
Abstract
The article examines the manner in which the learning-disabled subject is created as an object within contemporary psychiatric discourse by means of a genealogical analysis of the learning-disorders in the Diagnostic and Statistical Manual of Mental Disorders (DSM). It investigates how this pathology was formed historically in the text, what metamorphoses it underwent, and their epistemic significance. First, the theoretical underpinnings of the sociological discourse on DSM are presented, giving a brief background of the DSM status in the Israeli context. Many problematic characteristics in the text are unveiled, by means of critiques from sociology, anthropology and discourse studies. Second, the changing definitions and conceptualizations of learning-disorders in the seven editions of the Manual and the accompanying case studies (1952–2013) are examined. It becomes apparent that the disorders have undergone changes that have enabled the biomedical paradigm to triumph. The implications of these transformations are addressed.
Keywords
Introduction
In contemporary Western society, the DSM, 1 published by the American Psychiatric Association, serves as the canonical text for psychiatry and the clinical professions associated with it (Bailey, 2010; Crowe, 2000). The DSM, or, to use its full name, the Diagnostic and Statistical Manual of Mental Disorders, also serves as the main text, as a theoretical and empirical platform, and as a classification guide for the expert diagnosticians of learning-disabilities (didactic-diagnosticians and psychologists) in Israel (Katchergin, 2009, 2012a). The attraction of this text for the clinicians who depend on it in the West and in Israel is based on the claim that it can provide a descriptive, neutral and atheoretical presentation of disorders and mental illnesses (Tsou, 2008).
The aim of this article is to illuminate and examine a phenomenon that has been disregarded to date in both the research and diagnostic literature on learning-disabilities (both in Israel and in Western countries): the transformations in definition and conceptualization of these disabilities 2 as they are reflected in the textual history of the DSM, their epistemic meanings and practical ramifications. This disregard is surprising, for the field of learning-disabilities traditionally rests on the DSM as a scientific linchpin which provides the basis for its main assumptions and thereby advances the practices of identification, diagnosis and intervention that are commonly accepted. The present article will make several contributions. First, by means of genealogical analysis, it will uncover of the changing, vague and contradictory character of the definitions and conceptualizations of the disabilities; this raises crucial questions with regard to some of the central assumptions that are taken for granted in the contemporary field of disabilities. Second, the article will show that the multi-vocal paradigmatic exposure in the first manuals, and the transformations resulting in the triumph of the biomedical paradigm and the expunging of the alternative paradigms from the recent DSM, are indicative of the paradigmatic polyphony that has characterized the historical discourse on this issue; it also hints at the possible future inclusion of environmental paradigms into the contemporary field of learning-disabilities. This rehabilitation of the environmental paradigm for the understanding of the category of learning-disabilities is likely to be not only a historical purging of the category, but also a step towards establishing a more complex model for the understanding of it, a model that also examines cultural, social and environmental aetiology. Such a model is likely to constitute a complex alternative for the hegemonic model of the field of contemporary learning-disabilities: the reductionist and essentialist biomedical model. Third, the findings presented in the article are likely to contribute to the research focusing on sociological, anthropological and discursive aspects of medicine and disease in general and on psychiatric and clinical knowledge in particular. Fourth, sociology and discourse analysis of learning-disabilities are fields that are inadequately covered and undeveloped in the Israeli context. This article attempts to correct this disciplinary lacuna.
The article has two parts. The first sets out the theoretical and methodological basis for the discourse. The assertions presented are from the fields of sociology, the anthropology of medical knowledge and discourse research. In addition, the canonical status of the DSM in the contemporary Israeli context is presented. The broad range of critiques (sociological, anthropological, discursive) relating to psychiatric discourse in general, and to the DSM in particular, reveals the problematic nature of the text which, in the Israeli field of disabilities, is considered canonical and is the symbolic basis for learning-disabilities experts’ legitimization.
The second part presents findings from a genealogical analysis of the editions of the DSM, focusing on the conceptual transformation of learning-disorders and on the process whereby they were consolidated into a contemporary ‘clinical fact’ with clear biologistic characteristics, starting with DSM-IV. This is the first research study that employs this type of analysis to illuminate the conceptualizations of learning-disorders and their historical transformations in the text. The various ideas that emanate from the DSM at various stages of its transformation are shown to advance limited and narrowing biomedical understanding of disabilities at the same time as the ideas which advance environmental understanding are completely excluded.
Finally, I will sum up the implications of the textual construction of the disabled person in relation to the social and educational reality of our time, and particularly the potential ramifications of the transformation of the category of disability in the text on the increasing diagnosis of learning-disabilities.
Sociological and anthropological criticisms of the DSM
There are long-standing sociological and anthropological criticisms about psychiatry and its regulatory and labelling functions. Since the studies by Goffman (1961), Lemert (1967) and Scheff (1967), sociologists have been careful about descriptions of illnesses and psychiatric disorders as ‘natural’ categories, while uncovering the processes of social construction involved in diagnosis and labelling, and have dealt cautiously with social outcomes of exclusionary psychiatric practices like these.
Sociologists of medical and biological knowledge, such as Conrad (2005), Clarke et al. (2010) and Rose (2013), based their views on the conceptualizations of Foucault regarding the medical gaze as expressive of a new discursive historical disposition about knowledge/power (Foucault, 1984), and regarding the reciprocal founding of the science of psychiatry and its objects: ‘disturbed’ subjects requiring diagnosis and treatment (Foucault, 1986). Subscribing to Foucault’s precepts, these authors analysed the manner in which the psychiatric discourse creates an ever-increasing number of behavioural categories that can be subjected to clinical diagnosis, characterized by distinct mental and physical qualities. They argue that the psychiatric discourse has become the main model by means of which people think, experience and understand their problems, their lives and the world. This model confines the understanding of social manifestations to symptoms that are indicative, as it were, of the disorder or illness. Following Zola (1978), this confining conversion of social manifestations to clinical categories has been termed by them ‘medicalization’. In this context, the DSM constitutes an important instrument for promoting the process of medicalization. The symbolic status it enjoys, and the formal standardization of diagnostic criteria it facilitates, make it a professional textual apparatus that promotes the use of names of discrete clinical categories and their dissemination around the world (Clarke et al., 2010). The DSM also assists in allowing psychiatric illnesses to spread and become established, due to its being an integral component in the processes of psychiatric training and clinical work, in insurance procedures and in marketing strategies of pharmaceutical corporations (Rose, 2013). The DSM also serves as a social actor that, on the one hand, expedites the acceptance, by professionals and laymen, of new illnesses encoded in it and, on the other hand, delays the public’s and the experts’ acceptance of illnesses which were not encoded in it (Conrad, 1992). The various criticisms reveal how social and economic interests, as well as various pragmatic and institutional factors, are reflected in the DSM or advanced by it, despite its declared pretensions to be a pure and objective scientific classification system.
Anthropologists of psychiatric and biological knowledge, such as Gaines (1992), Gaines and Davis-Floyd (2004), Kleinman (1997) and Luhrmann (2000) based themselves on analyses of science as a paradigmatic organization of knowledge and practices embedded in culture (Kuhn, 1962), and criticized the universal, positivistic, dualistic and naturalistic assumptions of the psychiatric discourse. In this context, Gaines and his colleagues criticized the DSM for pretensions to be universal, describing it as an ethno-medical classification system embedded in a Western viewpoint, and they analysed its ethnocentric biases (Gaines, 1992; Gaines & Davis-Floyd, 2004). Kleinman (1991) criticized the DSM for enabling diagnosticians to discount the interpretive element of the diagnostic act, to blur the socio-cultural context in which it exists, and to block out the subjective experience and personal significance of difficulties, distress and suffering on the part of those undergoing diagnosis. Ironically, even the attempt to include cultural factors in the DSM, in the form of ‘culture-bound syndromes’, expresses Western bias both in their presentation as exotic and also in the sense that, in contrast to them, most psychiatric diagnoses (those that are, in practice, characteristic of Western societies) are not modified as culture-bound, but are presented in the DSM as culturally transparent, universal and standard (Kleinman, 1997). Luhrmann (2000) placed the DSM in the context of the advance of the psychiatric biological paradigm which rejected the psychoanalytical paradigm and relegated to the sidelines the competing psychiatric paradigms. It is in this sense that the DSM serves as an instrument for advancing and establishing the biomedical model and for advancing reductive understanding of the soul to bio-physiological components. Good (1996) criticized the oppressive logic of the psychiatric classification system embodied in the DSM, the disciplinary work and the labelling carried out through it, and the negative pragmatic ramifications for excluded populations, such as Afro-Americans, immigrants and the poor.
The present article takes a position in the lively theoretical, professional and political polemic about the appropriate location, if any, for the DSM in theory and in clinical practice touching on learning-disabilities, about the extent to which the would-be factual descriptions in this context are credible, reliable and valid; and in relation to its political origins, their social ramifications and their ethical implications. Nevertheless, this article does not attempt to directly shake the foundations of the biomedical model that serves as a theoretical infrastructure for this text, but rather to point out its hegemonic institutionalization (despite its lack of declared empirical validity) in the history of the text and its potential ramifications in this context. The polemic presence in Israel has particular importance, given the background of how the Israeli research and professional literature on learning-disabilities has ignored its existence, at the same time as it bases itself on this text to such a great extent. 3 Equally, it is important to present the biomedical model as one possible paradigm of many, particularly in light of the fact that the research and professional discourse about learning-disabilities in Israel is immured in a biologistic interpretive frame, which excludes alternative interpretive frames (sociological, cultural, psychological, political-economic, historical and environmental).
The Israeli context
In the Israeli context, the DSM serves as a theoretical and empirical platform and as a diagnostic guide for the various clinical professions, including psychiatrists, doctors, clinical and educational psychologists, social workers and diagnosticians who are expert in learning-disabilities (didactic-diagnosticians). 4 In effect, it is the main text whose symbolic authority provides the backing for the field of learning-disabilities in Israel and from which the diagnosticians, expert in learning-disabilities, draw their legitimacy. In the field of learning-disabilities, the DSM is considered to be the canonical text both by researchers and by diagnosticians (Katchergin, 2009, 2012a, 2014a). In their view, this is the text that underpins all aspects of accumulated knowledge about learning-disabilities. For them, its special importance lies in its being a scientific-medical text, that is, a text identified with a body of knowledge and with a profession, which are perceived by them as having overarching authority in definition, profiling, classification and treatment of these disabilities.
The American Psychiatric Association (APA) and its textual validation in the shape of the DSM serve as objects for many references, quotations and citations at conferences devoted to learning-disabilities in Israel, in research and professional literature and in publications of diagnostic and therapeutic bodies. The Ministry of Education, too, has adopted the American DSM’s definition of learning-disability (in practice, learning-disorder). 5 It was further found that many professionals in Israel use the DSM in order to validate their conceptual and practical decisions in the field of learning-disabilities, even when the latter contradict what the text states (Katchergin, 2012a, 2014a). These cases reveal the fact that the DSM has symbolic and authoritative functions for some of the professionals aside from its having value in terms of contents, diagnosis or therapy.
Research type
This research is based on a textual corpus that includes all seven editions of the DSM (1952 to 2013) as well as their casebooks (APA, 1981, 1989, 1994b, 2000). A close analysis of the methods of conceptualization of learning difficulties in the DSM was needed, as well as an examination of the textual methods of structuring these difficulties as categories that signify mental pathology; for this, the methodology of qualitative research was chosen, and particularly that of historical discursive analysis. The historical discursive analysis presented in this research is based on the assumption, following the work of Foucault (1972), that textual categories, such as learning-disabilities, constitute a discursive formation. In this they reflect a certain world-view, participate in the construction of the social reality, and advance a variety of political, social and professional interests (Crowe, 1998).
This is the first research study using this type of analysis to highlight the conceptualizations about learning difficulties in the text being studied, to chart the transformations and historical divisions in it, and to profile the process of their consolidation over time into a present-day clinical and biological fact.
Historical discourse analysis of learning disorders in the DSM
Academic, professional and public discourses have criticized and challenged the appearance of many clinical categories in the Manual, but it seems that the changing categories of learning-disorders have undergone a process of becoming textually permanent, and have become so prevalent (especially in DSM-IV and its revision DSM-IV-TR) that they have become a clinical fact with clear-cut characteristics. Thus, in a genealogical survey of these categories in the DSM, it is apparent that during the last few decades, learning-disorders became established as a ‘fact’ in the American psychiatric professionals’ discourse.
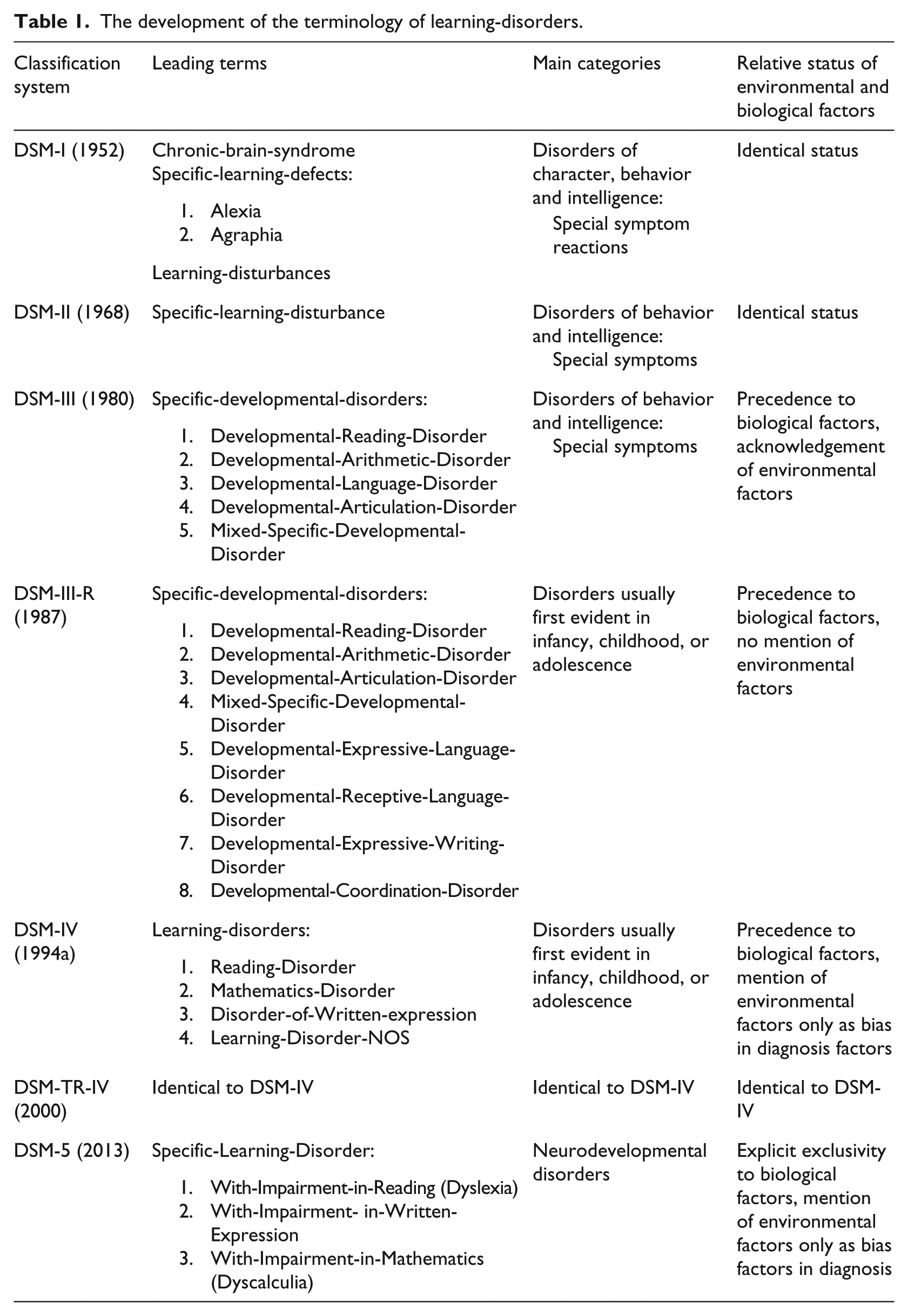
This transition in which they became consolidated as a clinical fact was accompanied by a reduction in the various questions that have appeared explicitly in the DSM itself (questions regarding the various aspect of the particular category) to the extent that the latter disappeared altogether from DSM-IV onwards. This change has been accompanied by conceptual transformations of the category and of the terminology and symptomatology associated with it, as well as by the reorganization of its location in relation to proximate categories in the classification system (see Table 1).
The development of the terminology of learning-disorders.
DSM-I
In DSM-I (APA, 1952) the category of ‘learning-disorders’ is not yet named. Instead, in a conglomeration and with some overlap, the terms ‘Chronic-Brain-Syndrome’, ‘Specific-Learning-Defects’ and ‘Learning-Disturbance’ appear. There is no clear distinction between these three terms and the conceptualizations of them. The Manual itself states (in referring in general to the categorization used in it) that in borderline areas of each term, the groupings could change in accordance with the immediate state of the person being diagnosed, and also in accordance with the nature of the training and skills of the examiner.
Moreover, the terminological system of ‘Specific-Learning-Defects’ is complicated in that it includes sub-categories such as ‘Alexia’ and ‘Agraphia’, the historical antecedents, as it were, of the terms dyslexia and dysgraphia used in our own time. However, it is interesting to note that the term popular today, dyslexia, does not even make an appearance in the body of the Manual, that is to say, the official approved list of clinical diagnoses, although it is nevertheless mentioned in Appendix C to the Manual. In this Appendix of Supplementary Terms, the term dyslexia is mentioned with the laconic clarification: reading difficulties.
With regard to the location of all the ‘Learning-Defects’ in relation to the other disorders in the Manual, they are combined under the clinical grouping of ‘Special-Symptom-Reactions’ in the cluster ‘Disorders of Character, Behavior, and Intelligence’ and ultimately under the syndromes associated with ‘Mental-Deficiency’ or ‘Chronic-Brain’ problems.
A remark distinguishing the ‘Learning-Defects’ from the syndromes adjacent to them points out that they include those whose sources are Unspecified or Nonorganic; that is to say, a specific brain location causing them has not necessarily been located. This remark anticipates the potential for locating and identifying learning-disabilities lacking indications of organic pathology (neuro-anatomic, neuro-physiological or genetic), as well as their potential for symbolic attraction that has been uncovered with renewed vigour in recent years (the vagueness in relation to the existence of an organic defect as the factor that causes learning-disabilities makes these disabilities popular even among those marked by them).
DSM-II
DSM-II was published in 1968 (APA, 1968), five years after Dr Samuel Kirk coined the term learning-disabilities. Despite the rapid acceptance of the term among professionals and parents, it still did not succeed in becoming accepted in the medical discourse. Indeed, it did not appear in this edition of the DSM, but it spread rapidly in the literature of teaching manuals for special education (Hallahan and Mercer, 2002).
DSM-II itself contains changes that constitute an additional stage in the process of consolidation and distinguishing between the various ‘Specific-Learning-Defects’. This term, which has a negative connotation, disappears while its ‘specific’ quality is preserved by being juxtaposed to another (pre-existing) category: ‘Learning-Disorder’. In this way, a new category is formed, ‘Specific-Learning-Disturbance’. The clinical grouping affiliated with this category is disconnected from the cluster of personal disorders and its name is shortened from ‘Special-Symptom-Reactions’ to ‘Special-Symptoms’ only.
These changes were an expression of the rising force of the biological Neo-Kraepelinian paradigm in American psychiatry at that time, and the place of personality disorders originating in psychopathology was delineated. Moreover, learning-disorders became disassociated from them, with emphasis placed on their being distinct clinical entities – both by means of their being qualified as specific, and through deletion of the modifier ‘Reactions’ in relation to them. The source of this reactive terminology was the psychoanalytical paradigm whose influence on American psychiatry was considerable in the first edition of the DSM. In the second edition, on the other hand, a comprehensive effort is made to emphasize the biological sources of the various mental disorders.
Interestingly, despite the above changes in terminology, and in contradiction to the general biologistic trend described, the disorders belonging to the new group of ‘Special-Symptoms’ (including ‘Special-Learning-Disturbance’) are presented as not being the outcome of an organic illness, defect or mental disorder. What is not mentioned, or even hinted at, is their possible origin. These changes, seemingly contradictory, display vagueness about the quality and causes of the learning disturbance – a vagueness that was to resonate in the complex interpretative paradigmatic framework of the field of learning-disabilities and to haunt it into our contemporary extra-textual social context.
DSM-III
In the third edition of DSM, published in 1980 (APA, 1980), additional changes were made in the classification method, the terminology and the definition of ‘Special-Learning-Disturbance’. The conceptual reclassification results in the cancellation of this category and its replacement with a new category of ‘Specific-Developmental-Disorders’. For the first time, the adjective ‘developmental’ is used in relation to learning-disorders; this is an expression of the increasing influence of the developmental biological orientation which identifies ‘delays’ in the specific age-appropriate stages as central to characterizing the disorder. From this point on, the disorder is associated with the ages of childhood and adolescence. Moreover, the new category is subdivided into a collection of affected clinical categories, distinguished by their main learning skills. Five formal clinical entities are formed in this way: 6
Developmental-Reading-Disorder
Developmental-Arithmetic-Disorder
Developmental-Language-Disorder
Developmental-Articulation-Disorder
Mixed-Specific-Developmental-Disorder.
The above five categories are still included in the ‘Special-Symptoms’ cluster. Their special status is emphasized through a sharpening of the distinction between them and the adjacent categories (particularly retardation and autism) by means of a statement that those marked in this way are ‘normal’ (those with defined and specific impaired learning skills). Similarly, for the first time, the diagnostic criteria for identifying learning-disorders are stated: the existence of gaps between the IQ measurement of the subject and his grades in various achievement tests relevant to the skill being tested. A ‘significant’ gap is not decided as long as the grades are lower (or higher) than the intelligence quotient, but only when these grades are not congruent with the ‘expected’ grades of the subject.
This first formulation of the criterion of the ‘gap’ appears in the paragraphs that sum up each clinical category. These passages are distinct from the wording that precedes them in that they are summarized and appear in a square frame with borders on a dark background. However, the presentation of the criteria in them raises many questions, for example: What are the justifications for using the artefact ‘expected’ grade as a comparative measure in relation to the intelligence quotient and the actual grades; and even if this indicator is accepted, how can it be measured? It can be understood from the summary that it is in some way dependent on the quality of learning that the subject benefited from, and on his chronological and mental age. Thus, elements coexist that are perceived as environmental, together with those identified as ‘biological’ and as ‘developmental’. The quality of the connections between them as well as the way in which the indicator of ‘expected’ grade depends on them, is not explained. Moreover, it is asserted that the subject’s actual grades in achievement testing must be ‘significantly below’ the ‘expected’ grade. At what point does the discrepancy in grades become ‘significant’? Also, what achievement tests are to be used? Here too there is no explanation in the Manual. Aside from all these perplexing matters, in the end a comparison must be made between that imaginary ‘expected’ grade and the IQ, which in itself is problematic. 7
To sum up thus far, the DSM-III does not create, in effect, a formula for the gap that has justified theoretical components or that are operational. On the contrary, the Manual creates a discursive tool that is much more powerful: the notion of the ‘gap’. This is an idea according to which the two constructs (that of the ‘expected’ grade and that of the IQ) are real, able to be identified, measured and quantified, and are relevant as the final arbiter in the diagnosis of learning-disabilities. This notion is likely to have a great influence on shaping the diagnostic tools, therapy and educational policy, and it is repeatedly expressed in different ways in the positions and statements of researchers and diagnosticians of learning-disabilities in Israel. Some of the additional innovations in this Manual, which were to become widespread in the Israeli learning-disabilities discourse, are: emphasis on the normality of the disabled; emphasis on the importance of the Intelligence Quotient as relevant for diagnosis and as an indicator of ‘normality’; and normalization of stages of learning. In other words, the perception is promoted that, under the proper conditions, there are fixed developmental stages in the learning of various skills.
Nonetheless, the greatest importance can be attributed to the fact that in DSM-III deviation from developmental stages is still not necessarily perceived as derived from biological factors. This Manual states explicitly that, despite the dominance of the developmental model, ‘there is no assumption regarding the primacy of biological etiological factors’ (p. 92). Indeed, the Manual not only acknowledges the possibility that there are non-biological factors involved in development, but insists on them: ‘Nonbiological factors are clearly involved in these disorders’ (p. 92).
Over and above this, the lack of agreement and the professional disputes, even in relation to the very existence of ‘specific-developmental-disorders’(!), are present in the Manual which explicitly, though briefly, deals with the educational context in which these clinical categories are formed:
The inclusion of these categories in a classification of ‘mental disorders’ is controversial, since many of the children with these disorders have no other signs of psychopathology, and the detection and treatment of the most common category, Developmental Reading Disorder, take place mainly within the educational system rather than the mental health system. Nevertheless, these conditions fall within the DSM-III concept of mental disorder … (p. 92)
This intra-textual undermining of the ontological status of these clinical entities is immediately thereafter suppressed within the act of creation of that same text. The allusions to the existence of an educational-medical complex and to the implications about the formation of the above-mentioned disorders fade away in the presence of the technical specification of those same disorders: a specification whose extent is much larger than the comments that undermine its validity. These include sub-headings that refer to aspects such as ‘age of presentation of the disorder’, ‘the evolving of the disorder’ and ‘possible complications’. What is the meaning of these statements that are not congruent with one another? How can we understand the simultaneous existence in the Manual of biological positions that identify the disorders with clinical categories with internal sources; environmental positions that assign varying weights to non-biological factors causing the disorders; and even positions that challenge, from the inside, the very conceptualization of problems in learning as clinical disorders? An attempt to track the professional conflicts that accompanied the preparation of the Manual in historical terms is beyond the scope and aspiration of the present article. The importance of presenting the textual polyphony aided in eroding the homogeneous, static and consensual image of the text. Its importance also lies in the fact that it precedes similar tensions which find expression in the extra-textual discourse on learning-disabilities in Israel (Katchergin, 2009, 2012a, 2014a).
DSM-III-R
To a large extent, the DSM-III-R (APA, 1987) continues the trends described in its predecessor. A new category of ‘Developmental-Disorders’ is created which, in addition to ‘Specific-Developmental-Disorders’, also includes ‘Pervasive-Developmental-Disorders’ and ‘Mental-Retardation’. These are grouped together with childhood disorders under the heading of ‘Disorders usually first evident in infancy, childhood, or adolescence’. Disorders associated with childhood are given a prominent position in the Manual and from then on take up a considerable amount of space in it. One of the stylistic expressions of this is its prominent placing at the head of the list of classifications. Especially prominent among them is the listing ‘Developmental-Disorders’, which is not only at the top of the list of classifications but is also ‘awarded’ a square box that emphasizes it even more.
With regard to the ‘Specific-Developmental-Disorders’, the grouping of clinical categories included in it continues to grow. The ‘Developmental-Language-Disorder’ is split into two new categories: ‘Developmental-Expressive-Language-Disorder’ and language disorder that relates to the ability to receive language (‘Developmental-Receptive-Language-Disorder’). Furthermore, a new category of ‘Developmental-Expressive-Writing-Disorder’ is created which gives guidance about writing skills below the ‘expected level.’ Finally, another new category of ‘Developmental-Coordination-Disorder’ is created.
The need to use ‘standard’ tests to diagnose the disorders is mentioned repeatedly. In addition to these texts, an important classifying criterion is added, whereby, in the case that a gap is revealed, it must ‘significantly’ harm learning achievements or everyday activities in order for the diagnosis to make the determination of a learning-disorder. Again, there is no accompanying discussion for determining the rule ‘significant harm’; the question of what constitutes significant harm is not raised, and accordingly no guidelines are given to identify it.
Also recurring are the warnings of the existence of disagreements about including these disorders in the Manual. Conversely, and interestingly, the reservations, introduced in DSM-III about biological aetiological interpretation of the development of disorders, disappear entirely. Even in the specific survey of each disorder, there is no longer a mention of the possible involvement of non-biological factors – the potential influence of inappropriate teaching as relevant to the aetiology is explicitly negated. At the same time, perinatal complications like family kinship are emphasized as relevant factors or predispositions for the disorders.
The various disorders are associated with young age groups. For example, it is noted that, in most instances, ‘Developmental-Reading-Disorder’ and ‘Developmental-Expressive-Writing-Disorder’ present at age seven, while ‘Developmental-Arithmetic-Disorder’ presents at age eight. Later presentation of these disorders (generally around age 9 or 10) is explained by means of a new professional idiom in this context: Compensation. In other words, this is the ability of the sufferer from the disorder to compensate for it and to keep it, for a time, in a latent condition, especially if he is highly intelligent. The prognosis for these disorders is good; if treatment is given, usually no signs of them remain in adulthood. In some of these, even a ‘spontaneous recovery’ is possible.
In the DSM-III-R, the incidence of most of these disorders is still unknown; however, the most prevalent of them is the ‘Developmental-Reading-Disorder’ – the rate of this among the population of school children was determined to be between 2%, for a restricted assessment, and 8% for a broader assessment of its prevalence.
The developments in the DSM-III-R promote a biologistic conceptualization of learning-disabilities as well as their conceptualization as disorders whose onset occurs at young ages. Similarly, in most cases, it is possible to recover from them with the aid of appropriate therapy, such that no vestige of them remains. For the first time, statistical rates are determined for the frequency of the disorders (no explanations are attached about how this was determined, nor are there references to the research on which this is based). 8 Another discursive tool in the shape of the Compensation idiom is added to the professional toolbox. These developments took place gainst the backdrop of the spread of the discourse on learning-disabilities, and were accompanied by an increase in the relevant professional institutions and the range of services provided by them (Katchergin, 2009).
DSM-IV
DSM-IV (APA, 1994a) is presented as a considerable advance on those preceding it, based on ‘objective’, observable, testable, empirical and replicable data relying on accumulated scientific knowledge, including a growing understanding of the field of developmental psychopathology (Katchergin, 2009).
The modern clinical category of ‘Learning-Disorders’ appears here for the first time. Following another transformation of the nosological system, the previous grouping of categories is dismantled and instead new sub-categories are formed:
Reading-Disorder
Mathematics-Disorder
Disorder-of-Written-Expression
Non-Specific-Learning-Disorder.
No attempt is made in the Manual to develop explanations for the categorical change and particularly for the deletion of the adjectives ‘developmental’ for the various disorders (a desultory mention of the changes can be found in Appendix D of the Manual which laconically states that ‘The name has been changed … to reflect common clinical usage’).
Another classification change includes the severing of the above sub-groups from Axis II and their codification in Axis I, together with ‘Pervasive-Developmental-Disorders’, ‘Communication-Disorders’ and ‘Motor-Skills-Disorders’ (Axis II retains the category of mental-retardation and personality-disorders). Thus, this is the final divorce of the conceptual and structural link that continued to weaken between ‘learning-disorders’ and ‘personality-disorders’. Moreover, a clear partition is introduced between ‘learning-disorders’ and ‘mental-retardation’.
It would be very difficult to defend the possible claim that the changes relate only to naming and do not encompass any indication of a qualitative-essential change in disorders. This is because, in the categories under discussion, there are changes of varying orders of magnitude in the definitions, in the symptomatology, in the description of their progression and in their prognosis. For example, the replacement of ‘Developmental-Arithmetic-Disorder’ with ‘Mathematics-Disorder’ opens up the option of identifying new sub-fields of information in the world of mathematical knowledge in which disorders could be located. 9
The various disorders are still associated with young ages, and the prognosis is still described as good. Nevertheless, in the margins of the description of the development of the various disorders, there is a note likely to make older and older age-groups into objects of tagging by means of this series of disorders. For example, the description of the progression of the development of the reading disorder ends by saying it is possible that this ‘might persist into adult life’. Turning the clinical gaze towards adult ages is even more prominent when this comment is compared with what is stated in the previous DSM, where it is noted that ‘There are often no signs of the disorder in adulthood’. This negation of the prevalence of the disorder in adults is not mentioned in DSM-IV. The expansion of the relevant age range to manipulation by means of the conceptual world of learning-disabilities, as well as the determination that the prognosis is indeed good but only for a ‘considerable percentage’ of the sufferers from the disorder, is likely to be expressed in the spread of the idiom of permanence in the field of learning-disabilities. The widespread perception today among Israeli researchers of disabilities and diagnosticians is that learning-disabilities accompany the sufferer for all his life and cannot be completely eradicated (Katchergin, 2009).
The prevalence of most of the disorders is not clear, but it is stated that the most widespread among them is the ‘Reading-Disorder’. It is interesting that assessments of their prevalence dropped to 4% of the population of school-children. It is also mentioned that in other countries using more stringent criteria, it is likely that the rate of prevalence would be even lower. An additional expansion of the range of application of the disorders is expressed in the statement that there is nothing in the existence of sensory deprivation or general medical problems (especially neurological conditions) to negate the feasibility of a simultaneous presentation of a learning disorder (an antecedent of the co-morbidity idiom in common use by diagnosticians).
In a casual remark, the Manual addresses the possibility of an invalid diagnosis of children who received inadequate education, whose first language was not English, or who had an ethnic or cultural background different from the culture of the school (a euphemism that obscures the fact that that same-school culture stands for values and norms identified with White middle-class Americans). 10 There is also a reference to the gender gap in the rates of those diagnosed – for example, in regard to the reading disorder, it has often been found that the proportion of boys diagnosed could reach 80% compared with 20% for girls.
The above remarks are swiftly translated into technical language which identifies them as problems of bias that does not necessarily arise from the diagnostic tools themselves (which are considered objective), but rather from the biased processes of identifying children in the school frameworks. Nevertheless, as in each edition of the Manual, the recommendation is to polish the classification system and refine the diagnostic procedures in the future. In this way, in effect, the various gaps, contradictions, biases and imprecisions serve as a justification for the publication of further editions of the Manual.
DSM-IV-TR
DSM-IV-TR (APA, 2000) promotes the individualistic and biologistic conceptualization of learning-disorders despite the atheoretical pretensions in it. Learning-disorders had become consolidated into a firm clinical fact, supported by a regime of scientific justification, and backed, as it were, by an abundance of empirical and clinical data (even though there is no evidence provided in the text). The many conceptual permutations they underwent do not receive explanations, not even superficial rationalizations. At most they are presented implicitly, as an expression of current updates and of re-organization of those same categories, as though these were the same entities with different names affixed to them at different historic periods.
The genealogy of these disorders reveals a gradual process of reduction of the textual polyphony, that is, of the voices of the experts who posed questions, and sometimes even objections about their inclusion in the DSM. It is apparent that the complete disappearance of the questions from the Manual indicates that the process of consolidation of these disorders was shut down: the most comprehensive and popular diagnostic system granted legitimacy to the learning-disabilities; the trends of intra-textual objecting were eradicated. It seems that the arguments about them revolved around the issues of developing new evaluation and diagnostic tools, as well as identifying and profiling of the sub-types of learning-disorders and improving the intra-paradigmatic practices of polishing and refining.
DSM-5
The contemporary body of medical knowledge, as it is presented in DSM-5 (2013), contains several new ideas. Learning disorders are now placed under the heading ‘Specific-Learning-Disorder’. Interestingly, it is apparent that this is a return to the ‘Specific’ terminology of the first three editions. The new category is divided into three clinical sub-categories, distinguished by ‘Specifiers’ according to the main learning skill affected:
Specific-Learning-Disorder-with-Impairment-in-Reading
Specific-Learning-Disorder-with-Impairment-in-Written-Expression
Specific-Learning-Disorder-with-Impairment-in-Mathematics.
This is the first time that the DSM has granted official recognition to the terms Dyslexia and Dyscalculia where these are identified by names that are alternatives for disorders (1) and (3), respectively. It is notable that this kind of recognition was not accorded to the term Dysgraphia, which is still entirely absent from the Manual.
Learning-disorder is no longer classified under the main category Disorders usually First Evident in Infancy, Childhood, or Adolescence, but rather under the new category of Neurodevelopmental-Disorders.
Another innovation is the deletion of the main criterion for diagnosis stated in DSM-III: the gap between the IQ measurement of the subject and the various achievement tests relevant to the skill being examined. The removal of the restriction with regard to the ‘gap’ opens up another potential for the diagnosis of those with learning difficulties as suffering from ‘Specific-Learning-Impairments’. From now on, states the text explicitly, those suffering from a developmental disability (retardation) on the one hand, and those with the highest intelligence (gifted) on the other, can all be diagnosed as having learning-disorders.
There are now four diagnostic categories: (A) Difficulties in learning academic skills and in using them that are expressed in at least one of six different symptoms (reading that is inaccurate, slow or a struggle, difficulties in reading comprehension, spelling difficulties, difficulties in written expression, difficulties in arithmetic and difficulties in grasp of mathematics). It is also determined that the difficulties must persist for at least six months despite clinical interventions intended to treat them. Thus, for the first time, the Manual gives voice to the logic of the RTI (Response to Intervention) model. (B) The difficulties referred to must be significantly below the expected achievements relative to chronological age, they must be quantified, and they must be causing significant harm in the conduct of academic, employment or everyday life. An explanation for what significant harm is or for the standards for quantifying it is not given in the Manual. (C) The age at which the disability is first supposed to present is assumed to be elementary school age. Nevertheless, there is an immediate reservation noting that the disability may also not be fully revealed until the demands for academic skills exceed the limited abilities of the disabled person. This formulation in effect opens the way for a legitimate first presentation of a learning-disability at any age. (D) The criterion of Exclusion Diagnosis states that diagnosing a learning-disability must be undertaken only if it is not possible to give a better explanation for the learning-disabilities based on other sources: intellectual, sensory, neurological or mental disabilities, psychosocial distress, lack of skills in the language in which academic skills are taught and inappropriate teaching. To put it another way, the environmental factors are mentioned in only one paragraph, and then only as a secondary aspect of possible bias factors in the diagnosis.
The last diagnostic innovation requires diagnosticians to note the severity of the disability on three levels: moderate, medium, profound. Particularly interesting is the concept of ‘moderate’, according to which the character of the specific academic difficulty in this case is such that the disabled person can compensate for it and function well provided that he gets appropriate support. Time will tell whether, and how, this concept of moderate is consistent with the requirement to diagnose learning-disorders only if the academic difficulties are found to be persistent in the face of intervention and therapy for at least six months (a requirement first stated in this very edition). In any event, it is apparent that this concept of ‘moderate’ has additional inflationary potential, because, thanks to it, there could be people functioning well in academic contexts who are identified as moderately learning-disabled.
DSM-5 states, without any reservations, that ‘Specific-Learning-Disorders’ have a biological origin: ‘Specific-learning-disorder is a neurodevelopmental disorder with a biological origin that is the basis for abnormalities at a cognitive level that are associated with the behavioral signs of the disorder’ (APA, 2013: 68). Thus, cognitive and behavioural dimensions are phenomena derived from biological origins. This statement expresses the triumph of the biomedical paradigm in the DSM and the exclusion of the competing aetiological paradigms, such as cognitive or educational-behavioural models of learning-disorders. Moreover, not only is the origin biological, but also the Manual asserts that in many cases it is hereditary. However, neither of these statements is supported by research or relevant literary sources. Even more notable are the two remarks in the Manual that undermine the validity of its categorical determination that disability has a biological origin. First, on the page following this statement there is a casual remark that there are no natural points of intersection by means of which it is possible to distinguish between individuals with this particular disorder and individuals without it:
Academic skills are distributed along a continuum, so there is no natural cutpoint that can be used to differentiate individuals with and without specific learning disorder. Thus, any threshold used to specify what constitutes significantly low academic achievement (e.g., academic skills well below age expectation) is to a large extent arbitrary. (p. 69)
This remark is astonishing in the light of the categorical statement that a disorder has a biological origin, since, if this is so, how is it not possible on the basis of aetiological biological markers to differentiate between someone disabled and someone who is not? Also, what is the meaning of the acknowledgement that any threshold used to specify what constitutes low academic achievement is arbitrary to a large extent? Moreover, two pages after the biological statement, there is a remark that pulls the rug out from under its feet: ‘There are no known biological markers of specific learning disorder … Cognitive testing, neuroimaging, or genetic testing are not useful for diagnosis at this time’ (p.70). We are being told that there are still no known biological indicators for the disorder!
Next, what about the statement that the disorder is hereditary in many cases, considering that the Manual states there are no relevant genetic tests? The only support for the fact that this is a hereditary disorder is to be found in the form of a remark under the heading ‘Genetic and physiological risk factors’:
Specific learning disorder appears to aggregate in families ….The relative risk of SLD … is substantially higher … in first-degree relatives of individuals with these learning difficulties compared with those without them. … There is high heritability for both reading ability and reading disability [heritability estimate values greater than 0.6] … (p. 72)
The genetic statement is only based on the statistical finding that the probability of finding people in families with the specific learning-disorder is substantially higher if they include people who already have this disorder. This finding could supposedly be explained by means of sociological, psychological or cultural explanations in which the common learning difficulties are a product of acquired familial, cultural and environmental context.
DSM-5 broadens the application of the definition of disabilities to those suffering from difficulties in various academic disciplinary skills, and not only to those with difficulties in basic learning skills (such as reading, writing and arithmetic): ‘Difficulties mastering these key academic skills may also impede learning in other academic subjects (e.g., history, science, social studies), but those problems are attributable to difficulties learning the underlying academic skills’ (p. 68).
DSM-5 explicitly states that the diagnosis of a learning-disorder can be made at any age: ‘Specific learning disorder can only be diagnosed after formal education starts but can be diagnosed at any point afterward in children, adolescents, or adults…’ (p. 70). In this way, it cancels out the assumption which was central to the field of learning-disabilities from the unfolding of this field, whereby difficulties that imply learning-disabilities must find actual expression during elementary school ages. If they appear after that, they are not evidence of the existence of a disability but must be treated as though the origin lies elsewhere (Katchergin, 2009). Furthermore, the text also invites a potential invasion into the territorial field of tender years in that it first determines ‘Precursors’ for disabilities among infants. From this point on, lack of interest in rhyming games, difficulty in learning nursery rhymes, inaccuracies in pronouncing words, inventing words, frequent use of baby-talk, difficulties in remembering letters, numbers or the names of the days of the week, inability to identify phonemes or letters, refusal to participate in activities in the kindergarten and even inability to write their first names – all these and others become legitimate grounds for diagnosing an infant as learning-disabled (APA, 2013: 71).
Conclusions
This article has attempted to uncover, through genealogical analysis and by means of tools from the fields of the sociology of medical knowledge and critical analysis of scientific discourse, the metamorphoses in the definition and conceptualization of learning-disorders in the DSM. The text is very important because, in the Israeli field of research and diagnosis, it is considered ‘neutral’ and ‘objective’, and it is traditionally acceptable to rely on it to validate and justify theoretical and conceptual claims and diagnostic and therapeutic practices. In comparison to its hegemonic status in the local field of disabilities, it has become clear that in the global discourse there is much criticism, from a variety of paradigmatic sources, about it and the assumptions embedded in it.
The article has traced the various textual ways in which the category of learning-disorders was formed as a truth-object, to use the term of the discourse scholar Linda Graham (2005); it has also considered the significant changes in the conceptualization of disorders, especially changes that have established them as biological and persistent disabilities. This research has also revealed the vagueness and often contradictory nature of the text, especially the fact that – in contrast to the paradigmatic polyphony that characterized the first editions – there has been a gradual acceptance of the biomedical paradigm as the only relevant model for understanding learning-disabilities, to the point that the latest edition has become hegemonic. As a result, a textual narrative has emerged in which learning difficulties are dislocated from all contexts: political, economic, cultural or educational.
It has also been shown that the main declarations in the DSM about the quality of learning-disorders, such as the suggestion that their origin is biological and even genetic, has no proven research or medical support in the DSM. In this sense, the many studies carried out in the field of disabilities in Israel, using biologistic assumptions based on the Manual, are deficient in terms of their scientific validity.
An analysis of the conceptual metamorphoses also makes it possible to point out their possible implications with regard to inflationary diagnosis of disabled subjects. The determination in DSM-5 that the origin of learning-disorders is biological and not environmental is likely to expand the processes of medicalization in the field of education by giving added validation to the present trend of translating learning difficulties from educational-environmental language into medico-clinical language. In doing so, it is likely to bolster the industry of psychodidactic diagnoses. In Israel one manifestation of this industry is the huge percentage of pupils diagnosed as learning-disabled in classrooms: 30–50% in affluent areas and cities is not uncommon (Katchergin, 2009). 11 The advantage of the DSM for this industry is embedded in its vagueness and ambiguity in all aspects related to translation of its assumptions into the practices of identification and diagnosis, since it does not relate, at all, to explicit and specific rules of assessment or to diagnostic procedures to be used in practice. Similarly, the most recent DSM contains additional inflationary potential: the cancellation of the principle that required use of intelligence tests as an essential stage in the diagnosis of learning-disabilities (from now on retarded and gifted persons can be diagnosed); the formulation of the new measure relating to the severity of the disability (from which it transpires that even people who function ‘well’ in academic contexts can now be identified as learning-disabled, though at a moderate level); the statement that any academic difficulty could imply a latent disability (not only difficulties in basic academic skills); the explicit determination that people with learning disorders are ‘normal’ (an anomalous phrase in the framework of a text whose aim is to catalogue all mental illnesses and disorders recognized by the science of psychiatry); and, finally, expanding the range of relevant ages for diagnosis, assigning new names to learning disorders as neurodevelopmental disorders, and the emphasis placed on the persistence of the disorder (from now on, infants on the one hand, and adults, on the other hand, lacking a history of difficulties, can become legitimate objects for diagnosis).
Additional studies are required to investigate the methods of acceptance of the DSM among members of the various clinical professions, as well as the strategies for using it, in practice, in the field of education.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.