
Abstract
Emotion regulation is central to psychological health. For instance, cognitive reappraisal (reframing an emotional situation) is generally an adaptive emotion-regulation strategy (i.e., it is associated with increased psychological health). However, a person-by-situation approach suggests that the adaptiveness of different emotion-regulation strategies depends on the context in which they are used. Specifically, reappraisal may be adaptive when stressors are uncontrollable (when the person can regulate only the self) but maladaptive when stressors can be controlled (when the person can change the situation). To test this prediction, we measured cognitive-reappraisal ability, the severity of recent life stressors, stressor controllability, and level of depression in 170 participants. For participants with uncontrollable stress, higher cognitive-reappraisal ability was associated with lower levels of depression. In contrast, for participants with controllable stress, higher cognitive-reappraisal ability was associated with greater levels of depression. These findings support a theoretical model in which particular emotion-regulation strategies are not adaptive or maladaptive per se; rather, their adaptiveness depends on the context.
Emotion regulation is critically involved in psychological health (Aldao, Nolen-Hoeksema, & Schweizer, 2010; Kring & Werner, 2004). Given this involvement, much attention has been focused on determining which emotion-regulation strategies are adaptive. Although many different strategies can be used to regulate emotions (for reviews, see Gross & Thompson, 2007; Koole, 2009), past research has identified cognitive reappraisal as a strategy that seems to be particularly adaptive (i.e., associated with better psychological health; Aldao et al., 2010; Gross & John, 2003; Webb, Miles, & Sheeran, 2012). Cognitive reappraisal involves reframing one’s thoughts about a stimulus to change its emotional impact (Gross, 1998). In recent work, we showed that cognitive-reappraisal ability (CRA) is associated with better psychological health and is particularly important for psychological health in people with high levels of life stress (Troy, Wilhelm, Shallcross, & Mauss, 2010).
A conclusion that we and others have drawn from this research is that cognitive reappraisal is an adaptive emotion-regulation strategy (Gross & John, 2003; Troy & Mauss, 2011). However, multiple theoretical accounts suggest that this conclusion is incomplete, because no psychological process is inherently and always adaptive (Grant & Schwartz, 2011; Lazarus, 1993; Mischel, 1968). In particular, interactionist accounts emphasize the importance of both the person and the situation in predicting outcomes (Bowers, 1973; Endler, 1975; Mischel & Shoda, 1995). According to this view, the adaptiveness of an emotion-regulation strategy should depend on the specific context in which it is used (Cheng, 2001; Westphal, Seivert, & Bonanno, 2010). These considerations raise the question of whether contextual variables moderate the adaptiveness of CRA.
Past research on emotion regulation has not examined this important question. However, theoretical considerations from the literature on coping suggest that the controllability of a situation (i.e., the degree to which a person can influence the situation’s outcome; Heth & Somer, 2002) may be a critical moderator of the adaptiveness of one’s regulatory efforts. For example, when encountering relatively uncontrollable stressors (e.g., a loved one’s illness), attempting to change the situation (i.e., problem-focused coping) may be futile. It has been suggested that the use of emotion-focused coping allows people to change the only thing they can control in this context: their emotions (Folkman, 1984; Lazarus, 1993). Cognitive reappraisal can be considered a type of emotion-focused coping. Thus, CRA may be highly adaptive in the context of uncontrollable stress. Conversely, when encountering relatively controllable stressors (e.g., potential job loss as a result of poor performance), it may be better for people to change the situation using problem-focused coping (e.g., putting in longer hours at work), rather than changing their emotions (Lazarus, 1993). Thus, CRA may be less useful or even maladaptive in the context of controllable stress.
In the present study, we first sought to replicate our past research, in which we showed CRA to be particularly adaptive in high-stress contexts (Troy et al., 2010). We also sought to extend this research by examining the idea that the type of stress encountered matters. To test this hypothesis, we recruited a community sample of people who had recently experienced a stressful life event. We predicted a three-way interaction in which CRA would be adaptive (i.e., associated with increased psychological health) in highly stressful contexts that were relatively uncontrollable, whereas CRA would be maladaptive (i.e., associated with decreased psychological health) in highly stressful contexts that were relatively controllable. Given our previous results (Troy et al., 2010), we did not expect CRA to be associated with psychological health at low levels of life stress.
The present study had three notable strengths. First, because increased depression is a common and often debilitating consequence of stress exposure (Tennant, 2002), and because previous research has shown that CRA is associated with less depression in high-stress contexts (Troy et al., 2010), we chose to use level of depression as a particularly relevant index of psychological health. Second, because self-reports of CRA may be subject to demand characteristics, we used a previously validated laboratory challenge to measure CRA (Troy et al., 2010). This laboratory challenge provided two indices of CRA, one based on change in self-reported emotion, and another based on change in skin-conductance activity, a measure of sympathetic nervous system activity. Third, previous research has shown that estimates of personal control can be inaccurate (Langer, 1975). Thus, we obtained an independent measure of stress controllability using an independent, secondary sample of participants who provided controllability ratings for the stressors that primary participants had experienced.
Method
Participants
Primary sample
Because we had specific predictions about stress severity, and to increase variance in level of depression, we required all participants to have experienced a stressful life event in the 8 weeks preceding study recruitment. One hundred ninety-two participants completed the laboratory session. Of these participants, 19 experienced no sadness during the baseline sadness induction and were therefore excluded from all analyses. Of the remaining 173 participants, skin-conductance activity data were unavailable for an additional 17 because of technical difficulties. This left 173 participants for analyses involving CRA quantified using change in self-reported sadness and 156 participants for analyses involving CRA quantified using change in skin-conductance activity. Values more than three times the interquartile range were excluded from all analyses. This left 170 participants for analyses involving self-reported sadness and 147 participants for analyses involving skin-conductance activity (see Table 1 for demographic information). 1
Demographic Characteristics for Participants in the Primary and Secondary Samples

Note: Because of different numbers of missing values, Ns differ across the comparisons. For family income, 18 participants in the primary sample indicated “don’t know,” and their data were therefore considered missing values.
Education was rated on a scale from 1 (less than 7th grade) to 7 (graduate training). bFamily income was rated on a scale from 1 (≤ $10,000 per year) to 7 (≥ $100,000 per year).
Secondary sample
We recruited a second sample (N = 22) that was matched with the primary sample on sex, age, race, education, and family income (see Table 1). These participants provided independent stress-controllability ratings for each of the stressors that the participants in the primary sample experienced.
Procedure
Primary participants completed the study in two stages. First, they completed an online survey assessing demographics and psychosocial characteristics (e.g., level of depression and life stress). Approximately 1 week later (M = 8.37 days, SD = 7.02), participants came to a laboratory session in which CRA was measured using a validated and standardized laboratory challenge (Troy et al., 2010). In this procedure, participants watched a 2-min neutral film clip to induce a baseline level of neutral emotion across participants. Next, participants were presented with three sad film clips (2 min each) pretested to evoke moderate amounts of sadness. The order of the films was the same for all participants.
Participants were asked to watch the first sad film clip (the baseline sad clip) carefully. To avoid confounding emotion-regulation effects with habituation, regression to the mean, or effects specific to one film clip, we randomly assigned participants to use cognitive reappraisal during either the second or the third sad film clip. Using the same instructions as in previous research, we asked participants to think about the situation they were watching “in a more positive light” (Troy et al., 2010). For more information about the film clips, see the Supplemental Material available online.
After each film clip, participants used a 9-point Likert scale to rate the greatest amount of sadness they experienced while watching that clip (higher numbers indicated greater sadness). Sadness ratings were z-scored for each film so that scores could be compared with skin-conductance-activity scores across participants who received reappraisal instructions during different film clips. Change scores were then calculated by subtracting sadness ratings for the reappraised film from sadness ratings for the baseline sad film. These scores were interpreted as a measure of participants’ CRA: A higher score indicated greater CRA (M = 0.3, SD = 1.0). As in previous research (Troy et al., 2010), we excluded participants who reported feeling no sadness during the baseline sad film clip (n = 19). 2
While the participants viewed the film clips, skin-conductance-activity measurements were acquired at a sampling rate of 1000 Hz using a constant-voltage device that passed 0.5 V between Beckman electrodes (Beckman Coulter, Brea, CA) in an electrolyte of sodium chloride in Unibase (Biopac Systems, Inc., Goleta, CA). The electrodes were attached to the palmar surface of the proximal phalanges of the first and second fingers of the nondominant hand. Skin-conductance responses were defined as change in skin-conductance activity from a zero-slope baseline exceeding 0.2 µS (Venables & Christie, 1980). Artifacts were excluded using customized analysis software (Wilhelm, Grossman, & Roth, 1999). The primary measure of skin-conductance activity was the number of skin-conductance responses per minute for each film clip for each participant. Previous research has found that increases in sadness are associated with decreases in skin-conductance activity (Kreibig, Wilhelm, Roth, & Gross, 2007; Mauss, Levenson, McCarter, Wilhelm, & Gross, 2005). On the basis of these findings, we calculated change scores by converting the skin-conductance-response rate for each film clip to z scores, and then we subtracted skin-conductance-response rate during the baseline sad film from skin-conductance-response rate during the reappraised film for each participant. Higher scores denoted greater CRA (M = −0.07, SD = 0.7).
Participants in the secondary sample completed an online questionnaire assessing demographics, and they also provided stress controllability ratings for each of the stressors that participants in the primary sample had experienced.
Measures
Stress severity
The cumulative negative impact of stressful life events experienced by primary participants in the 18 months before the experiment was measured with the Life Experiences Survey, a 46-item measure that indexes a range of potentially stressful life events (Sarason, Johnson, & Siegel, 1978). Participants rated the impact of life events on a scale from −3 (extremely negative impact) to 3 (extremely positive impact). Because we were interested only in negative life events, all negative impact ratings for each participant were summed and then multiplied by −1 so that a higher score indicated greater stress severity. Participants in the present sample reported a wide range of stress-impact levels and were, on average, highly stressed (M = 15.9, SD = 10.5, range = 1–46).
Stress controllability
The secondary sample was also given the Life Experiences Survey, but participants were asked to rate how controllable each stressor would be if it occurred in their own lives. Ratings were made on a scale from 1 (very uncontrollable) to 4 (very controllable). Across the 22 raters, the average intraclass correlation coefficient (averaged across all 46 stressors using a two-way mixed-effects model) was .97, F(34, 714) = 30.63, p < .001, which indicates a high degree of consistency across raters.
We calculated a controllability rating for each item by averaging the ratings across all 22 raters, and we calculated composite controllability scores for the primary sample by averaging the controllability ratings across all negative stressors that the primary participants had experienced in the past 18 months (M = 2.8, SD = 0.4). Thus, each participant in the primary sample received a controllability score that indicated the average estimated amount of control he or she was expected to have had over negative stressors that occurred in the 18 months preceding the study, as rated by the secondary participants. For example, a hypothetical participant who experienced a highly uncontrollable event (a score of 1) and a somewhat controllable event (a score of 2) in the past 18 months would receive an overall stress controllability score of 1.5.
Depression level
Current level of depression was measured in the primary sample using the Beck Depression Inventory (Beck & Steer, 1984), a self-report measure consisting of 21 items. Ratings on this measure are made on a scale from 0 to 3, with higher scores indicating greater depression. One question pertaining to suicidal thoughts was not included in the present study because of concerns expressed by the institutional review board at the University of Denver. In the present sample, reliability on the remaining 20 items was high (α = .93).
CRA
CRA was indexed as described in the Procedure section using change in self-reported sadness (CRA-sadness) and change in skin-conductance-response rate (CRA-skin conductance). Mean scores on CRA-sadness were 0.3 (SD = 1.0), and mean scores on CRA-skin conductance were −0.07 (SD = 0.7).
Emotional reactivity
The CRA task was also used to measure emotional reactivity by quantifying any change in sadness that occurred between viewing the neutral film clip and viewing the sadness baseline clip. It was important to measure emotional reactivity separately from CRA to ensure that the measure of CRA was not confounded with participants’ reactivity to the sad films. To parallel the two indices of CRA, we calculated two indices of reactivity: change in self-reported sadness (M = 0.2, SD = 1.3) and change in skin-conductance-response rate (M = −.002, SD = .61).
Results
Primary analyses
CRA-sadness
A multiple regression was conducted with level of depression as the dependent variable and CRA-sadness, stress severity, stress controllability, and all two- and three-way interactions among them as the independent variables. In the multiple-regression models, all main effects were mean-centered before we calculated interaction terms. Results are shown in Table 2. There were main effects of CRA-sadness and stress severity, a two-way interaction between CRA-sadness and stress controllability (see Additional Analyses and Fig. S1 in the Supplemental Material), and a three-way interaction between CRA-sadness, stress severity, and stress controllability. To examine the three-way interaction, we plotted values 1 standard deviation above and below the mean for each predictor according to the procedures outlined by Aiken and West (1991; see Fig. 1).
Results of Regression Analyses Predicting Level of Depression From Stress Severity, Stress Controllability, and Two Measures of Cognitive-Reappraisal Ability (CRA)
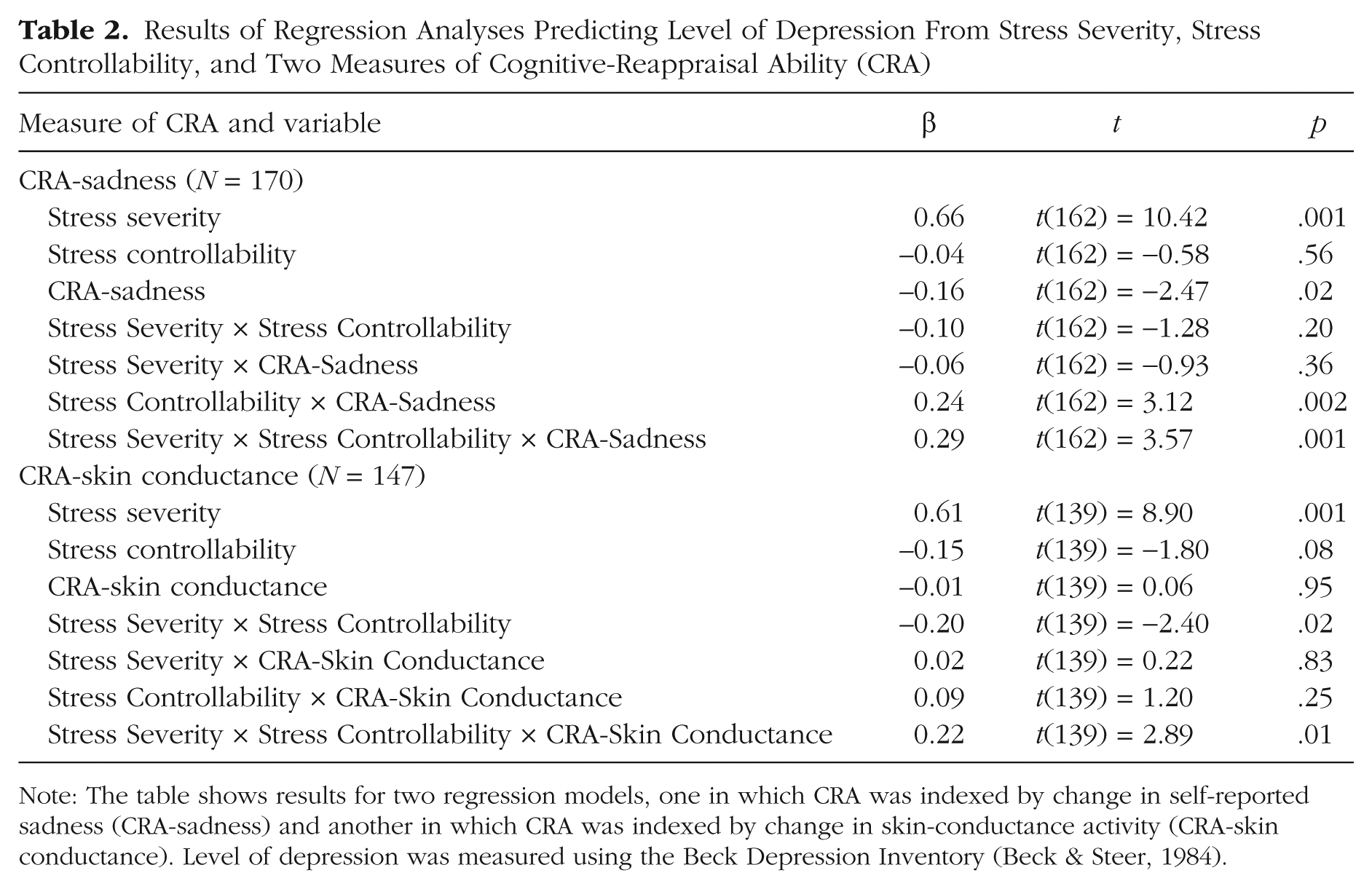
Note: The table shows results for two regression models, one in which CRA was indexed by change in self-reported sadness (CRA-sadness) and another in which CRA was indexed by change in skin-conductance activity (CRA-skinconductance). Level of depression was measured using the Beck Depression Inventory (Beck & Steer, 1984).

Mean level of depression as a function of stress severity and change in self-reported sadness during cognitive reappraisal (CRA-sadness). Results are shown separately for participants who experienced situations in which stress controllability was independently rated as (a) low and (b) high. High and low values in stress controllability, CRA-sadness, and stress severity refer to values 1 standard deviation above and below the mean, respectively. Level of depression was measured using a modified version of the Beck Depression Inventory (BDI; Beck & Steer, 1984); higher scores indicate greater depression. Error bars show standard errors of the mean.
In the context of low stress controllability, simple-slopes analyses revealed that the effect of stress was significantly greater than zero for participants with low levels of CRA-sadness, β = 1.1, t(162) = 5.8, p < .01, and for participants with high levels of CRA-sadness, β = 0.4, t(162) = 2.8, p < .01. However, the effect of CRA-sadness on level of depression in the context of low stress controllability and low stress severity was not significantly different from zero, β = −0.03, t(162) = −0.3, p = .79, whereas the effect of CRA-sadness in the context of low stress controllability and high stress severity was significantly less than zero, β = −0.8, t(162) = −3.6, p < .01. Thus, in the context of low stress controllability and high stress severity, greater CRA-sadness was associated with significantly lower levels of depression.
In the context of high stress controllability, the effect of stress was significantly greater than zero for participants with low levels of CRA-sadness, β = 0.3, t(162) = 2.6, p = .01, and for participants with high levels of CRA-sadness, β = 0.8, t(162) = 5.7, p < .01. However, the effect of CRA-sadness in the context of high stress controllability and low stress severity was not significantly different from zero, β = −0.2, t(162) = −1.5, p = .14, whereas the effect of CRA-sadness in the context of high stress controllability and high stress severity was significantly different from zero, β = 0.3, t(162) = 2.6, p = .01. This positive slope indicates that in the context of high stress controllability and high stress severity, greater CRA-sadness was associated with significantly higher levels of depression.
CRA-skin conductance
The same multiple regression model that was used to analyze CRA-sadness was run again, this time with change in skin-conductance activity as the index of CRA. Results are shown in Table 2. There was a main effect of stress severity, a two-way interaction between stress controllability and stress severity, and a three-way interaction among stress controllability, stress severity, and CRA-skin conductance. The three-way interaction is shown in Figure 2.

Mean level of depression as a function of stress severity and change in skin-conductance activity during cognitive reappraisal (CRA-skin conductance). Results are shown separately for participants who experienced situations in which stress controllability was independently rated as (a) low and (b) high. High and low values in stress controllability, CRA-skin conductance, and stress severity refer to values 1 standard deviation above and below the mean, respectively. Level of depression was measured using a modified version of the Beck Depression Inventory (BDI; Beck & Steer, 1984); higher scores indicate greater depression. Error bars show standard errors of the mean.
In the context of low stress controllability, the effect of stress on level of depression was significantly greater than zero for participants with low levels of CRA-skin conductance, β = 1.2, t(139) = 5.9, p < .01, and for participants with high levels of CRA-skin conductance, β = 0.5, t(139) = 3.07, p < .01. The effect of CRA-skin conductance on level of depression in the context of low stress controllability and low stress severity was not significantly different from zero, β = 0.2, t(139) = 1.2, p = .23, whereas the effect of CRA-skin conductance in the context of low stress controllability and high stress severity was significantly less than zero, β = −0.4, t(139) = −2.0, p = .04. Thus, this pattern is similar to that found for CRA-sadness: In the context of low stress controllability and high stress severity, greater CRA-skin conductance was associated with lower levels of depression.
In the context of high stress controllability, the effect of stress on level of depression was not significantly different from zero for participants with low levels of CRA-skin conductance, β = 0.04, t(139) = 0.24, p = .81, whereas the effect of stress was significantly greater than zero for participants with high levels of CRA-skin conductance, β = 0.7, t(139) = 4.7, p < .01. In the context of high stress controllability and low stress severity, the effect of CRA-skin conductance was not significantly different from zero, β = −0.2, t(139) = −1.6, p = .10, whereas in the context of high stress controllability and high stress severity, the effect of CRA-skin conductance was significantly greater than zero, β = 0.5, t(139) = 2.4, p = .02. Thus, in the context of high stress controllability and high stress severity, greater CRA-skin conductance was associated with significantly greater levels of depression. 3
Secondary analyses
Although level of depression was our primary outcome of interest, we also measured two additional indices of psychological health—psychological well-being and symptoms of anxiety. Results relating to those two outcomes are presented in the Additional Analyses section in the Supplemental Material.
Discussion
The present research adds to the existing body of literature in which it is suggested that emotion regulation is critically important for psychological health, particularly during times of high stress (Aldao, et al., 2010; Gross & John, 2003; Troy & Mauss, 2011). Much of this research has been guided by the question of what types of emotion regulation are adaptive (Troy & Mauss, 2011). We argue now that this question is incomplete because few, if any, psychological processes are inherently and always adaptive (Bonanno, Papa, Lalande, Westphal, & Coifman, 2004; Cheng, 2001; Lazarus, 1993). Thus, the present study extends past theorizing by highlighting that the degree to which emotion regulation is adaptive depends on the type of stress. Specifically, high CRA was associated with less depression and increased well-being in the context of uncontrollable stress. When stress was relatively controllable, however, higher CRA was associated with decreased psychological health. These findings support a novel theoretical model in which the effects of emotion-regulation strategies depend on the context in which they are used.
It may be surprising that in contexts in which a stressor was more controllable, CRA was not simply unrelated but was negatively related to psychological health. However, this makes sense if viewed from a functionalist perspective (Nesse, 1990; Parrott, 2002; Schwarz, 1990). For example, negative emotions can be adaptive because they motivate people to take action to solve a problem. People who decrease their negative emotions may no longer be motivated to take action, which leads to negative outcomes in situations in which action is needed (e.g., controllable stressors). Thus, it may be that people with high CRA over-rely on reappraisal as a regulatory strategy and use it inflexibly and in inappropriate contexts (cf. Bonanno et al., 2004). Future research is needed to fully examine this hypothesis.
Our findings also have implications for understanding how emotion regulation contributes to risk or resilience in the face of stress. In stressful conditions in which little can be done to change the situation, effective emotion regulation should be a particularly adaptive way to arm oneself against negative outcomes (Cheng, 2001; Folkman, 1984). When the situation is changeable, however, emotion regulation may be maladaptive. These results support a person-by-situation approach to understanding the effects of emotion regulation on psychological health.
The present results also have important implications for understanding what constitutes adaptive emotion regulation. In addition to examining which emotion-regulation strategy is being used and how effectively a person can use a particular strategy, the context in which the strategy is used must be considered. The present findings support flexibility models in which adaptive forms of emotion regulation involve the flexible deployment of different regulatory strategies depending on situational demands (Bonanno et al., 2004; Cheng, 2001; Kashdan & Rottenberg, 2010), and psychological dysfunction may be characterized by deficits in flexibility (Bonanno & Burton, in press; Rottenberg, Gross, & Gotlib, 2005).
The present results also have important clinical implications. Some clinical interventions aim to strengthen CRA (Campbell-Sills & Barlow, 2007; Mennin, 2004). Our study suggests that interventions should focus both on strengthening regulatory ability and learning to use reappraisal in context-appropriate ways. Specifically, clinicians could include psychoeducational components in their interventions to help clients understand when reappraisal would be a helpful strategy to use (i.e., in situations in which stress is uncontrollable). In addition, clinicians could help clients identify strategies besides reappraisal that could be used when stress is controllable, such as behavioral approaches (e.g., active problem solving) or other emotion-regulation strategies (e.g., acceptance). Further research is needed to identify which strategies are adaptive when used in the context of controllable stress.
It is important to note that the vast majority of research has shown a positive relationship between reappraisal and psychological health (Aldao et al., 2010; Gross & John, 2003). The present study is one of the first to suggest that reappraisal may lead to worse psychological-health outcomes in certain contexts. What might account for this apparent contradiction? Meta-analyses of cognitive reappraisal have shown small to medium effect sizes for predicting outcomes (Aldao et al., 2010; Webb et al., 2012). These relatively modest effect sizes suggest that although reappraisal is an adaptive process in many contexts, it is not adaptive in all contexts. Thus, rather than contradicting previous findings, the present results add to them in important ways.
The literature on coping has commonly contrasted emotion-focused coping (whereby cognitive reappraisal may be considered a subtype) with problem-focused coping (Folkman & Lazarus, 1980). However, these two broad categories of coping are not mutually exclusive. Indeed, Folkman and Lazarus (1980) found that people report using both types of coping when facing stressors. Thus, it may be best to consider the degree of emotion-focused coping relative to the degree of problem-focused coping. However, it still seems likely that if people can successfully reduce their experience of negative emotions, they are less likely to engage in more active coping strategies. In future research, it will be important to measure both emotion-focused and problem-focused strategies to test this hypothesis.
The present research focused on an important type of emotion regulation (reappraisal) and an important aspect of stress (controllability). However, to continue testing the general hypothesis that the adaptiveness of emotion regulation depends on the context, future research should examine other types of emotion regulation (e.g., suppression) and other contexts that may moderate the effects of emotion regulation (e.g., stressor predictability).
Finally, the cross-sectional nature of the current investigation prevents us from drawing strong causal conclusions about the effects of CRA on psychological health. It could be argued that current level of depression, life stress, and controllable stress influence levels of CRA, rather than the other way around. We theorize that CRA functions as a fairly stable characteristic that can protect against stress-related increases in level of depression when used in the appropriate context. Thus, we do not conceptualize CRA as simply a function of one’s present context, stress levels, or level of depression. Indeed, the current study provides empirical support for this notion: The three-way interaction among level of depression, stress severity, and stress controllability did not predict either index of CRA. In addition, there were no significant two-way interactions among level of depression, stress severity, or stress controllability, which suggests that CRA is not simply a side effect of these constructs. Thus, it seems most parsimonious to conclude that CRA interacts with life stress and stress controllability to influence level of depression.
Conclusion
Given the importance of emotion regulation for psychological health and the many ways emotions can be regulated, researchers have asked which types of emotion-regulation strategies are adaptive. The present research suggests that this question is incomplete. In addition to considering specific types of emotion regulation, researchers should also consider the context to understand how emotion regulation relates to psychological health. Indeed, results from the present study support a person-by-situation account of emotion regulation in which the adaptiveness of specific emotion-regulation strategies depends on the context in which they are used.
Footnotes
Acknowledgements
We thank Daniel McIntosh, Kateri McRae, Stephen Shirk, and the Emotion Regulation Lab at the University of Denver for feedback on a previous version of the manuscript.
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Funding
This research was supported by the National Institute on Aging (Grant 1R21-AG031967 to I. B. Mauss) and by a Dissertation Fellowship Award from the University of Denver (to A. S. Troy).
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.