
Abstract
Background
Human papillomavirus (HPV) associated cervical cancer remains the leading cause of cancer mortality among women in resource-limited settings. The WHO recommends HPV screening with a high-performance screening test for women by age 35 and 45 years. We compared the Cepheid Xpert HPV test to the hybriSpot laboratory-based assay among women living with Human Immunodeficiency Virus (WLHIV) starting antiretroviral treatment (ART).
Methods
In this cross-sectional analysis we performed a rapid Xpert HPV test on an endocervical liquid-based cytology (LBC) sample, which detects 14 high-risk HPV (hr-HPV) subtypes (HPV16, HPV18/45,
Results
Among 47 WLHIV included, the median age was 32 [Interquartile Range 28–39] years, and mean CD4 count 338 cells/µl. Overall, 32 (68%) WLHIV were positive for hr-HPV on the Xpert assay and 35 (74.5%) WLHIV were positive on the hybriSpot platform. Agreement between the Xpert and hybriSpot tests was good (kappa co-efficient ≥0.75) for the detection of HPV16, HPV18/45 and other hr-HPV subtypes, except for hr-HPV subtypes 51, 59 (kappa co-efficient 0.56). High sensitivity (>90%) was observed only for the P3 (HPV 31, 33, 35, 52, 58) and P4 (HPV39, 56, 66, 68) channels, while specificity exceeded 90% for all channels except P4. Among P3 HPV subtypes, particularly HPV52, prevalence was high in this subset as detected by the hybriSpot assay.
Conclusions
The Xpert HPV test demonstrated high agreement when compared to a laboratory PCR-based reverse dot-blot hybridisation assay among WLHIV at ART initiation. Near point-of-care HPV testing may be beneficial where HPV screen-and-treat models can be integrated into routine HIV care.
Introduction
Human papillomavirus (HPV)-associated cervical cancer remains the leading cause of cancer morbidity and mortality among women in resource-limited settings. 1 In South Africa cervical cancer is the leading cause of cancer deaths among women of reproductive age, who also share a significant burden of Human Immunodeficiency Virus (HIV). 2 The World Health Organization’s call to action for the elimination of cervical cancer in 2021 requires that 70% of women are screened with a high-performance HPV DNA test by age 35 years and again at 45 years, however in a recent survey screening uptake remains suboptimal at 40.5% nationally. 2
The Xpert HPV test is a molecular assay previously evaluated in various international settings and recently approved by the WHO as a primary screening test for cervical cancer, particularly in low- and middle-income countries (LMICs). 3 However, limited data exist on its performance in real-world clinic-based testing among women living with HIV (WLHIV) in South Africa. Point-of-care (POC) or near-POC clinic-based platforms offer same day testing and availability of results with the opportunity to refer those screening positive into rapid treatment pathways. The Xpert HPV test, compatible with liquid-based cytology sampling, is further compatible with GeneXpert Instrument systems, widely available for use in South Africa for other diseases like tuberculosis, which may offer an important opportunity to bring HPV testing to routine primary healthcare services. 3 However, results are reported qualitatively as positive or negative for all channels, making it difficult to distinguish individual high-risk HPV (hr-HPV) subtypes and concurrent infections within individual channels which may pose a challenge where HPV genotyping is used for triage.
WLHIV have a six-fold higher risk of cervical cancer compared to women without HIV due to increased risk for HPV acquisition, HPV persistence and faster progression to invasive cervical cancer. 4 National HIV care guidelines recommend screening from HIV diagnosis with 3 yearly screening intervals thereafter, until age 50 5 . For this group, novel approaches may be needed to offer women same day screen-and-treat options, shown to be implementable in local and other LMIC settings. 6
In this study, we aimed to evaluate the performance of the Xpert HPV test against a laboratory-based HPV assay in WLHIV in an HIV endemic setting.
Methods
Study design and setting
We conducted a prospective diagnostic accuracy study of the Xpert HPV assay, as a sub-study within a randomized clinical trial in Durban, South Africa. 7 Briefly, between February 2021 and June 2023, consenting women 18 years or older, were screened for cervical cancer using HPV and cytology co-testing. 8
HPV testing
Xpert HPV testing was performed on 1.1 ml of a ThinPreP cytology sample collected in a PreservCyt medium (Hologic, Marlborough, Massachusetts, USA).
8
The Xpert HPV assay (Cepheid, Sunnyvale, California, Unites States) is designed to detect HPV16, 18/45 and 11 other hr-HPV subtypes (
Test validation
For test validation, 200 µl of the same ThinPreP sample was tested using the HPV Direct Flow Chip assay on a hybriSpot 12 platform (Vitro S.A., Master Diagnostica, Sevilla, Spain), referred to here as the hybriSpot assay, once a minimum of 40 consecutive samples were collected. The hybriSpot assay evaluates the same hr-HPV subtypes as the Xpert HPV test and an additional 21 high-risk (26, 53, 73, 82) and low-risk HPV subtypes. The laboratory validation test was conducted retrospectively on samples stored at −80°C before testing. Briefly, the 200 ul sample was centrifuged and washed in phosphate-buffered saline, and 4 ul of the resuspended pellet was used as template for PCR. Amplification was performed using the kit’s ready-to-use reaction mix containing biotinylated L1 primers and β-globin internal control primers. Hybridisation and colourimetric detection were performed automatically on the hybriSpot 12 system, and results were interpreted using hybriSoft software, where a threshold value of 10 was established for positivity i.e. approximately 50–500 type-specific genome equivalents per PCR reaction. Each run included negative and endogenous amplification controls to verify assay integrity and sample adequacy. Validation samples were processed independently of the Xpert assay.
Statistical analysis
Diagnostic accuracy of the assays was measured by calculating sensitivity, specificity, positive and negative predictive values (PPV, NPV) and 95% confidence intervals using the Wilson score method. Agreement between the assays was measured using Cohen’s Kappa coefficient. Analyses were performed using SAS software version 9.4 (SAS Institute Inc., Cary).
Results
Baseline characteristics
Of 260 WLHIV who had HPV screening at or near the time of ART initiation, 47 women were included in this sub-analysis, based on test availability. 8 Women, median age 32.0 (28.0–39.0) years, had a median of 4.0 (3.0–6.0) lifetime partners and none were vaccinated against HPV. The mean CD4 count was significantly lower among women with HPV infection than those without (247 vs 526 cells/µL; p < 0.001).
HPV testing by Xpert HPV
The frequency of HPV for each channel was HPV16: 12.8%, HPV18/45: 29.8%, P3 (HPV31, 33, 35, 52 or 58): 46.8%, P4 (HPV51 or 59): 19.2% and P5 (HPV 39, 56, 66 or 68): 23.4%. HPV positivity was not mutually exclusive between channels. Multiple hr-HPV co-infection (>1 Xpert channel) was detected in 36% (17/47) of women. Median Ct values were similarly high across all channels reported as positive on the Xpert test (HPV16: 30.7 [IQR 23.8–33.0], HPV18/45: 30.9 [IQR 23.6–33.3]; P3: 27.8 [IQR 24.9–34.7]; P4: 29.4 [IQR 26.0–34.3]; P5: 32.3 [IQR 27.9–33.1].
HPV testing with the hybriSpot assay
Overall, the frequency of 14 hr-HPV subtypes was HPV16: 12.8%, HPV18: 14.9%, HPV31: 12.8%, HPV33: 4.3%, HPV35: 10.6%, HPV39: 8.5%, HPV45: 23.4%, HPV51: 4.3%, HPV52: 25.5%, HPV56: 6.4%, HPV58: 12.8%, HPV59: 4.3%, HPV66: 2.1% and HPV68: 8.5% on the hybriSpot assay. The frequency of HPV subtypes according to the Xpert channels was similar for all channels except for P4, with the Xpert frequency observed at 19.2% and hybriSpot at 8.5%. The hybriSpot assay detected concurrent hr-HPV infections in almost 30% (14/47) of women, while 44.7% (21/47) of women had a single HPV infection.
Diagnostic accuracy
Evaluation of the Xpert HPV point-of-care test against the hybriSpot assay overall and by Xpert HPV channels (n = 47).
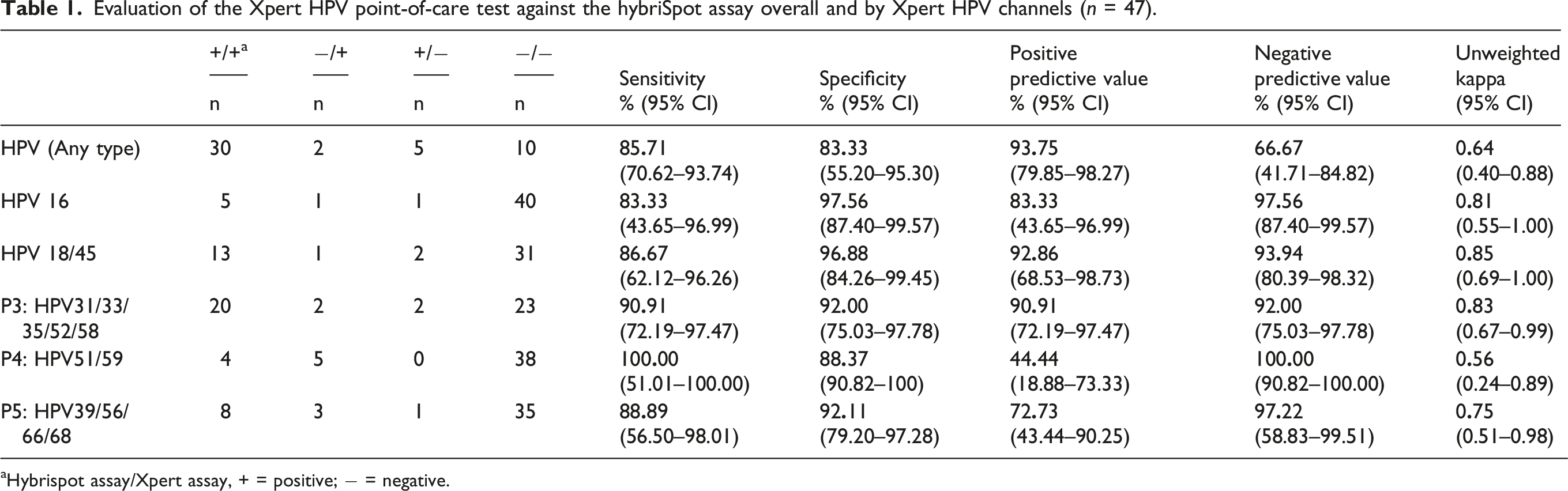
aHybrispot assay/Xpert assay, + = positive; − = negative.
Discussion
The Xpert HPV POC test demonstrated high specificity when compared to a laboratory-based reverse dot-blot PCR assay, indicating strong ability to correctly identify hr-HPV negative samples. Sensitivity was slightly lower overall in this cohort of WLHIV, who were known to have a high prevalence of multiple concurrent hr-HPV infections. 8 The frequency of HPV subtypes detected by each test was generally similar across channels, except for the P4 channel (HPV51 and 59), where the Xpert assay detected more cases than the reference assay. The P4 grouping in the Xpert assay was pre-specified by the manufacturer (Cepheid) to reflect regional HPV subtype prevalence and assay optimization priorities; however, lower concordance in this channel warrants further evaluation.
In the current analysis, the hybriSpot assay identified HPV52 as the most prevalent infection in this subset, detected in 25.5% (12/47) of women. Additionally, HPV31, HPV33, HPV35 and HPV58 were frequently detected, supporting the predominance of P3 subtypes reported previously in the same cohort. 8 Except for HPV35, these subtypes are common to the nine-valent HPV vaccine, suggesting the potential for substantial vaccine impact on HPV-associated disease in WLHIV.
The Xpert and hybriSpot assays have different sensitivities, specificities, reproducibility, and repeatability values, which may also differ for each HPV genotype. While the hybriSpot assay is based on the amplification and detection of a fragment in the viral L1 region of papillomaviruses, the Xpert assay detects the E6/E7 region of the viral DNA genome. The HPV16 results may be a more accurate reflection of test validity as this is the only single genotype that the Xpert test measures. For this analysis, although consecutive samples were collected for test validation, these were randomly selected from the larger cohort. The small sample size is a limitation of this analysis therefore the study findings should be interpreted with caution given the wide confidence intervals in some accuracy estimates. Reassuringly, the trends observed align with other validation studies in WLHIV. 10
This study demonstrates the comparability of the Xpert HPV test to complementary testing of individual HPV subtypes to support the national surveillance of viral prevalence and dynamics required for prevention and control of HPV-associated cervical cancer, particularly in WLHIV.
Supplemental material
Supplemental material - Diagnostic accuracy of the Xpert HPV assay in women starting antiretroviral treatment in South Africa
Supplemental material for Diagnostic accuracy of the Xpert HPV assay in women starting antiretroviral treatment in South Africa by Nivashnee Naicker, Lenine Liebenberg, Kunthi Naidoo, Farzana Osman, Kirusha Naidoo, Sharana Mahomed, Natasha Samsunder, Paul K. Drain, Nigel Garrett in International Journal of STD & AIDS
Footnotes
Acknowledgements
The authors would like to thank the STREAM HIV study participants for their contribution to this study.
Ethics considerations
Ethics approval of the STREAM HIV study protocol, version 2.3, 5 October 2020, was granted by the University of KwaZulu-Natal (UKZN) Biomedical Research Ethics Committee (BREC) [BREC/00000833/2019], the University of Washington Institutional Review Board [STUDY00007544], and the Division of AIDS Regulatory Support Center [38,509]. ![]() ID: NCT04341779 and South African National Clinical Trial Registry Number DOH-27-072,020-7877.
ID: NCT04341779 and South African National Clinical Trial Registry Number DOH-27-072,020-7877.
Consent to participate
Study participants provided written informed consent at study entry.
Author contributions
NN: Sub-investigator STREAM HIV trial, provided clinical oversight of cervical cancer screening, Xpert HPV test implementation, test validation and manuscript preparation. LL: Mucosal immunologist, provided oversight of test validation procedures and manuscript preparation. Kunthi Naidoo: Laboratory technician, conducted all Xpert HPV assays on the GeneXpert platform and manuscript review. FO: Statistician, completed all statistical analyses and manuscript preparation and review. Kirusha Naidoo: Sub-investigator STREAM HIV trial, provided clinical oversight of trial participants and manuscript review. SM: Sub-investigator STREAM HIV trial, manuscript review and editing. NS: Laboratory Director, oversight of all laboratory procedures and manuscript preparation. PD: Principal Investigator STREAM HIV trial, study supervision, manuscript review and editing. NG: Principal Investigator STREAM HIV trial, study supervision, manuscript review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The STREAM HIV study was funded by the US National Institutes of Health (R01AI147752). Cepheid provided the Xpert HPV cartridges for this evaluation at no cost. NIH and Cepheid have no role in study design, implementation, data management, analysis, interpretation of outcomes or preparation and dissemination of findings.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The full dataset that supports the findings of this study are available from the corresponding author, Nivashnee Naicker, upon request by the journal. The STREAM HIV protocol paper may be accessed at: PMCID: PMC8493905. DOI: ![]() .
7
.
7
Supplemental material
Supplemental material is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.