
Abstract
Adequate perception of bodily sensations is essential to protect health. However, misinterpretation of signals from within the body is common and can be fatal, for example, in asthma or cardiovascular disease. We suggest that placing interoceptive stimuli into interoceptive categories (e.g., the category of symptoms vs. the category of benign sensations) leads to perceptual generalization effects that may underlie misinterpretation. In two studies, we presented stimuli inducing respiratory effort (respiratory loads) either organized into categories or located on a continuous dimension. We found pervasive effects of categorization on magnitude estimations, affective stimulus evaluations, stimulus recognition, and breathing behavior. These findings indicate the need for broadening perspectives on interoception to include basal processes of stimulus organization, in order for interoceptive bias to be understood. The results are relevant to a wide range of interoception-related phenomena, from emotion to symptom perception.
Keywords
Health is not “une vie dans le silence des organes” (“life in the silence of organs”; Valéry, 1942, p. 112). In disease and in health, individuals are continuously exposed to a wide range of signals from the body, such as breathing sensations, heart rate, and gastrointestinal sensations. Early and accurate detection of signs of pathology is of vital importance for health. However, misperception and misinterpretation of bodily sensations are common in chronic and acute conditions (e.g., stroke, myocardial infarction, asthma), sometimes with life-threatening consequences (e.g., Banzett, Dempsey, O’Donnell, & Wamboldt, 2000; Mandelzweig, Goldbourt, Boyko, & Tanne, 2006).
Bias in interoception has typically been conceived as resulting from (motivated) inattention or hypervigilance to bodily sensations and from erroneous illness beliefs that result in bodily sensations being interpreted as indicating greater safety or danger than they actually do (Petersen, van den Berg, Janssens, & Van den Bergh, 2011). However, we assume that more fundamental perceptual processes underlie misinterpretation. As is the case for perception of stimuli outside the body (exteroception), perception of stimuli originating inside the body (interoception) can be organized by representing sensations as groups of stimuli (e.g., symptom categories) or on continuous dimensions (e.g., breathing effort; Petersen, Orth, & Ritz, 2008). Categorization is usually based on the assumption that members of the same group are sufficiently similar to be treated the same and sufficiently different from members of other groups to be treated differently from them. Assigning a sensation, for example, to either the category “asthma symptoms” or the category “benign respiratory sensations” may start a cascade of top-down processes that modulate the very perception of the stimulus (Petersen et al., 2011), whereas not assigning a sensation to a category (i.e., dimensional representation) may reduce such perceptual bias.
Little is known about effects of categorization on interoception. However, categorization effects have received extensive attention in other fields of psychology. Grouping of stimuli (i.e., gestalt formation; Wertheimer, 1912/1961) plays a crucial role in the perceptual process (for a review on traditional and “neo-Gestalt psychology,” see Wagemans et al., 2012) because categories provide “maximum information with least cognitive effort” (Rosch, 1978/1999, p. 191). They allow one to make inferences about unobserved features of a stimulus on the basis of class membership (Lewandowsky, Kalish, & Ngang, 2002) and to gain expertise in recognizing and differentiating stimuli (Gillebert, Op de Beeck, Panis, & Wagemans, 2009). However, the simplification that contributes to smooth perception can easily turn into overgeneralization. Even if category members are no more similar to each other than to non-category members (i.e., even if categorization does not relate to similarities and differences between stimuli in a meaningful way), categorization can lead to an increase in perceived similarity within classes (assimilation), an increase in perceived differences between classes (accentuation), or both. These effects occur in visual perception (Corneille, Klein, Lambert, & Judd, 2002; Goldstone, 1995; Tajfel & Wilkes, 1963), perception of syllables (Campbell, 1956), and haptic evaluation of objects (Gaißert, Buelthoff, & Wallraven, 2011). Thus, merely knowing that stimuli are located within categories (without seeing the stimuli grouped in a category or gestalt) is sufficient to change perception (see also Gillebert et al., 2009).
However, results from exteroception may not generalize to interoception in a straightforward way. Interoception differs from exteroception in important ways. Interoception is private, and the distal stimulus (located inside the body) cannot be shared with other individuals. As a consequence of this privacy, there is no objective standard for perceiving, for example, too much or too little breathlessness or pain in response to a specific stimulation. Furthermore, the onset and location of bodily sensations are often ambiguous, whereas this is not the case for most exteroceptive stimuli. It seems reasonable to assume that lack of objective standards and increased ambiguity should increase categorization effects for interoceptive stimuli given that high uncertainty increases the influence of categorical information (Corneille et al., 2002). This assumption, however, has not been tested despite the fact that a categorical approach in diagnostics (e.g., asking for symptom categories) is more common than a dimensional approach.
Another fundamental difference between exteroceptive stimuli used in prior research and interoceptive stimuli is that interoceptive stimuli are tightly connected to emotions and physiology (Dunn et al., 2010). Internal sensations may easily act as alarm signals, such that they become affectively loaded and highly self-relevant. Indeed, positive or negative affect elicited by interoceptive sensations might serve as a basis for categorizing these sensations into affective categories (Bruner, Goodnow, & Austin, 1956; Niedenthal, Halberstadt, & Innes-Ker, 1999). However, the vast majority of research on the role of categorization in perception has focused on exteroceptive stimuli that are low in complexity, low in self-relevance, and of neutral valence (e.g., line drawings; Corneille et al., 2002; Gillebert et al., 2009; Tajfel & Wilkes, 1963). Whether affect and self-relevance of interoceptive stimuli might interfere with basic cognitive processes and possibly influence categorization bias has received little attention. Moreover, the self-relevant affective component of categorizing an interoceptive stimulus may induce motivational tendencies that may be reflected in behavior toward that stimulus. Thus, using interoceptive stimuli makes it possible to study fundamental processes in interoception and also provides an opportunity for directly testing the effect of categorization on affect and behavior.
The studies presented here tested effects of categorical structure on the perception of breathing. We chose breathing as our focal interoceptive domain because the feeling of breathing effort can be induced in different degrees of intensity on a continuous dimension, while avoiding the more aversive experience of, for example, pain. In Study 1, we tested the effect of categorization on basic magnitude estimation and on explicit affective evaluation of respiratory stimuli assigned to categories labeled A and B. In the Supplemental Material available online, we present a study that also addressed the effect of categorization using an implicit measure of affective evaluation; this additional study confirmed and extended results of Study 1. In Study 2, we tested whether categorization of respiratory stimuli changes stimulus recognition and behavior involved in coping with those stimuli.
Study 1
Participants
Sixty-two participants (20 male, 42 female) without known respiratory disease were randomly assigned to an experimental group (n = 32; mean age = 23.7 years, SD = 4.4) and a control group (n = 30; mean age = 22.1 years, SD = 2.4). Participants were invited via online platforms and flyers. All participants gave informed consent at the start of the experiment. The protocol was approved by the local ethics committee.
Instruments
We manipulated breathing effort via respiratory load, switching valves (Threshold IMT, Respironics Inc., Parsippany, New Jersey) in a breathing circuit. We used six loads that successively increased inspiratory resistance by a constant factor of 0.4 (7, 10, 14, 20, 28, and 40 cm H2O). The lowest load was well above the average perceptual threshold (Petersen & Ritz, 2010). According to Weber’s law, which also applies to respiratory stimuli (Wiley & Zechman, 1966), higher background noise increases perceptual thresholds. In the case of breathing through respiratory loads, this noise is internal airway resistance (Rint), which can be increased by chronic (asthma) or acute (cold) conditions. We measured and controlled statistically for Rint (MicroRint, CareFusion Ltd., Chatham, United Kingdom). Participants rated the intensity and unpleasantness of respiratory sensations using visual analog scales from 1 through 100, which were presented on a computer screen. Participants also responded to questions on their age, gender, and history of respiratory disease.
Experimental protocol
Participants completed three blocks of trials (Table 1). We presented each load six times per block, for a total of 108 trials. Participants in both groups were asked to breathe in and out two times while each load was presented, before rating the intensity and unpleasantness of the respiratory stimulus. In Block I, the six loads were presented to both groups in ascending order (i.e., from the smallest to the highest load) without category information (the same six loads were presented in the same order six times). In Block II, loads were again presented in ascending order. This time, participants in the experimental condition were instructed that the three smaller loads belonged to Category A and the three larger loads belonged to Category B. Loads were labeled A1, A2, A3, B1, B2, and B3, and the appropriate label was presented on-screen while each load was attached to the breathing circuit. Apart from this categorical information, Block II was identical to Block I for participants in the experimental group. Participants in the control group did not receive information on categories, so for this group, Block II was identical to Block I. In Block III, we used the online program Research Randomizer (Urbaniak & Plous, 2011) to create a random presentation order for both groups; the six loads were presented in six separate random-presentation blocks. Participants in the experimental group were reminded that the three smaller loads belonged to Category A and the three larger loads belonged to Category B (no category information was provided to the control group), but in contrast to Block II, labels were not presented on-screen.
Labeling and Order of Presentation of the Respiratory Loads in Study 1
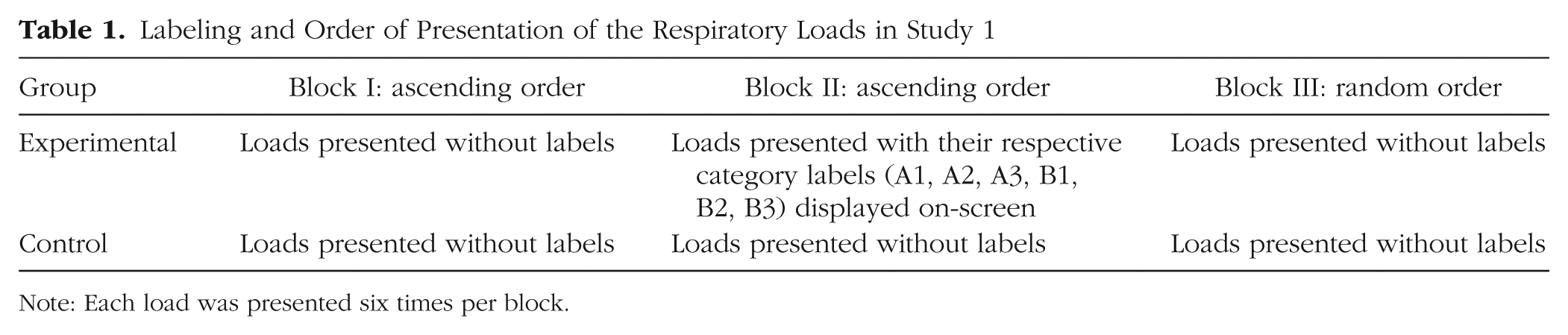
Note: Each load was presented six times per block.
Data analysis
We used SPSS 18 software for all analyses. We calculated the percentage of perceived increase in intensity and unpleasantness between adjacent loads (i.e., between loads of neighboring magnitude). We then calculated (separately for each participant and experimental block) three aggregated measures of perceived differences: differences within Category A (mean perceived increase between adjacent loads in A), differences within Category B (mean perceived increase between adjacent loads in B), and between-category differences (mean perceived increase from the largest load in A, or the third load in the control condition, to the smallest load in B, or the fourth load in the control condition).
For each of the three blocks, we examined perceived differences in reported intensity and unpleasantness using repeated measures analyses of variance (ANOVAs) with difference measure (differences within A, differences between A and B, differences within B) as a within-subjects variable and group (experimental, control) as a between-subjects variable. For the experimental group, we tested for assimilation effects by testing whether perceived differences within categories were smaller in Block II and Block III compared with Block I (in which the category labels were not used). Furthermore, for this group, we also tested whether perceived differences within categories were smaller than perceived differences between categories in Blocks II and III. For post hoc tests of assimilation relative to Block I (no categorization), we used paired-sample t tests. As a post hoc test for smaller differences within categories than between categories, we tested (for each block separately) a quadratic within-subjects contrast. We included Rint as a covariate and calculated η p 2 as our measure of effect size.
Results
Figure 1 summarizes the mean perceived differences for each group in Blocks II and III. We found that organizing the loads into categories had a significant effect on both intensity and unpleasantness ratings, but only when the loads were presented in random order. That is, for the experimental group in Block III (random order), but not in Block II (ascending order) or in Block I (no category information), within-class differences were smaller than between-class differences, as indicated by significant within-subjects quadratic contrasts—intensity: F(1, 30) = 20.45, p < .001, η p 2 = .405; unpleasantness: F(1, 30) = 14.33, p = .001, η p 2 = .323. Furthermore, in the experimental group, assimilation effects in Block III relative to Blocks I and II were significant; that is, differences within A and within B were lower in Block III than in Blocks I and II (all ps < .023). The experimental group’s perceived between-class differences in Block III were not greater than actual differences (40% increases in resistance) or than this group’s perceived between-class differences in Block I or II; also, perceived between-class differences in Block III were not greater for the experimental group than for the control group. Thus, accentuation was found only when we compared between-category differences with within-category differences within the same block.

Results from Study 1: differences in reported (a) intensity and (b) unpleasantness of breathing (perceived increases between adjacent loads) as a function of difference measure (within Category A, between Categories A and B, within Category B), group (experimental, control) and block (II, III). Also shown is the percentage of actual difference between respiratory loads. Results for Block I (respiratory loads presented in ascending order, no categorization information given to either group) are omitted for the sake of clarity; the values for that block did not differ significantly from the corresponding values in Block II. Error bars represent standard errors of the mean.
We did not find a Difference Measure × Group interaction for perceived differences in intensity or unpleasantness, both Fs(2, 57) < 0.585, ps > .560. This lack of an interaction was due to perceived differences being smaller for higher compared with lower loads regardless of group and block. Main effects of difference measure in Blocks I through III (separate analysis for each block) were significant for both differences in perceived intensity, all Fs(2, 59) > 5.14, ps < .007, η p 2s > .080, and differences in unpleasantness, all Fs(2, 59) > 2.53, ps < .090, η p 2s > .041. The fact that higher loads were perceived to be more similar than lower loads in all three blocks obscured group differences in assimilation effects. However, in Block III (random-order condition), the control and experimental groups differed significantly in perceived differences in intensity and unpleasantness within Category A, p = .036 and p = .047, respectively. In accordance with our hypothesis, the quadratic contrasts for intensity and unpleasantness ratings were significant only in the experimental group (see the previous paragraph), and not in the control group—intensity: F(1, 28) = 0.017, p = .898; unpleasantness: F(1, 28) = 0.676, p = .418.
However, when we examined raw values (i.e., absolute magnitude of intensity and unpleasantness ratings, rather than percentage differences between adjacent loads), we found a significant interaction of the within-subjects factor (loads in Category A vs. loads in Category B) and group in Block III—intensity: F(1, 60) = 6.76, p = .012, η p 2 = .101; unpleasantness: F(1, 60) = 6.12, p = .016, η p 2 = .093—but again not in Block I or II (Fs < 1). In Block III, the absolute values of the experimental groups’ ratings were significantly higher for Category A and significantly lower for Category B, compared with the control group’s ratings. In short, ratings of load magnitude and unpleasantness were more moderate when the loads were categorized with the neutral category labels A and B.
When Rint was introduced as a covariate in the model of perceived differences, it interacted significantly with difference measure for Block III ratings, but only in the experimental group—intensity: F(1, 30) = 16.67, p < .001, η p 2 = .357; unpleasantness: F(2, 29) = 11.88, p = .002, η p 2 = .284 (control group: both Fs < 1). To illustrate these findings, we calculated mean assimilation scores for Block III by subtracting mean within-category differences from mean between-category differences. In the experimental group, higher Rint was related to lower assimilation effects for both intensity, r(32) = −.598, p < .001, and unpleasantness, r(32) = −.533, p < .001 (control group: p > .158 for both relationships).
Discussion
Grouping stimuli in categories affected self-reports of intensity and unpleasantness of breathing, but only if loads were presented in random order. These results confirm prior research showing that higher uncertainty about a stimulus (as in the case of random order) is associated with greater influence of category information (Corneille et al., 2002). They extend results from prior research in showing that categorization (when stimuli are presented in random order) also increases similarities in affective evaluation. However, we did not find that between-category differences were larger than absolute differences between loads. Accentuation (larger between- than within-category differences) was significant only within Block III in the experimental group. In Study 1.2 (reported in the Supplemental Material), we confirmed results of Study 1, finding categorization effects on ratings of intensity and unpleasantness only when stimuli were presented in random order. Note that in that study, we also found categorization effects using an alternative, implicit measure of affective stimulus evaluation.
The category labels were neutral and did not provide anchor points that would induce either overperception or underperception, as would have been the case, for example, with meaningful labels such as “sensations” and “symptoms.” The fact that we found reduction in extremity of ratings (i.e., more moderate intensity and unpleasantness ratings in Block III in the experimental condition than in the control condition) using this neutral categorization highlights that bias induced by categorization (increased perceived similarity) is not necessarily related to overperception or underperception as such. The direction of deviation in interoceptive accuracy may strongly depend on whether or not category labels serve as meaningful information.
The impact of airway resistance on the results is interesting. Physiological background noise should not be related to a reanchoring of self-reports, but it affects perception on a sensory level. Our study design did not allow us to test whether effects of categorization were merely post hoc effects of reanchoring according to the category prototype or mean. In Study 2, we used measures that were not dependent on self-report of magnitude estimates and unpleasantness. Instead, we measured perceived similarity by calculating confusion frequencies between loads (Shepard, 1987) and assessed breathing behavior (inspiratory flow, i.e., liters of air inhaled per second). Flow rates are directly related to respiratory effort (e.g., breathing through a straw gets harder the faster one tries to suck air through the straw). Adjusting flow can be interpreted as part of coping with a respiratory load.
Study 2
Participants
Participants were 30 individuals (10 male, 20 female; mean age = 19.4 years, SD = 1.7) with no self-reported history of respiratory diseases. Participants were invited via flyers and online platforms. All participants gave written informed consent. The protocol was approved by the local ethics committee.
Instruments
We used an electronic device that manipulates external breathing resistance and measures inspiratory flow (liters per second) breath by breath (Breathelink K5, POWERbreathe International Ltd., Warwick, United Kingdom). We presented eight different loads, four categorized in A (6, 9, 12, and 16 cm H2O) and four in B (21, 28, 37, and 49 cm H2O). We assessed positive and negative affect with the Positive and Negative Affect Schedule (PANAS; Watson, Clark, & Tellegen, 1988).
Experimental protocol
At the start of the respiratory task, participants were informed that the loads were categorized in A (four smaller loads) and B (four larger loads). In Block I, we presented each load four times, for two breaths each time, and measured inspiratory flow breath by breath. Before each presentation, participants saw the label of the load (A1, A2, A3, A4, B1, B2, B3, or B4) on the computer screen; they were asked to memorize their breathing experiences and the label. In Block II, loads were presented in random order; each load was presented four times, again for two breaths. In this block, participants had to identify the loads and to type in the label of each load. After this task, participants completed the PANAS and demographic questions.
Data analysis
As mentioned, participants took two breaths per load presentation. We calculated mean inspiratory flow for each load presentation in Block I and then calculated mean differences in flow between adjacent loads within A, within B, and between A and B. Furthermore, we calculated mean confusion frequencies for Block II. The perceived similarity of two stimuli can be indexed by the frequency with which they evoke the same response (i.e., the extent to which they are confused), relative to the frequency of correct identifications (Shepard, 1987). This measure of generalization, gij, is calculated as [(pij × pji)/(pii × pjj)]1/2, with pii and pjj being the likelihood of correctly identifying stimuli i and j, and pij and pji being the likelihood of misidentifying j as i and vice versa.
Results
Categorization changed breathing behavior and led to assimilation in respiratory flow in Block I (Fig. 2). Differences within categories were significantly smaller than differences between categories. Both the quadratic contrast, F(1, 29) = 8.49, p = .007, η p 2 = .226, and the main effect of difference measure, F(2, 28) = 7.17, p = .002, η p 2 = .198, were significant.
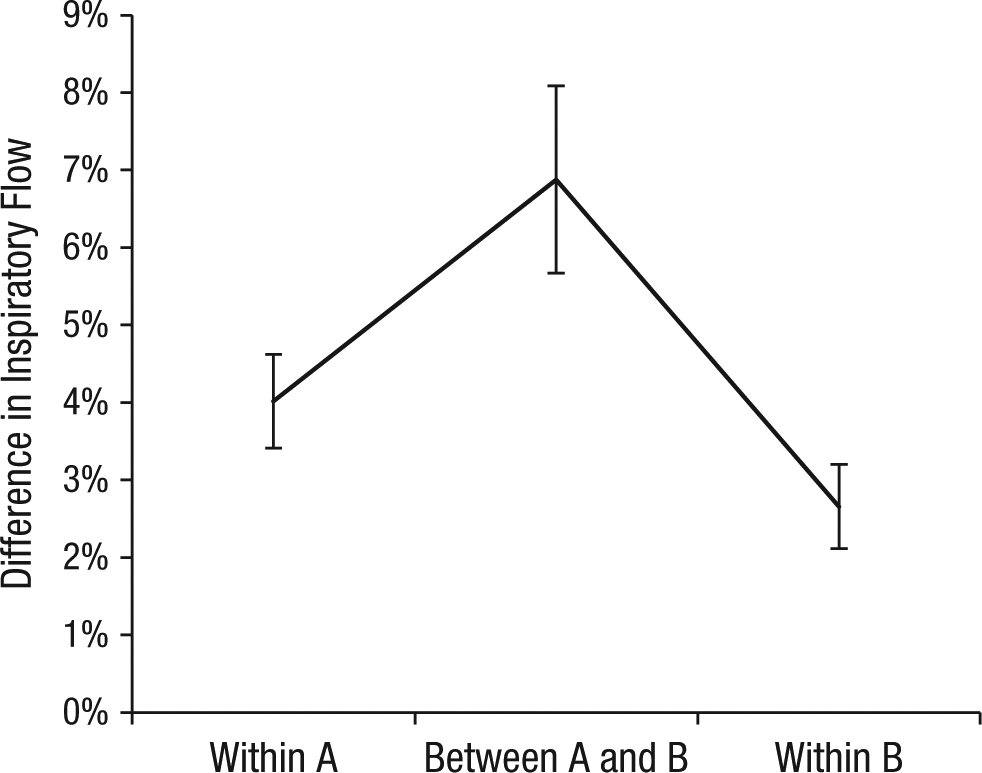
Results from Study 2: differences in inspiratory flow within Category A, between Categories A and B, and within Category B in Block I. Error bars represent standard errors of the mean.
In Block II, loads were confused more often within than between categories (Fig. 3). Both the quadratic contrast, F(1, 29) = 65.52, p < .001, η p 2 = .693, and the main effect of difference measure, F(2, 28) = 43.94, p < .001, η p 2 = .602, were significant.
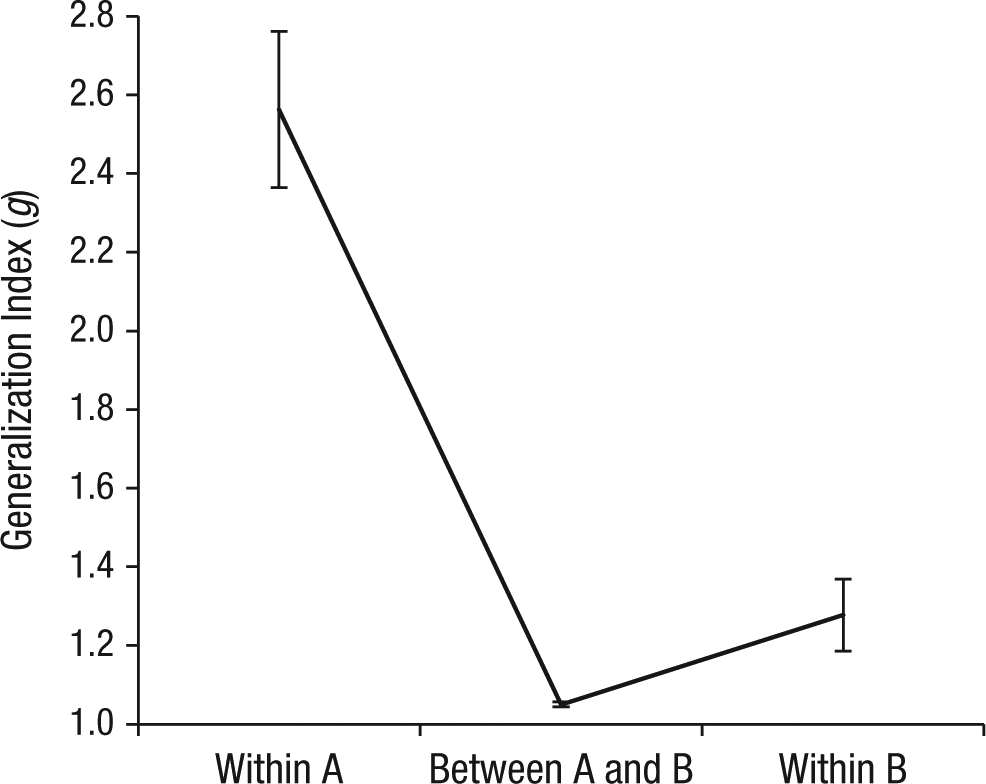
Results from Study 2: confusion frequencies within Category A, between Categories A and B, and within Category B in Block II. Higher values indicate greater perceived similarity. Error bars represent standard errors of the mean.
Neither positive nor negative affect had an impact on either inspiratory flow or confusion frequencies, Fs < 1.
General Discussion
Categorization of interoceptive sensations changes perception of their magnitude and unpleasantness, stimulus recognition, and coping behavior directed toward these stimuli. These effects occur even when categorization is based on abstract labels (“A” and “B”), representing “less intense” and “more intense” stimuli. However, we found a significant quadratic effect indicating that perceived within-category similarity was greater than perceived between-category similarity only when the constant increase between stimuli was obscured by random presentation (Study 1). These results mirror findings that uncertainty about stimuli increases the value of category information and, thus, categorization effects (Corneille et al., 2002).
Our findings regarding confusion frequencies and inspiratory flow suggest that categorization effects in interoception (and probably also in exteroception) do not arise merely from post hoc changes in self-report. Voluntary adjustment of confusion frequencies or inspiratory flow to reflect category membership of a stimulus is (although not impossible) exceedingly more difficult than voluntary adjustment of self-report to make ratings match a category label. Our results suggest that categorization effects are more likely to be found when there is greater uncertainty about stimulus magnitude (or other stimulus characteristics) and when the response to the stimulus reflects more automatic, less voluntarily controlled processes. Research focusing on self-reported stimulus evaluation alone might underestimate the impact of categorization on perception, stimulus-related affect, and behavior.
An important finding of Studies 1 and 2 (and of Study 1.2 in the Supplemental Material) is that categorization had an impact on affective stimulus evaluation and behavior directed toward stimuli. In classical social cognition studies on categorization effects, stimuli were mostly of neutral valence (lines, colors, or shapes; e.g., Corneille et al., 2002; Goldstone, 1995; Tajfel & Wilkes, 1963), so affective evaluation and behavioral measures were of little relevance. Nevertheless, these classical experiments are used as a theoretical basis for more applied research on prejudices, that is, affectively loaded psychological phenomena that can have relevant behavioral consequences. The studies here contribute to closing a gap in research and theory development, demonstrating that grouping stimuli within the same category leads individuals not only to think more similarly about those stimuli, but also to have more similar affective reactions to them, and to approach them in a more similar way.
The results also suggest that categorization is important for emotion perception. Most signs of increased physiological activation (heartbeat, visceral sensations, etc.) are unspecific and similar for positive and negative emotions. Strong bodily sensations experienced, for example, during a roller-coaster ride can be interpreted as either signs of intense enjoyment or signs of the start of an asthma attack, depending on how much a person likes to take such a ride (Rietveld & van Beest, 2007). Ambiguity of interoceptive sensations in emotion perception requires categorization for the individual to select coping strategies. At the same time, it opens the door for increasing similarity of affective interpretation and potentially more similar emotions. If, as our results suggest, categorization affects affective evaluation and emotions, perceptual reorganization of stimuli so that they are perceived less as category members and more as individual stimuli, or stimuli along a dimension, might reduce bias in affective evaluation as much as recategorization and decategorization have been shown to reduce bias in other fields of psychology, for example, intergroup bias (Gaertner, Mann, Murrell, & Dovidio, 1989).
Categorization effects in interoception are highly relevant to the clinical context. Priming categories such as “symptoms” rather than “sensations,” as is done in most medical consultations and by most diagnostic instruments, may alter perception of the intensity of one’s internal sensations, as well as one’s affective evaluation and behavioral coping. Emphasizing the dimensional character of sensations by asking, for example, how much breathing has changed on an effort dimension (rather than asking whether symptoms are present) can increase bottom-up processing and reduce bias, with beneficial outcomes for diagnostics and disease management.
Limitations
We note that our experiments have several limitations. First, our participants did not have a history of respiratory illness, and results obtained with healthy individuals do not necessarily generalize to patients who have detailed and complex preexisting knowledge structures about their illness. Second, results obtained with a breathing manipulation may not generalize to all interoceptive sensations.
In addition, we used symmetrical categories (as did, e.g., Tajfel & Wilkes, 1963), but effects might increase if participants are allowed to choose cutoff points or if categories are asymmetrical. Furthermore, we did not use more than two categories, because we could not increase load strength infinitely and wanted to keep loads distinguishable. Moreover, future studies should explore different measures of assimilation (see, e.g., Park & Judd, 1990). We found significant effects of explicitly measured positive affect on implicit evaluation of respiratory loads in Study 1.2 (Supplemental Material), but further research in which higher levels of positive and negative affect are induced will be necessary to explore the interaction of categorization with affect.
Conclusion
The organization of bodily sensations into categories can bias interoception. Categorization as a perceptual organization process in interoception precedes and underlies affective evaluation, cognitive elaboration, and coping behavior.
Footnotes
Acknowledgements
The authors thank Anne Koehler and Elina Schuermann for their help in data acquisition and data preparation for the analysis of inspiratory flow in Study 2.
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Funding
This research was funded by the Research Foundation Flanders.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.