
Abstract
Although preconception and prenatal maternal stress are associated with adverse outcomes in birth and childhood, their relation to infant mortality remains uncertain. We used logistic regression to study infant mortality risk following maternal stress within a population-based sample of infants born in Sweden between 1973 and 2008 (N = 3,055,361). Preconception (6–0 months before conception) and prenatal (between conception and birth) stress were defined as death of a first-degree relative of the mother. A total of 20,651 offspring were exposed to preconception stress, 26,731 offspring were exposed to prenatal stress, and 8,398 cases of infant mortality were identified. Preconception stress increased the risk of infant mortality independently of measured covariates, and this association was timing specific and robust across low-risk groups. Prenatal stress did not increase risk of infant mortality. These results suggest that the period immediately before conception may be a sensitive developmental period with ramifications for infant mortality risk.
Keywords
Infant mortality, or death in the 1st year of postnatal life, places substantial stress on families and imposes a financial burden on society (Mathews & MacDorman, 2008). Despite substantial reductions in rates of infant mortality over recent decades, the rate is estimated at 6 to 7 deaths per 1,000 live births in the United States and, unfortunately, has remained stable for more than a decade (Mathews & MacDorman, 2008). Rates of infant mortality vary by maternal socioeconomic status and ethnicity and across nations (Kitsantas & Gaffney, 2010). Sweden experiences 2.7 deaths per 1,000 live births, whereas Afghanistan reports the highest rate of infant mortality worldwide, a distressing 121.6 deaths per 1,000 live births (Central Intelligence Agency, 2009). Identifying robust risk factors, vulnerable periods of development, and etiological mechanisms of infant mortality is essential for designing effective global prevention programs (March of Dimes, Partnership for Maternal, Newborn and Child Health, Save the Children, & World Health Organization, 2012).
Research on the roles of preconception stress and prenatal maternal stress on infant mortality has been limited. Intervention research, however, has suggested that both preconception and prenatal stress may influence infant mortality (Berghella, Buchanan, Pereira, & Baxter, 2010; Catov, Bodnar, Olsen, Olsen, & Nohr, 2011). Poor preconception maternal mental health is associated with increased risk of having a stillbirth or a low-birth-weight child (Witt, Wisk, Cheng, Hampton, & Hagen, 2012). Preconception multivitamin use (Catov et al., 2011) and improved preconception self-care, characterized in part by reduced stress (Berghella et al., 2010), are associated with reduced risk of adverse birth outcomes, such as preterm birth and small-for-gestational-age (SGA) status, which are among the strongest predictors of infant mortality (Mathews & MacDorman, 2008). Animal research has indicated that preconception stress is associated with long-term impairment in offsprings’ brain functioning and plasticity (Huang et al., 2010). Prenatal maternal stress increases the risk for adverse birth outcomes (Class, Lichtenstein, Langstrom, & D’Onofrio, 2011; Khashan et al., 2009) and stillbirth (Wisborg, Barklin, Hedegaard, & Henriksen, 2008). Thus, preconception and prenatal maternal stress may directly or indirectly (through adverse birth outcomes) increase offsprings’ risk for infant mortality.
Exploring whether vulnerability differs by stress-exposure period may help to clarify sensitive developmental periods (Glynn, Wadhwa, Schetter, Chicz-DeMet, & Sandman, 2001) and thereby improve our understanding of etiological mechanisms of infant mortality. Preconception stress may affect the mother for several months (Stroebe, Schut, & Stroebe, 2007) and, therefore, affect fetal development during conception and the vulnerable process of organogenesis. The prenatal period may be a period of increased sensitivity because of the rapid development of essential systems (Gluckman & Hanson, 2004).
We sought to rigorously examine the potential associations between preconception and prenatal maternal stress and infant mortality in a large Swedish population. We hypothesized that exposure to both preconception and prenatal maternal stress would moderately increase infant mortality risk and that associations would be mediated partially by gestational age and SGA status (Altman, Bonamy, Wilkstrom, & Cnattingius, 2012).
Method
Study population
After approval by the institutional review boards at Indiana University and the Karolinska Institutet, we constructed a large, population-based Swedish sample by linking several population registries. The Medical Birth Registry (Cnattingius, Ericson, Gunnarskog, & Kallen, 1990) included data on more than 99% of all births in Sweden between 1973 and 2009 and was used to obtain information on gestational age at birth and SGA status. Information on family relatedness was drawn from the Multi-Generation Registry (Statistics Sweden, 2006). The Cause of Death Registry was used to identify cases of infant mortality and family members’ dates of death to indicate exposure to stress. The Education Register (Statistics Sweden, 2010) provided data on parents’ highest level of completed formal education, and the National Crime Register provided data on parental criminal convictions.
The initial sample comprised 3,632,650 individuals born between 1973 and 2008 whose data included their mother’s identity. The offspring year of birth was truncated at 2008 to allow all offspring to have the potential to live through the risk period. We removed offspring whose grandmother (n = 416,927; 11.5%) or father (n = 35,408; 1.0%) could not be identified. We excluded cases of multiple births (n = 75,777; 2.1%) because the rate of adverse birth outcomes for multiple births differs from that for singleton births (Mathews & MacDorman, 2008). We also excluded children with missing data on gestational age at birth (6,466; 0.2%), which was required for calculating the date of conception and determining risk-exposure windows. Because of potential erroneous values, offspring with a gestational age of more than 42 weeks and 6 days (n = 36,497; 1.0%) were removed. We also removed families with more than 13 children (54 families; < 0.1%) and one case (< 0.1%) for which parity information was missing. We then excluded offspring whose parental nationality status was unknown (n = 2,623; < 0.1%) and offspring who had emigrated out of Sweden with their families before their first birthday (n = 3,536; < 0.1%). The final cohort consisted of 3,055,361 (84.1%) infants who were still residing in Sweden at their first birthday.
Measures
The preconception period was defined as the 6 months prior to conception. The prenatal period was defined as the period between conception and birth. Preconception was further divided into two periods (6–4 months prior to birth and 3–0 months prior to birth). Similarly, the prenatal period was divided into trimesters (Trimester 1: 0–12 weeks; Trimester 2: 13–24 weeks; Trimester 3: 25 weeks to birth).
Preconception and prenatal maternal stress were defined as death of a first-degree relative of the mother. For preconception stress, first-degree relatives included parents, siblings, and already-born children of the mother. For prenatal stress, first-degree relatives also included the biological fathers of offspring. If more than one of a mother’s relatives died within one exposure period, the first date of exposure was used. Offspring of mothers who experienced both preconception and prenatal stress were removed from analyses (n = 204; < 0.01%). (No cases of infant mortality were identified within this subsample; therefore, sensitivity analyses could not be performed using this group.)
All models predicted a dichotomous indicator of infant mortality defined as death of the offspring within the 1st year of life. Preterm birth was defined as birth at or before 37 weeks of gestation. SGA status was indicated by birth weight less than 2 standard deviations below the mean for gestational age according to standard curves for the Swedish population (Marsal et al., 1996).
Analyses
We used PROC SURVEYLOGISTIC in SAS 9.2 to obtain odds ratios (ORs) from logistic regression analyses that accounted for family clustering at the maternal level. The first model was unadjusted. The second model controlled for measured statistical covariates associated with stress exposure, infant mortality, or both (Mathews & MacDorman, 2008). Covariates included offspring birth year, sex, and birth order (first born, referent; second born; third born; or fourth born and later); maternal and paternal age (< 20 years; 20–24 years; 25–29 years, referent; 30–34 years; or > 34 years); highest level of maternal and paternal education (missing; primary or lower secondary education of 9 years or fewer; 1–3 years of upper secondary school, referent; or postsecondary education); parental country of birth (binary and categorized as Swedish or non-Swedish); and maternal and paternal lifetime history of criminality (binary). Analyses also were adjusted for previous infant mortality in the family, defined as the death of an already-born sibling outside of the pregestational or prenatal exposure window, because previous infant mortality may predict future conception outcomes and infant death (Wilcox & Gladen, 1982).
To evaluate possible mediation by gestational age and reduced fetal growth, we examined whether preconception and prenatal stress predicted preterm birth and SGA status (Khashan et al., 2009). We separately examined whether preterm birth and SGA status were associated with infant mortality (Altman et al., 2012; Mathews & MacDorman, 2008). To test for mediation, we predicted infant mortality from stress exposure while adjusting for gestational age at delivery (22–27 weeks, 6 days; 28–30 weeks, 6 days; 31–33 weeks, 6 days; 34–36 weeks, 6 days; or 37–42 weeks, 6 days, referent) and SGA status.
Sensitivity analyses
Sensitivity analyses were used to rule out alternative hypotheses for the associations found. First, we examined moderation by offspring sex (Mathews & MacDorman, 2008). Second, risk for infant mortality following maternal stress in preconception months 18 to 13 and 12 to 7 was examined to test whether stress in preconception months 6 to 0 conferred a unique risk to the offspring. Third, we explored whether associations were present in offspring without adverse birth outcomes, restricting the cohort to offspring that were born full term, had a normal birth weight (≥ 2,500 g), and were not SGA. Fourth, in cases of offspring with siblings, we restricted analyses to include only those from sibling pairs with an average interpregnancy-interval length (12–35 months from birth of an older sibling to conception of the index offspring). Fifth, we limited the sample to offspring exposed to stress due to death of a maternal parent or sibling only, not an already-born child. Thus, we tested whether associations were independent of immediate-family mortality risk or due to cascading stress from a previous child’s death. Finally, we restricted the sample to offspring for whom information on maternal smoking during pregnancy was available (birth years 1982–2008).
Results
We identified 8,398 (0.3%) infant deaths. Table 1 provides descriptive characteristics by stress-exposure status. As presented in Table 2, preconception stress predicted infant mortality in unadjusted analyses (OR = 1.65, 95% confidence interval, CI = [1.34, 2.02]), and the association remained robust to the inclusion of measured covariates (adjusted OR = 1.53; 95% CI = [1.25, 1.88]).
Descriptive Characteristics of All Singleton Pregnancies in Sweden (1973–2008) With Live-Born Offspring by Maternal Stress Exposure Status
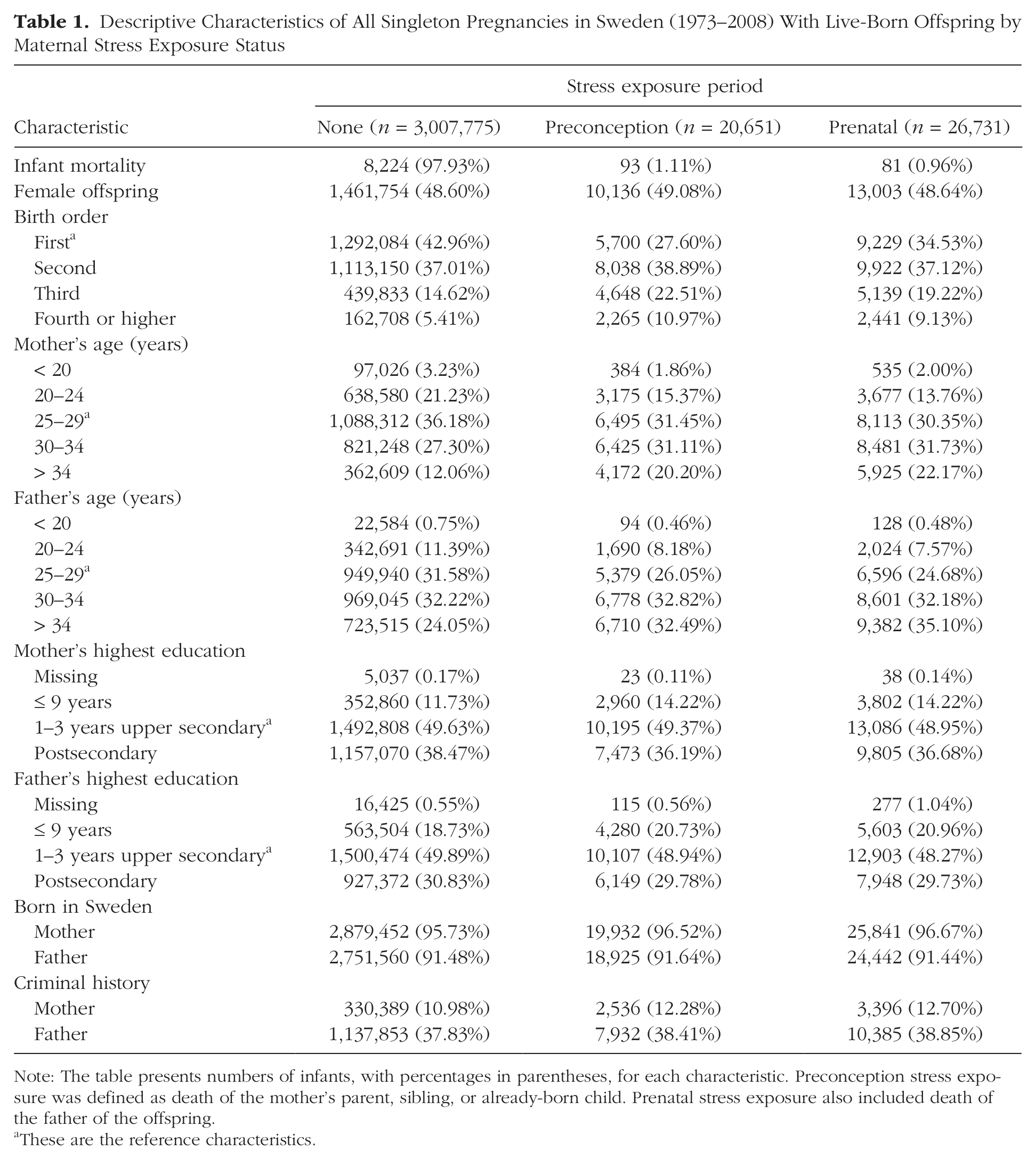
Note: The table presents numbers of infants, with percentages in parentheses, for each characteristic. Preconception stress exposure was defined as death of the mother’s parent, sibling, or already-born child. Prenatal stress exposure also included death of the father of the offspring.
These are the reference characteristics.
Risk for Infant Mortality Across the Preconception and Prenatal Stress Exposure Periods
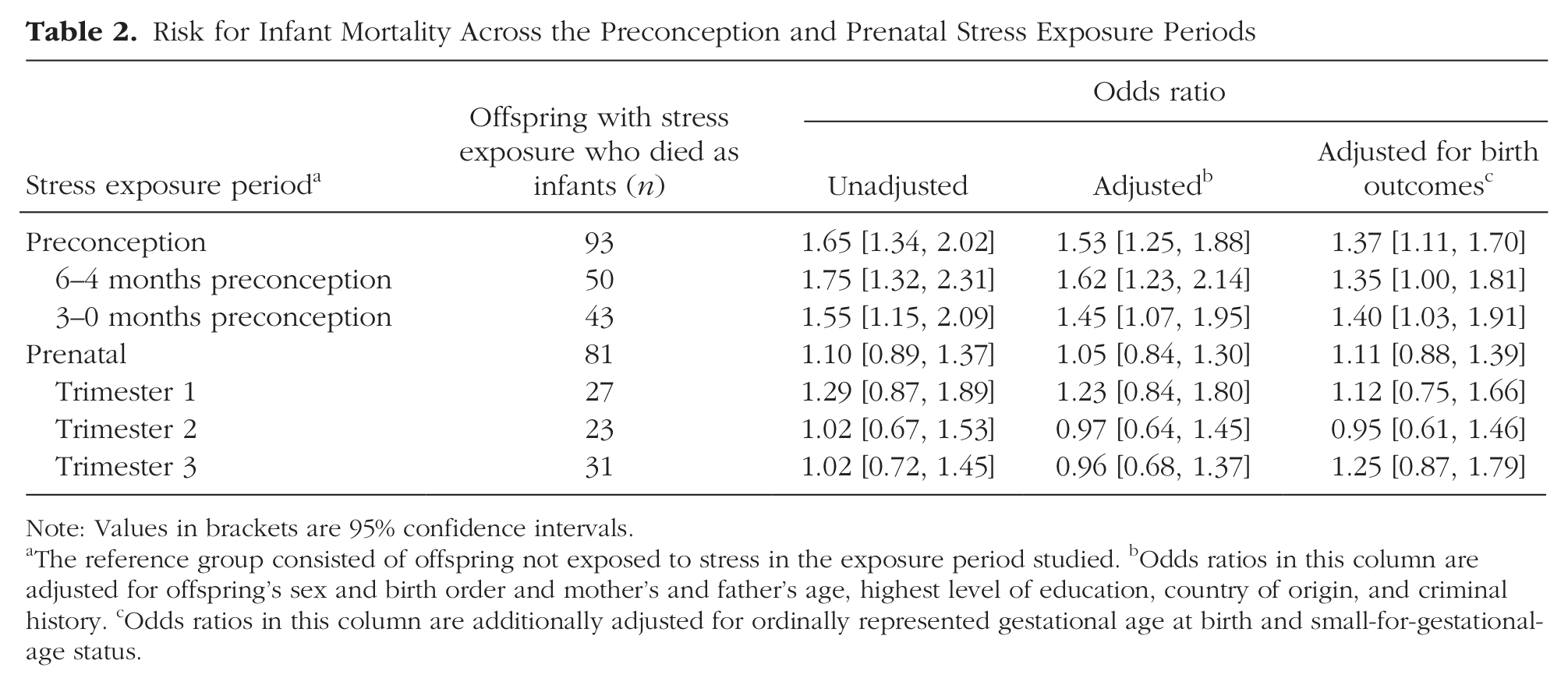
Note: Values in brackets are 95% confidence intervals.
The reference group consisted of offspring not exposed to stress in the exposure period studied.
Odds ratios in this column are adjusted for offspring’s sex and birth order and mother’s and father’s age, highest level of education, country of origin, and criminal history.
Odds ratios in this column are additionally adjusted for ordinally represented gestational age at birth and small-for-gestational-age status.
Preconception stress increased risk for preterm birth (adjusted OR = 1.19; 95% CI = [1.12, 1.26]) and SGA status (adjusted OR = 1.14; 95% CI = [1.05, 1.23]). Preterm birth (adjusted OR = 16.05; 95% CI = [15.35, 16.77]) and SGA (adjusted OR = 9.04; 95% CI = [8.55, 9.56]) were associated with increased risk for infant mortality. Therefore, we further adjusted for gestational age and SGA status to study their potential mediating effects. The association with preconception stress remained robust (adjusted OR = 1.37; 95% CI = [1.11, 1.70]; see Table 2). Nevertheless, the reduction in magnitude (i.e., OR = 1.53 vs. OR = 1.37) suggests that shorter gestational length and SGA status partially mediated the association between preconception stress and infant mortality.
Prenatal maternal stress was not associated with infant mortality in unadjusted models (OR = 1.10, 95% CI [0.89, 1.37]), adjusted (OR = 1.05; 95% CI = [0.84, 1.30]), or models adjusted for birth outcomes (OR = 1.11; 95% CI = [0.88, 1.39]; see Table 2). We did not find large or statistically significant associations when we separated the prenatal period by trimester. We did, however, find associations between prenatal stress and increased risk for preterm birth (Trimester 2 adjusted OR = 1.16; 95% CI = [1.05, 1.27]) and between prenatal stress and SGA status (Trimester 2 adjusted OR = 1.19; 95% CI = [1.05, 1.34]).
As Table 3 shows, preconception sensitivity analyses revealed an interaction of mortality with sex, b = −0.45, SE = 0.22, p = .04, wherein male offspring were at a greater risk for infant mortality (adjusted OR = 1.83; 95% CI = [1.42, 2.35]) compared with female offspring (adjusted OR = 1.15; 95% CI = [0.81, 1.64]). Stress exposure during preconception months 18 to 13 (adjusted OR = 0.91; 95% CI = [0.68, 1.22]) and preconception months 12 to 7 (adjusted OR = 0.97; 95% CI = [0.76, 1.26]) did not increase risk for infant mortality (Fig. 1). Risk for infant mortality remained elevated in infants born at full term who were at normal birth weight and normal weight for gestational age (adjusted OR = 1.61; 95% CI = [1.20, 2.17]). The association was robust in offspring born within an average (12–35 month) interpregnancy interval (adjusted OR = 2.09; 95% CI = [1.37, 3.21]) and when stress was defined as the death of a maternal parent or maternal sibling only (adjusted OR = 1.31; 95% CI = [1.01, 1.69]). Finally, preconception stress continued to independently predict infant mortality when we controlled for smoking during pregnancy (adjusted OR = 1.35; 95% CI = [1.01, 1.81]).
Results of Sensitivity Analyses Examining Preconception Stress Exposure
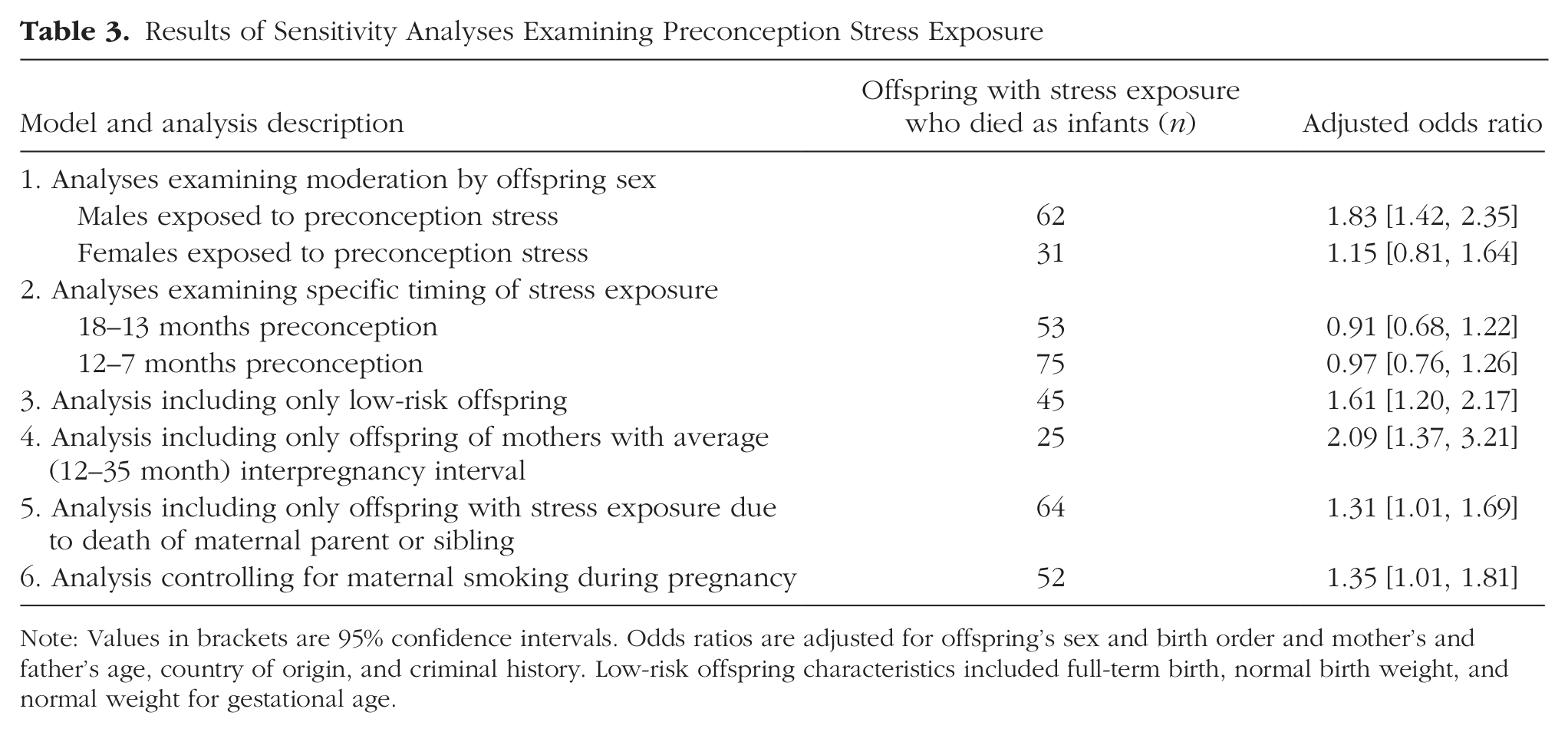
Note: Values in brackets are 95% confidence intervals. Odds ratios are adjusted for offspring’s sex and birth order and mother’s and father’s age, country of origin, and criminal history. Low-risk offspring characteristics included full-term birth, normal birth weight, and normal weight for gestational age.
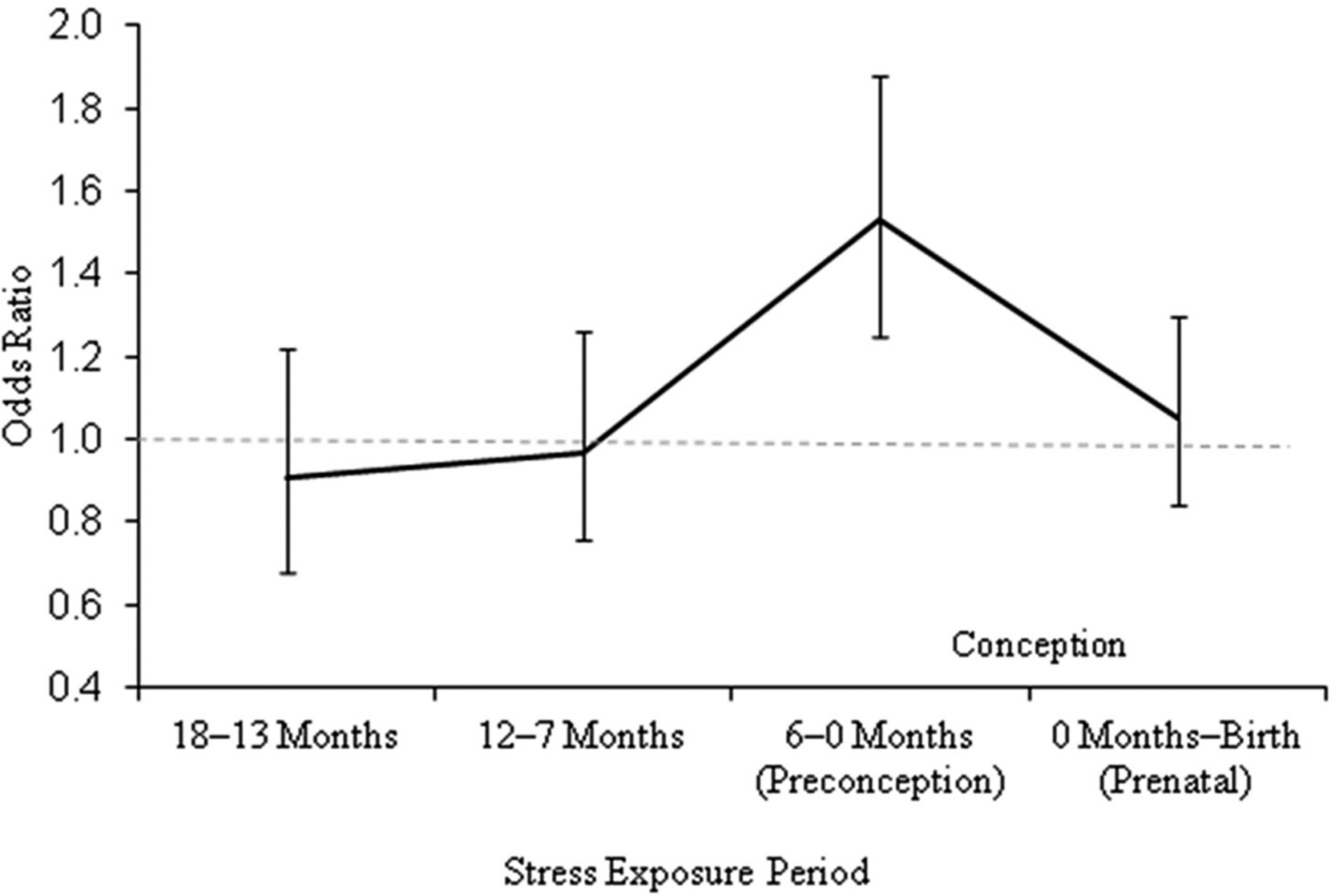
Risk (adjusted odds ratio) of infant mortality following maternal stress exposure during the preconception (18–13 months, 12–7 months, and 6–0 months before birth) and prenatal periods. Error bars represent 95% confidence intervals. The dashed reference line represents an odds ratio of 1.0, or no increased odds.
Discussion
Using Swedish population data, we found a novel and robust association between preconception maternal stress and risk for infant mortality. Preconception stress also predicted increased risk for preterm birth and SGA status (Catov et al., 2011; Khashan et al., 2009), and these adverse birth outcomes partially mediated the association between preconception stress and infant mortality. We did not identify associations between prenatal stress and infant mortality. These counterintuitive findings may be explained by an examination of potential mechanisms and future exploration of cause of death. Little is known, however, about potential mechanisms that may act during the preconception period. The mediating role of gestational age and SGA status suggests that preconception nutritional depletion may play a role in the association between preconception stress and infant mortality (Berghella et al., 2010; Catov et al., 2011). Congenital malformations and sudden infant death syndrome (SIDS), both of which are leading causes of infant mortality (Altman et al., 2012; Mathews & MacDorman, 2008), may be more strongly influenced by preconception and early prenatal insults than by events later in pregnancy (Hansen, Lou, & Olsen, 2000). SIDS may be associated with brainstem-based control of autonomic functioning of breathing (Duncan et al., 2010) through the serotonergic and noradrenergic neuronal systems (Klintschar & Heimbold, 2012), which develop early in organogenesis.
Stress due to bereavement following the death of a loved one affects the survivor’s psychological, cognitive, behavioral, endocrine, physiological-somatic, and immunological characteristics and can do so for months after the death (Stroebe et al., 2007). Etiological epigenetic mechanisms also may translate the effects of maternal preconception stress to the future fetus by affecting nutritional or hormonal maternal systems (Berghella et al., 2010; Catov et al., 2011; Witt et al., 2012) and thereby affecting the mother’s preparedness for pregnancy and affecting the fetus during the vulnerable period of organogenesis (Chmurzynska, 2010; Kelly & Trasler, 2004; Van den Bergh, Mulder, Mennes, & Glover, 2005).
Sensitivity analyses suggested that male offspring were at greater risk for infant mortality than were female offspring (Glover & Hill, 2012; Mathews & MacDorman, 2008), although statistical power may have affected our ability to detect a similar association in females. A male-specific mechanism affecting the likelihood of SIDS has been identified and may act during early organogenesis (Klintschar & Heimbold, 2012). The risk associated with preconception stress remained elevated in offspring of mothers with an average interpregnancy interval (12–35 months), which is notable because both short (Smits & Essed, 2001) and long (Stephansson, Dickman, & Cnattingius, 2003) interpregnancy intervals are associated with infant mortality. The association also was present when we included only mothers who had experienced the death of a parent or maternal sibling only (Cleiren, Diekstra, Kerkhof, & van der Wal, 1994), which helps to rule out alternative explanations involving factors such as family mortality risk or cascading stressors from a previous child’s death. The association also appeared to be specific to the period just before conception (see Fig. 1).
Our sample was large (covering births over a span of 35 years), and we controlled for a breadth of statistical covariates and used a precise and reasonably random indicator of stress (Rutter, 2007). Despite these strengths, future research must take additional methodological and statistical efforts to account for possible selection factors that contribute to both infant mortality and preconception stress exposure (Rutter, 2007). The death of a relative causes stress with a level of intensity that varies by individual and situation. It is possible that the death of a first-degree relative did not induce substantial stress in all mothers and that, in cases of death due to a long-term illness, it may have provided relief (Schulz et al., 2003). In addition, mothers might have experienced unmeasured stressors. Future research would benefit from considering the specific causes of death in infancy.
In agreement with findings from clinical intervention studies (Berghella et al., 2010), the results reported here suggest that preconception care is essential; maternal preconception stress increases the risk for infant mortality and adverse birth outcomes in offspring. Prenatal maternal stress, however, does not appear to influence risk for infant mortality. Our findings suggest that the 6 months immediately prior to preconception may be a sensitive developmental period with ramifications for the likelihood of offspring infant mortality. Longitudinal studies of women experiencing severe stress before conception might provide important knowledge about the mechanisms of infant mortality.
Footnotes
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Funding
This study was supported by National Institute of Mental Health Grant MH094011, National Institute of Child Health and Human Development Grant HD061817, the Swedish Research Council, and the Swedish Prison and Probation Services.