify vital status and identify silent transfers (i.e., ART retrieval at other facilities), a factor not considered in the DRC study, which may have led to an overestimation of loss to follow-up.
This study also highlights the high prevalence of structural factors that increase vulnerability among TGW, such as sex work, substance use, and low levels of formal education. Participants who had a record of cocaine use were 83% less likely to be on ART at 1 year of follow-up. These results are consistent with studies from this region30,31 and among other vulnerable populations,32,33 underscoring the need for integrated interventions. Specific strategies that address both substance use and other structural determinants are essential to improve outcomes across the care cascade.
Our results suggest that once retention in care and sustained ART use are achieved, baseline characteristics do not appear to significantly influence virological suppression rates at 1 year. However, considering all individuals linked to care, less than half achieved virological suppression after 1 year (44.1%). Better outcomes have been observed in studies from high-income countries, 25 even in cohorts with similar characteristics. 24 Individual, structural, and health system barriers may explain these differences, underscoring the need for further research comparing the care cascades of TGW and the general population.
Among the strengths of this study is the integration of multiple data sources—the hospital’s electronic medical records, digital laboratory records, and national surveillance systems—which allowed for detailed follow-up and reduced potential data bias. However, several limitations must be considered. While the study’s single-center nature could be seen as a constraint, we argue that its setting in a large, public, tertiary-level hospital within a major Latin American metropolis makes it a representative case study for similar urban environments across the world. The high participant mobility observed—with nearly 60% of participants diagnosed at other centers and 40% having prior ART experience—is therefore not just a methodological challenge but a key finding that reflects the real-world complexities faced by public health systems globally.
The retrospective design limited analysis to routinely collected data; crucial factors like housing instability, mental health, stigma, 34 and hormone therapy 23 were not systematically documented. Potential non-differential misclassification bias regarding substance use (reference group including those with no data) likely biases findings towards the null, suggesting stronger true associations. Pharmacy pickups as adherence proxies and historical viral load variations may affect precision. While systematic, our EHR-based identification (using structured sex/gender fields) relies on disclosure, potentially missing ‘stealth’ individuals. Finally, unmeasured sexualized drug use (chemsex) precluded exploring hidden collinearity with sex work.
Conclusions
In this first real-world analysis of the HIV care cascade for TGW in Argentina, we demonstrate that significant gaps in care persist, driven by a complex interplay of clinical, social, and structural factors. Our findings underscore that while prompt ART initiation is a powerful tool for improving retention, it is insufficient on its own. Addressing structural barriers, such as substance use, through integrated and interdisciplinary health services is essential to improve outcomes for this key population. This study provides critical evidence needed by Ministries of Health and public health programs to design sustainable public policies that create safe, accessible healthcare environments for TGW globally. Future research should build on these findings to identify targeted interventions that can close these persistent health disparities.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a fellowship granted by the Ministry of Health of the Autonomous City of Buenos Aires, under Resolution N° 1549-MSGC-2022.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.