
Abstract
Mental illness in a hospital in a medium-sized town in Sweden was studied. Consecutive case records from 1896 to 1905, and also from 2011, were selected. In the historical sample, neurasthenia was the most common diagnosis, followed by affective disorders and alcohol abuse. ICD-10 diagnoses corresponded well with the historical diagnoses. Melancholia resembled modern criteria for depression. Mania, insania simplex and paranoia indicated more severe illness. Abuse was more common among men and hysteria among women. Those with a medical certificate for mental hospital care were very ill and showed no gender difference. There were no diagnoses for abuse, but 17% had a high level of alcohol consumption. The pattern of signs and symptoms displayed by patients does not appear to change with time.
Introduction
The nineteenth century in Sweden was an era of social change, from an agricultural to an industrial society. After several years of war in previous centuries, ending in 1814, the country was poor. A series of bad harvests, and subsequent importation of cheap cereals, deprived many Swedish farmers of their source of income. One million people were forced to emigrate during the second half of the nineteenth century, most often to the USA. In 1900, Sweden had 5 million inhabitants and an infant mortality rate of approximately 10%, comparable with present day Angola (Childmortality, 2015).
Care for the mentally ill was poorly developed during the first half of the nineteenth century. Most people were cared for at home, in poorhouses or in secluded parts of hospitals caring for the old and infirm. The first hospital exclusively for the insane was opened in Vadstena in 1826 (Qvarsell, 1982). The appalling conditions of the mentally ill, and the successful reforms initiated in neighbouring Norway, motivated a group of reformers, led by the physician Carl Ulric Sondén, to draft the first Swedish Lunacy Act in 1858. This Act stressed that patients should be treated with great respect and receive good care. Insane people were to be regarded as ill in the medical sense, and should be cared for by doctors and nurses in hospitals, either in a general hospital or in a specialized mental hospital (SFS, 1858).
There were 41 general hospitals in Sweden in 1861; the number had grown to 72 local general hospitals by 1900, each with a responsible hospital physician (BiSOS, 1862, 1902). Mental patients in the general hospital paid half the ordinary hospital fee. Patients who were considered clearly unable to care for themselves could be admitted to a mental hospital, where care and treatment were paid for by the state. Applications for treatment in a mental hospital could be made by the patient or his/her relatives, and a medical certificate had to be appended (SFS, 1858).
In 1859 psychiatry became part of the curriculum for medical students in Sweden, at first as a theoretical subject, and two years later it included two months of clinical training in a lunatic asylum. The teaching of psychiatry started at Uppsala University and was led by Gustaf Kjellberg, who was appointed professor in 1863. In 1861 the first Swedish professor of psychiatry, Wilhelm Öhrström, had been appointed at the new mental hospital Konradsberg, in Stockholm, which opened the same year (Harding, 1975).
Although little is known of the content of the psychiatric education during the later part of the nineteenth century, most Swedish psychiatrists of the time were influenced by German psychiatric thinking, and mainly by the school of Wilhelm Griesinger. He was nominated to the Royal Swedish Academy of Sciences by Carl-Ulric Sondén and elected as a member of the Academy in 1868, the year of his death (Sjögren, 1868). Sondén had travelled extensively in Europe, and corresponded with colleagues in Germany and France.
In 1861 Sweden had 9 mental hospitals with 1258 patients in total; in 1900, 12 cities had a mental hospital, with a total of 5016 patients. In 1900 there were 1131 physicians in the entire country, 26 of whom worked at a mental hospital (BiSOS, 1862, 1902). Since the mental hospitals were run by the state, the doctors in charge sent detailed yearly reports from 1861 to 1877 to the Royal College of Medicine (Kungliga Sundhets-kollegium), and from 1878 to the Royal Board of Medicine (Kungliga Medicinalstyrelsen). These reports still exist and contain a wealth of information about conditions in the mental hospitals, including the diagnostic spectrum.
All patients were tabulated in diagnostic categories. In 1861 the categories were: mania, melancholia, ecnoia, paranoia, dementia, idiotia, paralysia generalis, epilepsia. In 1900 the diagnostic system had been slightly changed; it categorized mental illness into: insania simplex (with the subcategories melancholia, mania, paranoia, dementia), dementia paralytica, insania epileptica, idiotia. Ecnoia – a delusional condition characterized by raised self-esteem but no confusion – disappeared in 1882 (BiSOS, 1862, 1884, 1902).
The care received by psychiatric patients towards the end of the nineteenth century in a general hospital and in the mental hospital responsible for the needs of the same geographic area can be studied in some detail for the town of Kristianstad in southern Sweden and the surrounding countryside. This is due to the psychiatric interest and the diligent records kept by the doctor in charge of the general hospital, Johan August Hedlund (see Figure 1a). He finished his medical education in Stockholm in 1888, and thus had received the compulsory two months of psychiatric training. His specialty was surgery, but he had broad medical interests and spent his holidays on the European continent, visiting colleagues and learning about new treatment methods which he subsequently tried out in Kristianstad (Ahlström, 2010).
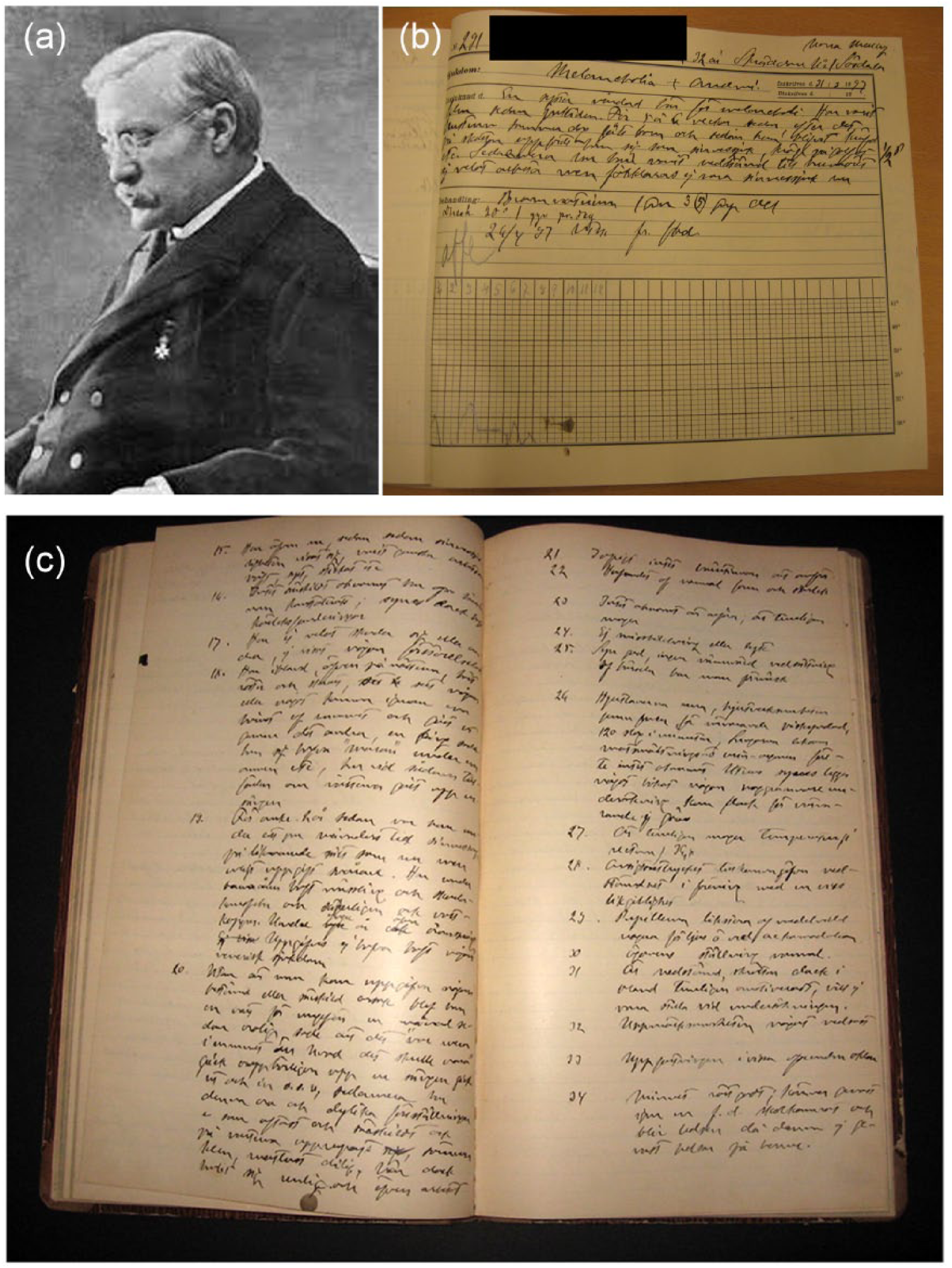
(a) Dr Johan August Hedlund; (b) a typical general case record; (c) two pages from a medical certificate for mental hospital care. Both records were written by Dr Hedlund.
The first aim of the present study is to describe the diagnostic range of the psychiatric patients cared for in the general hospital during the period 1896–1905. Level of functioning among those with a medical certificate for hospital care was evaluated according to the Global Assessment of Functioning Scale (GAF) (Hall, 1995). Due to the richness of detail in the certificates for mental hospital care that Dr Hedlund issued for the patients he referred to the mental hospital, it is possible to re-diagnose the patients according to a more modern system, the ICD-10 (WHO, 1993). A second aim of this study is to compare the two sets of diagnoses: the modern cohort with ICD-10 diagnoses and the cohort from 1896–1905. Finally, gender differences are considered.
Patients and methods
General hospital patients
The first general medical hospital in Kristianstad was built in 1864. At the end of the nineteenth century, it held 146 hospital beds, of which 7 were reserved for the mentally ill. Together with two other general hospitals, Kristianstad served an area with approximately 220,000 inhabitants. The other two general hospitals (Ängelholm and Simrishamn) were 100 km and 70 km, respectively, from Kristianstad; they had in total 148 beds, with 7 reserved for the mentally ill. The region was rural and characterized by poverty and emigration (Ahlström, 2010; Appelquist and Nilsson, 2005; BiSOS, 1903).
From 1896 to 1905 the Kristianstad hospital had 11,458 inpatient admissions. Data could be retrieved for all but 150 (1.3%) of them, and 589 (5.1%) had a main diagnosis of mental illness, representing 503 individual patients. Of the admissions with mental illness, 208 (35.3%; representing 180 individuals) resulted in a medical certificate for care in the mental hospital in the city of Lund, 100 km from Kristianstad. Thus, the majority of the mentally ill were treated exclusively at the general hospital.
When patients were admitted to the general hospital, they were registered in a ledger and a case record was written. As a result of a home visit, some of the psychiatric patients had already received a medical certificate for mental hospital care prior to admission to the general hospital. More often, a certificate was written during the patient’s stay in the general hospital. The mental hospital had a waiting list for admission, and direct admission to the mental hospital was rare, if it occurred at all.
Historical records
Three types of records were available from Kristianstad general hospital from 1896 to 1905, and all were used for the study. All records were written by hand and are still in excellent condition.
Admissions ledgers
The ledgers contain the patient’s name, date of birth, diagnosis, admission and release dates, and in more than half of the cases also the cost of the stay. A new ledger was started each year.
General hospital case records
The general hospital case records are brief, and contain a short patient history, data about treatment and its outcome, day of arrival and release from the hospital, and the diagnosis. The case record includes a temperature chart and notes about drugs and other treatments (see Figure 1b). The chart form covered one month and, for patients who stayed longer, charts were sewn together. Records from consecutive patients were also sewn together in bundles of 50. All case records are stored in wooden chests, one for each year.
Medical certificates for mental hospital care
At the time, admission to a mental hospital was considered a favour – it was paid for by the state. Therefore, admission required (1) a detailed medical certificate, the content of which was strictly regulated by the Royal Board of Medicine. Admission also required (2) an application written by the patient, or his/her family, and details about the illness history provided by the family on a printed (or handwritten) form. The family’s knowledge was important, as the doctor seldom met patients regularly, so relatives were better suited to describe the development and pattern of the illness (Gadelius, 1913). This form was countersigned by the vicar, with an annotation as to whether the family members were credible. Finally, (3) a clerical certification was appended, including information about which parish the patient belonged to and whether he or she had attended church services. Interestingly, this last certificate was needed for any hospital admission. Admission to the mental hospital could be denied, but this appears to have been rare.
Instructions on how to write the medical certificate were found in the second version of the Swedish Lunacy Act of 1883 and the third of 1901 (SFS, 1883, 1901). Questions on heredity, childhood, upbringing, education, abuse of alcohol or illicit drugs, former illnesses, current living circumstances, and symptom development had to be answered. A comprehensive mental and physical state had to be documented. If any question could not be answered, the reason had to be stated. The medical certificates describe symptoms well and in detail, but usually do not contain a diagnosis.
All medical certificates, including appendices, were copied by hand in a bound book (see Figure 1c), one for each year, which was stored in the Kristianstad hospital archive. The original was sent to the mental hospital in Lund. The richness and quality of the patient descriptions in the historical records is often quite impressive.
Modern records
In 2011 the psychiatric clinic in Kristianstad had 28 hospital beds serving 140,000 inhabitants in the catchment area; 945 patients – representing 1384 admissions – received inpatient care. The clinical case records are computerized. Anonymized information about age, gender, length of stay and diagnosis was retrieved and tabulated, to use as a comparison for the historical material.
Procedure
All patient admissions that had a main diagnosis of mental illness, from 1896 to 1905 at the general hospital in Kristianstad, were studied (n = 589). Since some patients were readmitted for a second or third hospitalization, this represents 503 individual patients. Those with a primary diagnosis of a physical illness, for example anaemia complicated by hysteria, were not included. Patients who were treated for other conditions, for example a gunshot wound, were not included, even if the cause of the injury might well have been a suicide attempt. Those who received the diagnosis suicidum had made a definite suicide attempt and were included. The diagnoses of the patients with a medical certificate for mental hospital care (n = 208), representing 180 patients, were most often found in the general case records.
The historical case records were studied by the first author (MA). The handwritten medical certificates for mental hospital care (n = 208) were read and transcribed on a computer. The information from the handwritten general case records and the ledger were transcribed by hand.
None of the 208 medical certificates for mental hospital care were missing for the years studied. Some general hospital case records were missing: cases 1–500 in 1896, cases 1–150 in 1900, cases 1–449 in 1902, and cases 750–1253 in 1905. The relevant information could, however, be retrieved from the ledgers, with the exception of the 150 patients from 1900. Data are thus available from 11,308 admissions. Hypothetically, the missing data represent eight patients with mental illness.
Classification
The information from the historical sources was tabulated by name, gender, age, length of stay, diagnosis, and whether the patient had recovered or improved during the hospital stay. This structure, together with the 208 detailed medical certificates, enabled a re-diagnosis of all cases but one according to the ICD-10 research criteria (WHO, 1993).
The medical certificate for mental hospital care contained a case history, including the one written by the patient’s relatives, and provided ample information about the progression of the disease. When re-diagnosing a patient with an ICD-10 diagnosis, current diagnostic principles were used. For example, if a patient had a manic state on their first admission, and no evidence of previous depression, the diagnosis became mania (F301). If the patients had had depression, and suffered from mania, the diagnosis became bipolar disorder (F31). In addition to the ICD-10 diagnosis, those patients who got a medical certificate for hospital care were rated on the Global Assessment of Functioning (GAF) scale (APA, 1987).
To check the validity of the re-diagnosis, a trained psychiatrist read 19 randomly selected case records out of the 208. The two sets of diagnoses were identical up to the third figure in ICD-10 (Fxx.x) in 16 of the cases (84%). The three cases where diagnoses differed were diagnosed by the first author (MA) as Affective disorder with psychosis (F3), and as Psychosis (F2) by the second diagnostician.
In order to have diagnostic groups of a reasonable size, some historical diagnoses were grouped together. Thus, puerperal psychosis was grouped within psychosis, neurasthenia sexualis with neurasthenia, and insanity with insania simplex, that is ‘simple mental illness’. Mania acuta and periodea was grouped within mania. Dementia senilis and paralytica were included as dementia. Alcoholismus acuta or chronica were grouped together as one category together with cases of delirium tremens. When double diagnoses were used in the original material, for instance Insania Simplex cum paranoia, the more specific diagnosis, in this case paranoia, was used. The results are presented mainly as cases rather than as individuals, on the basis that the diagnosis sometimes changed from one illness episode to another.
By Swedish law, medical case records are protected by strict confidentiality for a period of 70 years. Since all our case notes were more than 100 years old, and the reference records were anonymized, no research ethics review was considered necessary. We made an ethical application for another study in our project, concerning causes of death in the same patients as in this study. The ethical Review Board in Lund did not consider that an ethical review was needed, and its concluding comment was that they did not see any objection to the project from an ethical point of view (2016/497).
Results
Original historical diagnoses
Neurasthenia was the most common diagnosis (27%), followed by hysteria (12%) and, in the same category, hysteroneurasthenia (3%). Alcoholism was as common as hysteria (12%). Mania, melancholia and insania simplex were equally common (10–11%). Paranoia and psychosis together accounted for 9%. Other diagnoses (7%) were idiotia, hypochondria, dementia, amentia, paralysé generale, intoxico phosphores, suicidum, traumatic neurosis, hysteromelancholia, thrombosis arteria, apoplexia cerebri, tumores hemoroides, katalepsia and insania epileptica.
Figure 2 illustrates the distribution of diagnoses between the cohort with a medical certificate (n = 208) and the cohort without (n = 381). There was a clear difference between the two groups, and some diagnoses, e.g. neurasthenia, hysteria, hysteroasthenia, alcoholism, were virtually absent among the patients referred to the mental hospital.

Historical diagnoses in Swedish patients who were admitted to a general hospital for a mental illness and were certified and referred to mental hospital care (n = 208) or were not certified but remained in the general hospital for care (n = 381) in the period 1896–1905; for ‘Others’, see Figure 3.
The group of admissions without a medical certificate for mental hospital care most often had neurasthenia (42%), followed by alcoholism and hysteria (each 18%). Delirium tremens was quite common among those who had an alcohol diagnosis (27/68, 40%). Paranoia, psychosis, mania, melancholia and insania simplex were less frequent (2–4%). Traumatic neurosis, hypochondria, amentia, hysteromelancholia, suicidum and intoxicatio are included in ‘others’ (2%).
In the group with a certificate for mental hospital care, mania was the most common diagnosis (26%), followed by insania simplex (24%) and melancholia (22%). Paranoia (11%) and psychosis (5%) were also represented. Neither alcohol diagnoses nor neurasthenia were found in this group. Other diagnoses (7%) included tumor hemoroides, thrombosis arteria, apoplexia cerebri, paralysé generale, insania epileptica, hypochondria, amentia and katalepsia. Alcoholism was not used as a diagnosis, although 17% (36 of 208) in this cohort had a high consumption of alcohol. A high alcohol consumption was most common in the group that was re-diagnosed to the F2-group, namely those with psychotic diseases (22%).
Of the 65 patients who had more than one admission during the 10 years covered by the study, 16 received a medical certificate on all admissions, and 23 never had a certificate. The readmitted patients included 30 women, with 39 repeated admissions in total, and 35 men with 47 repeated admissions. In 38 of those 65 patients the historical diagnoses were not the same for the different admissions. Most often the first episode was diagnosed as insania simplex, while subsequent episodes were diagnosed more specifically, for example as melancholia or mania, but changes also occurred from mania to melancholia/neurasthenia, and from mania to psychosis or paranoia. There were also a few switches between neurasthenia, hysteria and hysteroneurasthenia.
The average GAF score in the cohort with a mental certificate was 29, median 30.
Re-diagnosis of historical cases
The comparison between original historical diagnosis and re-diagnosis according to the ICD-10 is given in Table 1. The table illustrates the ‘translatability’ of historic diagnoses into modern ones, and suggests that for melancholia (modern diagnosis F3) in particular the concurrence is quite good. A diagnosis of mania (a term which was originally designated a psychotic state with excitement) on the other hand, could correspond either to F2 (psychosis) or F3 (affective disorder). A similar pattern was obvious in patients with the historical diagnosis insania simplex (which could be used for a range of psychotic disorders), which was re-diagnosed as F2 or F3 in about equal proportions.
Rediagnosis from historical diagnoses into ICD-10 diagnoses in a cohort of 208 Swedish patients admitted to a general hospital and referred to the regional mental hospital during the years 1896–1905. Figures refer to number of cases.
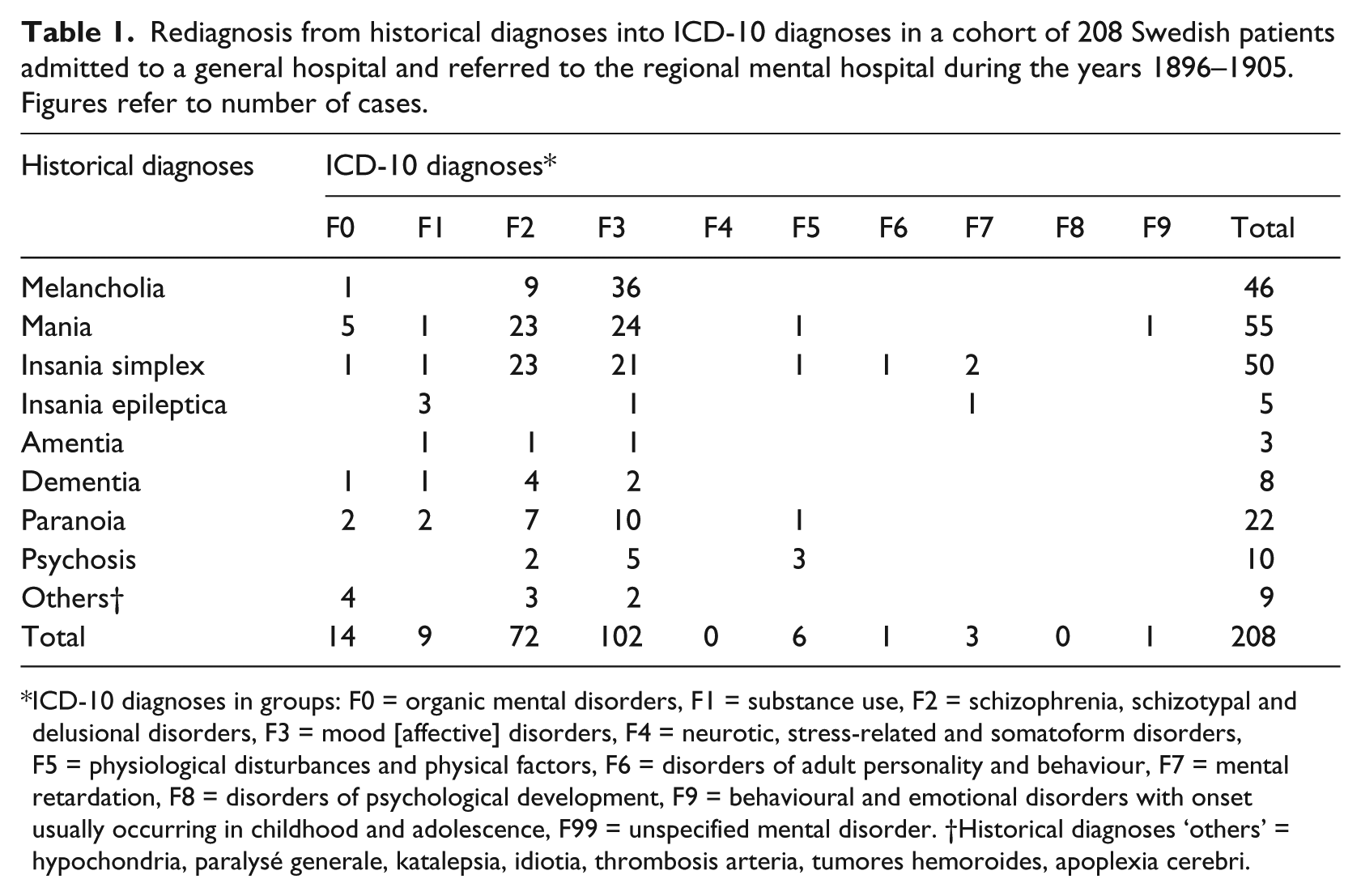
ICD-10 diagnoses in groups: F0 = organic mental disorders, F1 = substance use, F2 = schizophrenia, schizotypal and delusional disorders, F3 = mood [affective] disorders, F4 = neurotic, stress-related and somatoform disorders, F5 = physiological disturbances and physical factors, F6 = disorders of adult personality and behaviour, F7 = mental retardation, F8 = disorders of psychological development, F9 = behavioural and emotional disorders with onset usually occurring in childhood and adolescence, F99 = unspecified mental disorder. †Historical diagnoses ‘others’ = hypochondria, paralysé generale, katalepsia, idiotia, thrombosis arteria, tumores hemoroides, apoplexia cerebri.
The patient group with mental certificates did not include a single case of neurasthenia, suggesting that this diagnosis was not considered severe enough to merit treatment at a mental hospital. Thus, we were not able to re-diagnose this condition into a formal ICD-10 diagnosis. The information contained in the case records suggests that a modern diagnosis might well be an anxiety disorder. The different meanings of the term ‘mania’ in the old records and in current diagnostic practice is further illustrated by the finding that only 38% of the patients with mania in the historical records were re-diagnosed as mania or manic state according to the ICD-10. This is in contrast to melancholia, which appears to be more or less equivalent to the modern concept of depression, since it was re-diagnosed as a depressed state (depressive episode in bipolar disorder (F31.4 or F31.5), or depression (F32.2, F32.3, F33.2 or F33.3), or depressive episode in schizoaffective disorder (F25.1)). Of those with the diagnosis ‘melancholia’, I re-diagnosed 7 with F32.2, 22 with F32.3, 2 with F33.3 and 2 with F25.1; thus, 33 of the 46 melancholia cases (72%) got an ICD-10 diagnosis of depression or depressive state in the schizoaffective disorder.
The equivalence was even more pronounced for the historical cases of psychosis, which were re-diagnosed as a psychotic disorder (affective disorder with psychotic symptoms (F30.2, F31.2, F31.5, F32.3, F33.3), schizophrenia (F20), delusional disorder (F22) or schizoaffective disorder (F25)) in every single case. Paranoia was re-diagnosed as a psychotic condition in 82% according to ICD-10.
In some medical certificates the term ‘manio-cholic fits’ is used for patients with repeated episodes of elated and depressed mood. In our material, 37 admissions (21%) met the ICD-10 criteria for bipolar disorder; 19 of these (51%) had the historical diagnosis mania.
Just as the historical diagnosis of mania can be re-diagnosed either as an affective or a psychotic disorder in the ICD-10, the cases diagnosed as insania simplex can be re-diagnosed as either affective or psychotic, in equal proportions. The difference between the historical mania and insania simplex appears to be one between psychotic excitement and a quieter condition characterized mainly by thought disorder. For insania simplex cases, 80% were re-diagnosed with a psychotic condition in the ICD-10; the remaining 20% had ICD-10 diagnoses of nonpsychotic bipolar disorder, major depression, dysthymia, or personality disorder. The most common ICD-10 diagnosis was severe depression (57 cases, i.e. 27%), of whom 75% had psychotic symptoms. Another two had severe depression as part of a bipolar disorder. A relatively small number (21, i.e. 10%) of the cases were re-diagnosed as schizophrenia according to the ICD-10. In the modern cohort from 2011 there were 52 cases out of 1384 (3.8%) with schizophrenia.
Diagnoses in the modern cases
The modern cohort from 2011 was distributed across all the ICD-10 groups. Diagnoses within the affective group (F3) were the most common (22%), closely followed by neurotic disorders (F4, 20%). Substance use disorders (F1) and psychotic disorders (F2) were equally common (17% each). Personality disorders (F6) were less common (10%), and the remaining categories – organic (F0), physiological (F5), mental retardation (F7), psychological developmental disorders (F8) and behavioural and emotional disorders (F9) – were relatively rare, varying between 2 and 4%. Patients with physiological disorders in the modern cohort mainly had diagnoses of eating disorders, whereas the historical cohort had only post-partum disorders.
Gender
In the historical cohort, 47% of the patients were women. There were wide variations in the gender distribution between the historical diagnoses, as shown in Figure 3. Alcoholism, for instance, was very rare in women (3%), and hysteria was rare in men (10%). Women were more represented with hysteria, hysteroneurasthenia, melancholia and psychosis (most often puerperalpsychosis). Interestingly, neurasthenia was more common in men (59%) than in women. However, there was another, much less common, diagnostic category called hysteroneurasthenia, which was more common in women (69%). Among the neurasthenia cases, only 7% were subclassified as neurasthenia sexualis; this diagnosis was only used in men.

Gender distribution (% women) in historical diagnostic groups in 589 admissions for mental illness to a Swedish general hospital 1896–1905; in total, 47% of admissions were women. (Others = Amentia, Apoplexia cerebri, Dementia, Hypochondria, Hysteromelancholia, Idiotia, Insania epileptica, Intoxico phosphores, Katalepsia, Paralysé generale, Suicidum, Traumatic neurosis, Thrombosis arteria, Tumor hemoroides).
Medical certificates for mental hospital care were issued about equally often for men and women (105 men versus 103 women). Figure 4 shows the gender differences across the diagnostic distribution in the re-diagnosed historical cases, and in the modern cohort in which 53% were women. The gender distribution in the historical cases re-diagnosed according to the ICD-10 was remarkably similar for the diagnostic categories that occurred in the historical material (organic disorders, psychoses, affective disorders, physiological disorders). None of the patients with an alcohol abuse diagnosis in the historical cohort had a medical certificate, which suggests that such patients were not referred to mental hospital care. This correlates with the absence of substance abuse diagnoses in the reports from the Royal Board (see earlier). Other categories that occurred in the modern cohort, but were rarely or not at all re-diagnosed in the historical cohort, were anxiety disorders, personality disorders, autism spectrum disorders and behavioural and emotional disorders.
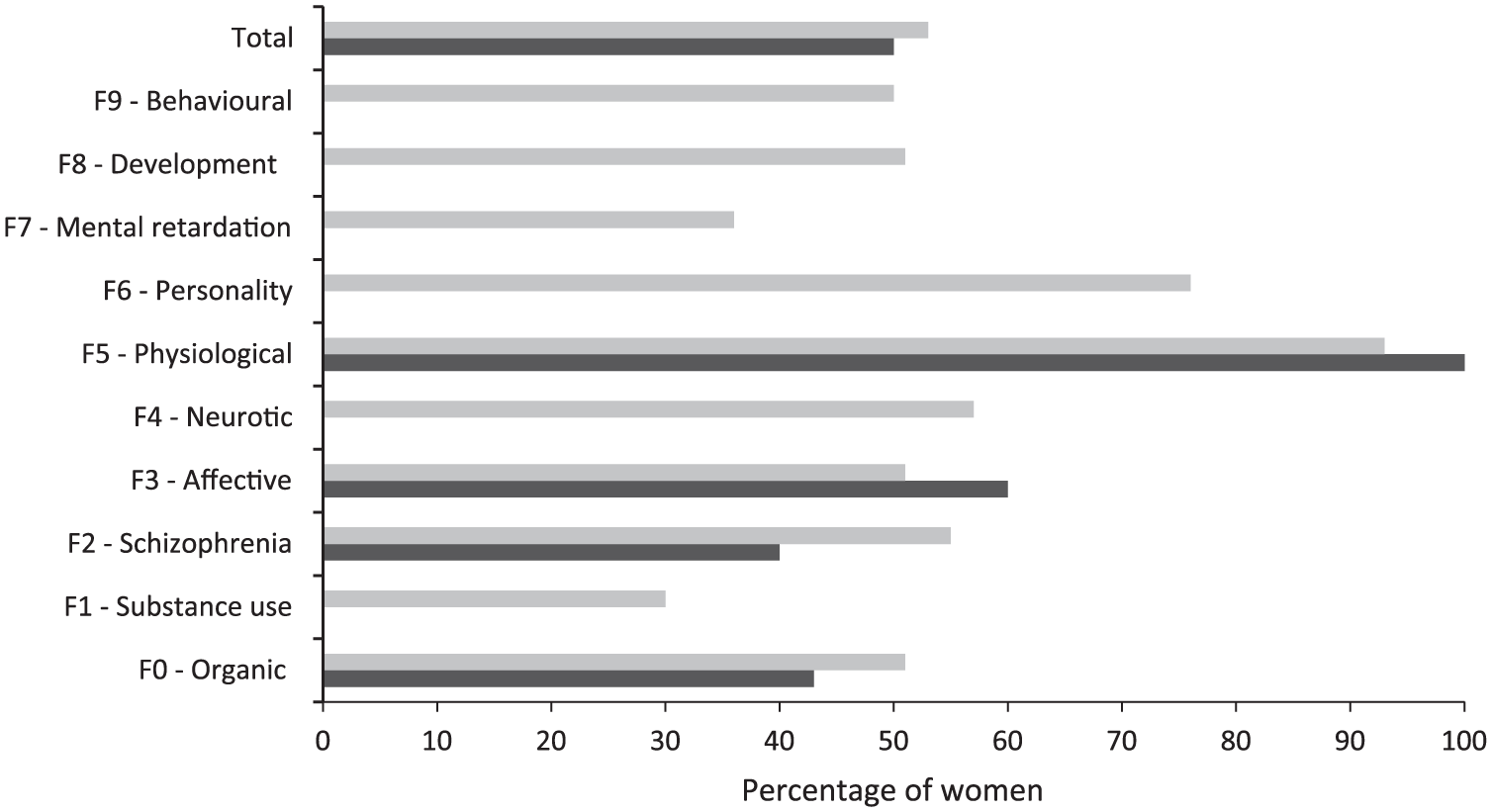
Gender distribution (% women) in ICD-10 diagnostic categories in patients with a psychiatric condition admitted to a Swedish general hospital in 1896–1905 and referred to a mental hospital (208 admissions, rediagnoses based on medical certificates; black bars), and patients admitted to the psychiatric clinic of the same hospital in 2011 (when all patients were cared for in the same hospital; 1384 admissions, grey bars). The ICD-10 groups are listed below Table 1.
Discussion
In this study of psychiatric case records from the years 1896–1905 from a general hospital in a middle-sized town in southern Sweden, there were several similarities to the diagnostic panorama of today. Referral to a mental hospital occurred in 36% of the patients, and these patients had very low GAF scores, comparable to those of patients admitted for involuntary psychiatric care in Norway today (Hustoft et al., 2013). The patients who were referred to the mental hospital almost always had psychotic symptoms, while patients with nonpsychotic diagnoses such as neurasthenia and hysteria were virtually never referred. There was a modest over-representation of men among the Kristianstad General Hospital admissions, possibly due to the more favourable economic status of the men – there was a fee for general hospital care, while the care in the mental hospital was free and paid for by the state. There was no gender difference in admissions to the mental hospital.
The medical certificates for admission to the mental hospital were of sufficient quality to allow re-diagnosis according to modern principles (ICD-10), with satisfactory reliability. For some conditions, the diagnostic labels were very similar to the modern ones, for example melancholia. For others, the labels differed but the conditions were still recognizable today. Thus paranoia, psychosis and insania simplex were almost always re-diagnosed as psychotic disorders, while mania could not be re-diagnosed as easily.
The modern concept of mania entails a condition with pathologically elevated mood and over-activity. The diagnosis of mania in the historical cohort could, however, be re-diagnosed not only as mania according to the ICD-10, but also as depression, psychosis or an organic disorder. The more restricted use of the term mania in modern diagnostic systems probably reflects the development of the concept of manic-depressive disorder by Kraepelin (1916) and his followers, and later of the bipolar disorders where mania represents one of the poles.
Our findings are generally in line with the study by Healy et al. (2005) of case records from 1896 in a Welsh mental hospital. They were able to re-diagnose the patients according to the ICD-10, suggesting that the historical cases were sufficiently similar to the modern ones to allow this. A later study from the same hospital (Harris et al., 2011) focused on melancholia and likewise found support for the continuity of this condition for the last 100 years.
A popular medical book from 1902 states that ‘The madhouse doctors are far from agreement concerning the classification of mental illnesses’ (Lütken, 1902: 464; our translation). Psychiatric diagnostics is and has been a subject of lively discussion. Many current diagnostic labels have ancient roots, but their meaning and use have varied over the centuries. For example, the concept of melancholia described by Robert Burton in his classical Anatomy of Melancholy appears to the modern psychiatrist to cover not only melancholia, but also several anxiety disorders as well as obsessive-compulsive disorder, not to mention several personality disorders. Other terms, such as neurasthenia, became very popular for a limited time (Leonhardt, 2002), only to disappear almost entirely after a few decades. Does this mean that the spectrum of conditions changes over time, or does it mean that the conditions remain more or less the same while labels change (Berrios, 1999)? Our study favours the second alternative. Although the diagnostic labels in our historical material are not always recognizable, the conditions are.
Neurasthenia, which was the most common diagnosis among the psychiatric patients admitted to the general hospital in Kristianstad, is probably an example of a condition with a symptomatology that remains the same, although diagnostic labels change. It was the most common diagnosis at Elizabeth General Hospital in London in 1880 (Hankoff, 1991). The Google Ngram Viewer program illustrates the rise and fall of the neurasthenia concept very well: neurasthenia was a commonly used word at the end of the nineteenth century and the beginning of the twentieth; it more or less disappeared after World War I, and was apparently supplanted by ‘neuroses’, which disappeared as a diagnosis in DSM-III in 1980, and was succeeded by anxiety and personality disorders, particularly borderline personality disorder (Ngram, 2016). Sigmund Freud’s suggestion that the neurasthenia concept was over-inclusive, and that cases of neurotic anxiety should be separated from it (Freud, 1895), was probably part of the reason for the loss of popularity the concept encountered after the end of the First World War.
A reliable re-diagnosis of the neurasthenia patients in our historical records was not possible because they were never referred to the mental hospital. Only brief descriptions of symptoms were available in the case notes, but these were consistent with an ICD-10 diagnosis of an anxiety disorder (and sometimes with a personality disorder, or a neuropsychiatric condition). During most of the twentieth century, the diagnosis would probably have been ‘neurosis’, until DSM-III, the third version of the American psychiatric diagnostic system (APA, 1980), tried to eradicate this term, substituting it with anxiety and personality disorders, respectively (Townsend and Martin, 1983).
Most often neurasthenia is described as a typically female condition (Johannisson, 1994; Taylor, 2001). This is in contrast to our finding that the diagnosis was more common in men. Swedish health statistics from the early twentieth century show a female over-representation in urban populations, while there are relatively more men with neurasthenia in rural populations. There is also a lasting trend in the male over-representation in the rural population, which tends to decrease with time (BiSOS, 1896–1905). Possibly, this trend reflects a decreasing social status of the diagnosis.
Another explanation may be that doctors in the nineteenth century had similar difficulties in diagnosing depression in men to those described today, with ‘male depression’ showing a different psychopathology compared with the more common female variety (Rutz, 2001). Some support for this notion may be derived from our finding that the cases re-diagnosed as ICD-10 F3 (affective) cases are less often men (40% of the cases) than in our modern affective cohort (49% men). Neurasthenia cases were often described in the case notes as a result of untoward events and were characterized by fatigue and passivity, which suggests a depressive component (Beard, 1869). An ongoing study of subsequent suicide in our historical cases may shed further light on this.
The next largest diagnostic group of patients who were hardly ever referred to the mental hospital was hysteria, and here the classical gender difference was upheld, with a female proportion of 90%. The term hysteria appears to include cases that would today be referred to as somatization disorders, and emotionally unstable personality disorder. There were no cases of conversion, the type of symptoms that were considered most typical for the diagnosis during the twentieth century, until the category finally disappeared in the DSM as well as the ICD classifications (Fink, 1994).
No patient was referred to mental hospital care for the sole diagnosis of alcoholism, but alcohol abuse was a comorbid diagnosis in 22% of the patients who were referred to the mental hospital for a psychotic condition. Interestingly, a very similar frequency of comorbid alcohol abuse disorder in patients with schizophrenia has been reported more than 100 years later: 24.6% in a study in the USA (Tsai and Rosenheck, 2013) and 25.7% in a sample of Australian patients (Sara et al., 2014).
The last century saw many revisions of psychiatric diagnostic systems. Some diagnostic categories, like hysteria, have disappeared entirely, while new ones, such as the bipolar disorders, appear (or reappear). In spite of this, the underlying disorders appear to have been relatively stable over the years. According to GE Berrios (1996: 1), the vocabulary of mental symptoms was composed in Europe during the first half of the nineteenth century and has been surprisingly stable. The detailed descriptions by a general physician who worked more than a hundred years ago are well recognizable to the modern psychiatrist and can be re-diagnosed with some confidence using a more modern diagnostic system.
Apparently, meticulous descriptions of patients and their symptoms in the case records last longer than diagnoses. Systems of diagnosis and classification are volatile, but the pattern of signs and symptoms displayed by patients appear to change less with time.
Footnotes
Appendix: Examples of patient cases from Kristianstad hospital
Man 30 years, trader. Treated 6 days, 1898.
Had typhoid fever 8 years ago, otherwise healthy. Says he has a couple of drinks every day because, as a trader, he must drink with his customers. Now complains about severe insomnia, and in recent weeks he has hardly slept at all – no sleep at all last night. Tremors in the whole body. Sees rats and mice everywhere in his home.
Diagnosis: Delirium tremens.
Treatment: Chloral, morphine, cognac (tapering dose), bromine.
Discharged healthy.
Woman, 38 years, maid living on the poorhouse. Treated 27 days, 1900.
Has always had delicate health, but no severe illnesses. Around 10 years ago, she was treated for complaints similar to those of today for 10 months. On discharge at that time, she was in good health. Around one year ago, the patient was once again afflicted with her old complaints: tiredness and faintness, dizziness and humming inside the head, palpitations, vomiting, tremors and tensions in arms, legs and throat.
Diagnosis: Neurasthenia.
Treatment: Castor oil, breakfast test, infusum amarum with bicarbonate.
Discharged improved.
Woman 23 years, maid. Treated 29 days, 1898.
Has felt nauseous for about 14 days. Ache in the stomach, in the limbs, “all over the body”. Headache. Somewhat tender in the abdomen. Menstruation not fully complete, usually followed by ache in the abdomen and headache. Menstruation is now very abundant and goes on for 5-6 days. No appetite. Stools normal.
Diagnosis: Hysteria.
Treatment: Infusum ferri amarum, warm bath, salicylic acid, valeriana, china.
Discharged improved.
Woman 55 years, tenant wife. Treated 22 days, 1898.
Well brought up, given a normal education, confirmed, had a good home, married since autumn 1868, lived in a calm and peaceful marriage, and engaged in normal housewifely activities. Lived under good economic conditions.
Has had 11 children, 8 of which are still alive. Sleeping problems lately. Loss of appetite in the past week. Kept herself clean. Serious and edgy. Increased worry. Depressed and melancholic. Has not been violent, but 3 months ago tried to cut a vein in her arm. No desire to work. Feels she is possessed by evil powers, sees snakes in the window. Afraid of the slightest sound. Anxious, worried look. Depressed mood, cries. Slowed thinking and movements.
Diagnosis: Melancholia.
Treatment: bromine, chloral. Given a medical certificate for hospital care and taken to Lund Mental Hospital.
Man 21 years, farmer’s son. Treated 64 days, 1902.
From six days ago, more difficulty sleeping, more worried, loss of appetite. Has become more hot-tempered. About 3 weeks ago, became more melancholic, absentminded, had difficulty performing work duties. A change occurred about a week ago, more excited. Laughed when he read, outspoken without cause. Became increasingly violent against people he had previously been close to. Has had false notions, in the first week he thought that people around him were Russian spies and sawfilers, and has subsequently in his excited state talked about many people, kings, ministers, etc. Gabbled volubly. Slept a bit in recent nights when he was successfully administered sleeping medication (trional, and bromine sedative) but otherwise negligible sleep.
A somewhat lethargic look, depressed and melancholic. Excited, talks incessantly, constantly switching from one subject to another, swears and talks about devils, kings, cousins, a whole lot of people, spits, kicks, etc, etc. Loses attention. Unclear understanding. Poor memory. Accelerated thought process. Rapid switches in thoughts. Has had a couple of periods of melancholia earlier in life.
Diagnosis: Mania acuta.
Treatment: trional, bromine. Given a medical certificate for mental hospital care.
Discharged improved.
Man 32 years, labourer. Treated 122 days, 1898.
Illegitimate. Has been fond of strong drinks. Unmarried. Perceived as strange, 1892. Treated in 1896 after being taken into care on the boat to America because of insanity. Saw snakes, felt persecuted, showed a revolver on the boat. After that, hid in the forest and was found emaciated. Was then worried and afraid, felt that everyone was persecuting him. Treated for 182 days in hospital in 1896, but according to relatives he could not look after himself after discharge. Received care on a farm, but was violent.
Came with his employer to the hospital again in 1898. Sleeps poorly. Does not dare to eat but is hungry. Believes that England has issued an authorization to Sweden about his execution. This cannot happen as long as he starves himself and does not sleep. Has had false perceptions for many years.
At the examination he is calm, talks about incomprehensible things with no coherence. Is worried about being killed. He sat calmly studying his newspaper and said “that was a long will you are writing and I understand what it was about” and then started a long speech about a Russian steam boat, about the Russian tsar, about trade unions, engagements, execution, etc., but with absolutely no coherence. He talks about an engagement between himself and a senior nurse at the hospital, who wanted to protect him, when they wanted to ‘nail’ him at the hospital. On the English steam boat, he claims that they wanted to nail, burn, ‘box’ and execute him; that there were 2 Italian executioners on the boat and they had come on board last to arrest and execute him, and everyone wanted to protect him, and they are out in the hospital area. A Swedish princess, a named count and a teacher “comes to [illegible]” if Nilsson does not starve, etc.
Diagnosis: Paranoia.
Treatment: chloral and china. Given a medical certificate for mental hospital care.
Discharged from Kristianstad unimproved.
Was treated at Lund Asylum 1899. He also appears in the medical records in 1901 after trauma – had cut off his penis.
Acknowledgements
The authors thank the librarians and archivists at the Kristianstad Hospital and the University of Lund for their invaluable help. The support of the psychiatric clinic in Kristianstad and its operations manager, and of the Sjöbring Foundation, is gratefully acknowledged.
Declaration of Conflicting Interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.