
Abstract
We compared admission rates and outcomes for bipolar disorder patients using the medical records of patients with a first hospital admission in 1875–1924 retrospectively diagnosed based on International Classification of Diseases (ICD)-10 criteria, and patients with a first admission in 1994–2007. The incidences of first admissions in the historical and contemporary periods are comparable: 1.2 and 1.3 per hundred thousand per year, respectively. Manic episodes constituted a greater proportion of admissions historically, while depressive episodes made up more in the contemporary sample. There is no evidence for a reduction in the mean inter-admission intervals with duration of illness. This study suggests that modern treatments may have decreased lengths of stay in hospital, but at a cost of contributing to more admissions. It also points to a shift in the threshold for admissions.
Introduction
The utilization of services for mental disorders in North Wales followed the trend of the UK through the nineteenth and twentieth centuries, with the commonest admissions in the asylum population being for schizophrenia and related psychoses, along with severe unipolar and bipolar affective disorders (Harris et al., 2005).
A comparison of contemporary and historical epidemiological data offers the opportunity to track the evolution of mental disorders in terms of their diagnostic categorization, incidence, prevalence and service utilization in a population. It also opens a window on the impact of advances in treatment with psychotropic medications on service utilization.
North West Wales (NW Wales) offers an exceptionally good opportunity to use historical data to shed light on current approaches to the management of a range of mental disorders, including bipolar disorder. In comparison with elsewhere in the UK, NW Wales has not seen a general rise in its population in the last 120 years. A census of the population broken down by age in 1891 showed that there were 232,000 people and in 2001 there were 235,452 in the same area (Healy et al., 2001). Also, in other parts of the UK, there have been population shifts to urban areas over the past century, making it difficult to draw a direct comparison between admissions to a rural asylum about 100 years ago and contemporary admissions to an urban district general hospital unit. These shifts did not happen in NW Wales (Healy et al., 2001).
This study focuses on bipolar disorder, manic-depressive illness, perhaps the most iconic medical disorder. We have analysed admissions from NW Wales to the North Wales asylum at Denbigh from 1875 to 1924 and compared the results with admissions to the corresponding district general hospital unit from 1994 to 2007. We have also profiled historical and contemporary bipolar patients by age, gender and sex, along with lengths of hospital stay and outcomes.
Methods
The datasets used to look at admission rates and outcomes for bipolar disorder were drawn from the periods 1875–1924 and 1994–2007. In NW Wales, geographical and financial constraints ensured there was nowhere else for nineteenth- or twentieth-century patients to be admitted other than the asylum at Denbigh. With the closure of this asylum in 1995, the District General Hospital unit in Bangor, which was opened in 1993, became the only place for admissions in NW Wales. There are no private facilities or alternative public facilities for patients. Furthermore, patients from NW Wales who became mentally unwell elsewhere, in both historical and modern periods, have normally been returned to the area for treatment.
The datasets
The historical dataset consists of all admissions from NW Wales to the asylum at Denbigh between 1875 and 1924. The asylum records offered the following sets of information relevant to diagnosis: medical and legal certificates outlining the circumstances of detention and mental state features; standard demographic data including age, sex, education, employment and marital status, family history of mental illness, prior mental or physical illness and possible triggers to the disturbance; standard assessments of dangerousness, suicidality, seizure-proneness, along with food refusal and a range of clinical features; descriptions of patients’ mental and physical states on admission; and case notes covering patients’ stays in hospital until discharge or death. It was also possible to trace records back to 1865 to ensure there were no earlier admissions and to track subsequent admissions through to 1965.
The records were made available to a panel of psychiatrists who determined the retrospective diagnoses based on ICD-10 criteria. In the case of the contemporary patients, data were collected up to the end of 2012. Hence diagnostic judgements were made on the overall career of the patients rather than limited to details of the presenting mental state. The panel consisted of psychiatrists currently covering the same catchment areas as those from which the historical patients would have come. This meant that whatever biases an individual consultant had in determining diagnosis applied to both the historical dataset and the contemporary dataset.
These retrospective diagnoses – which included bipolar disorder, schizophrenia, delusional disorder and other non-organic psychoses as well as mood disorders, neurotic disorders and conditions with an organic origin – were made before the beginning of this study. The bipolar episodes were coded as depressive (F31.4, F31.5), manic (F31.1, F31.2), mixed (F31.6), postnatal and unspecified (F31.9). The diagnosis of bipolar disorder in both the historical and contemporary datasets refers exclusively to bipolar I disorders.
Analysis
For the purpose of this study we included in the historical dataset only those patients with diagnoses of bipolar disorder and specifically those who had their first admission from 1875 to 1924. We were able to determine 5- and 10-year outcomes from the date of first admissions for these individuals. For the contemporary sample, all bipolar patients with first admissions occurring between 1994 and 2007 were included in the 5-year follow-up analysis. Ten patients were excluded from the 10-year follow up analysis because of missing data. Census data from the Office of National Statistics (ONS) were used to standardize the datasets from which the mean and median incidence of first admissions were calculated.
An initial analysis of the mean and median length of stay in hospital included all bipolar patients in the historical data. A subsequent analysis excluded patients who had admissions lasting more than five years including significant periods when their bipolar disorder was in remission. In these cases, the admission was sometimes prolonged because of chronic medical conditions such as tuberculosis and sometimes for social reasons rather than for symptoms of bipolar disorder.
We analysed the length of illness as well as the number of days spent in hospital. In the historical group this meant adding the illness days before admission and estimating from the case notes when the patient went into remission. Patients in the historical period often spend weeks or months in hospital after recovery. For the contemporary group the records do not reliably reveal when an episode began or ended. We also analysed the mean inter-admission intervals. A majority of the individuals in each cohort had three or fewer admissions (corresponding to two or fewer inter-admission intervals) in the sampling period following their first admission. This meant the result was skewed by a reducing minority of patients in both cohorts with a short but stable interval period between successive admissions
To eliminate the skew caused by patients with a lower number of admissions, we excluded those patients in each cohort who did not have a minimum of five inter-admission intervals. This choice was dictated by the modal number of admissions per patient. For the historical cohort, the modal number of patients (n = 14) occurred in those with seven admissions, thus reflecting six inter-admission intervals. For the modern cohort, the modal number of patients occurred in those with seven admissions (n = 16), thus reflecting six inter-admission intervals.
Results
Incidence rates
1875–1924. Using contemporary diagnostic criteria, it was determined that 135 individuals had first admissions for bipolar disorder in this period. Of these, 65.2% were females while 34.8% were males. The mean age at first hospitalization was 36.5 years; it was 35.9 years for females and 37.8 years for males, with a median age for both genders of 35 years. The ages at first admission ranged from 16 to 73 years, but 53% were aged 20–39 years on first admission, 7% were aged below 20 years, 26% were aged 40–49 years and 14% were aged over 50. The mean incidence of first admissions was 2.7 per year, or 11.64 per million per year–an incidence rate of 0.0012%.
1994–2007. The contemporary sample was made up of 43 patients who had their first admission for bipolar disorder in this period. Of these, 58% were female and 42% male. The ages at first admission ranged from 19 to 62 years. The mean age at first admission was 33.4 years; it was 33.7 years for females and 33 years for males, with a median age for both genders of 32 years. A majority (74.4%) were aged 20–39 years on first admission; 2.3% were aged below 20 years, 14% were aged 40–49 years and 9.3% were aged 50 years and above. The mean incidence of first admissions for bipolar disorder in this cohort was 3.07 per year, or 13.04 per million per year, an incidence rate of 0.0013% (see Table 1).
Service utilization 1875–1924 and 1994–2012 compared.

Hospitalization prevalence rates
1875–1924. The rate of admissions within 5 years of the first hospitalization differed between the two cohorts. For the historical sample, 135 patients had a total of 209 admissions, with a mean of 1.5 admissions per patient in 5 years (median 1). In 10 years this cohort of patients had a total of 272 admissions, with a mean of two admissions per patient in 10 years (median 2). The total number of admissions from the bipolar patients admitted in this period was 440. Hence, cumulatively, this cohort had on average 8.8 admissions per annum. This represents a service utilization rate of 37.9 admissions per million per annum, or 0.00379%.
1994–2007. In contrast, the 43 patients in the contemporary sample had a total of 164 admissions within 5 years of their first admission, with an average of 3.81 admissions per patient (median 3). The 33 patients in this cohort who were followed for up to 10 years had a total of 209 admissions, with a mean of 6.3 admissions per patient in 10 years (median 4). This represented a 3.1-fold increase in admissions per patient with bipolar disorder in the contemporary sample when compared with their historic counterparts. The total number of admissions from this cohort between 1994 and 2012 was 325. Hence, cumulatively, this cohort of bipolar patients had on average 17.1 admissions per annum. This represents a service utilization rate of 72.6 admissions per million per annum, or 0.00726%.
Length of hospital stay
1875–1924. Historically, patients generally remained in hospital after recovery from an episode of bipolar disorder, sometimes for months, for a variety of reasons. These included inadequate social support in the community or chronic medical conditions. Furthermore, following recovery, patients were allowed home on extended leave lasting months before they were officially discharged. All these factors mean that the period of hospitalization does not necessarily reflect the duration of illness, which might be considerably shorter. A period of hospitalization might also represent multiple episodes of relapses and remissions.
For the historical cohort (n = 135), over the first 5-year period the mean number of days spent in hospital in total for each patient was 587 days (median 375) and the mean duration of illness was 444 days (median 240). During the 10-year period, the mean length of stay for each patient was 1025 days (median 579) and the mean duration of illness during this period of hospitalization was 624 days (median 336).
The data on this cohort was subsequently re-analysed excluding 21 patients whose case notes revealed extensive periods of admission lasting more than 5 years with bipolar disorder in remission for a significant part of that time. In these cases the admission was prolonged because of a chronic medical condition, such as tuberculosis. Re-analysis revealed a mean 5-year length of stay of 399 days (median 295) and a mean duration of bipolar disorder during the hospitalization of 284 days (median 211). In 10 years, the mean length of stay was 608 days (median 423), while the mean duration of illness was 396 days (median 311).
1994–2007. The mean number of days spent in hospital in total for each patient in the contemporary sample in the 5 years (n = 43) after first admission was 124 days (median 93) and in 10 years (n = 33) was 210 days (median 158). Analysis of this group revealed that they were ill for the total duration of admissions, albeit in a recovery phase prior to discharge, with no indicators as to how long they had been ill beforehand. Duration of admission does not represent the full duration of the illness.
Comparative mortality
In the historical cohort, there were 10 deaths within 5 years and 15 deaths within 10 years of first admission, representing 11% of patients. The deaths were from TB (2), heart disease (4), pneumonia (4), cancer (1) and exhaustion (4). In comparison, 28% of schizophrenia patients from this same historical cohort died within 10 years of their first admission, almost half of whom died from TB (4). In the contemporary cohort, there was one death in 10 years, from respiratory disease, with no deaths occurring in the first 5 years. This again contrasts with the deaths among schizophrenia patients admitted for the first time between 1994 and 2010 to the same unit, where there were 11 deaths in the first 5 years, 10 of which were suicides (Healy et al., 2012b).
The role of gender
The 88 women in the historical cohort had a total of 142 admissions (mean 1.61) in 5 years and 184 admissions (mean 2.09) in 10 years, with an average length of stay in hospital of 610 days in 5 years, and 1015 days in 10 years. Their mean duration of illness while in hospital was 444 (median 258) days in 5 years, 637 (median 358) days in 10 years. Excluding the 12 chronic patients aforementioned, the total number of admissions for the remaining 76 female patients was 122 admissions (mean 1.61) in 5 years and 164 (mean 2.16) in 10 years; the mean duration of illness was 306 (median 228) days in 5 years and 407 (median 319) days in 10 years.
The 47 men had a total of 67 admissions (mean 1.43) in 5 years and 88 admissions (mean 1.87) in 10 years with an average length of stay in hospital of 544 days in 5 years and 1046 days in 10 years. Their mean duration of illness while in hospital was 444 (median 212) days in 5 years, 600 (median 304) days in 10 years. Once again excluding the 9 chronic patients from this group, the remaining 38 male patients had a total of 54 admissions (mean 1.42) in 5 years and 75 admissions (mean 1.97) in 10 years, with a mean duration of illness of 240 (median 166) days in 5 years and 375 (median 287) days in 10 years.
In the contemporary cohort, with a mean duration of illness at least the same or possibly longer than the hospital stay, the 25 females had a total of 80 (mean 3.20) admissions in 5 years with an average length of stay in hospital of 109 (median 78) days. The 18 females with a full 10-year history (i.e. first admitted after June 2003) had 97 (mean 5.39) admissions in 10 years, with a mean duration of illness of 179 (median 135) days in 10 years. The 18 males had a total of 84 admissions (mean 4.67) in 5 years with a mean duration of illness of 144 (median 110) days. The 15 males with a full 10-year history had 112 admissions (mean 7.47) in 10 years, with a mean duration of illness of 246 (median 158) days in 10 years.
Mania–depression balance
Manic episodes constituted 62.5% of the first admissions in the historical cohort, while depressive episodes made up 17.0%. In the 10 years from first admission, 67.5% of the historical episodes were for mania and 17.7% were for depression. In the contemporary cohort 60.5% of the first admissions were for a manic episode, while 34.9% were for depression. The mixed episodes and postnatal episodes were 2.3% in each group. In the 10 years from first admission, 45.9% of the admissions were for manic episodes, while 49.4% were for depressive episodes (see Table 2).
Profile of bipolar episodes 1875–1924 and 1994–2012 compared.

Inter-admission intervals
Analysing all inter-admission intervals in the historical cohort shows a continuous decrease in the mean inter-admission interval in the cohort from 1750 days for the first interval to 934 days for the fourth interval. In the contemporary cohort, there is a comparable overall trend with time, as can be seen in Figure 1.
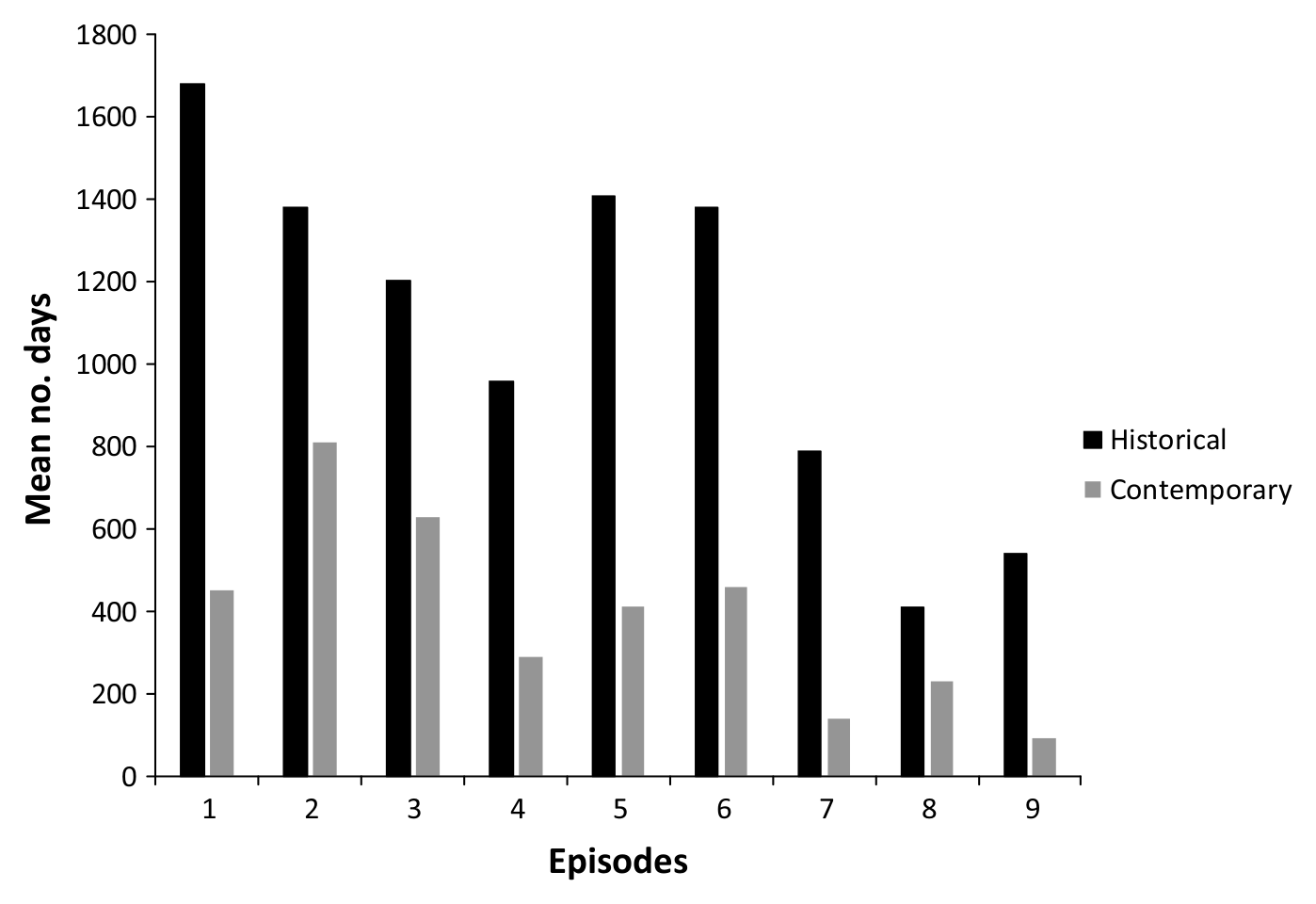
Comparative mean inter-admission intervals.
To test whether the reduction in inter-admission interval with time is an artefact because the majority in each cohort (58% for the contemporary group and 90% for the historical group) had two or less inter-admission intervals in the period following first admission, we excluded all patients with less than five inter-admission intervals. When this is done, the results do not reveal a decline in mean inter-admission intervals over time in either the historical (n = 14) or the contemporary sample (n = 16), as shown in Figures 2 and 3. The inter-admission intervals are markedly longer in the historical cohorts when compared with the contemporary cohort.
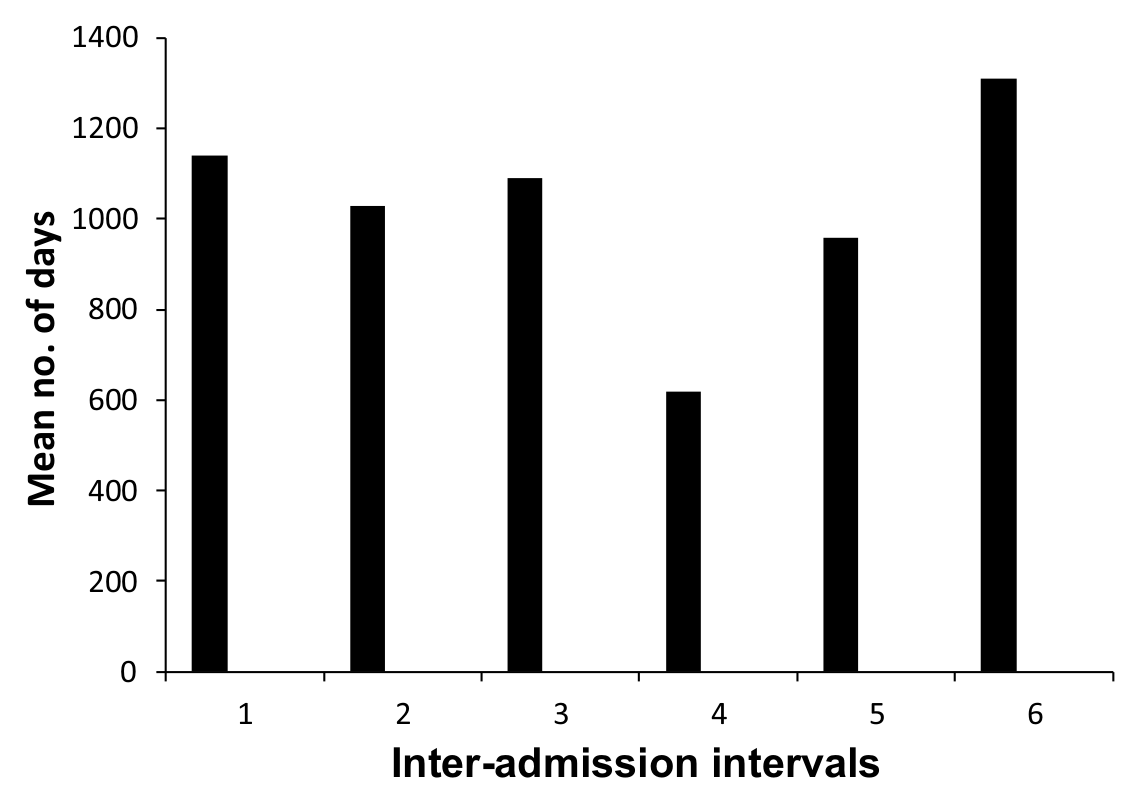
Mean inter-admission intervals of historical patients with a minimum of seven admissions.

Mean inter-admission intervals of contemporary patients with a minimum of seven admissions.
Discussion
This study has been conducted against a backdrop of an increasing interest in bipolar disorder. This interest has led to a range of studies in other parts of the world which have noted wide variations in the incidence of bipolar affective disorder: from 1.7 to 20.0 per 100 000 per year (Daly et al., 1995; Lloyd and Jones, 2002; Lloyd et al., 2005; Rasanen et al., 1998). The incidence of hospital admissions in this sample falls at the lower end of this range. This is probably to some extent a consequence of the study methods used. Looking at cases with confirmed episodes of bipolar disorder and tracking cases over a relatively short time frame of 10 years is likely to miss cases of unipolar disorder who convert to bipolar disorder.
We have studied rates of both unipolar depression and schizophrenia in the same historical and contemporary samples using the same methods, and these are close to five times higher than the bipolar admission rate (Harris et al., 2011; Healy et al., 2012a). The readmission rates of bipolar disorder patients were higher than for unipolar depression or schizophrenia in both historical and contemporary samples; bipolar disorder patients are ‘noisier’.
It is of interest that our contemporary hospital admission incidence of 1.34 per 100,000 per year is similar to the historical incidence rate. Possible factors that have conserved incidence rates over time are the very low number of migrants in this population, a single point of access to services, a predominantly rural population and consistent diagnostic and admission thresholds amongst psychiatrists. Another factor is that we have excluded patients from both historical and contemporary samples who have presented with a single manic episode. Unlike the Diagnostic and Statistical Manual of Mental Disorders (DSM), ICD-10 does not force a diagnosis of bipolar disorder in these circumstances, and the small number of cases involved appeared to be acute and transient psychoses rather than enduring disorders.
The age and sex profile of the patients in the historical sample maps onto the profile outlined by Kraepelin (1896). The profile is also very similar to the profile we established in a cross-sectional study of admission prevalences during the 1890s compared with the present day (Healy et al., 2005). This study had a larger contemporary sample as it included all admissions rather than just incident admissions.
As regards admission prevalence, this is increased in the modern sample. In part this is simply because historical patients spent more time in hospital, which means they had less time at home from where they could be readmitted. Related to this, several contemporary admissions may stem from one illness episode. It is clear that patients today, when stabilized on treatment, are often discharged before the illness episode has remitted. In the case of contemporary admissions, the medical records give no indication as to the duration of the current episode. It is not possible therefore to extrapolate figures for the frequency of illness episodes from these figures for admission prevalence. These considerations play a part in assessing the role of treatment today. Psychotropic medications clearly enable earlier discharges, but do not appear to forestall admissions. Whether the increased frequency of admissions is due to a less frequent use of mood stabilizers other than lithium during this period in North Wales compared with elsewhere is unclear. It is possible that a relatively common use of antidepressants may precipitate rapid cycling in some cases (Ghaemi et al., 1999).
Some other possible factors to consider are the possibility of reduced compliance of patients with medication during the inter-admission intervals and also the fact that these findings for bipolar disorder are comparable to findings for the other major psychiatric syndromes studied in this sample. We have found an increased admission prevalence for patients with schizophrenia and unipolar mood disorders also (Harris et al., 2011). This increased service utilization for psychiatric syndromes in general overlaps with increases in service utilization in the other specialties of medicine. Hence, a set of general health factors in addition to any specific bipolar disorder factors may be at play in producing at least part of the change reported here (Healy et al., 2001).
A further factor lies in the nature of the episodes that lead to admission. While manic episodes consistently remained the commonest reason for admission in the historical patients, it is the commonest reason only for first admissions in the contemporary patients. In this cohort, depression afterwards becomes more prominent as a reason for admission. The depression cases that are admitted now may well be suicidal but in general not psychotic, compared with depressive admissions during the historical period. This suggests a shift in the threshold for depressive admissions. This increase in depressive admissions may also indicate that current treatments are relatively limited when it comes to preventing depressive relapse.
As shown by Figures 2 and 3, the rate of relapse leading to hospitalization does not appear to increase with the number of previous episodes in either the contemporary patients or the historical (pre-lithium era) patients, in contrast with other published studies. These data call for more studies into changes in duration of inter-admission intervals with time.
Among the strengths of this study is the fact that any change in the consistency of a diagnosis of bipolar disorder over time has been limited by the fact that the same set of psychiatrists made the diagnoses in both modern and historical cohorts using the same criteria, thereby limiting initial presentation bias (Kessing et al., 2004; Ruggero et al., 2010). One limitation is that the study was necessarily confined to patients with bipolar I disorder as only such patients were admitted to hospital in the historical period. This has produced relatively small samples. A further limitation is that it was not possible to establish a true illness duration in the contemporary sample.
Footnotes
Conflict of interest
None of the authors has any links to any company making medications for the treatment of mood disorders or to any company engaged in treatment.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.