
Abstract
‘Mad doctors’ specialized in treating the insane, but what about the doctors whose own mental health was jeopardized? Oppenheim found that doctors who attended the mad were presumed to be particularly vulnerable, but there has been no research investigating this claim, nor identifying practitioners’ experiences as patients. This article analyses medical admissions to asylums via both case notes and other sources such as newspaper reports, revealing the responses of medical superintendents to their former colleagues and, in some cases, the judgements of practitioners on their institutional surroundings. It indicates the impact of work-related stress, as medicine became self-consciously professional, and the evolution of public reactions to doctors who could not maintain an appropriately sane identity.
Introduction
James Pownall was a mad doctor in every sense of the phrase. He experienced his first period of mental instability in 1839, and was a patient of two different private asylums in 1839–40. On recovery he went home to Wiltshire and turned his experiences to account, by obtaining a licence and running his own establishment for the insane, Northfield House at Calne. This was not a large institution, catering for 5–15 inmates, but was successful enough until 1854 when Pownall attacked one of his patients and the incident was reported to the Lunacy Commissioners. He was committed once more, this time to Munster House in Fulham and, not surprisingly, his own asylum was closed by 31 March 1855 (PP, 1855, 1860). Pownall appears to have lived free of maniacal episodes between 1856 and 1858, but in March 1859 he attempted suicide and in April launched a murderous assault on his mother-in-law. This time he was admitted to the licensed Northwoods Asylum at Winterbourne in Gloucestershire, under the superintendence of Dr James Davey. Pownall was controversially discharged ‘cured’ by Davey and placed in the house of a Dr Leete at Lydney in Gloucestershire. Leete was probably supplying a single lodging for Pownall, a strategy employed for an estimated 1500–2000 disturbed patients nationwide at this time (Hervey, 1985: 118). Davey apparently regarded Pownall as sane, but Pownall’s wife was not so confident, which gave rise to this intermediate level of care. Unfortunately, while at Leete’s house in August 1859 Pownall murdered a servant and at his trial he was judged insane. 1 Lunacy Commissioners then entered a period of peevish and rather one-sided debate with Davey about the wisdom of Pownall’s discharge from Northwoods, while Pownall was again detained. He was never again at liberty. He was transferred to Broadmoor after the hospital opened in 1863 and died there in 1882 (PP, 1860). 2
Pownall is one extreme example of a host of medical practitioners who were deemed by their nineteenth-century contemporaries to be suffering from severe mental-health problems, specifically complaints of such gravity that they warranted asylum admission. The supposed causes of their complaints covered the same range as for non-medical patients, in that these were ascribed to contextual causes such as overwork, domestic disharmony, financial troubles, and physical or moral causes including alcohol consumption, heredity and masturbation. But medical patients were different from other asylum inmates in that they were the former (and in some cases future) colleagues of their keepers.
There is a good deal of anecdotal evidence that doctors who held roles caring for or treating the mad were particularly prone to suffer mental disturbance. In Shattered Nerves, Janet Oppenheim makes the point that in 1860 medical officers of asylums were urged to be careful of their own mental health, and she alludes to instances of medical depression or neurasthenia more generally; but her claims are substantiated by contemporary allegations rather than by sufficient concrete examples (Oppenheim, 1991: 153–4). It has since emerged that 15 medical practitioners were admitted to Ticehurst Asylum in Sussex between 1845 and 1885, including Samuel Hill, the former superintendent of the North Riding asylum in Yorkshire, thought to be suffering from ‘over- pressure of duties’ (MacKenzie, 1992: 130, 132, 153). But this does not explain whether Ticehurst entirely accounted for the nation’s doctors who suffered disruptions to their mental health, or whether (given the high fees there) these 15 men were the tip of the iceberg. If Oppenheim’s general points are correct, then professional men in general, and medical practitioners in particular, may have been prone to stress, breakdown and even ‘insanity’, whether or not they were themselves doctors of the mad.
However, even average levels of vulnerability to mental distress are difficult to detect from the sources left directly by doctors. There were good reasons for medical men to be reticent about their mental ill-health in their public and even private writings. Micale (2008) has argued that between 1790 and 1860 there was medical denial that hysteria, for example, could be suffered by men. He sees this as part of a broader redefinition of masculinity, such that ‘By the end of Victoria’s reign, the spectrum of emotions deemed appropriate for adult men in Britain had greatly diminished, as the familiar historical image of stoical insensibility and the stiff upper lip emerged and hardened’ (Micale, 2008: 57). Consequently expressions of uncertainty, anxiety, fear or distress became increasingly problematic.
At the same time trends within nineteenth-century medicine to define and regulate the profession were clearly increasing the potential pressures and work-based stresses on practitioners. By the late 1880s, the concept of the professional medical man had acquired numerous potential attributes. These did not all necessarily have to be represented in one man, but individuals needed to display a suitable range to qualify. Criteria included education and qualification by recognized bodies, membership of learned or professional societies, holding public office, subscription to dedicated journals, and espousing values indicative of participation in a collective community of doctors. 3 This latter quality was not regulated by anything as concrete as a formal code of medical ethics, but could still seem to an interested observer to be highly exacting. Thorold Rogers defended the posthumous reputation of his brother Joseph who had been a doctor; he may well have overstated his case, but he claimed that the professional doctor was held to higher standards than other men, eschewing evident rivalry with colleagues and being required to be wholly open on matters of treatment: ‘It is no easy matter to win position and fortune in a calling which is regulated by the strictest rules of professional honour’ (Rogers, 1889: vii). Rogers was tacitly recognizing the tensions between the active medical marketplace and the emergent but uncodified yardsticks of medical integrity. But professional standards were not the only criteria being weighed. Alongside these, there were implicit personal qualities which were also essential to the successful medical man as a gentleman (Waddington, 2002: 49). Financial probity, mental resilience, sexual continence, civil obedience, emotional self-command and the appropriate expression of ambition (energetic but honest) were all embedded to some extent in the professional persona, in that they were also markers of late-Victorian middle-class masculinity.
These factors contributed to a mutable but still stringent ideal, which might be the object of many but the attainment of rather fewer. Medical careers and personal lives rarely ran so smoothly as to permit a steady acquisition of these multiple attributes. Students might fall at the first clear hurdle, namely by failing their examinations or falling prey to examination stress. Once secure in their qualifications they might struggle to obtain a remunerated post. The strains of juggling private practice, public responsibility, domestic solvency and personal ambition could and did wreak havoc on individual men’s physical and mental health, prompting hundreds of medical suicides. 4 The evolution of a professional ideal ensured the emergence of its antithetical counterpart, giving rise to the anxious, overworked, disappointed or fearful practitioner, who could not always withstand the pressures imposed by their professional and personal goals.
Increasingly sharp definition of professionally-appropriate qualities and behaviour should theoretically have rendered professional achievement more difficult at the same time as public tolerance to doctors’ mental breakdowns would arguably have been in decline. Did the fluid but gradually more stringent professional ideal have the effect of reducing public tolerance and/or raising expectations among medical men by widening the gap between the ideal and experience? This very large question can be investigated in part via an examination of unstable practitioners whose difficulties became subject to an institutional context and to systematic record-keeping.
It should not be surprising to find medical men as patients in establishments for the insane, particularly if Scull (2006: 79) is right to argue that ‘men who were active in business or the professions tended to be institutionalised more rapidly than their womenfolk’ owing to the impact of their reduced earnings or their potential for violence. Yet to see medical practitioners as the recipients rather than the providers of mental-health care is also to run counter to the historiography of the asylum. Historians who would support the general outline of Foucault’s ‘great confinement’ thesis have characterized doctors as among those responsible for defining, capturing and incarcerating the insane. The rationales for admitting pauper patients to county asylums or workhouses have circled around the limitations of domestic care, the function of Poor Law officers in determining the criteria for institutional admission, or the wholesale consignment of inconvenient people away from public view (Walton, 1985). Movement of middling and elite patients into and out of private asylums was not dependent on local government policy but was similarly guided by household, family, community and institutional definitions of unacceptable behaviours. The impulses which acted in admissions of middling, professional patients have not been surveyed discretely but it is reasonable to suppose that shifting norms of professional identity may well have given rise to controversial cases; eccentricities of personal, professional or public demeanour might be understood as mental illness.
Analysis of the institutional destinations of ‘insane’ practitioners is complicated by the heterogeneous provision of private and public placements. Licensed houses run by private entrepreneurs were assumed to be most suited to the middle-class patient, but the capacity of county asylums and the demand for affordable accommodation meant that asylums could offer and readily secure custom for different ‘classes’ of admission among paying patients, as Melling and Forsyth (2006: 146) demonstrated at Exminster. The routes by which doctors were admitted to one or more types of institutional care offer insights into the role of family members, fellow practitioners and others in certifying, admitting and cataloguing the case of a doctor deemed ‘insane’. Consequently, patterns of admission suggest complicity or conflicts within medicine in determining the boundaries of institutionalized ‘madness’.
Consideration of aspects of asylum care demands some attention to the case notes generated by institutions. The potential and pitfalls of case-note scrutiny have been surveyed for Gartnavel Royal Hospital in Glasgow, and the generalities observed there are broadly applicable to the case notes of the first English county asylums. In the Glasgow case notes there is a discernible difference between notes written for pauper or working-class patients and those from a more prosperous background or who had been well educated (Andrews, 1998: 266). Additionally, I will argue that case notes could sometimes achieve a particular pitch of poignancy when the medical author (frequently the asylum superintendent) was annotating the case of a fellow medical man. The disparity between the career ambitions or achievements of a fellow practitioner and their some-time asylum residence, combined with empathy from their medical observers, could inspire unduly personal reflections amid the more routine chronicle of case developments. Furthermore where the medical training and professional experiences of patients influenced the specific forms of their paranoia, delusions or hallucinations, an occupational affinity between asylum doctors and their patient could also facilitate enhanced transcripts of patient testimony. As a result, it may be plausible to examine the pressures of practice driven by both market concerns and by the strain of supporting a professional identity by reference to the obsessive preoccupations of incarcerated practitioners.
The experiences of medical men as patients need not be considered exclusively through the prism of institutional case notes, however; the same men can be tracked through censuses, vital registration and other genealogical materials. What is more, the public identity of the former (and sometimes future) practitioner can be traced in trade directories and newspapers. Only 10 years ago, such a pursuit of a specific cohort of individuals through these amassed sources would have entailed both a lifetime of commitment and a good dose of luck. Fortunately some projects to digitize these types of historical source have now reached fruition so that everything from a fleeting hospital appointment to a fulsome obituary may be located with relative ease. Searching digital sources and particularly newspapers via surnames and keywords offers the opportunity to view public reactions to medical practitioners before, during and after evidence of mental ill-health. Patients may reasonably have been either shocked and disdainful or sympathetic and generous when their doctors themselves fell ill.
The research that follows provides a means to test the validity of these multiple assumptions and to set the numbers of doctors who were themselves diagnosed ‘insane’ into context. The article will begin by considering the permeability of different institutions to medical patients across England and Wales, by a simple count of asylum patients whose former occupation was given as medical in the census of 1881. This introductory survey provides a setting for a closer, detailed study of over 70 practitioners who were admitted to one or more county or borough asylums up to 1890, with a particular focus on 10 selected institutions. How were admissions and the resulting cases of medical patients captured, justified and elaborated in case notes? What happened when encounters between doctors on both sides of the treatment divide spilled over into the public domain? Is it possible to discern the reactions of the general public to evidence of practitioners’ instability and weaknesses via press reporting?
Medical patients in English and Welsh asylums in 1881
The institutional options available for the care of the insane varied according to the fees that families could afford. For those with little or no money to spare, there were the county ‘pauper’ asylums which charged patients to Poor Law Unions or levied modest fees for paying places. The range of fees was more diverse among the private licensed houses, which were frequently small-scale and potentially exclusive; Ticehurst Asylum was undeniably elite and, depending on their wealth, residents might pay in excess of 1000 guineas a year for the benefits of a place, but the majority of licensed houses commanded more moderate fees of up to £150 per patient per year (PP, 1879: 113). The numbers of these establishments naturally fluctuated over the nineteenth century; there were 86 in 1819 (37 located in Middlesex) but only 59 at the time of the 1881 census (and they were noticeably more dispersed across the provinces) (PP, 1819). It is quite likely that market pressures forced the consolidation of the private house ‘market’ in the face of increased supply from county asylums. In addition there were a few charity hospitals funded by endowment or subscription that accommodated greater numbers than the private houses but fewer than the county asylums; these could offer fee bursaries or exemptions. In this way the variety of settings ranged from the domestic through to the large-scale, even ‘total’ institution (Scull, 2006: 80–1).
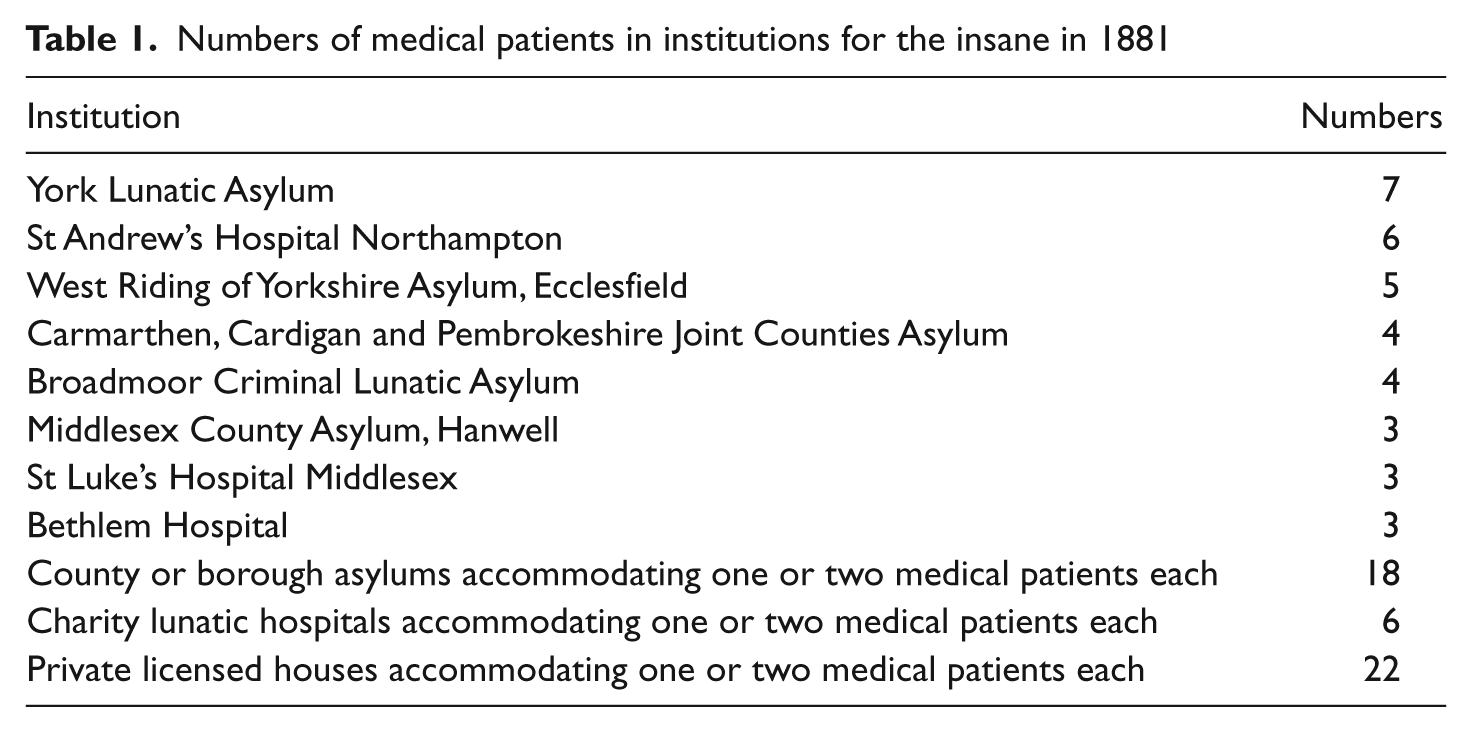
A snapshot of the choice of establishments made by medical patients and their families can be confirmed via the institutional listings within census returns. A comparison of the 137 asylums listed in appendix ‘P’ of the 35th annual report of the Commissioners in Lunacy with the contemporaneous 1881 census has located all but eight of the extant asylums. 5 A survey of the inmates in each place identifies 81 medical men under confinement across 43 establishments; see Table 1. The definition of ‘medical men’, here and throughout this article, is confined to a fairly narrow range of occupational labels in line with nineteenth-century denotations of the ‘profession’. The 1881 census grouped physicians, surgeons and general practitioners together as emphatic representatives of the ‘medical profession’ in its occupational tables. Medical students and assistants were accounted separately, as were dentists, midwives and those in ‘subordinate’ medical service such as sick nurses. Since this article is chiefly concerned with medicine and the particular stresses of medical professionalization, it includes consideration of physicians, surgeons and general practitioners, along with medical students and assistants (who were almost certainly striving for medical professionalism) but not dentists, midwives or members of the ‘subordinate’ group. Dentists and others will have had their own trajectories of professionalization, but these are outside the scope of this study. Of the 81 men identified, 60 were physicians, surgeons or general practitioners while 21 were medical students or assistants. Given the total numbers of men in each of these two groups enumerated by the census, this means that in 1881 one in every 255 qualified medical men was confined as insane, and that one in every 320 medical students or assistants was similarly confined. 6 Throughout the remainder of this article, references to ‘medical patients’ can be taken to include representatives of both qualified and student groups.
Numbers of medical patients in institutions for the insane in 1881
No institution accommodated more than seven of these patients at any one time in 1881 and, as might be supposed given their greater capacities, the county asylums and charity hospitals tended to account for the highest numbers. The York Asylum and St Andrew’s at Northampton were the most popular destinations for medical patients, and both happened to be charitably rather than publicly-funded. Even so, the presence of the Ecclesfield County Asylum in Yorkshire in Table 1, among other county and some borough institutions, provides further confirmation that the ‘pauper’ lunatic asylums were not exclusively reserved for the impoverished but were also used by families of the middle-income ‘insane’. Medical patients were proportionately more likely to enter private establishments, however, since a quarter of them were found in licensed houses (and these supplied only 9% of all male institutional places). 7 These data testify to the demand for affordable, private or charity places for unstable members of the middle-class, later expressed in the popularity of the Holloway sanatorium (Shepherd, 2007).
The distribution of medical patients across individual institutions goes some way to conceal their geographical spread, which broadly conformed to the overall distribution of practitioners and students across England and Wales. Around a third of all practitioners and students were located in London or its constituent counties of Middlesex, Surrey and Kent, as were just under a third of medical patients. Yorkshire and Lancashire also featured concentrations of resident doctors; the former is somewhat over-represented as the destination for medical patients, while the latter is under-represented. Numbers for other counties are rather too small for firm conclusions. Therefore geographical spread alone does not hint at regional or local foci of stress in the medical marketplace.
Medical patients in the West Midlands in England
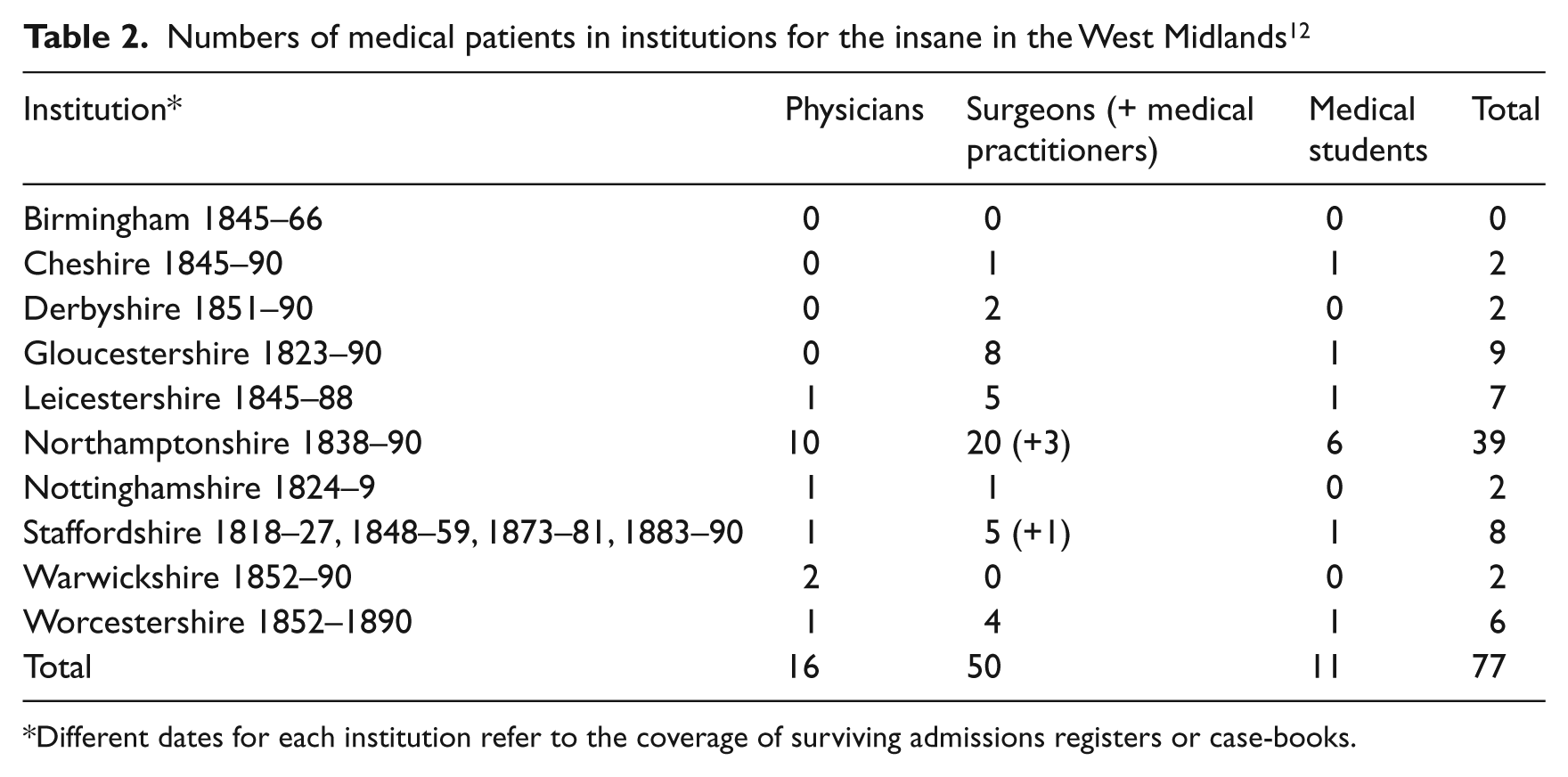
The admissions registers and case notes of nine county asylums and one city institution, all in England between Gloucestershire in the south and Cheshire in the north, have been analysed to learn the details of medical cases for all years for which records survive, up to 1890. These hospitals were chosen for the quality of their records, their representation of different types of institution, and their geographical contiguity. Nine were founded as county or city pauper asylums. Cheshire, Gloucestershire, Leicestershire, Nottinghamshire and Staffordshire asylums were created under the auspices of the permissive legislation of 1808. Those in Birmingham, Derbyshire, Warwickshire and Worcestershire were founded following the statutory requirement to make provision for the insane from 1845. Northamptonshire’s St Andrew’s Hospital was different, in that it was both a charitable foundation and the first de facto county asylum without conforming to either the 1808 or the 1845 Act (Smith, 2007). Admittedly a mixed-funding model incorporating charity was used in Nottingham, but the Northampton hospital was funded exclusively by charity and was explicitly designed to benefit the middle and upper classes, to spare them the ignominy of the pauper institution. 8 As a result of this policy, St Andrew’s made a significant difference to the supply of places available to medical patients and accounted for 40% of all the medically-related admissions in these asylums.
In studying institutions catering to contiguous counties, it was initially intended to maximize the chance of witnessing not only admissions but also transfers between asylums and so following cases across different institutional regimes. This phenomenon was evident from the medical cases, but in the event it proved more likely to involve institutions outside the counties under study. 9
The 77 admissions in Table 2 related to 75 individual medical men who experienced life in one of these asylums. 10 There are some distinctive features of practitioners’ tenure as inpatients which mean that they tended to fit one of three models of institutional career. One was the short-lived stay prior to death; 29 men were admitted and died within six months (although typically within a much shorter time). One example of this trajectory would be Henry Day, a surgeon admitted to the Leicester Asylum in March 1859, who died on 7 May in the same year. He was in all likelihood suffering the final stages of tertiary syphilis, for which the cause of death was typically denoted ‘general paralysis of the insane’ or GPI. The second model was a short- to mid-length stay of up to two years, when the patient was discharged relieved or cured, or transferred to an alternative setting; this was the experience of a quarter of the men. Angus Cameron stayed in the Warwickshire Asylum for over seven months, and on his discharge found his way back to medical practice in Somerset. The third model was of the long-stay resident, who remained in the same institution for five years or considerably longer, and a third of the patient-doctors endured this. Henry Holman, for instance, was admitted to the Northampton Asylum aged 43, and he remained there for the next 30 years until his death in 1912. 11 This pattern means that if doctors did not die quickly after admission, or recover quite promptly and obtain discharge, they could expect a very protracted institutional stay. In this respect the experience of medical patients was starkly at odds with the general patients at the Buckinghamshire Asylum, where half were eventually discharged (most within 12 months of admission) (Wright, 1999: 108).
Numbers of medical patients in institutions for the insane in the West Midlands 12
Different dates for each institution refer to the coverage of surviving admissions registers or case-books.
Medical patients were shunted between county asylums, private houses and family care in exactly the same manner as their non-medical counterparts. Thirty-five or nearly half of all medical patients had some experience of another mental health setting (by the definitions of the day). Three were detained in gaols or workhouses prior to asylum admission, while a further five had been admitted to Bethlem or to a county asylum before being transferred to a West Midlands hospital. 13 Sixteen stayed in a private or licensed house before removal to a county asylum. On departure, 15 were transferred from a county hospital to a different setting, ranging from a union workhouse to the Holloway Sanatorium. The most travelled of the doctors identified here was Paris Bradshawe, who by the age of 30 had already been admitted to five different establishments in the south-east of England, including Bethlem and a private house at Epsom.
The professional background and experiences of medical men admitted to asylums cannot be characterized simply. They ranged very widely from the individual who had hardly practised to the high-profile professional. An example of the former was John Daniel who was admitted to the Derbyshire Asylum in June 1853 and may never have practised medicine. The 1851 census described him as ‘M.R.C.S. London not practising’ and his case notes elaborated ‘his attainments are of the most meagre kind. Indeed it is difficult to believe than anyone with his peculiarly slender knowledge should have ever been enrolled as a Member of a scientific body.’ 14 In contrast, Cornelius Suckling was as illustrious as his name was florid. His qualifications were impeccable and the roster of his professional responsibilities was lengthy, including poor-law duties and teaching obstetrics at Queen’s College Birmingham (London and Provincial Medical Directory, 1875: 632). What is clear, however, is that, contrary to Oppenheim’s claim, men who had made a career from the care of the insane were not prominent among the doctors admitted to Midlands asylums. Only one man fits this profile: Edwin Bishop, who ran his own institution for female patients at Culworth Hall near Banbury prior to admission at Northampton. 15
Eleven of the men studied were medical students, predominantly aged in their late teens or early twenties. The aetiology of some disorders suggests that young males are notably vulnerable to the onset of mental illnesses. Men who would be diagnosed in the twenty-first century as schizophrenic or bipolar, for example, might in the nineteenth-century context have been subjected to asylum admission. What is more, in the modern era, medical students are recognized as unduly vulnerable to psychiatric morbidity (Firth-Cozens, 1987: 5). Therefore medical students might be regarded as under-represented among these patients in purely numeric terms, but their relative absence is perhaps suggestive of the differential judgements being made about behaviours among qualified as opposed to unqualified practitioners. Wild, promiscuous or drunken exploits among medical students might be deprecated by their contemporaries but were not necessarily seen as evidence of mental aberration, while similar conduct among established practitioners might be more likely to give rise to suspicions of illness than to condemnation (Waddington, 2002: 48).
The diverse career profiles and backgrounds of these medical patients support the idea that the strains of professional life were diffuse, because no specialism or geographical location proved unduly difficult. The challenges of medicine per se may have been exacerbated, however, by the personalities of the individuals who made it their occupation. In the twenty-first century, there is good reason to suppose that medical training and practice are undertaken by ambitious, competitive and self-critical people who are not always well placed to deal with stress. 16 The detailed evidence of the case notes cannot support a retrospective allocation of personality type (which would perhaps be a more egregious error than even retro-diagnosis) but it certainly provides repeated allusion to the pressures of collaboration or competition between doctors.
Case notes and medical patients
The case notes compiled by asylum superintendents provide one way to assess the reactions of doctors to mental fragility among their peers. Case notes for asylums in the West Midlands were kept patchily from the 1820s and more reliably from 1845; this was similar to the practice elsewhere, since maintenance of a formal case record was desultory until the County Asylums Act of 1845 demanded that one be kept (Andrews, 1998: 257). As with any other source, the reading of case notes must be cautious and critical, preferably augmented by sources relevant to the period before and/or after admission, or by additional constituents of the institutional archive. Disparities can be exposed between different elements of the institutional collection, as between competing interpretations of information at admission, different understandings of mental illness by successive medical super- intendents, or contradictions between warder testimony and patients’ accounts. Andrews (1998: 265) has argued convincingly that the case-note element of a hospital archive will show most reliably the perceptions of the medical officers, and only tangentially or unevenly the patient experience.
The reactions of asylum superintendents to their medical patients were mixed, and seem to have been regulated less by the former careers of their patients than by the perceived likelihood of their recovery. When men were suffering from tertiary syphilis or where admission was swiftly followed by death, there was little prospect of a relationship based on shared education and professional experience. A longer stay and a remission of symptoms, however, offered the opportunity for collaboration over treatment, exchanges of books and ideas, or a form of professional counselling. Charles Herbert was effectively permitted to prescribe for himself on at least one occasion after admission to the Northampton Asylum in September 1862. 17 Both Angus Cameron at the Warwickshire Asylum in 1873 and John Hewitt at Staffordshire 1888–9 spoke to or wrote to their superintendents about their intention to return to practice. 18 The most determined and poignant attempt to restore a medical man to his mental faculties via shared medical knowledge was tried in Derbyshire by John Hitchman, a former student of John Conolly and in 1856 President of the Association of Medical Officers of Asylums and Hospitals for the Insane (Scull, 1993: 246). Hitchman was the superintendent of the Derbyshire Asylum for 21 years and so supervised the admission and ensuing patient career of Frederick Wright, a Derby surgeon who was transferred to the asylum from the town gaol. 19 Wright had exhibited erratic behaviour for some time, but things reached a head when he was bound over to keep the peace towards the other medical practitioners of the town. He believed that his fellow doctors were conspiring against him and he became violent in consequence. He arrived at the Derbyshire Asylum on 11 March 1856 and was still there at the time of Hitchman’s retirement in February 1872.
Hitchman’s case notes suggest that, from the start, he was compelled to manage Wright’s violence towards his fellow patients. From the time of his admission to the early 1860s Wright is recorded as having successfully hit, kicked or knocked down a number of other inmates. He was able to talk sensibly, but the people around him were quickly incorporated into his world view (in other words, implicated in the supposed conspiracy against him) at which point he became a danger to them. In particular, he considered that his good reputation was being maligned. He would approach strangers and expostulate: ‘Why have you traduced my professional character? What have you been saying respecting my midwifery practice?’
20
Hitchman perceived ample grounds for empathy with Wright, as a fellow middle-class professional and a doctor to boot. In October 1858 he reflected:
It is a distressing case – because apart from these especial delusions – that is towards parties for whom he entertains no morbid dislike – he is amiable enough if they speak to him; and as an educated man he feels his detention among illiterate and rude paupers to be a cruel act; I consult his feelings as far as possible because I know that his brain is in a very unhealthy state. I give him his choice of Wards – but in each one, he soon discovers an Enemy – and becomes dangerous from this circumstance.
21
Indeed Wright was capable of such seeming rationality that Hitchman quickly became alerted to Wright’s ability to smear the innocent. Wright would routinely make allegations against his keepers of ‘a serious character’, including the murder of patients who died. He did so ‘with such plausibility, that it requires some investigation to elucidate their real nature’ and as such might genuinely ‘prove dangerous to the reputation of his attendants’.
22
This combination of the prospect of rational conversation and unpredictable aggression eventually took their toll on Hitchman, and by February 1860 he was beginning realize that the amelioration of Wright’s case may well be impossible. In a very personal outburst, quite uncharacteristic of generic case notes, Hitchman wrote:
Daily for more than four years – I have endeavoured by unremitting kindness – by unswerving good humour – by the daily offer of a change of room, of Ward, of scene – by the use of my Library – and every other possible expedient to gain his confidence – but in vain; and latterly he rarely addresses me, by any better term, than ‘Scamp’ or ‘Rascal’.
23
Their relationship broke down entirely in the early 1860s when Wright eventually became violent to Hitchman himself, by hitting him on the neck. Hitchman reacted to this so negatively that it seems he could no longer bring himself to interact with Wright at any level; Wright’s case notes cease on the day after the assault, and are not resumed until 1872 by Hitchman’s successor.
Superintendents would have been justified in viewing their medical charges with some caution, on the grounds of their good education combined with their ability to argue a case. Wright was not the only doctor to cause problems for hospitals by damaging and plausible allegations. Charles Beard was admitted to St Andrew’s Northamptonshire in 1886. 24 He had been in general practice at Brighton and was said to have been suffering from some disturbance of mind for the previous 15 years (although he had never before been admitted to an institution). He had become convinced that he was the subject of a conspiracy (masterminded by another Brighton doctor) arising from an increase in deaths following vaccinations in his district. The police, the post office, the local curate, Lord Brownlow and eventually his family were all implicated in the supposed conspiracy. At the time of his admission he was described as ‘courteous, affable and highly intelligent. He converses freely and quite rationally upon all general topics & most of the incidents of his past life’. In 1889, however, he caused significant problems for the hospital when he reported to the House Visitors that a named patient had been assaulted by the attendants shortly before his death, and miscellaneous others were victims of employee brutality. The allegations were proved groundless, but still gave rise to serious enquiry.
Wright and Beard represent two well-documented examples of practitioners whose delusions circled around conspiracy, professional jealousy, and allegations of wrong-doing by colleagues, but they were by no means the only men to suffer such apprehensions. However, the clarity of patient voices in such instances is always suspect, being muffled, mediated or silenced (in Wright’s case) by their medical superintendents.
Patient voices and the press
The reactions of doctors themselves to their confinement, especially if they were adverse or negative, must largely be sought beyond case notes since the official institutional transcript was unlikely to record them. There are occasional hints that patients perceived their admission with resentment. Herbert Williams at Gloucester initially refused to eat ‘while in this Bastille’, so invoking the standard nineteenth-century motif of oppression. 25 Some also apprehended forces detrimental to their medical identity. Cornelius Suckling at Warwick tried to reason with his keepers on the grounds of lost income; ‘he asked if he could not get out as he was losing £1000 a year by remaining here’. 26
Yet a very negative response to asylum admission might plausibly be deemed rational (both from a modern and a contemporary perspective, given the Victorian preoccupation with potentially false asylum detentions), and one doctor took up this issue passionately as both a practitioner and a sometime patient. Francis Fox spent 14 months in the Nottinghamshire Asylum. He could not be identified in the asylum case-books (which survive only for 1824–9) and so does not feature in Table 2; instead, evidence of his experiences derives largely from his letters to the press. 27 Fox was a high-ranking member of the Derbyshire medical fraternity, as a physician who held an honorary appointment at the Derbyshire Infirmary in the mid-1830s. He hailed from an established local family; his father and namesake had been a Derby doctor and two of his three brothers were also practitioners in the locality. Fox wrote a number of articles for The Lancet and was noted for the interest he took in the working class. 28
However, his reputation and standing underwent drastic revision in 1836 when he started to make complaints about the conduct of the infirmary. His concerns were initially treated with the utmost care and inspired some enquiries about the treatment of both servants and patients in the Derbyshire Infirmary, but by the end of June the hospital’s weekly board was beginning to react to Fox cautiously. Fox for his part mobilized the considerable following which he enjoyed among the working people of Derby to ensure their vocal support for his complaints. The infirmary board took drastic action and held a special general meeting on 2 August to propose the motion that Dr Fox be removed as a physician and governor, and his subscription be returned. The motion was carried by 53 votes to 14. There was then some debate at the infirmary about the legality of Fox’s removal, in which Fox was publicly defended by his younger brother Douglas, but it was finally confirmed by a repeat vote in September. 29
His public loss of face must have been difficult enough, but Fox’s family was also about to move against him. Douglas seems to have become alarmed by Francis’ behaviour, and eventually this concern gave rise to the latter’s admission to the Nottinghamshire Asylum in late autumn 1836. Fox’s subsequent, detailed account of what occurred between the summer of 1836 and his release in December 1837 cannot be corroborated, but nonetheless he made a powerful, lucid and very public statement of wrongful restraint. Fox wrote a series of over 20 letters and articles on the subject, published in The Satirist between November 1838 and December 1839. 30 The choice of such a notorious mouthpiece may not have helped to agitate widespread support among the reading public. Indeed, his revelations seem to have generated no interest in the remainder of the lay press. Yet across his collected writings Fox provides a coherent account of the controls placed on him at home and later his appalled reaction to the Nottinghamshire Asylum. According to his recollection, on 10 August 1836 his brother Douglas suddenly began to treat him as though he were insane, specifically by locking him in a garret room and using bolts, bars and handcuffs to ensure he remained in his room and strapped to his bed. Fox claims that his friends were not permitted to see him and that at least one ‘keeper’ employed by Douglas was turned away, from an unwillingness to impose such a drastic scheme of restraint. This treatment allegedly persisted for 12 days, whereupon Douglas is said to have sent Francis to Barrow upon Trent for the restoration of his health in the hands of a ‘keeper’. This arrangement persisted until 6 September when he was returned home and imprisoned once more. His amateur confinement ended only when he was conveyed to the asylum at Nottingham on 10 October by another younger brother Archibald Fox (Fox, 1838b, 1839a, 1839b).
Francis recognized absolutely that his own angry responses were liable to be misinterpreted. He postulated:
… if it be granted that it is within the range of possibility that I might have been in my senses all the time, I am fully convinced that every individual action can be shown to be consistent with a man of sound mind, having to deal with almost unheard of persecutions, misrepresentations, and barbarous cruelties! … But when an individual is once stamped with even the name of lunatic, self-defence ceases to be defensible – every resistance is quoted as a proof of insanity. (Fox, 1839b)
He went on to name and shame the doctors of Derby who authorized his incarceration by certificating his ‘madness’, but he reserved his most damning criticisms for the staff of the Nottinghamshire Asylum, superintendent Andrew Blake and surgeon Thomas Powell. Blake he characterized as an army surgeon who obtained his post through patronage rather than ability. Powell was allegedly Blake’s jackal, a failure in private practice ‘who is better suited to certain occupations in the West Indies than to manage the delicate fabric of the mind’. These men were effectually unlimited in their actions, if Fox was right to describe the body of governors as unwilling to interfere ‘from feelings of etiquette’ (Fox, 1838a).
Fox’s version of events is given some confirmation by a letter written in June 1839 by Andrew Blake to the Home Secretary Lord Russell. 31 Blake’s stance is predictably defensive, but he did report that Fox’s brother confined him at home until he became unduly violent, and that Fox was discharged into the care of a brother in London (albeit disputing the circumstances of the release). Furthermore, some of the complaints which Fox had made against employees of the Derbyshire Infirmary, that had initiated the whole series of events, were eventually substantiated. 32 After the late 1830s Fox seems to have retained command of himself, living for some time in Derby and also in Charing Cross. He died at Camberwell in 1860 without apparently having been hospitalized again. 33
Collectively, Fox’s experiences are suggestive of the peculiarly vulnerable position of middle-class medical men once their mental health had been questioned. He was rapidly cast down in the opinion of his social and medical peers, so that in June he was seriously regarded as a physician and a man but by October he could be certified insane by his former colleagues (who were also, as Fox pointed out, his rivals for business). This is arguably an early demonstration of the high standards demanded of the personal and professional conduct of medical men. There was apparently insufficient room for eccentricities or erratic behaviours by Fox to be accommodated by his family or his acquaintances in Derby – he must either be treated as an equal or labelled as a madman. Ironically his reputation was rehabilitated for posterity, at the celebrations for the 60th anniversary of the opening of the Derbyshire Infirmary. At that safe distance of time, Francis was eulogized as among the men ‘whose souls were centred in their profession, and against whom the tongue of slander could affix no stigma’ (Derby Mercury, 17 Nov. 1869).
Fox’s case was probably exacerbated by his feeling for, and influence among, the working class; Blake’s letter to Lord Russell alleged that Fox had on one occasion assembled a crowd of thousands of Derby’s ordinary citizens, an event which inspired the town to send for military reinforcements from the garrison at Nottingham. The event if not the magnitude of the crowd is confirmed by contemporary newspaper reports (e.g. Caledonian Mercury, 18 Aug. 1836). This raises the possibility that too much sympathy for the poor (especially if expressed in opposition to one’s medical colleagues) could be construed as a form of mental aberration.
Fox’s decision to draw attention to his own asylum experiences was at odds with the reactions of most former patients and their family members. Practitioners and their families attempted to maintain a public face of probity, sanity and competence even where this was a poor reflection of a person’s perceived mental state. There was nothing to prevent the public maintenance of a professional presence while not actually capable of practice. Charles Beard, mentioned above, was admitted to St Andrew’s Hospital in Northampton in 1886, was moved to an alternative asylum at the suggestion of the Lunacy Commissioners in 1889 ‘not improved’, and he died at the Holloway Sanatorium in 1916. 34 Yet his family kept up his entries in the medical register throughout his terms as an asylum patient. 35 After he had effectively ceased to practise, there was no reason for his repeated listing. Indeed, continued inclusion in the register, and updating the entry, took a modicum of effort. But there was nothing to require the exclusion of a man by reason of illness. It was perhaps presumed that recovery was possible, and that any return to home life or even to work would benefit from continuous representation on the register. Absence from the register during life might also look as though a doctor had been subject to formal removal under the disciplinary processes of the General Medical Council, and so reflect poorly on his character, while continued presence might yield rewards for the maintenance of professional visibility. Even so, continued inclusion could also be construed as fairly misleading. Beard, for instance, was listed at home in Brighton for the 1887 register (a year when he plainly spent the majority of his time at St Andrew’s). His address was given as a private house in Shepherd’s Bush throughout the 1890s and into the twentieth century (when it is highly questionable whether he was living at home), but he or his family did not balk at giving his address as Virginia Water in 1915, presumably a concession to his admission to Holloway. At his death his son Hugh assiduously published an obituary listing Charles’ qualifications and appointments but making no allusion to illness or even effective retirement (The Times, 26 Dec. 1916).
The reaction of the broader public to these medical admissions, among contemporaries who might be patients but never fellow practitioners, can only be recovered partially and by inference. After all, there was hardly any reason why one person’s admission to a hospital would give rise to a newsworthy report, except in the most dramatic of circumstances (as was the case with the murder committed by James Pownall, cited above). Consequently, discernible reactions arise only where a practitioner’s illness was forced upon public notice, where asylum admission gave rise to immediate or eventual public consequences. The two physicians admitted to the Warwickshire Asylum provide some of the only evidence available here. Cornelius Suckling held a variety of official posts at the onset of his illness, among them the role of medical officer to the Birmingham Bluecoat School. Given Suckling’s prolonged absence from home, he had to be replaced in his multiple official roles, but nowhere in the Birmingham press was his ‘serious illness’ given further elaboration (e.g. Birmingham Daily Post, 22 Apr. 1876). Reportage surrounding the death of Angus Cameron is even more poignant. After his departure from the Warwickshire Asylum, Cameron pursued a successful career in Bath, first by gaining a post at the Batheaston dispensary and later in private practice. But his mental health obviously remained fragile because in 1878 he took hydrocyanic acid and successfully committed suicide. The inquest heard evidence from Cameron’s brother Alexander, who reported that Angus had been ‘under restraint’ in 1872 (actually in 1873) following the death of his only two children. The jury found that he had acted during ‘temporary insanity’, clearly a misnomer whatever the conventions in relation to suicide verdicts at this time (Bristol Mercury and Daily Post, 27 July 1878). Reports of the inquest beyond the local papers for Bristol suppressed the references to his period of mental illness. The Times (22 July 1878: 7) went so far as to claim that ‘None of his friends had the slightest suspicion that his mind was affected’. This admittedly slender evidence begins to suggest that wherever information about the jeopardized mental health of a practitioner was somewhat propelled into the public, the press did nothing to capitalize on it and may have actively occluded the facts. Even if this is a fair inference, though, it remains unclear whether doctors’ ill-health was shielded from motives of class-cohesion or whether this sort of protection was specific to the medical profession.
Conclusion
A tiny proportion of medical practitioners experienced life as a patient in an asylum, but this group is significant because it represents some dimensions of the difficulties facing doctors in a period of professionalization. It is clear that these men were admitted to a range of institutions, but that assumptions about the preference for private licensed houses over charity hospitals or ‘pauper’ asylums can be confirmed. Doctors who treated the insane were no more at risk of serious mental ill-health than their fellows.
Medical superintendents of asylums who found themselves responsible for the treatment of their former colleagues exhibited a fairly muted response to medical patients who were not likely to recover. Unusually John Hitchman became significantly engaged with his patient Frederick Wright. The stormy and sudden ending to their shared experience is perhaps a testament to the challenges facing any arrangement other than a clear division between doctors and patients, no matter what their former occupations. Medical patients could, and sometimes did, express considerable aversion to their institutional surroundings, but only Francis Fox was fortunate enough to secure his release and then find a public outlet for his anger. The potential gravity of his account was dissipated, however, by the fact that his correspondence was supported by a satirical, lay publication rather than in any medical journal. Indeed, the medical and other periodical press alike seems to have given no additional attention to Fox’s barrage of letters in The Satirist.
Wright and Fox are the two most prominent examples of asylum admission under substantial external coercion (one was delivered from gaol, the other forcibly admitted by his brothers) and both men expressed vocal or violent resentment towards medical colleagues as complicit in their diagnosis and detention. The inter-personal competition that was an inherent feature of the medical marketplace was intensified in these two men’s perceptions to assume an overwhelming character. It was not the specifics of their practice, but rather the pursuit of medicine per se that informed their obsessions.
The seeming lack of public notice for Fox’s story in the 1830s, and his ideological inclusion in the medical fold in Derby after his death, is echoed by the way the press avoided drawing undue attention to the instability or prior incarceration of the two physicians at Warwick in the 1870s. Practitioners themselves and their families may have been highly protective of their professional reputations, to the extent of maintaining representation on the Medical Register when most or all future prospect of practising medicine had disappeared, but the press and public were not necessarily seeking every opportunity to undermine them. Indeed, they may have been similarly if not equally anxious to shield doctors, or the professional middle-classes more widely, from personal criticisms. If this is an accurate reflection of the attitudes of both practitioners and patients, of investment on both sides, it would suggest that the process of rising status in medicine was promoted by failure, as well as by success. Success received plaudits, and failures (here, the perceived failure to maintain sanity) encouraged complicity and silence, an absence of prurient inquiry and a willingness consciously to gloss misfortune.