
Abstract
Socioemotional risks associated with nonparental care have been debated for decades, and research findings continue to be mixed. Yet few studies have been able to test the causal hypothesis that earlier, more extensive, and longer durations of nonmaternal care lead to more problems. To examine the consequences of age of entry into nonparental care for childhood aggression, we used prospective longitudinal data from Norway, where month of birth partly determines age of entry into Early Childhood Education and Care (ECEC) centers. In this sample of 939 children followed from ages 6 months through 4 years, ECEC teachers reported the children’s aggression when they were 2, 3, and 4 years old. We found some evidence that age of entry into ECEC predicted aggression at age 2, albeit modestly and not robustly. Between the ages of 2 and 4 years, the effect of age of entry on aggression faded to negligible levels. The implications for psychological science and policy are discussed.
In the 1980s, following increases in women’s labor-force participation, U.S. researchers began reporting associations between the amount of time infants spent in nonmaternal-care settings and behavioral dysregulation, noting that extended time in these settings was associated with later elevations in externalizing problems, such as aggression (Belsky, 1986; Clarke-Stewart & Fein, 1983). Positioned at an intersection between psychological science and public concern, this topic has continued to generate interest and debate for three decades. Prospective longitudinal work in the United States that began in the 1990s indicated that large amounts of time in any form of nonmaternal care (including paternal care) during the first 4.5 years of life might bring accumulating risks for aggression and other externalizing problems (e.g., NICHD Early Child Care Research Network, 2003). Yet debate has been fueled by the fact that across research samples and methods, studies have varied in whether they have found an association between time in early child care and externalizing problems, as well as in the magnitude of this association when it has been found (Huston, Bobbit, & Bentley, 2015; McCartney et al., 2010). Moreover, it has remained unclear why early child care might pose risks to children’s socioemotional development; although some researchers have hypothesized that disrupted parent-child attachment or social learning of maladaptive behaviors may be the cause, results have not proven entirely consistent with either attachment or social learning theory (for reviews, see Belsky, 2001; Huston et al., 2015; McCartney et al., 2010).
Recently, this field of study has grown in two critical directions: First, it is now international rather than U.S.-centric (Lekhal, 2012; Love et al., 2003; Zachrisson, Dearing, Lekhal, & Toppelberg, 2013). Second, researchers have given increasing attention to the causal hypothesis that earlier, more extensive, and longer durations of nonmaternal care lead to more problems (Crosby, Dowsett, Gennetian, & Huston, 2010; Jaffee, Van Hulle, & Rodgers, 2011; McCartney et al., 2010). Even with these advances, however, results have remained less than uniform, indicating that moderate risk, no risk, or even protection from risk is associated with early nonparental care. Within this empirical context, we examined links between age of entry into nonparental Early Childhood Education and Care (ECEC) centers and later aggression in Norway, where month of birth partly determines age of entry into ECEC.
Early, Extensive, and Continuous Nonparental Care: A Perfect Storm?
Among wealthy nations, the United States provides what is arguably a peculiar policy context (e.g., its unusually conservative parental leave policy), but evidence on the association between nonparental care and behavioral dysregulation from outside the United States is also mixed (Zachrisson et al., 2013). This heterogeneity in findings may partly reflect heterogeneity in methods. Belsky (2001) persuasively argued that early child care likely poses a developmental risk for aggression and other problems only when three necessary conditions create a perfect storm: The nonparental care must begin in infancy, involve a large number of hours, and last continuously throughout the first few years of life. Still, conceptual, theoretical, and operational questions remain with regard to how early is too early, how extensive is too extensive, and how continuous is too continuous.
There is some support for linear dosage effects, particularly regarding age of entry. For example, Loeb, Bridges, Bassok, Fuller, and Rumberger (2007) demonstrated linear increases in risk for behavior problems: Children who entered child-care centers before they were 1 year of age were at greater risk than those who entered between the ages of 1 and 2, who in turn were at greater risk than those who entered between the ages of 2 and 3, who were at greater risk than those who entered between the ages 3 and 4. In short, risk decreased at a steady rate as children’s age of entry increased, but there was still some developmental risk associated with entering care even as late as in the 4th year of life. Yet, as Loeb et al. acknowledged, because they controlled only for observed covariates (as is the case in most work on this topic), their estimates were susceptible to bias caused by unobserved selection forces.
Addressing Selection Effects
All extant studies on whether child-care quantity is associated with socioemotional risk have employed nonrandomized designs, and there is reason for concern that unobserved factors influencing time in child care (i.e., selection effects) may have biased the observed associations. Selection is a problem if influences on both parents’ child-care choices and children’s socioemotional development—including characteristics of parents, children, and their communities—are unmeasured or measured poorly. Attempting to address selection bias, researchers have typically used statistical techniques to hold a variety of measured family and child characteristics constant, but it is highly questionable as to whether this method can adequately account for unobserved sources of bias (Duncan, Magnuson, & Ludwig, 2004). Consequently, design strategies that isolate the exogenous effects of time spent in nonparental care are needed (McCartney et al., 2010; Zachrisson et al., 2013).
Age of Entry Into ECEC in Norway
In the early 2000s, Norway set a goal of universal access to publicly subsidized and quality-regulated ECEC centers from age 1 (Ellingsæter, 2014). Today, the majority of 1- to 2-year-old Norwegian children (> 80%) are in ECEC settings (Statistics Norway, 2015b). Moreover, although there is variability in the number of hours that children attend these centers, children generally attend them continuously up until they enter school. However, children rarely enter ECEC prior to 9 months of age because parental leave policy provides 10 months of leave at full pay or 12 months of leave at 80% pay.
At the time the children in our sample entered ECEC (2007–2010), municipalities were required to coordinate enrollment into all centers using one primary enrollment date per year (Ministry of Education, 2007a). That enrollment date generally mirrored school enrollment practices: Most municipalities, including those from which we sampled, offered care to children who were at least 1 year old by the enrollment date of either August 1 or August 15 (Ministry of Education, 2007b). Remaining free slots were allocated via a waiting list that gave first priority to children who were 11 months old by the enrollment date and second priority to those who were 10 months old by that date. Most infants who were not 10 months of age by August enrolled in ECEC in August of the following year.
The Present Study
We argue that the effect of birth month on enrollment into ECEC can be exploited to partial out variability in age of entry unrelated to parental choice or other selection forces and, in turn, estimate the effects of this variability on the development of aggression. Specifically, we examined the association between age of entry into continuous ECEC and the development of aggression across ages 2, 3, and 4 years in a Norwegian sample of children (n = 939), allowing estimates to vary by the number of hours children attended ECEC. We first used conventional covariate adjustments and propensity-score weighting to handle selection effects and then exploited the effects of birth month on age of entry by means of instrumental-variable (IV) analysis. We examined both the similarities and the differences in results across these methodological approaches, paying special attention to the sociopolitical context in which this study was conducted.
Method
Sample and procedure
We use data from the Behavior Outlook Norwegian Developmental Study (BONDS), a longitudinal study of 1,159 children (559 girls) from five municipalities in southeast Norway. The BONDS is approved by the Regional Committee for Medical and Health Research Ethics and the Norwegian Data Inspectorate, and all parents provided informed written consent. Families were informed about the project in 2006 through 2008 when they took their 5-month-old children for medical examinations at child health clinics in the following five municipalities in the counties of Telemark and Buskerud: Bamble, Porsgrunn, Skien, Tinn, and Drammen. (In Norway, care at child health clinics is free, and use of these clinics is almost universal; the 5-month visit is part of standard practice in Norway.) The inclusion criteria were that the child be 5 months of age and at least one parent be able to participate without a translator. Families were informed about the study by the nurse and provided contact information if they agreed to be contacted. The families of 1,931 eligible children received initial information; 1,465 (76%) agreed to be contacted, and 1,159 (79%, or 60% of those originally informed) eventually agreed to participate. The sample fairly well resembles the eligible families (for complete details, see Nærde, Janson, & Ogden, 2014). Two families later withdrew from the study and had all their data deleted. Thus, the final sample size was 1,157.
In the present study, we focused our analyses on the 939 children who entered ECEC by 24 months of age. We were concerned primarily with this group for two reasons. First, it was reasonable to assume that a child’s birth month most strongly determined age of entry into ECEC within the first 2 years of the child’s life, given that parental leave ended at either 10 or 12 months and publicly funded care began at 12 months; all children had the opportunity to enroll by at least their second birthday. Second, our first measure of the children’s aggression was completed when they were 24 months old; there was no reason to expect that variation in age of entry after 24 months would have relevance (beyond associated selection effects) to aggression at that time. Nonetheless, as we describe later, we reestimated all models with the full sample of 1,157 children as a robustness check.
Trained assistants conducted interviews with parents in the lab (or in the home setting, if parents preferred) when the children were ages 6 months and 1, 2, 3, and 4 years. Each interview included a computerized questionnaire completed by the parent. Both parents were invited to participate in the 6-month interview, whereas fathers were primarily targeted in the 1- and 3-year interviews, and mothers in the 2- and 4-year interviews. Also, questionnaires were sent to the ECEC teachers when the children were ages 2, 3, and 4 years, with the request that the teacher who knew a given child the best complete the questionnaire for that child. The teacher questionnaires were completed either on a computer or on paper, as the teacher preferred. In addition, three brief telephone interviews (3 months apart) were conducted each year with parents in between the in-person interviews until the children were 3 years old.
Measures
Aggression
Teachers reported on the children’s physical aggression by rating eight items when the children were 2, 3, and 4 years old: “hits other children,” “hits adults,” “pushes someone to get his/her way,” “pulls hair,” “pinches someone,” “throws things at others,” “kicks someone,” and “bites someone.” Responses were made on a frequency scale ranging from 1 (never/not in the past year) to 7 (3 times daily or more), αs = .85, .87, and .89 at ages 2, 3, and 4, respectively. At the same three times, parents rated an almost identical set of seven items, with “hits other children” dropped and “hits adults” replaced by “hits you,” αs = .77, .78, and .79, at ages 2, 3, and 4, respectively. Item scores were averaged to create the indicators of child aggression.
Age of entry into ECEC
At every contact point (in-person and telephone interviews), parents were asked, “Where is the child during the daytime?” Response categories were “home with Mom or Dad,” “home with other family member,” “home with a nanny,” “with a nanny,” “in family day care,” and “in center care.” If the response was “in center care,” the follow-up question was, “On which date did the child enter center care?” If the child had not entered center care, the parent was asked whether entry was planned and, if so, when. This question was asked at every contact point until an exact starting date was obtained following the child’s entrance into ECEC. Additional telephone interviews were scheduled immediately prior to and immediately after the age at which the parent expected the child to enter ECEC, so that the exact age of entry could be confirmed. Each child’s birth date was registered at initial recruitment.
Although not drawn to be nationally representative, the sample for this study provides a recent estimate of the percentage of children in ECEC by the age of 12 months, which was about 27% in this sample. Unfortunately, national data on age of entry are not readily available. Approximately 4% of all 0- to 12-month-olds are in ECEC, but this figure considerably underestimates the total percentage of children who enter by age 1; some of the 0- to 10-month-old children not in ECEC at a given date will enter ECEC before they are 1 year old. At the time the data for this study were collected, ECEC coverage for children younger than 1 year and for 1- to 2-year-olds was slightly higher, on average, in the five municipalities from which our participants were sampled than in the nation as a whole (4.2% vs. 5.8% for children less than 1 year old and 74.98% vs. 76.6% for 1- to 2-year-olds; Statistics Norway, 2015b).
Covariates
When the children were 6 months old, the mothers reported their own birth country; they were then categorized as Norwegian, Western (born in Europe, North America, or Oceania), or non-Western (born in Asia, Africa, Latin America, or Turkey). The mothers also reported the family composition (i.e., single- or two-parent family), whether a sibling (full sibling, half sibling, or biologically unrelated sibling) similar in age to the child in the study (i.e., age difference up to 5 years) was present in the household, whether they received any social benefits (unemployment benefits, disability pension, or other social allowances, which were mutually exclusive with employment), and the number of years of education they had completed. An index of poor housing was created by summing mothers’ reports of whether they were dissatisfied with their housing (yes = 1, no = 0), lived in a one-bedroom or smaller home (yes = 1, no = 0), and did not own their home (yes = 1, no = 0; home ownership is normative in Norway). Furthermore, the mothers’ distress (i.e., symptoms of depression and anxiety) was indexed by their mean score on the 13-item version of the Hopkins Symptom Check List (Strand, Dalgard, Tambs, & Rognerud, 2003), α = .89. The mothers’ current employment status (employed vs. unemployed) was drawn from parent interviews when the children were 2, 3, and 4 years old; mothers were considered to be unemployed if they indicated that they were students, on parental leave, at home full time, unemployed, or on social benefits (e.g., disability pension). Dummy variables were created for birth cohort (i.e., whether the child was born in 2006, 2007, or 2008; the latter was omitted as the reference category) and for site (i.e., the municipality; Drammen was the omitted reference).
Parents provided data for child variables as part of the 6-month interview. They reported their child’s gender and whether the birth was preterm. Temperament was indexed by the mother’s ratings on two scales from Rothbart’s (1981) Infant Behavior Questionnaire-Revised, which was administered by computer with a modified 3-point response format (1 = most of the time, 2 = sometimes, 3 = rarely or never). Mean scores were calculated separately for Activity Level and Distress to Limitations, αs = .71 and .77, respectively.
Data for a number of ECEC covariates were also collected when the children were 2, 3, and 4 years old. The number of hours they spent in center care per week was assessed at these three in-person interviews by asking, “How many hours a week does the child spend outside of the home” (the interviewer was instructed to include only time in child care, with a nanny, in family day care, etc.). ECEC group size and behavior issues in the group were assessed in the questionnaires sent to the ECEC centers at these times. Teachers were asked, “How large is the group that can be considered the child’s group?” and “Are there any children in the group displaying so much challenging behavior that it is a problem for other children?” For the latter question, teachers were told not to count the target child, and examples of challenging behavior were provided. Response categories were 0 (no), 1 (yes, one child), and 2 (yes, two or more children); responses were recoded into two dummy variables, and classrooms with no children with challenging behaviors were the reference group. The teacher completing each questionnaire was asked, “For how many months have you been in daily contact with this child?” This covariate was included to account for potential report bias due to degree of familiarity with the child or staff turnover.
Statistical analyses
For our primary analyses, we examined teachers’ reports of aggression; we then used parents’ reports as a robustness check. Specifically, we estimated associations between age of entry and the repeated teacher-rated aggression measures using random-effects regression models, with observations nested within children over time. We included both time-invariant predictors (e.g., age of entry) and time-varying predictors (e.g., number of hours in care per week). Consider, for example, the following simplified model: yit = α + βxxi + βzzit + ε it , where yit is the aggression score for the ith child at time t, α is the sample intercept for aggression (allowed to vary randomly across families), xi is the age of entry for the ith child, zit is a time-varying covariate (e.g., hours in care for the ith child at time t), and ε it is the error term. Change in aggression between ages 2 and 4 and the association between age of entry and change in aggression were estimated by including the main effect of child’s age and, in turn, the interaction between age of entry and child’s age. Child’s age was centered such that the main effect of age of entry corresponded to that variable’s average association with aggression across study waves. Within this random-effects framework, we specified models that handled potential selection effects in three different ways. Combined, the results allowed us to consider causality and robustness through a process of triangulation.
Covariate-adjusted estimates
The first model we specified used covariate adjustment for potential selection effects. Specifically, the family, child, ECEC, cohort, and site variables (some time-invariant and others varying with time) listed in Table 1 were included as covariates. In addition, we included birth month as a covariate in this model. If the model is correctly specified, this approach can provide unbiased and consistent estimates, and it is a conventional approach to examining associations between nonparental care and child outcomes. Exclusive reliance on covariate adjustment to remove selection bias, however, rests on the questionable—and difficult to prove—assumption that all relevant variables have, in fact, been included (i.e., the error term is not correlated with the predictor of interest as a result of unobserved factors; Duncan et al., 2004). Yet when correctly specified, covariate-adjusted models provide efficient (precise) estimates.
Descriptive Statistics for the Samples Used in the Covariate-Adjusted, Propensity-Score-Weighted, and Instrumental-Variable Analyses
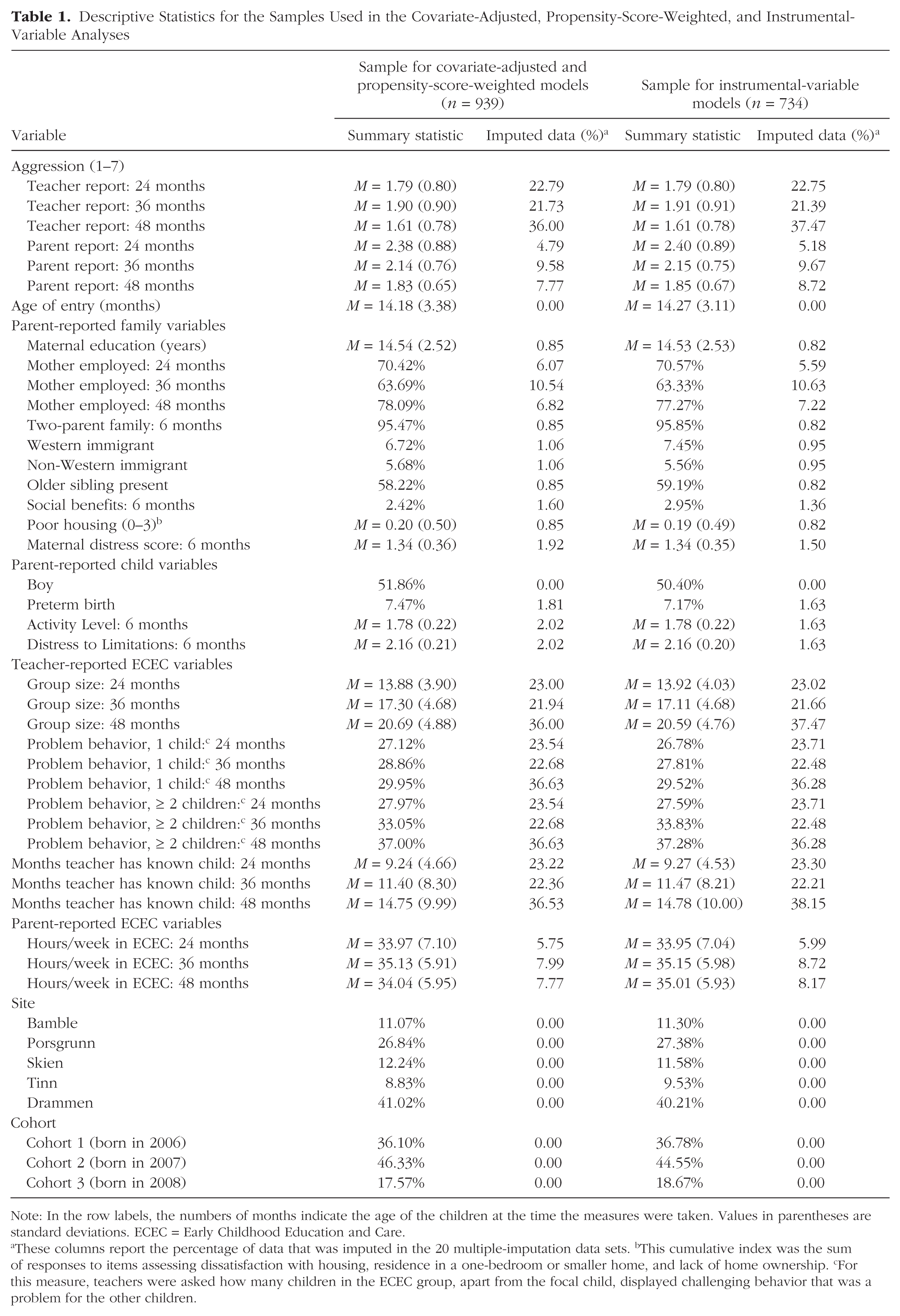
Note: In the row labels, the numbers of months indicate the age of the children at the time the measures were taken. Values in parentheses are standard deviations. ECEC = Early Childhood Education and Care.
These columns report the percentage of data that was imputed in the 20 multiple-imputation data sets. bThis cumulative index was the sum of responses to items assessing dissatisfaction with housing, residence in a one-bedroom or smaller home, and lack of home ownership. cFor this measure, teachers were asked how many children in the ECEC group, apart from the focal child, displayed challenging behavior that was a problem for the other children.
Propensity-score-weighted estimates
The second model we estimated included propensity scores as model weights and as a model covariate. Propensity scores were estimated by dividing age of entry into three categories: prior to 12 months, 12 to 17 months, and 18 to 24 months. Then, using the full covariate set plus birth month, we estimated ordinal logit models predicting these age-of-entry categories; this covariate set explained 15.1% of the variance in age of entry. From the ordinal logit model, each child’s propensity score was calculated as 1/(1 – p), where p was the child’s predicted probability of being in the age-of-entry category that the child was, in fact, observed to be in. Although not a panacea for potential selection bias in nonexperimental data because of the reliance on observed variables (Agodini & Dynarski, 2004), propensity scores can provide a more conservative control for potential selection effects than covariate adjustment (Rosenbaum & Rubin, 1983).
Instrumental-variable (two-stage) estimates
The third model we estimated used birth month as an instrument in a two-stage random-effects specification. In nonexperimental studies, IVs can be used to identify the causal effects of a “treatment” when assignment to the treatment condition is, at least partly, determined by the instrument in a manner that approximates randomization (Angrist, Imbens, & Rubin, 1996; Gennetian, Magnuson, & Morris, 2008). We argue that birth month provided a plausible instrument for isolating random variation in age of entry due to ECEC enrollment policy in Norway.
IV models rest on three key assumptions, one relating to instrument strength and two relating to instrument validity. First, a good instrument should have a strong influence on the likelihood of exposure to the treatment (by convention, this means an F-test statistic ≥ 10). Second, the instrument should be independent of factors that influence the outcome. Third, according to the exclusion restriction, the instrument should influence the outcome only through the treatment. In our model, the endogenous predictor, X (age of entry), and the outcome, Y (aggression), were continuous indicators, so both stages were appropriately conducted using two-stage linear estimators. First, age of entry was regressed on birth month, the instrument:

Second, aggression was regressed on that portion of the variability in the age of entry that was predicted by birth month:

Justification for instrument validity is equal parts empirical evidence and logical argument, and should be considered on a continuum from “less plausible” to “more plausible” (Sovey & Green, 2011). We argue that the policy favoring August enrollments allowed us to identify exogenous variation in age of entry. Note, however, that enrollment policy and practice did not (and does not now) prohibit children under age 1 from entering ECEC, nor did it prohibit children from entering ECEC in months other than August. And it did not require children to enter ECEC at age 1. As a result, birth month was strongly related to age of entry for most months of the year, but not perfectly so, and most modestly in months furthest from August, when parental choice and luck came increasingly into play; for example, parents of a child born in January faced choices such as enrolling the child at age 7 months with 3 to 5 months of paid parental leave remaining, if they were able to obtain an open slot, or enrolling the child at age 19 months, 7 to 9 months after paid leave had ended.
Figure 1 presents the median age of entry for the children in our sample who entered ECEC by 24 months of age. The graph shows that the median age of entry for children who were born from February through October decreased in a linear fashion, which is consistent with the expected effects of the enrollment timing. Children born in February had the highest median age of entry, 18 months (i.e., they were 6 months old when August enrollments occurred, and most parents thus waited a year), and the lowest median age of entry was for children born in September, who were about 11 months old when ECEC slots were allocated. Although fewer than 1 out of 4 children (23.67%) born between February and July enrolled at age 1 or earlier, more than 3 out of 4 children (76.23%) born between August and October enrolled at age 1 or earlier.
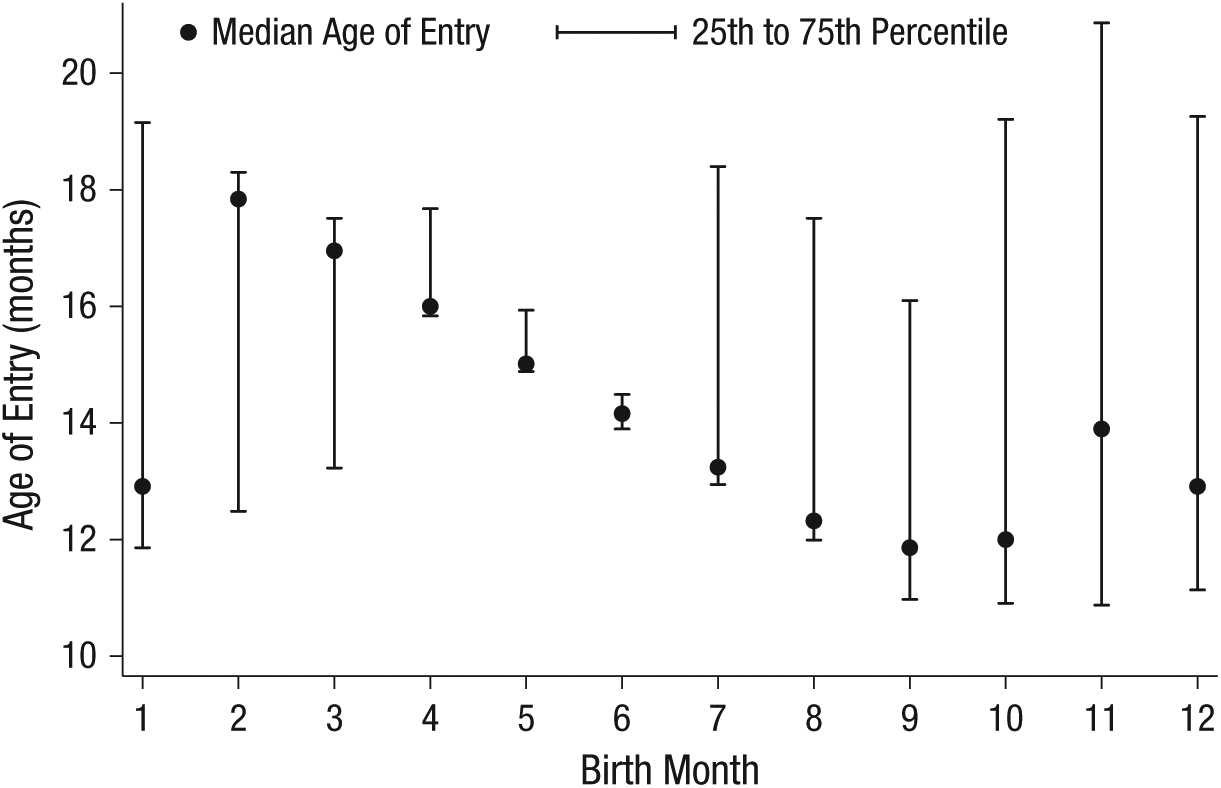
Median age of entry into Early Childhood Education and Care as a function of birth month for those children in the sample who entered center care by 24 months of age.
In contrast, entry times for children born from November through January deviated from the linear trend and were quite variable. For children born in September and October, there was likely a strong incentive to enroll in August (just before age 1) because parental leave would end when the children were 10 or 12 months old, and policy for waiting-list priority increased these children’s odds of obtaining a slot relative to younger children’s odds. From the distribution in Figure 1, it is evident that many of these families did, in fact, find an available slot, although this was truer for children born in September (11-month-olds) than for those born in October (10-month-olds). In turn, for winter births (i.e., November through January), parental choice and luck unrelated to birth month should have come increasingly into play, as indicated by the variation in Figure 1.
Thus, for the IV modeling, we restricted our sample to children born from February through October (n = 734), a time frame that limited the influences of parental choice on age of entry. Compared with using the full sample (F = 13.48) or samples defined by a variety of other possible restrictions (e.g., excluding children born in October through January, F = 27.68), using children born in these 9 months provided the strongest association between the instrument and age of entry (F = 38.13). However, we replicated the results obtained with our IV model when we used the full sample, including November through January births, and, similarly, we replicated the results of our covariate-adjusted and propensity-score-weighted models when we included only the restricted sample of 734 in those models. In both cases, effect sizes for the association between age of entry and aggression were statistically indistinguishable, and nearly identical, at every age.
Given evidence that including interactions between birth month and sampling covariates can be a useful means of improving the precision of IV estimators (Angrist & Krueger, 1992)—assuming that first-stage F values remain sufficiently large (i.e., F ≥ 10; Bound, Jaeger, & Baker, 1995; Staiger & Stock, 1997)—we also included Birth Month × Site, Birth Month × Cohort, and Birth Month × Site × Cohort interactions as instruments in our model. Including these interactions resulted in smaller Stage 2 standard errors compared with including only the main effect of birth cohort or smaller interaction sets, while maintaining an F value of 12.96.
We estimated IV specifications that included (a) the full covariate set in Table 1, (b) the full covariate set in Table 1 plus propensity-score weights, and (c) propensity-score weights and propensity scores (rather than the covariate set) as covariates. The coefficients for age of entry obtained with these specifications were nearly identical; thus, we present results for the third approach, which resulted in the most precise estimates (i.e., the smallest standard errors).
It should be noted that there is an extensive empirical literature reporting studies using birth month (in some cases, season of birth), in a manner parallel to that employed here, as an instrument for the age at which children start school or preschool and, in turn, the number of years of schooling they complete or maternal labor-force participation (Angrist & Krueger, 1992, 2001; Fitzpatrick, 2012; Gelbach, 2002; Puhani & Weber, 2006; Schlotter, 2011; Strøm, 2004). Yet the method is not without potential limitations. Age of entry into school or ECEC, as the case may be, is confounded with dosage (Strøm, 2004), although this is not so problematic for the present study given the literature’s suggestion that it is both early and continuous care that places children at risk. More problematic is the fact that birth month can vary nonrandomly with family markers of risk; for example, children of teenage mothers and of mothers who have not completed high school may be more likely to be born during the winter than in other months, at least in the United States (Buckles & Hungerman, 2013). Our sample, however, included very few of these high-risk families (e.g., fewer than 2% of the mothers were teenagers when their children were born and of those who were, none had given birth during winter months), and we excluded most winter births (November through January) from our IV models. In addition, although policies favoring children born in certain months theoretically could incentivize fertility decisions, data from Statistics Norway (2015a) show that monthly birth rates have been stable from 2000 through 2008 (the birth year of our last cohort), a time period during which national ECEC enrollment for 1- to 2-year-olds increased from 30% to 77%, according to Statistics Norway (2015b; note that we accessed the Statistics Norway data using the “Statbank” tool, which is available online at the cited Web pages).
Nonetheless, we were careful to ensure that covariates were balanced (i.e., not significantly different) across birth months. Of the 38 covariates, all but 2 were balanced across birth months; the exceptions were cohort (children in Cohort 1 were somewhat more likely to be born in later months than were children in the other two cohorts, r = .33) and the 24-month measure of the length of time teachers knew the children (as expected given the effect of birth date on age of entry, teachers reported knowing children born in earlier months somewhat longer, r = −.07). In addition, we found substantively identical results (not presented here) when we limited our sample to children born in May through September, a group for which all covariates except cohort were balanced. As we discuss later, we also examined the exclusion restriction using two variables that were modestly related to age of entry into ECEC (r = −.06 and −.08, respectively), estimating maternal employment and the length of time teachers knew the children as alternative paths from birth month to aggression.
Missing data
The percentage of missing data due to nonresponse was less than 10% across all items, and missing responses were replaced with scale averages. For parent reports, few data were missing (i.e., across all parent-reported variables, < 1%, 5.3%, 7.6%, and 10.0% of data was missing for the 6-, 24-, 36-, and 48-month interviews, respectively). Levels of missing data, however, were higher for teacher-reported variables (21.7%–36.6% of data missing). Using multiple imputation, we computed 20 data sets based on all covariates in Table 1. Results were substantively identical when we used listwise deletion for missing values; we therefore report results from the multiple-imputation analyses only.
Results
Table 1 provides descriptive statistics for all variables. The 939 children (81% of the total sample) who attended ECEC at age 2 constituted our analytic sample. For this group, the number of hours in care per week was stable, on average, from age 2 to 4 (33.97 hr at age 2 and 34.04 hr at age 4). The average within-child standard deviation across ages 2 through 4 was 0.59 hr, very similar to the between-children standard deviation of 0.58 hr during this time.
Primary analyses
Table 2 summarizes results from models using covariate adjustment and propensity scores to handle potential selection effects. Overall, results from these two approaches were very similar. The association between age of entry and average teacher-rated aggression from age 2 to 4 years was negligible in both models; for example, although this association approached statistical significance (p = .09) in the covariate-adjusted model, a 6-month difference in age of entry (i.e., ~1.70 SD) predicted less than a 0.10-SD difference in average aggression. However, the interaction of change in aggression with age of entry was significant. Figure 2 illustrates this interaction, showing change in aggression for children who started ECEC relatively early (1 SD below the mean) and relatively late (1 SD above the mean). Given that the patterns in the two models were nearly identical, we present only the covariate-adjusted estimates in this figure.
Random-Effects Regression Estimates From the Covariate-Adjusted and Propensity-Score-Weighted Models Assessing Associations Between Age of Entry Into Early Childhood Education and Care (ECEC) and Teacher-Rated Aggression From 2 to 4 Years of Age

Note: Standard errors are given in parentheses. All family, child, ECEC, and demographic variables listed in Table 1 were included as covariates in the models.
This variable was centered such that the main effect of age of entry estimated the association between age of entry and average teacher-rated aggression at ages 2 through 4 years.
p < .1. *p < .05. **p < .01.

Predicted marginal means for teacher-rated aggression at 2, 3, and 4 years, for children who entered Early Childhood Education and Care early (i.e., at age 10.80 months, 1 SD below the mean age of entry) and late (i.e., at age 17.97 months, 1 SD above the mean age of entry). Error bars represent 95% confidence intervals.
When the children were 2 years old, those who had entered at earlier ages displayed significantly (p < .05) higher levels of aggression, although these differences were quite small: A 6-month difference in age of entry was associated with less than a 0.18-SD difference in aggression in the covariate-adjusted model and less than a 0.17-SD difference in the propensity-score-weighted model. In addition, aggression levels declined at significantly faster rates for children who had entered ECEC earlier. As a result, for 3-year-olds, age of entry was no longer significantly associated with aggression, and for 4-year-olds, the effect size was zero in both models.
Next, we estimated our IV model. Birth month and its interactions with site and cohort appeared to offer valid instruments, as they were significantly (and moderately) associated with age of entry, F(15, 1000) = 12.96, p < .001, but unrelated to teacher-rated aggression (e.g., effect-size rs for birth month never exceeded .01). In addition, two important findings were evident in the second stage of the analysis (see Table 3). First, the IV model was consistent with the prior models in that age of entry was not significantly associated with average aggression. Second, as in the prior models, the interaction between change in aggression and age of entry was significant: Children with earlier ages of entry had steeper declines in aggression between the ages of 2 and 4 years. This last result was due, in part, to the fact that children who had entered earlier had slightly higher aggression levels at age 2, albeit at even more modest, nonsignificant levels than indicated by the covariate-adjusted and propensity-score models (i.e., in the IV model, a 6-month difference in age of entry predicted a difference in aggression of about 0.14 SD, p = .37).
Results of the Instrumental-Variable Analysis of the Association Between Age of Entry Into Early Childhood Education and Care (ECEC) and Teacher-Rated Aggression Across Ages 2, 3, and 4 Years (n = 734)

Note: The instruments in this model were birth month and its interactions (i.e., birth month, Birth Month × Site, Birth Month × Cohort, and Birth Month × Cohort × Site); age of entry was the endogenous variable. Estimates in Stage 2 were weighted by propensity scores. In Stage 2, age of entry was centered such that the main effect estimated this variable’s association with average aggression across ages 2, 3, and 4 years. Values in parentheses are standard errors.
p < .05. **p < .01.
Figure 3 summarizes the results from all three models, showing the predicted effect of a 6-month delay in age of entry (e.g., entering ECEC at 18 months vs. 12 months) in SD units of teacher-rated aggression. It is evident that the estimated effects of age of entry were remarkably consistent across the models. The effects were small and diminished in size as the children grew older. The IV estimates were the least precise, yet their confidence intervals remained narrow enough that fairly small effects could have been detected; effect sizes smaller than those reported previously in the literature (e.g., NICHD Early Child Care Research Network, 2006) would have been easily detectable. Indeed, a 0.18-SD change in aggression given a 1-SD change in age of entry would have been sufficient for statistical significance (p < .05), but the largest IV estimate (at age 2) indicated a change in aggression of only 0.08 SD given a 1-SD change in age of entry, and by age 3, the predicted change in aggression was less than 0.01 SD.
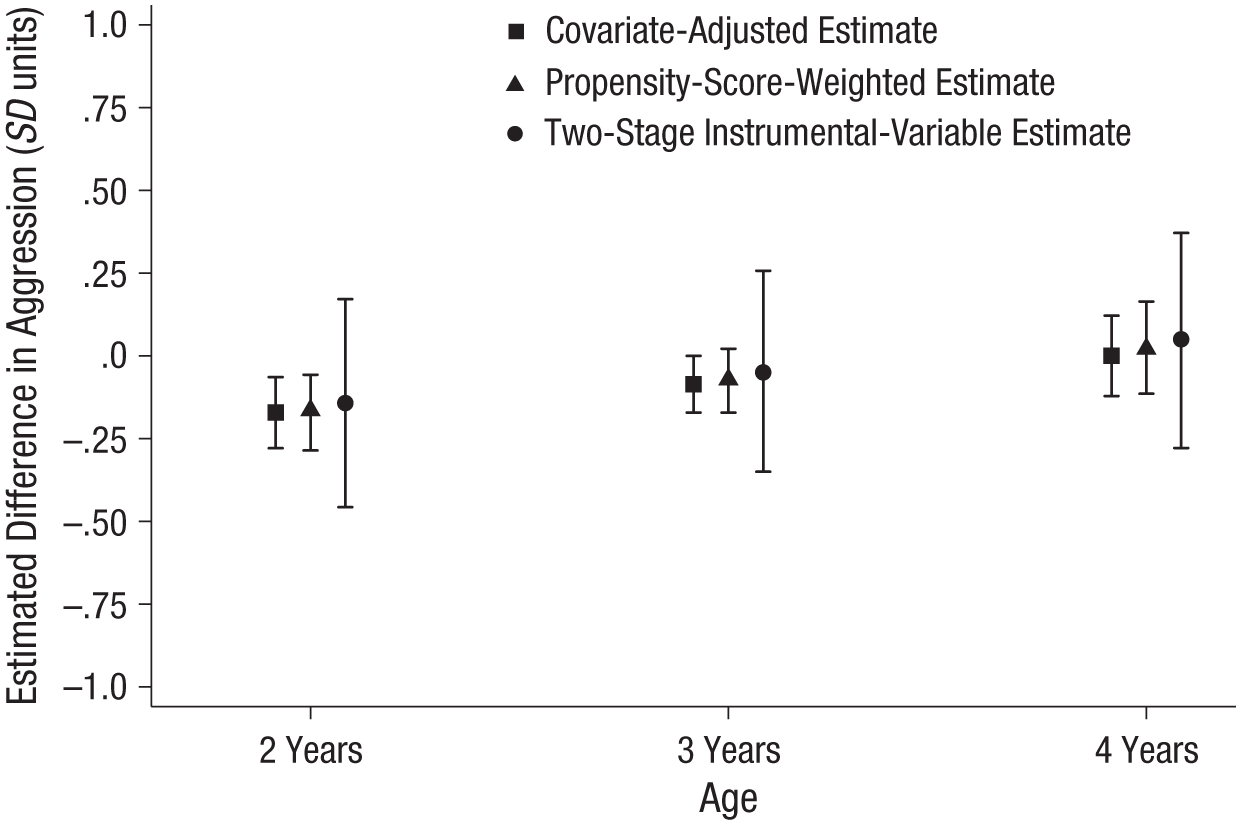
Estimated effect on aggression of delaying entry into Early Childhood Education and Care. The graph shows the three models’ estimates for the difference in teacher-rated aggression at ages 2, 3, and 4 years associated with delaying entry by 6 months (e.g., entry at 18 months vs. 12 months). Negative values indicate that later age of entry was associated with less aggression. Error bars represent 95% confidence intervals.
Sensitivity and robustness checks
To examine the robustness of our results and their sensitivity to model respecification, we estimated a variety of models beyond those described thus far. First, we reestimated our models using parents’ reports of aggression. In these models, neither age of entry nor the interaction between change in aggression and age of entry had a significant association with parent-reported aggression at 2, 3, or 4 years, regardless of our approach to handling selection bias.
Second, to examine the exclusion restriction, we reestimated our IV models for both teacher- and parent-reported aggression, but using maternal employment or the length of time the ECEC teacher had known the child, rather than age of entry into ECEC, as an endogenous predictor of aggression. There was no evidence that either predictor was related to aggression in the second stages of these models, and these variables also were not related to aggression in covariate-adjusted and propensity-score-weighted models.
Third, we estimated all of the models including the full sample of children in the BONDS (n = 1,157), regardless of when they had entered ECEC and regardless of their birth month. None of these models yielded results that differed substantively from our primary results; the patterns of null and statistically significant associations were identical. This was not surprising given that there were no significant differences in aggression levels for children who had entered ECEC after age 2 and those who had entered ECEC before age 2 (r = −.05 for aggression at 2 years and r = .00 for aggression at 4 years).
Finally, we estimated models to determine whether our results would differ according to the number of hours per week children attended ECEC, comparing those who attended less than 20 hr per week with those who attended more than 20 hr per week and allowing the effects of age of entry to vary in a linear fashion across number of hours. There was no evidence that hours of ECEC attendance moderated the effects of age of entry.
Discussion
For more than three decades, scientific and public excitement has surrounded questions of the socioemotional risk associated with early nonparental care. Recently, investigating the effects of nonparental care in diverse sociopolitical contexts has been prioritized, and researchers have become increasingly aware that potential selection effects are a matter of serious concern for much of the research to date (Zachrisson et al., 2013). Within this empirical zeitgeist, we exploited ECEC enrollment practices in Norway that caused variation in age of entry to test the causal hypothesis that early, extensive, and continuous ECEC attendance has lasting consequences for physical aggression during childhood. Our results provide little support for this hypothesis; early, extensive, and continuous ECEC attendance had, at most, faint and fading consequences for young children’s aggression in this study.
We did find that at age 2, modestly higher levels of aggression were associated with earlier entry into ECEC, but only when we used conventional covariate adjustments or propensity scores to handle selection bias. The size of the difference in age-2 aggression between children who entered ECEC early and late was too small to reach significance in the IV model; the coefficient was smaller and the confidence interval was wider in the IV model at age 2 compared with the covariate-adjusted and propensity-score-weighted models. Moreover, across the models, there was very consistent evidence that even when statistically significant, the effect sizes were small: Even 6-month differences (i.e., about 1.70 SD) in age of entry produced as little as a 0.14- to 0.18-SD difference in aggression. Although even small effects could have practical (and clinical) significance given the serious harm of persistent aggression problems, our results also indicated that these small effects faded to zero as children grew older.
Across methods of estimation, by age 4, aggression levels appeared all but identical for children who had entered ECEC prior to age 1 and those who had entered much later. We also found no evidence that this pattern of results changed as a function of how extensive children’s ECEC experiences were (i.e., their average hours per week in care). In light of these results, it is worth considering ways in which the Norwegian sociopolitical context might protect children from the risk found to be associated with early, extensive, and continuous nonparental care in other studies. First, it may be relevant that ECEC quality is federally regulated in Norway (e.g., adult:child ratios are fixed at or below 1:4 for the youngest children). However, there is very little evidence in the literature that ECEC quality moderates the effects of amount of time in care, despite much attention to this possibility (e.g., McCartney et al., 2010; Vandell, Belsky, Burchinal, Steinberg, & Vandergrift, 2010). Second, children in Norway rarely enter ECEC before they are 10 months old, because of the length of the parental leave allowances. Some researchers speculate that care initiated early in the first year of life is most risky, and that parental leave through the first year is one way to reduce that risk (Belsky, 2001). However, we have found little evidence in the literature that consequences of child-care quantity are exclusive to, or exceptional for, children who enter care in the first year (a relevant exception is work on cognitive risks associated with maternal employment in the first year of life, e.g., Lucas-Thompson, Goldberg, & Prause, 2010); instead, for physical aggression and related behavioral problems, researchers have reported a linear risk across developmental epochs during the first 3 to 4 years of life (e.g., Loeb et al., 2007; McCartney et al., 2010; Vandell et al., 2010).
Nonetheless, the majority of the children in the present study entered center care when they were more than 9 months old (as is true in Norway at large); the question of socioemotional risk associated with nonparental care in the first few months of life is a matter requiring further study in countries where this issue has sociopolitical relevance. Our results are also specific to physical aggression and do not preclude the possibility of risk in related domains of socioemotional functioning, such as generalized externalizing problems. Moreover, although effect sizes decreased linearly through age 4, we cannot rule out the possibility that the harm of early entry may not fully emerge until later ages. Given the argument that continuous nonparental care is most risky, however, it is noteworthy that the effects of ECEC became increasingly small as the children got older and had, therefore, spent more and more time in these settings.
Conclusion
Exploiting the effects of birth month on age of entry into ECEC in Norway—a sociopolitical context of generous parental leave allowances and nearly universal access to high-quality center care—we found that entering ECEC at relatively younger ages had, at most, faint and fading consequences for children’s aggression, even when their time in ECEC was extensive and continuous from about age 1 to age 4. If early, extensive, and continuous nonparental care does, in fact, cause high levels of aggression in children, then this study suggests that 1 year of parental leave, and entry into high-quality center care thereafter, may help prevent such an outcome.
Footnotes
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Funding
This research was funded by two grants from the Research Council of Norway (Grant Nos. 202438/S20 and 234828/H20).