
Abstract
Communication is a cooperative endeavor that goes well beyond decoding sentences’ literal meaning. Listeners actively construe the meaning of utterances from both their literal meanings and the pragmatic principles that govern communication. When communicators make pragmatically infelicitous statements, the effects can be similar to paltering—misleading speech that evokes false inferences from true statements. The American Diabetes Association’s (ADA’s) “Diabetes Myths” website provides a real-world case study in such misleading communications. Calling something a myth implies that it is clearly false. Instead, the ADA’s “myths” are false only because of some technicality or uncharitable reading. We compared participants’ baseline knowledge of diabetes with that of participants who read either the ADA’s myths or the myths rewritten as questions that do not presuppose the statement is false. As predicted, exposure to the ADA’s “myths,” but not to the rephrased questions, reduced basic knowledge of diabetes. Our findings underscore the need to consider psycholinguistic principles in mass communications.
Record numbers of Americans rely on the Internet for health information (Fox & Duggan, 2013). Although researchers have evaluated the accuracy of online health information (Silberg, Lundberg, & Musacchio, 1997; Wilson & Risk, 2002), they have largely neglected to assess how people actually interpret the material. For health websites to communicate effectively, it is crucial that they be informed by insights from psycho-linguistics.
Decades of work in psycholinguistics have established that the pragmatics of utterances is fundamental to linguistic communication across a wide range of contexts (see E. Clark, 2004; H. Clark, 1996; Sperber & Wilson, 2005, for reviews). In foundational work, Grice (1975) argued that successful communication is a cooperative endeavor between speakers and listeners. Conversational partners do not simply decode the literal meaning of each other’s utterances but instead work to figure out their communicative intent. Grice’s cooperative principle of communication specifies maxims by which conversational partners establish what information is mutually available, what level of detail is expected, how truthful the utterance is, and more. These are not norms of politeness but instead are integral to how communication takes place. If, for example, a shopper asks a salesperson, “Can you tell me how much this costs?” it would be uncooperative for the salesperson to respond “Yes,” full stop. The shopper is not asking a literal yes-or-no question about the ability of the salesperson but is using that question as an indirect request (H. Clark, 1979) to discover the item’s price. The clerk should address the shopper’s communicative intent, not the literal question.
Gricean guidelines for effective communication apply equally to mass communications, such as websites conveying health information, where authors must act as cooperative speakers and visitors as active listeners. If these guideline are not followed, the effects can be similar to paltering 1 —the act of deceiving through true statements (Schauer & Zeckhauser, 2009). Often, paltering relies on a victim drawing false inferences from the pragmatics of a speaker’s semantically true utterance. Suppose someone is selling a car and a potential buyer asks, “Does this car need any maintenance?” The car is scheduled to need extensive maintenance fairly soon, but a paltering seller might respond, “It’s a great car; it’s always run beautifully.” This statement might be literally true, but it gives the false impression that the car does not need maintenance. As this example illustrates, conversational implicatures can be just as misleading as outright falsehoods (Rogers, Zeckhauser, Gino, Norton, & Schweitzer, 2017).
The risks and consequences of unintentional paltering may be especially severe for well-respected and expert sources of advice. Readers are most likely to trust sources they believe are expert, upstanding, and benevolent (Goldman, 2001; Hendriks, Kienhues, & Bromme, 2015) and to therefore be less critical of their claims. Moreover, pragmatic inferences often depend on what a listener assumes a speaker knows: When speakers are assumed to be highly knowledgeable, stronger pragmatic inferences can be licensed (e.g., Goodman & Stuhlmüller, 2013). Readers likely assume that experts intend to be constructive and helpful, to guide them to take appropriate actions—further licensing strong pragmatic inferences. Compounding these challenges is the fact that experts often struggle to take the perspectives of laypeople (see Nickerson, 1999). This may make it difficult for them to anticipate how laypeople will interpret their communications and what pragmatic inferences people may draw, underscoring the need to raise awareness of these issues among health professionals.
If health communicators fail to honor cooperative principles, there is a risk that readers will misinterpret communicative intentions and will thereby be misled. As a case study of how health communicators may mislead by unintentionally paltering, we analyzed a prominent link featuring “Diabetes Myths” on the website of the American Diabetes Association (ADA). We argue that the expression of these myths violates the cooperative principle for successful communication. Readers of a respected health website that lists myths likely assume the authors are targeting completely false statements, not statements that are pretty much true, not quite right, or false only because of some technicality or uncharitable reading. In contrast, the ADA characterizes as “myths” many statements that either are largely true or false only because of some technicality. Labeling partly true statements as “myths” is infelicitous and can mislead readers who seek to use that information to figure out how to improve their health.
The ADA presents 10 “myths” about diabetes. On our reading, 7 of these myths are misleading. Here are analyses of 2 of the “myths” from the ADA’s website that illustrate these problems (http://www.diabetes.org/diabetes-basics/myths/):
“Myth: If you are overweight or obese, you will eventually develop type 2 diabetes.” Although it is true that being overweight or obese does not guarantee one will develop Type 2 diabetes, calling this statement a myth could lead readers to infer that being overweight or obese is not a significant risk factor for developing Type 2 diabetes.
“Myth: People with diabetes can’t eat sweets or chocolate.” If this is a myth, the implied truth is that “people with diabetes can eat sweets and chocolate.” From this, people could reasonably infer that people with diabetes are free to regularly include sweets and chocolates as part of their diet.
Together, the seven infelicitous myths on the ADA’s website could lead people to infer that being overweight is not a significant risk factor for developing diabetes, that people with diabetes can continue eating sweets the way they normally do, that they do not need to improve their diets, that they have a robust immune system, and that nothing much can be done to stop diabetes from progressing. In this way, the ADA’s myths webpage could be a real-world demonstration of misinformation through unintentional paltering.
Given that the ADA’s “myths” are pragmatically infelicitous, we predicted that they not only will fail to improve people’s knowledge about diabetes but will actually mislead people. To test this, we compared people’s knowledge of diabetes in five experimental conditions. In the first condition, participants’ baseline knowledge was assessed without any new information. In the second condition, we presented the ADA’s myths alone and then assessed participants’ beliefs. This condition addressed what visitors to the site infer from just reading the myths. In the third condition, we rephrased the myths as questions. For example, instead of presenting the myth, “People with diabetes can’t eat sweets or chocolate,” we transformed it into a question: “Can people with diabetes eat sweets or chocolate?” Questions do not have the same presuppositions as myths; listeners do not assume that the underlying statement must be false but rather expect to find out what the truth is. A comparison between this condition and the myths condition permits a controlled test of the effects of infelicitous statements by experts. To elaborate on the myths, the ADA also provides explanations (what they call “facts”) after each myth. In two other conditions, we presented these explanations along with either the myths or reframed questions.
Method
Participants
A total of 250 participants living in the United States were recruited online from Amazon Mechanical Turk (MTurk). A sample size of 50 participants per condition was chosen on the basis of the results of an initial pilot study. All participants were compensated $1.00, with an additional $1.00 bonus given to participants in certain conditions. Two participants were excluded from data analyses for failure to pay attention, leaving 248 in the final sample (126 women, 122 men; mean age = 38.5 years).
Of those willing to respond, 5.7% reported being diabetic. Among nondiabetic participants, 13.4% indicated that they are prediabetic and 68% indicated that they have a close family member or friend who is diabetic. In total, 19% of participants have been diagnosed as either diabetic or prediabetic and 68% of participants have someone close to them with diabetes. Compared with nationwide U.S. demographics, participants in this sample are generally more educated (48% hold a bachelor’s degree or higher) and have a relatively high income (median income between $50,000 and $70,000). Asian participants are overrepresented (8.1%), and Hispanic participants are underrepresented (3.6%) in the sample. Although MTurk participants may not be a representative U.S. sample, they are likely very similar to people who seek health information via the Internet (Huff & Tingley, 2015; Paolacci & Chandler, 2014).
Materials and design
Each participant was randomly assigned to one of five conditions (a between-subjects design): a no-intervention control condition or one of four different educational-intervention conditions. The educational conditions were based on the list of “diabetes myths” available on the ADA website (http://www.diabetes.org). The site lists 10 alleged myths about diabetes along with a brief explanation for each. Seven of these myths appear infelicitous and are reproduced as they appeared at the time of the study in Table 1.
Infelicitous Myths and Their Accompanying Facts, as Listed on the American Diabetes Association’s (2017a) Website
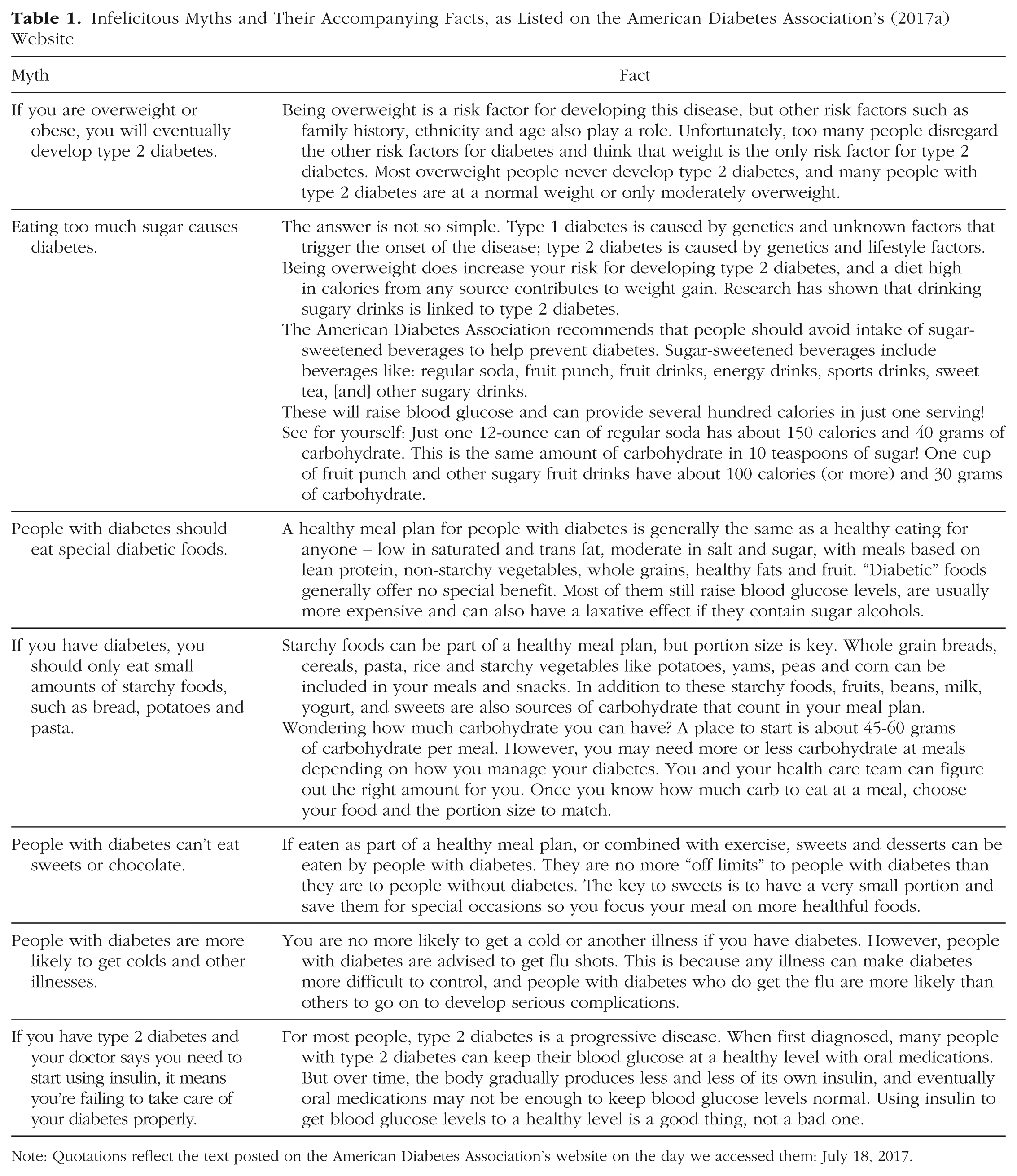
Note: Quotations reflect the text posted on the American Diabetes Association’s website on the day we accessed them: July 18, 2017.
We used the ADA’s materials in a factorial design to produce four different educational interventions by (a) including or omitting the facts for each myth and (b) using the original myth language or rephrasing the myths into questions. We thereby created four separate interventions: myths only, questions only, myths plus facts, and questions plus facts. In the myth conditions, participants were told that they would read some myths about diabetes. In the question conditions, participants were told they would read some common questions people have about diabetes. In all four conditions, participants were told that the information they would read came from the ADA.
To assess the impact of these interventions on participants’ diabetes knowledge, we generated 10 true/false items testing knowledge about diabetes that we thought might be undermined by the ADA’s myths. We therefore predicted that performance on these items would be reduced after reading the myths. For each item, participants were asked to indicate whether the statement in the question was “definitely true,” “probably true,” “probably false,” or “definitely false.” The correct answers were drawn from the ADA’s websites. The statements that participants needed to judge and the ADA’s sources for the correct answers are listed in Table 2.
Diabetes Knowledge Questions Used in the Present Study and Answer Sources

Note: Quotations reflect the text posted on the American Diabetes Association’s (ADA’s) website on the day we accessed them: July 18, 2017.
The correct answer is “false.”
Procedure
After being recruited from MTurk (via TurkPrime; Litman, Robinson, & Abberbock, 2016), participants were directed to a Qualtrics (Provo, UT) survey software website where the study was administered. Each participant was randomly assigned to read one of the four interventions or to a baseline control group with no intervention, for a total of five conditions. Participants assigned to the myths-plus-facts or questions-plus-facts conditions were informed that their participation would take additional time and that they would be compensated an additional $1.00. After responding to demographic questions, participants advanced to their assigned reading. Once they completed the reading, they were given the diabetes knowledge questionnaire. Participants in the no-intervention control condition advanced directly to the diabetes knowledge questionnaire. Included in the diabetes knowledge questionnaire was an attention-check question that simply asked participants to enter “probably false.”
Results
Two participants were excluded from analyses because they failed the attention-check question, leaving 248 participants in the final analysis. First, we recoded participants’ responses as correct and incorrect (binary coding). Figure 1 shows the proportion of correct responses participants gave in each condition.
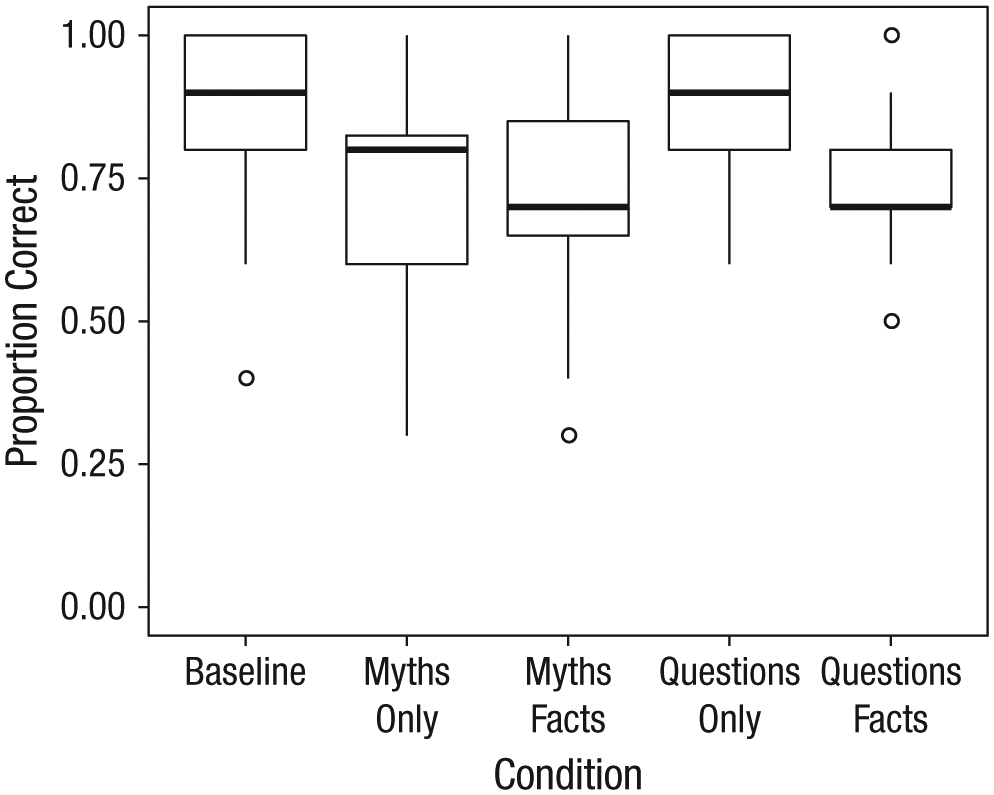
Proportion of correct responses across the 10 items, separately for each of the five conditions. The box-and-whisker plots indicate the distribution of observed values, labeling the medians (bold lines), upper and lower quartile values (box tops and bottoms), and the maximum and minimum points within 1.5 times the interquartile range (whiskers). Observations lying outside this interval are plotted individually as points.
We first compared each intervention condition with the baseline control condition, which assessed participants’ prior knowledge without information from the website. As seen in Figure 1, participants in the baseline condition scored highly (mean proportion correct = .89), indicating a solid grasp of these basic points. As predicted, there was a significant detriment to diabetes knowledge in the myths-only condition: Welch’s t(73) = 5.27, p < .001, d = 1.09. In contrast, when the myths were rewritten as questions, in the questions-only condition, performance was as high as baseline, t(98) = 0.73, p = .47. Including the ADA’s facts with the myths or questions the participants read was not beneficial but instead resulted in a decrement in knowledge in both the myths-plus-facts condition, t(108.3) = 5.97, p < .001, d = 1.12, and in the questions-plus-facts condition, t(88.7) = 6.20, p < .001, d = 1.26.
A two-way analysis of variance (ANOVA) examined the effects of myth language and the presence of facts across all intervention conditions. There was a significant interaction between myth language and presence of facts, F(1, 190) = 12.90, p < .001, η p 2 = .064. Neither main effect was significant (Fs < 1). Consistent with the comparisons against baseline, these results suggest that both the presentation of myths and the corresponding facts reduced participants’ knowledge of these basic diabetes facts. Comparing the myths-only and myths-plus-facts conditions revealed that the inclusion of facts alongside myths did not mitigate their negative effects on diabetes knowledge, t(85.2) = −0.32, p = .75. Moreover, comparing the questions condition with the questions-plus-facts condition confirmed that these explanations actually led to confusion even when the myths were rephrased as questions, t(86) = 5.46, p < .001, d = 1.15.
Next, we examined participants’ confidence in their correct and incorrect responses, recoded from their scale responses as either high or low. Figure 2 shows participants’ average confidence across items in each condition.
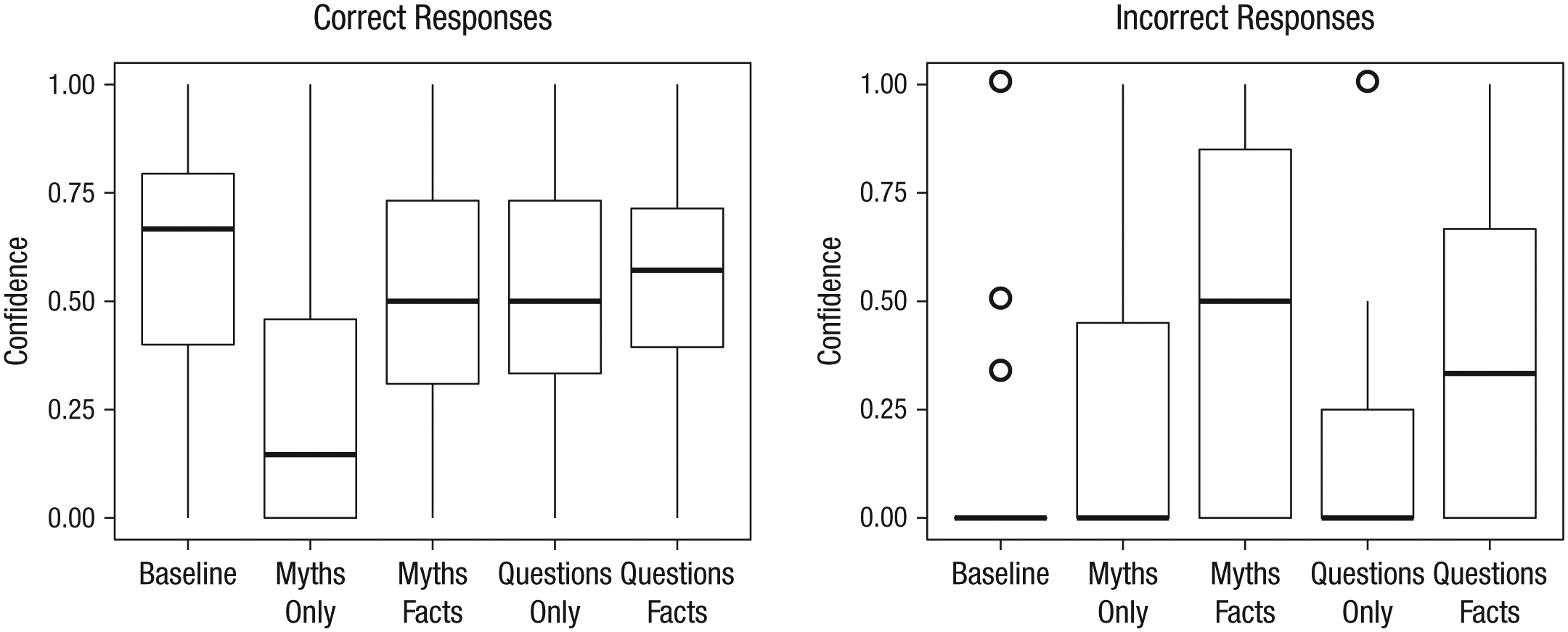
Proportion of highly confident responses, separately for correct (left graph) and incorrect (right graph) responses. The box-and-whisker plots indicate the distribution of observed values, labeling the medians (bold lines), upper and lower quartile values (box tops and bottoms), and the maximum and minimum points within 1.5 times the interquartile range (whiskers). Observations lying outside this interval are plotted individually as points.
Beneficial materials should have increased participants’ confidence in their correct answers. Instead, we found that the ADA’s myths undermined confidence in the knowledge that they retained in the myths-only condition, where participants’ confidence in their correct answers was reduced relative to the control condition, t(85.6) = 4.67, p < .001, d = 0.96. We then examined the effects on confidence for correct answers across all the conditions. A two-way ANOVA examined the effects of myth language and the presence of facts across all intervention conditions on participants’ confidence in correct answers. Confidence in correct answers was lower for interventions without facts, F(1, 190) = 13.31, p = .003, η p 2 = .065. There was no main effect of myths language, F(1, 190) = 1.16, p = .28, but there was a significant interaction between these two factors, F(1, 190) = 5.158, p = .024, η p 2 = .026, reflecting the larger reduction in confidence observed in the myths-only condition.
These results suggest that the ADA’s explanatory facts may have buffered against a loss of confidence in correct responses. However, this potential benefit is undercut by the facts’ effect on incorrect answers. If the explanatory “facts” from the website had been truly beneficial, they should have reduced participants’ confidence in their incorrect answers. Instead, the opposite occurred. Participants actually became more confident in their incorrect responses following the myths-plus-facts interventions, t(72.6) = −4.71, p < .001, d = 1.02, and questions-plus-facts interventions, t(69.6) = −3.00, p = .004, d = 0.70, compared with the baseline condition. Consistent with this, a two-way ANOVA across intervention conditions revealed a significant main effect of the presence of explanations, F(1, 162) = 14.41, p < .001, η p 2 = .082, and no other significant effects (ps > .20). The presence of facts inflated confidence in incorrect responses, indicating that the ADA’s facts generated additional confusion about basic diabetes knowledge.
Discussion
After examining the myths presented on the ADA website, we concluded that many were pragmatically infelicitous and likely to confuse or mislead readers. According to the cooperative principles that govern communication, if an expert describes something as a myth, people will assume the myth is robustly false, but the ADA’s myths were either at least partly true or only technically false. In a controlled experiment, we found that these “diabetes myths” misled participants, reducing the knowledge that the myths addressed. Participants who read the myths performed worse than participants who read nothing or who read the myths rephrased as questions that do not presuppose that the underlying statements are false.
These findings are particularly striking, given that the diabetes knowledge we tested was reasonably basic. At baseline, participants displayed a solid grasp of this material: For instance, 98% of participants in the baseline condition knew that “being overweight significantly increases the likelihood that someone will become diabetic,” but after reading the diabetes myths, only 81% of participants answered correctly. On a more challenging item, “people with diabetes have a compromised immune system and are more likely to have serious infections” (true), 76% of participants in the baseline condition answered correctly, but only 38% in the myths conditions did. These findings illustrate the power of pragmatics: Failing to honor the cooperative principle resulted in unintentional paltering strong enough to disrupt even reasonably basic diabetes knowledge.
Coupled with the myths, the facts did nothing to improve participants’ diabetes knowledge or to prevent them from being misled. Worse, when coupled with the myths rephrased as questions, the ADA’s explanations themselves led to a reduction in diabetes knowledge. Although they contain technically true statements, these explanations misled readers toward drawing incorrect inferences. For instance, one fact says that “most overweight people never develop Type 2 diabetes, and many people with Type 2 diabetes are at a normal weight or only modestly overweight” (ADA, 2017a). This reinforces the incorrect inference that being overweight is not a significant risk factor for diabetes. Another fact claims that sweets and chocolate “are no more ‘off limits’ to people with diabetes than they are to people without diabetes” (ADA, 2017a). Since many people without diabetes frequently eat sweets and chocolate, this falsely implies that people with diabetes could safely do so as well. The need to respect conversational pragmatics is not limited to the pragmatics of myths. Rather, unintentional paltering appears to have occurred in the explanations as well.
Genuine palterers communicate to deceive rather than to communicate truths. We suspect that the ADA, although well-intentioned, unintentionally paltered because it also had goals beyond conveying factually true statements: It seems to have underplayed the role of individuals’ behavior in managing their diabetes and the need for serious lifestyle changes in an attempt to avoid stigmatizing or discouraging diabetic readers. Although health education should avoid blaming or stigmatizing people, it also needs to motivate them to make the changes necessary to improve their health outcomes (Funnell et al., 1991).
This delicate communicative balancing act applies well beyond diabetes education: It is one that health professionals must face when treating patients for any disease driven by lifestyle factors such as diet and exercise. To empower people to improve their health, health professionals must entrust them with the information they need to make decisions and take appropriate actions. It is possible to be straightforward about the challenges people face while still empowering them to improve their situations (e.g., see Brady et al., 2018). More broadly, we suggest that health communicators should be forthright in their communicative intentions rather than risk missteps that could lead unintentionally to paltering.
Further, the consequences of misleading statements—intentional or accidental—are not easily reversed. For example, presenting corrections or clarifications directly following misleading claims in prescription drug advertising can sometimes be successful (Aikin et al., 2017) but often fails to entirely reverse their misleading effects (Aikin et al., 2015; also see Chan, Jones, Hall Jamieson, & Albarracín, 2017). Worse, attempts to debunk myths and correct misconceptions can even backfire, leading to even more deeply entrenched misconceptions (Lewandowsky, Ecker, Seifert, Schwarz, & Cook, 2012). Even when myths are debunked felicitously, these interventions may backfire if the repetition of the myths strengthens people’s memory for the incorrect information (Schwarz, Sanna, Skurnik, & Yoon, 2007). Given these difficulties, it is clearly vital to avoid misinforming health consumers in the first place.
Our findings highlight the more general need to empirically validate educational materials and interventions. Many interventions are designed by thoughtful people using their best judgment, but common sense cannot always anticipate the nuanced and counterintuitive ways that human psychology works (Wilson, 2005, 2011). From his extensive review, Wilson (2011) concludes, “It is no exaggeration to say that common sense interventions have prolonged stress, increased drug use, made people unhappy, and even hastened their death” (p. 15). Interventions must be based on evidence. Because health websites are readily available communications from trusted experts and widely used by people seeking advice, their authors should ensure that the messages they provide accomplish what they intend.
Supplemental Material
PowellOpenPracticesDisclosure – Supplemental material for Misleading Health Consumers Through Violations of Communicative Norms: A Case Study of Online Diabetes Education
Supplemental material, PowellOpenPracticesDisclosure for Misleading Health Consumers Through Violations of Communicative Norms: A Case Study of Online Diabetes Education by Derek Powell, Martin Keil, Dru Brenner, Liliana Lim and Ellen M. Markman in Psychological Science
Footnotes
Action Editor
Rebecca Treiman served as action editor for this article.
Author Contributions
All authors contributed to the study design. D. Powell conducted the experiment and analyzed the data. All authors contributed to early drafts of the manuscript. D. Powell, M. Keil, and E. M. Markman wrote the final manuscript.
Declaration of Conflicting Interests
The author(s) declared that there were no conflicts of interest with respect to the authorship or the publication of this article.
Open Practices
All data and materials have been made publicly available via the Open Science Framework and can be accessed at https://osf.io/38apk/?view_only=66833d11e36f4af8a17e56d45ac5e379. The design and analysis plan for this experiment were not preregistered. The complete Open Practices Disclosure for this article can be found at http://journals.sagepub.com/doi/suppl/10.1177/0956797617753393. This article has received badges for Open Data and Open Materials. More information about the Open Practices badges can be found at ![]() .
.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.