
Abstract
One of the ways in which therapists treat anxiety disorders is to expose patients to a fear-evoking stimulus within a safe environment before encouraging more positive stimulus-related thoughts. In the study reported here, we adapted these psychotherapeutic principles of exposure therapy to test the hypothesis that imagining a positive encounter with a member of a stigmatized group would be more likely to promote positive perceptions when it was preceded by an imagined negative encounter. The results of three experiments targeting a range of stigmatized groups (adults with schizophrenia, gay men, and British Muslims) supported this hypothesis. Compared with purely positive interventions, interventions in which a single negative encounter was imagined just prior to imagining a positive encounter resulted in significantly reduced prejudice. Furthermore, reduced anxiety uniquely derived from the mixed-valence imagery task statistically explained enhanced intentions to engage positively with the previously stigmatized group in the future.
It is almost universally the case that psychological approaches to reducing prejudice try to promote positive perceptions of stigmatized groups—with good reason. These approaches have yielded some significant success in improving intergroup relations (Crisp & Turner, 2009; Pettigrew & Tropp, 2006; Turner, Hewstone, & Voci, 2007). In contrast, negative thoughts, feelings, and beliefs about other groups are the foundation of prejudice toward all manner of groups in societies across the world (Paolini, Harwood, & Rubin, 2010). Conversely, one of the ways in which therapists treat anxiety disorders is to first expose patients to fear-evoking stimuli before introducing positive images or experiences to counter the recurrent negative thoughts—an approach that has been found to effectively diminish the anxiety associated with the phobic stimulus (see Holmes & Mathews, 2010). In the research reported here, we drew on the principles used in the psychotherapeutic treatment of anxiety disorders to develop a short form of “exposure therapy” to “treat” prejudice against stigmatized groups. We found that when it comes to promoting positive group perceptions, negativity is not all bad, and that, a small dose of negativity administered just prior to a positively focused intervention can be surprisingly effective in reducing prejudice toward stigmatized groups.
Anxiety: The Etiology of Prejudice
Research on intergroup contact has firmly established anxiety as the most robustly supported determinant of prejudice (Pettigrew & Tropp, 2006). Anxiety about potentially poor, embarrassing, or difficult interactions with stigmatized group members leads individuals to avoid contact (Stephan & Stephan, 1985), compels them to rely on stereotypes (Wilder, 1993), lowers the communication quality (Gudykunst & Shapiro, 1996), and causes them to experience physiological stress (Blascovich, Mendes, Hunter, Lickel, & Kowai-Bell, 2001).
Research developing interventions to reduce prejudice have correspondingly focused on combating anxiety about interacting with stigmatized groups. Most notable among these approaches is intergroup contact theory (Allport, 1954; Brown & Hewstone, 2005; Pettigrew, 1998). According to a recent meta-analysis of over 500 contact studies, reduced anxiety is the primary mechanism through which exposure (i.e., contact) reduces prejudice (Pettigrew & Tropp, 2006), and much work has shown anxiety to be a major mediator in prejudice reduction (e.g., Blascovich et al., 2001; Page-Gould, Mendoza-Denton, & Tropp, 2008; Paolini, Hewstone, Cairns, & Voci, 2004; Stephan & Stephan, 1985; Voci & Hewstone, 2003). Given the importance of anxiety for reducing prejudice, it makes sense to develop interventions that target anxiety as the cause of prejudice. To do this, we looked beyond research on intergroup relations to other fields. We focused on specialized approaches to reducing anxiety: psychotherapeutic treatments for anxiety disorder. What we found in this literature qualifies the practical truism that to reduce prejudice, researchers must unequivocally promote positive perceptions to combat stigma and discrimination; instead, our findings suggest that a little negativity can go a long way in combating the causes of stigmatization.
Reducing Anxiety Through Exposure: Psychotherapeutic Principles
A common disorder-maintaining symptom in anxiety disorders (e.g., posttraumatic stress disorder, social phobia, or phobias for specific things such as animals or height) is negative imagery (Hirsch & Holmes, 2007). Research in clinical and cognitive psychology proposes a special link between mental imagery and emotion, especially anxiety (Holmes & Mathews, 2005; Kosslyn, 1994). Clinical treatments of anxiety disorders therefore focus on repeating or modifying such images with the aim of reducing their emotional power. Early forms of treatment used imagery as part of a desensitization approach for treating phobias (Wolpe, 1959), and more-recent forms use cognitive-behavioral therapy (Hirsch, Clark, Mathews, & Williams, 2003).
There are a number of forms of cognitive-behavioral therapy that draw on the power of imagery in tackling anxiety disorders. Exposure therapy (also referred to as systematic desensitization, imaginal exposure, or in vivo exposure; e.g., Foa, Rothbaum, Riggs, & Murdock, 1991) confronts the patient with fear- evoking objects or situations within a safe environment, with patients instructed to actively visualize and describe the phobic stimulus. Similarly, in systematic desensitization, therapists work with the client to form a graduated anxiety hierarchy and to tackle these with concomitant imaginal relaxation techniques, as these are antagonistic to an anxious physiological state. This technique has been found to be a highly effective way to reduce anxiety in clinical contexts (Choy, Fyer, & Lipsitz, 2007; Himle, 2007; Rothbaum & Schwartz, 2002; Tarrier et al., 1999; Wolpe, 1959).
In their emotional-processing theory, Foa and Kozak (1986) argue that fear emerges through a development of a fear memory, which elicits escape and avoidance. Their logic is based on Lang’s (1977, 1979) bioinformational theory of emotional imagery, in which fear represents a network in memory— the “fear structure.” These cognitive representations contain stimulus information, responses to the stimulus (verbal, physiological, and behavioral), and interpretive information about meaning (threat or danger). Exposure therapies operate through emotional processing, which is defined as “the modification of memory structures that underlie emotions” (p. 20). Successful therapies can modify this fear structure if two conditions are met. First, the fear memory can only be modified when it is activated. Second, corrective information must be available to form a new memory structure that replaces the old, anxiety-provoking structure. The therapy fails if these conditions are not met—for example, because of cognitive avoidance or overvalued ideation (Foa & Kozak, 1986).
An Imaginal Intervention
Drawing on the principles of exposure therapy, we conceived of stigmatized groups as a type of phobic stimulus and intergroup anxiety as a nonpathological fear structure. If this analogy holds, then just as activating negative thoughts and feelings associated with the phobic stimulus before introducing positive countervailing thoughts is maximally effective at decreasing negative reactions in the treatment of anxiety disorders (Foa & Kozak, 1986), this should be the case in tackling negative perceptions of stigmatized groups. In three experiments, we therefore tested the hypothesis that prepositive negative imagery would enrich and enhance, rather than reduce, the impact of receiving positive information about stigmatized groups.
Experiment 1
In Experiment 1, we sought preliminary support for the hypothesis that imagining a negative experience followed by a positive experience with the stigmatized group would be more effective at reducing intergroup anxiety than imagining a positive experience followed by another positive experience. Although seemingly counterintuitive, this hypothesis is derived from firm theory and research in psychotherapeutic methods and, if substantiated, would establish an important new principle in research developing interventions to reduce prejudice. In Experiment 1, we focused on stigma toward people with mental health problems—specifically, adults with schizophrenia.
Method
Twenty-nine participants (25 female, 4 male) without mental health problems, aged between 18 and 38 years (M = 21.14, SD = 4.96), took part in an online study and were randomly allocated to two imaginal-exposure conditions. One group was asked to imagine two positive contact situations with an adult with schizophrenia (positive-positive imaginal exposure); the other group imagined a negative contact situation first and then a positive contact situation (negative-positive imaginal exposure). We compared the effects of negative-then-positive imaginal exposure with the effects of positive-then-positive imaginal exposure to control for the number of exposures. Participants received course credit as reward for their participation.
Procedure
Participants were told at Time 1 that the aim of the study was to investigate “imagery and group perceptions” and were then randomly assigned to two conditions. Participants in the positive-positive condition were first asked, “Please take a moment to imagine yourself meeting an adult with schizophrenia for the first time. Imagine that the interaction is positive, relaxed, and comfortable.” Participants in the negative-positive condition received the following instruction: “Please take a moment to imagine yourself meeting an adult with schizophrenia for the first time. Imagine that the interaction is negative, tense, and uncomfortable.” Following this, to reinforce the effects of the imagery task, all participants were instructed to write down what they imagined in as much detail as possible before completing an intergroup anxiety measure.
At Time 2, participants in both conditions received the positive imaginal-exposure instructions: “Please take a moment to imagine yourself meeting an adult with schizophrenia for the first time. Imagine that the interaction is positive, relaxed, and comfortable.” As at Time 1, participants were instructed to write down what they imagined in as much detail as possible before completing the remaining dependent measures. Finally, participants were thanked and debriefed.
Dependent measures
Anxiety concerning a future interaction with adults with schizophrenia was measured after both imaginal exposures. Participants were asked, “The next time you find yourself in a situation where you might interact with an adult with schizophrenia, to what extent do you think you will feel . . . ,” followed by 10 items from the Intergroup Anxiety Scale (Stephan & Stephan, 1985). Participants reported how awkward, suspicious, embarrassed, defensive, anxious, happy (reverse-scored), comfortable (reverse-scored), self-conscious, confident (reverse-scored), and careful they would feel on a 7-point Likert scale (1 = not at all, 7 = very much). Items were recoded such that higher scores represented higher intergroup anxiety. A composite intergroup anxiety score was created by computing the mean of these items for Time 1 (α = .74) and Time 2 (α = .78).
Results and discussion
To determine whether a change in the valence of the imaginal-exposure instruction influenced anxiety about a future interaction with an adult with schizophrenia, we conducted a mixed-model analysis. Imaginal exposure (positive-positive vs. negative-positive) was entered as a between-participants factor, and time (intergroup anxiety at Time 1 vs. intergroup anxiety at Time 2) was entered as a within-participants factor. The hypothesis was that imagining negative contact followed by positive contact with an adult with schizophrenia would lead to lower anxiety at Time 2 compared with imagining two positive contact experiences.
There was a significant main effect of time. Overall, anxiety was significantly lower at Time 2 (M = 2.93, SD = 0.70) compared with Time 1 (M = 3.91, SD = 0.78), F(1, 27) = 48.17, p < .0005. More important, the predicted interaction between imaginal exposure and time was significant, F(1, 27) = 23.61, p < .0005. To decompose this interaction, we computed simple main effects for both time points using the method specified by Howell (2002). Unsurprisingly, at Time 1, imagining a negative encounter produced higher anxiety (M = 4.31, SD = 0.80) compared with imagining a positive encounter (M = 3.48, SD = 0.48), F(1, 27) = 11.26, p = .002. However, critically, at Time 2, despite participants in both conditions imagining a positive encounter, subsequent anxiety was lower after first imagining a negative encounter at Time 1 (M = 2.69, SD = 0.81) compared with first imagining a positive encounter at Time 1 (M = 3.19, SD = 0.45), F(1, 27) = 4.21, p = .046 (see Fig. 1).
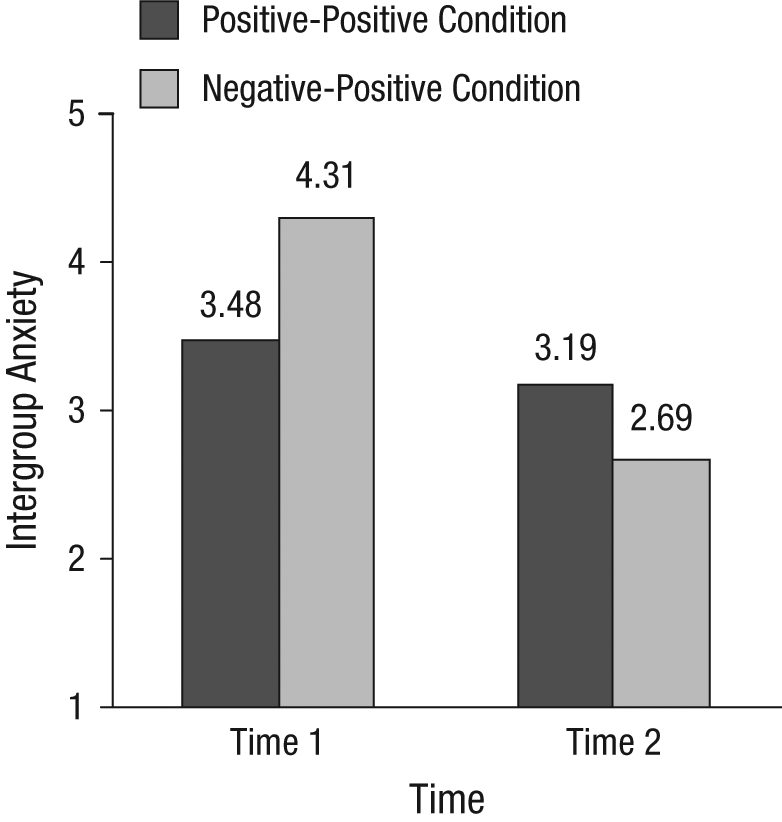
Results of Experiment 1: participants’ ratings of intergroup anxiety as a function of measurement time and imaginal-exposure condition.
The pretest-posttest design that we employed meant that we could also compare Time 2 anxiety in the negative-positive condition with Time 1 anxiety in the positive-positive condition. This analysis confirmed that imagining a positive encounter after imagining a negative encounter resulted in lower anxiety (M = 2.69) compared with imagining a single positive encounter at Time 1 (M = 3.48), t(27) = 3.17, p = .004.
Experiment 2a
In Experiment 1, we established support for the basic principle of exposure therapy that negative feelings directed toward stigmatized groups were more effectively banished when imaginal exposure begins with a negative encounter. Imagining a negative experience with the stigmatized group member prior to imagining a positive experience led to a greater reduction in anxiety compared with imagining two positive encounters. This is consistent with emotional-processing theory (Foa & Kozak, 1986) and the idea that to counter negative associations in memory with positive information, it is first necessary to activate the “fear structure” in memory. In Experiment 2, we sought to replicate this effect with a different target group and to test whether the reduced anxiety elicited by this approach would drive a broader change in orientations toward the stigmatized group: intentions of contacting that group in the future.
Method
Thirty-two male heterosexual students aged between 18 and 24 years (M = 19.59, SD = 1.64) were randomly allocated to two imaginal-exposure conditions in an online study. One group was asked to imagine two successive positive contact situations with a gay man (positive-positive condition); the other group was asked to imagine a negative contact situation first and then a positive contact situation afterward (negative-positive condition). Participants received course credit for their participation.
The imaginal-exposure procedure was identical to that used in Experiment 1. Intergroup anxiety (α = .78) and future contact intentions were measured following the completion of the second imaginal exposure. Future contact intentions were assessed with seven items (taken from Husnu & Crisp, 2010a), such as “How willing would you be to participate in a discussion group that includes both heterosexual men and gay men that will focus on issues of homosexuality in the UK?” These items were measured on a 9-point Likert scale (1 = not at all, 9 = very much). A composite intentions score was created from the mean of these items (α = .87).
Results and discussion
Table 1 shows means and standard deviations for the measures of anxiety and future contact intentions. Despite participants in both Time 2 conditions imagining a positive encounter, anxiety was lower after participants had first imagined a negative encounter (M = 2.18) compared with a positive encounter (M = 2.81), t(30) = 3.06, p = .005. Furthermore, future contact intentions were higher in the negative-positive condition (M = 5.25) compared with the positive-positive condition (M = 3.99), t(30) = −2.48, p = .019.
Mean Ratings of Anxiety and Future Contact Intentions in Experiment 2a
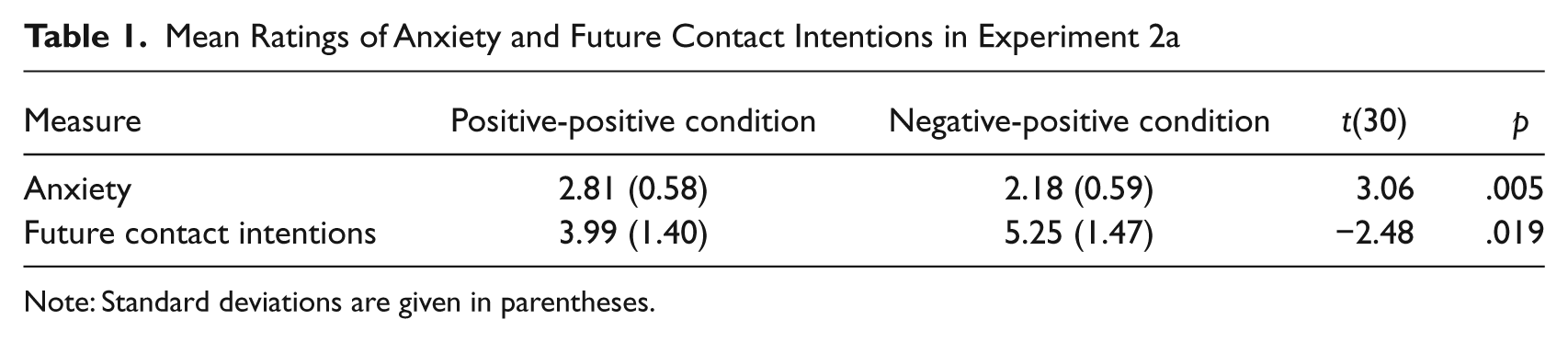
Note: Standard deviations are given in parentheses.
We computed a mediational analysis to assess whether the impact of imaginal exposure on future contact intentions was mediated by intergroup anxiety (see Fig. 2a). Imaginal exposure was recoded as −1 (positive-positive condition) and +1 (negative-positive condition) and predicted contact intentions (β = 0.41), t(30) = 2.48, p = .019. Imaginal exposure also significantly predicted the mediator, intergroup anxiety (β = −0.49), t(30) = −3.06, p = .005. The path between intergroup anxiety and future contact intentions while controlling for imaginal exposure was significant (β = −0.46), t(29) = −2.64, p = .013. When intergroup anxiety was controlled, the relationship between imaginal exposure and future contact intentions became nonsignificant (β = 0.19), t(29) = 1.08, p = .287. A Sobel test was significant (Z = 2.06, p = .039).
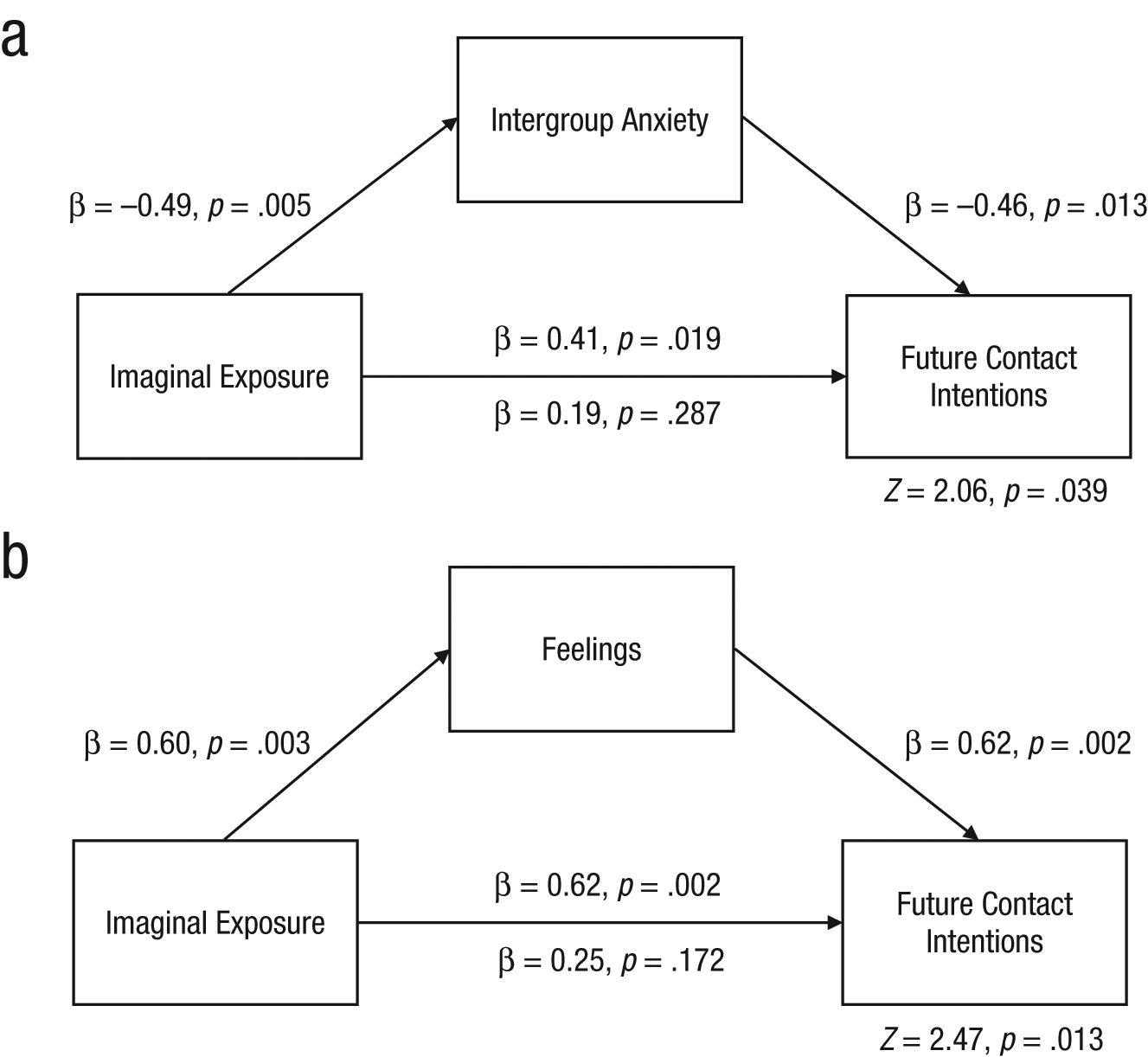
Mediation models showing the influence of imaginal exposure on future contact intentions, as mediated by intergroup anxiety (a; Experiment 2a) and feelings (b; Experiment 3). In both models, the statistics below the lower path show results when controlling for the mediator, and the statistics above the lower path show results when the mediator was not included in the model.
In sum, imagining a negative intergroup encounter with a gay man before imagining a positive encounter reduced intergroup anxiety to a greater extent than simply imagining two positive encounters, and this reduced anxiety led directly to improved future contact intentions toward gay men.
Experiment 2b
A potential alternative explanation for these results is that we simply observed a contrast effect in the negative-positive condition (e.g., Mussweiler, 2003). To rule out this explanation, we replicated Experiment 2, replacing the target group with an in-group. We did this because although the predictions for the contrast-effects and emotional-processing accounts converge for out-group targets, they diverge for in-group targets. The contrast-effects account predicts the same accentuated positivity in the negative-positive condition irrespective of whether the target is an in-group or an out-group. However, this is not the case for the emotional-processing account. Because there is no fear structure for the in-group that can be activated or modified, this account predicts no accentuated impact in the negative-positive condition.
Thirty straight men (mean age = 21.5 years, SD = 6.65) took part in an online study. The procedure was largely identical to that employed in Experiment 2, except that we replaced the gay men (out-group) with straight men (in-group). Anxiety was measured at Time 1 and Time 2. Simple main effects revealed that at Time 1, imagining a negative encounter produced higher anxiety (M = 2.75, SD = 0.86) compared with imagining a positive encounter (M = 2.25, SD = 0.48), F(1, 28) = 4.12, p = .048. However, at Time 2, anxiety did not differ between the imaginal-exposure conditions (positive-positive: M = 2.13, SD = 0.63; negative-positive: M = 2.16, SD = 0.70), F(1, 28) < 1, p = .895. This finding is consistent with the emotional-processing account and inconsistent with a simple contrast-effects explanation.
Experiment 3
In Experiment 3, we sought to more closely align research on exposure therapy with research in reducing prejudice and to further enhance the generalizability of the observed effects. Previous work on imaginal exposure has almost exclusively examined the impact of positive contact imagery after a single exposure (for a review, see Crisp, Husnu, Meleady, Stathi, & Turner, 2010; but see Husnu & Crisp, 2010b). This work has established a mediational route from positive imagery to intentions via intergroup anxiety (see Husnu & Crisp, 2010a). We therefore compared affect and intentions following this standard single-exposure imaginal task with affect and intentions following the combined negative-positive imaginal task used in Experiments 1 and 2. Although this no longer controls for number of exposures, we know from Experiments 1 and 2 that the effects cannot be attributable to this, and what we gain is a closer direct comparison with existing work on prejudice reduction. In addition, we made two further changes. First, instead of simply measuring anxiety, we employed a more generic measure of positive feelings toward the stigmatized group, one that is used frequently in the literature on prejudice reduction. If reduced anxiety is driving more-general changes in affective orientation toward the stigmatized group, then convergent support should be gleaned from consonant but relevant measures of affective reaction. Second, we shifted focus to a third group that suffers from stigmatization: British Muslims.
Method
Twenty-two non-Muslim British students (13 female, 9 male) aged between 18 and 41 years (M = 21.05, SD = 4.56) were randomly allocated to two imaginal-exposure conditions. One group was asked to imagine a single positive contact experience with a British Muslim stranger (positive-only condition), and the other group was asked to imagine first a negative contact experience and then a positive contact situation (negative-positive condition). Participants received a small payment (£3) for their participation.
The procedure was identical to that employed in Experiments 1 and 2 except focused on British Muslims, and we compared participants who carried out only a single positive imaginal-exposure task with participants who carried out a negative then a positive imaginal-exposure task. Feelings toward British Muslims were measured by asking participants to describe how they felt about British Muslims in general on a semantic differential ranging from 1 to 9 (adapted from Wright, Aron, McLaughlin-Volpe, & Ropp, 1997): cold-warm, positive-negative (reverse-scored), friendly-hostile (reverse-scored), suspicious-trusting, respectful-contempt (reverse-scored), and admiration-disgust (reverse-scored). Items were recoded such that higher scores represented more positive feelings toward British Muslims (i.e., lower prejudice). A composite score was created by taking the mean of these items (α = .87). We measured future contact intentions as in Experiment 2, with a composite index created by taking the mean of the items (α = .86).
Results and discussion
Table 2 shows means and standard deviations for participants’ ratings of feelings and future contact intentions. Results supported the hypothesis. Feelings toward British Muslims were more positive in the negative-positive condition (M = 6.89) compared with the positive-only condition (M = 5.37), t(20) = −3.36, p = .003. Future contact intentions were higher in the negative-positive condition (M = 6.62) compared with the positive-only condition (M = 4.77), t(20) = −3.52, p = .002.
Mean Ratings of Feelings and Future Contact Intentions in Experiment 3
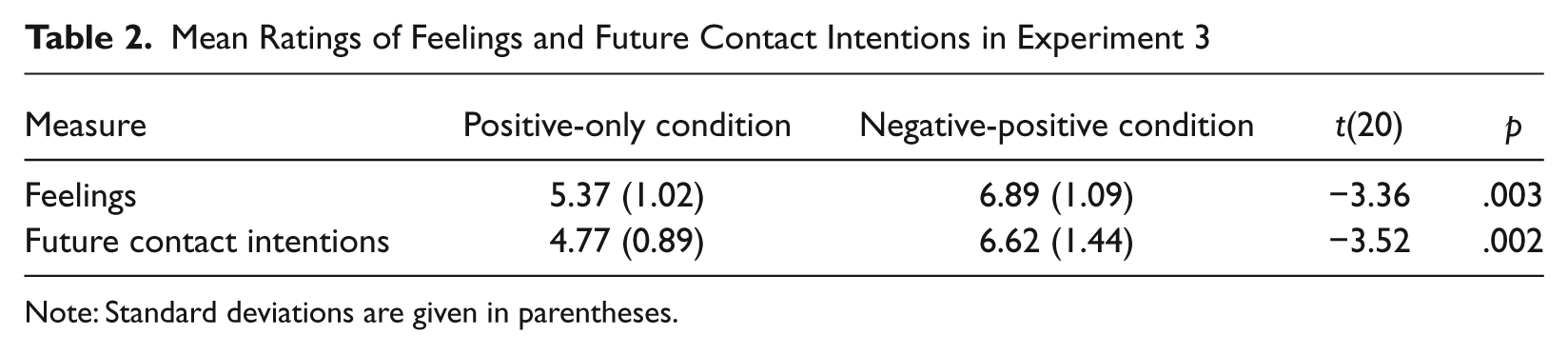
Note: Standard deviations are given in parentheses.
We computed a mediational analysis to assess whether the effect of imaginal exposure on future contact intentions was mediated by the elicitation of more positive feelings toward British Muslims (see Fig. 2b). Imaginal exposure was coded as −1 (positive-only condition) and +1 (negative-positive condition) and predicted contact intentions (β = 0.62), t(20) = 3.52, p = .002. Imaginal exposure also significantly predicted feelings (β = 0.60), t(20) = 3.36, p = .003. The path between feelings and intentions controlling for imaginal exposure was significant (β = 0.62), t(19) = 3.50, p = .002, and when feelings were controlled, the relationship between the imaginal-exposure task and intentions became nonsignificant (β = 0.25), t(19) = 1.42, p = .172. A Sobel test was significant (Z = 2.47, p = .013).
In sum, Experiment 3 showed that imagining a negative out-group encounter prior to imagining a positive out-group encounter was more effective at enhancing future contact intentions than simply thinking about a single positive encounter. Furthermore, in line with the theory underlying exposure therapy, results showed that intentions to engage in future contact were enhanced because the negative-positive exposure order elicited more positive feelings about the out-group than the positive-only exposure did.
General Discussion
In psychotherapy, two steps are effective in reducing anxiety. Patients are confronted with anxiety-provoking objects or situations to activate the fear memory, and once this is activated, it can be modified through corrective information (Foa & Kozak, 1986). We tested whether adapting the principle of prepositive negative imaginal exposure would enhance the effectiveness of subsequent positive imaginal exposure. Previous research on reducing prejudice has established the benefits of positive imaginal exposure to stigmatized groups (for recent reviews, see Crisp, Birtel, & Meleady, 2011; Crisp et al., 2010). In the research reported here, we investigated the benefits of negative imaginal exposure.
In Experiment 1, participants without mental health problems imagined a positive encounter with an adult with schizophrenia after having imagined a negative encounter. Participants reported less intergroup anxiety compared with participants who imagined two positive encounters. In Experiment 2, heterosexual male participants imagined a positive encounter with a gay man after having imagined a negative encounter. These participants experienced less intergroup anxiety, which mediated enhanced future contact intentions, compared with participants who imagined two imagined positive contact experiences. In Experiment 3, British non-Muslim participants who imagined a negative encounter with a British Muslim before imagining a positive one reported greater future contact intentions toward British Muslims compared with participants who engaged in a single positive imaginal encounter, a tendency mediated by the development of more positive feelings toward the previously stigmatized group.
The negative impact of anxiety is a link between research on psychotherapies and social interventions aiming to promote more positive intergroup relations. The studies reported in this article demonstrate the efficacy in exploring convergences between the two domains. Intergroup anxiety contaminates or even prevents interactions between conflicting groups. Because the prospect of intergroup contact can evoke both the subjective experience of intergroup anxiety and a physiological threat response, it is important to introduce the idea of contact to individuals who might otherwise be disinclined to entertain such thoughts.
In this research, we drew on the emotional-processing account of exposure therapy to inform our theoretical model of the underlying process driving the observed effects. We chose this because it provided the clearest point of synthesis with research on intergroup contact (particularly with respect to the key role played by anxiety reduction). However, it is important to note that several parallel processes are involved in exposure therapy in clinical practice (Tryon, 2005). For instance, as well as the process that we identified in intergroup contexts (the activation and correction of the fear network; Foa & Kozak, 1986), increasingly positive attitudes toward the phobic stimulus can be achieved through the restructuring of cognitive appraisals (e.g., Beck, 1976). With respect to the latter, exposure therapy can involve a conscious recognition, reflection, and correction of the maladaptive beliefs (Hoffmann, 2008; Tryon, 2005). Research has shown that exposure therapy involves not only low-level processes, such as those observed in the present research, but also higher-order metacognitive processes that compel individuals to reevaluate the rationality of their beliefs (see Samoilov & Goldfried, 2000). This process of conscious recognition and reflection (or, to use an analogy from the contact literature, the motivation to avoid appearing prejudiced; Monteith, 1993) does not rule out our explanation and is, as with cognitive-behavioral therapy, a component parallel process. An important endeavor for future research will be to identify self-regulatory and other processes that might be involved in this intersection of clinical therapy and intervention techniques designed to reduce prejudice.
Conclusion
Previous research has established the benefits of imaginal exposure to stigmatized groups. We have shown for the first time that a negative tone can be helpful (when used in a controlled setting) and a positive tone follows. This work also demonstrates the value in integrating insights from other areas, such as clinical psychology, for developing maximally effective intervention strategies. The research reported in this article supports the idea that such imaginal interventions should not necessarily be unequivocally positive but that a small dose of negativity may most effectively reduce intergroup anxiety and improve intergroup perceptions.
Footnotes
Acknowledgements
We are grateful to Amy King for her assistance in conducting this research.
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.