
Abstract
Background
Genital mpox has been scarcely described in Central and West Africa where the disease is endemic. This study aimed to describe the clinical manifestations of genital mpox acquired through sexual contact in heterosexual African couples.
Methods
This was a case series of patients presenting with genital lesions associated or without febrile pustular or vesicular eruptions and confirmed with a positive PCR. Medical records of patients were scrutinized between March 2022 and December 2025 in three dermatology centres located either in Cameroon or Benin. Sociodemographic characteristics, clinical features, laboratory results, treatment, and outcomes were systematically documented.
Results
In total, nine cases of genital mpox from six heterosexual couples were documented. Patients’ median age was 35 years (IQR 31-42 years; range: 28–45 years). Two heterosexual partners were living with HIV with undetectable plasma viral loads. Sexual contact preceding genital lesions’ onset was reported in seven of 9 cases (78%). The incubation period ranged from 3 to 10 days. Clinical manifestations included vesicles, pustules, erosions, ulcerations, genital edema, umbilicated necrotic papules, and inguinal lymphadenopathy. The morphology of lesions varied from rounded/oval to arcuate and linear patterns. The recovery time ranged from 2 to 8 weeks, though longer for ulcerations. People living with HIV experienced severe presentations and prolonged recovery.
Conclusion
Genital manifestations of mpox on black skin are polymorphic and can present with atypical features. Mpox should be considered as a differential diagnosis of genital lesions following condomless sexual intercourse, particularly in endemic areas.
Introduction
Mpox was first described in 1970 in a 9 months old infant living in the Democratic Republic of the Congo. Since then, Central and West Africa have become endemic to this infectious disease. In 2022, a global mpox outbreak occurred, affecting both Africa and other regions including Europe, Asia, North America and Australia, with a total of 119 countries and territories confirming at least one case of mpox. 1 In 2022 and 2024, WHO declared mpox as a Public Health Emergency of International Concern. 1
Clinical manifestations of the disease, after an incubation period of 7 to 17 days, are very similar to those of human smallpox. 2 They consist of functional and general symptoms (fever, asthenia, myalgia, odynophagia), cutaneous or mucosal signs (vesicles, pustules or pseudo-pustules, erosions, skin necrosis, ulcerations), and superficial polyadenopathies.3,4 However, genital manifestations of mpox on the black skin during contamination through sexual intercourse may present particular features. 3 Biological diagnosis of the disease is based on detection of viral DNA by polymerase chain reaction (PCR) from skin, mucosal, or blood samples. 5
In Western countries, numerous studies have described genital manifestations of mpox, particularly among men who have sex with men (MSM), who represented the most affected group. 1 In contrast, African data remain limited despite the endemicity of the disease. In Nigeria, Ogoina and James reported mpox among linked heterosexual partners, confirming that heterosexual transmission also occurs in endemic settings. 6 These findings highlight the need for better characterization of genital mpox in Black African patients, particularly through sexual transmission, as specific clinical features may remain underreported. 3
Willing to contribute in filling this gap, this study was undertaken, aiming to provide a more detailed clinical description of genital manifestations of mpox in Black Africans living in endemic areas.
Patients and Methods
This was a case series study conducted between March 2022 and December 2025 in three dermatology centres, namely the Department of Dermatology and Venereology of the Hubert Koutoukou Maga National University Hospital Centre in Cotonou (Benin), the Buruli Ulcer and Leprosy Screening and Treatment Centre in Pobè (Benin), and the Ad Lucem Medical Foundation in Douala (Cameroon).
We reviewed medical records of patients presenting with genital lesions, with or without associated febrile vesicular or pustular skin eruptions. Eligible patients were adults (≥18 years) with PCR-confirmed mpox and documented genital involvement, defined as lesions affecting the external genitalia (penis, scrotum, vulva, labia), perineum, or perianal region. Only patients with complete medical records were included, and informed consent was obtained for prospectively identified cases.
Patients with either suspected mpox but negative or unavailable PCR confirmation, or incomplete medical records lacking critical clinical data were not included in this study.
Data were collected on sociodemographic characteristics (age, sex, occupation), relevant medical history (including HIV status and sexual orientation), clinical features (disease onset, duration of symptoms, type and distribution of lesions), laboratory findings (mpox PCR, HIV serology, syphilis serology), therapeutic management and evolution.
Data were subsequently coded, entered and analysed using Microsoft Excel 2019. Quantitative data are summarised using median and interquartile range (IQR) while qualitative data are summarised using frequencies and percentages.
The study was conducted in accordance with the Declaration of Helsinki and national ethical guidelines, and approved by Institutional Review Board along with the Directors of the various study sites. All identifying information were removed from data collection forms and clinical photographs.
Results
Between March 2022 and December 2025, a total of nice patients meeting all inclusion criteria were included in the study. They had a median age of 36 years (interquartile range [IQR]: 31-42 years; range: 28-45 years). There were five males (56%), giving a male/female sex ratio of 1.25.
Among these patients, there were two partners both living with HIV, regularly followed-up with undetectable HIV viral loads.
Sexual contact preceding genital lesion onset was reported in seven of 9 cases (78%)
Clinical characteristics
Systemic symptoms were reported in a subset of patients. Fever (≥38°C) was observed in 4/9 patients (44.4%), myalgia in 3/9 (33.3%), odynophagia in 2/9 (22.2%), and arthralgia in 2/9 (22.2%). Inguinal lymphadenopathy was present in all patients (9/9, 100%).
Cutaneous lesions were polymorphic, with multiple types of lesions observed on the same patient. The most common lesions were umbilicated necrotic papules (6/9, 66.7%) (Figures 1 and 2), ulcerations (5/9, 55.6%) (Figure 3), pustules or pseudo-pustules (4/9, 44.4%), vesicles (3/9, 33.3%), genital oedema (3/9, 33.3%) (Figure 4), and skin erosions (2/9, 22.2%). Characteristic umbilicated papules with central necrosis of vulva. Necrotic papules of pubis. Linear ulcer on right major labia. Edema and necrotic lesion on penis.



The configuration of lesions was predominantly round or oval (6/9, 66.7%). Less common patterns included deep linear ulcerations (1/9, 11.1%), notably with a “knife-cut” appearance on the labia majora, arcuate lesions (1/9, 11.1%), and irregular or polymorphic lesions (1/9, 11.1%).
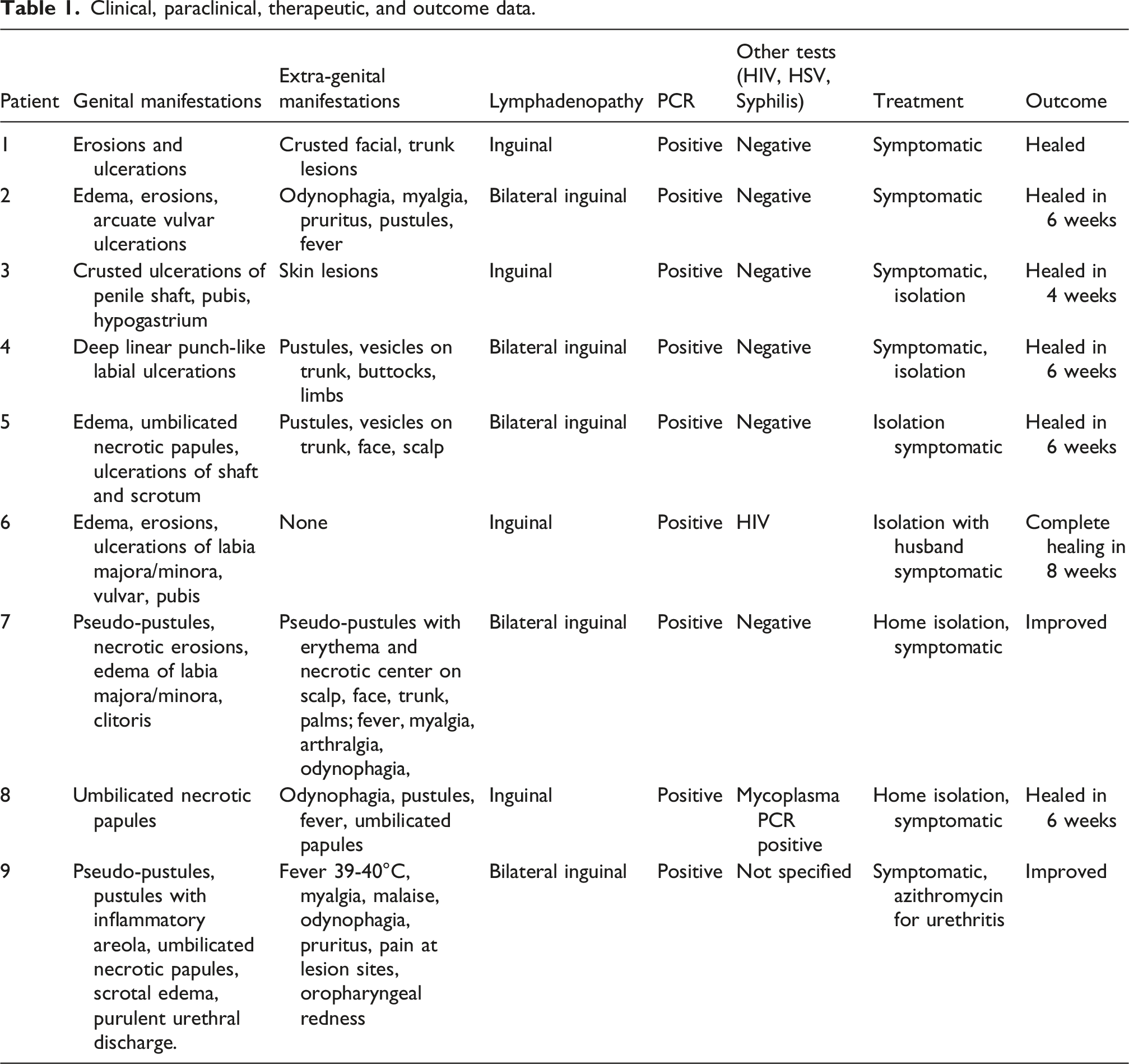
Clinical, paraclinical, therapeutic, and outcome data.
The shape of lesions varied: sometimes round or oval (6/9; 66.7%), sometimes arcuate (1/9; 11.1%), sometimes linear and deep (1/9; 11.1%). The base was often dirty and necrotic. The borders were sharp, sometimes irregular. The lesions were sometimes isolated, sometimes coalescent, forming plaques with irregular borders. The number of genital lesions ranged from two lesions to more than 100 lesions (Figure 5). Multiple copper like papules on vulve.
Syphilis serology was negative for all patients. Concomitant mycoplasma infection was present in 1 patient (positive PCR). One patient had urethral discharge caused by Neisseria gonorrhea.
All patients were treated symptomatically with antiseptics, analgesics, and antibiotics in case of superinfection. They were all isolated. The recovery time of lesions ranged from 2 to 8 weeks. This period was longer for ulcerations than for erosions.
Discussion
This case series highlights several noteworthy features of mpox in Black African patients presenting with predominant genital involvement in a heterosexual context.
Similar observations have been reported in West Africa, particularly in Nigeria, where mpox is endemic and where several outbreaks have predominantly involved heterosexual individuals. Indeed, studies conducted in Nigeria have described transmission patterns consistent with close physical and possibly sexual contact, including within households and intimate partnerships, highlighting a broader transmission dynamic than initially reported in non-endemic settings. 7
In this study, genital involvement was prominent with a high density of lesions located at the presumed site of inoculation, while extra-genital involvement was limited and less severe. This distribution supports the hypothesis of direct mucocutaneous transmission during intimate contact. In contrast, extra-genital areas such as the face, trunk, and limbs showed fewer lesions, typically vesicular or pustular. Similar genital predominance and clustering of lesions at the site of contact have been described in sexually transmitted mpox cases, further supporting this transmission route.4,6
Another striking finding from this study is the marked polymorphism of genital lesions. An unusual morphology was deep linear or arcuate ulcerations, which may reflect a Koebner-like phenomenon where mechanical or frictional factors contribute to the linearity of lesions. These atypical and heterogeneous presentations can lead to significant diagnostic confusion with other ulcerative sexually transmitted infections, particularly genital herpes or syphilis. 8 This diagnostic challenge is even greater in endemic regions where sexually transmitted infections are highly prevalent and frequently overlap clinically. As highlighted in dermatology reviews, mpox should therefore be considered in the diagnostic workup of atypical genital ulcerations, especially in patients with risk factors for sexually transmitted infections (STI). 9 Furthermore, recent epidemiological analyses, including systematic reviews from Nigeria, emphasize the role of sexual behaviour in mpox transmission and support the integration of mpox testing into routine STI screening strategies in endemic settings. 10
Conclusion
Genital manifestations of mpox on the black skin demonstrate marked clinical polymorphism and may present with atypical morphological features. Mpox should be considered as a differential diagnosis of any genital lesion contracted through condomless sexual intercourse, particularly in endemic areas. A non-judgmental and sensitive approach is essential to optimize patient management and limit viral transmission while addressing the stigmatization associated with this sexually transmitted infection.
Supplemental material
Supplemental Material - Sexually-acquired genital manifestations of mpox in black-skin African patients: A case series of nine cases
Supplemental Material for Sexually-acquired genital manifestations of mpox in black-skin African patients: A case series of nine cases by Felix Atadokpede, Dahlia Noelle Tounouga Ndanga, Florys Mastaki, Boubacar Mahaman, Christelle Legonou, Abilogoun Aurel Chokki, Pascal Bisimwa, Syvaine Pentoue, Laura Dotsop, Akimath Habib, Berenice Degboe, Angele Azonkouanou in International Journal of STD & AIDS.
Footnotes
Ethical considerations
Patient confidentiality was maintained throughout the study in accordance with institutional guidelines.
Author contributions
AF: conceptualization of the study; AF, TNDN, BM: literature review and writing of the first draft. TNDN, and AF: review and editing and all authors approved the final draft.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.