
Abstract
In the early nineteenth century, physicians designed the first manufactured showers for the purpose of curing the insane. Sustained falls of cold water were prescribed to cool hot, inflamed brains, and to instil fear to tame impetuous wills. By the middle of the century showers had appeared in both asylums and prisons, but shower-related deaths led to their decline. Rather than being abandoned, however, the shower was transformed by the use of warm water to economically wash the skins of prison and asylum populations. In stark contrast to an involuntary, deliberately unpleasant treatment, by the end of the century the shower was a desirable product for the improvement of personal hygiene and population health.
Introduction
Showers are a familiar part of the bathroom landscape in which people around the world clean and preen their bodies (Euromonitor International, 2014). However, the manufactured shower first emerged from within the walls of the early nineteenth-century asylum for a purpose quite different from that of washing. 1 For over 150 years prior to the development of showering to get clean, physicians contrived devices that could pour cold water on the heads of ‘maniacal’ men and women in order to cool ‘hot brains’ and break ‘impetuous wills’. This paper uses Foucault’s genealogical approach to history to explore the arrangements that made the shower a thinkable object.
In this article, we outline a period of radical change in the medical discourses regarding insanity and the treatment of the insane during the nineteenth century. We propose that these shifts can be seen in the design and application of the shower, in addition to its naming. The article begins with unpleasant but effective hydropathic devices for the insane such as the ‘fall of water’ (Smith, 1723), followed by manufactured devices such as the ‘douche’ (Pinel, 1806a) or ‘shower bath’ (Stock, 1805). Towards the end of the nineteenth century, the use of the shower as a treatment for insanity fell out of favour. However, the shower was transformed into an ‘ablution system’ (Delabost, 1875) and re-emerged as a pleasant and economical device for washing the skins of the population.
The birth of the shower
The happy consequences of the cold shower, the psychological effect of the unpleasant surprise which interrupted the course of ideas and changed the nature of sentiments. (Foucault, 2001: 253)
While the use of water to treat mental illness can be traced back to antiquity, accounts suggest that modern medical science appropriated water to cure insanity quite by accident in the mid-seventeenth century: This invention, supposedly dating from the middle of the seventeenth century was the fortunate result of chance: a heavily chained madman was being transported on an open wagon; he managed, however, to free himself from his chains and jumped into a lake, tried to swim, fainted; when he was rescued, everyone thought he was dead, but he quickly recovered his spirits, which were abruptly restored to their natural order, and he ‘lived a long time without experiencing any further attack of madness.’ This anecdote supposedly enlightened Van Helmont, who began to plunge the insane indiscriminately into the sea or into fresh water; ‘the only care that must be taken, is to plunge the sufferers into the water suddenly and unawares, and to keep them there for a long time. One need have no fear for their lives’. (Menuret, n.d., quoted in Foucault, 2001: 167–8)
After a century of plunging patients into water, Van Helmont’s methods were considered ‘exceedingly reprehensible to a well-informed physician of the present day’ (Davis, 1806: xlvii). However, it was neither the water treatment nor the lack of regard for bringing someone close to death that the early nineteenth-century physicians considered reprehensible. Rather, it was Van Helmont’s lack of discrimination about who and what should be treated with water that was considered primitive.
The late eighteenth-century saw a growing interest in the potential for medicine to cure the insane. It was argued that medical treatment was needed not only to save the individual, but for the benefit of the nation. In England, for example, the House of Commons was advised that there were: many thousands, perhaps some tens of thousands, of our fellow beings, languishing in the hopeless confinement as incurable Lunatics, who, under a better system of treatment, might have been useful, safe, and happy members of society … incurable Lunatics, cost the State about six hundred pounds each upon average, besides the loss of a subject; while the cost of cure, in those that recover, averages about forty pounds only. (Bakewell, 1815: 7–8)
The ‘well-informed’ physician aimed to establish authority over the diseases that caused insanity, naming their limits and possibilities. 2 These physicians used a science of ‘minute and accurate observation’ (Pinel, 1806b: 1) that aimed to pinpoint the nature and expression of the disease and document the effects of prescribed treatments. Various apparatus that harnessed therapeutic forces emerged during this time to aid in curing those diagnosed as insane. The shower was one such apparatus.
Showers for cooling the hot brain
The mind cannot act with precision on a disordered brain. (Rowley, 1793: 10)
A quality that defined mania in the 1700s was a violent heat that boiled the blood and dried out the brain (Foucault, 2001: 129). Thus, cooling the brain seemed an obvious solution. Dr Blair was an early proponent: Dr Blair, who in a Letter to Dr Baynard, declares, That he cured a Man raving mad, who being bound in a Cart, stript of his Clothes, and blindfolded, that the Surprise might be the greater; he on a sudden had a great Fall of Water let down on him from the height of twenty foot, under which he continued so long as his strength would permit: and after his Return home, he fell into a Sleep, and slept twenty-nine Hours, and awaked in as quiet a State of Mind as ever, as so had continued to the time of writing that letter, which was twelve Months … a hot Brain being the Cause, perhaps, of several disorders in the Understanding, and is in great part found to be true, in the ridiculous behaviour of some drunken men, which, when their Heads are become cool, abhor what they before did do or say. (Smith, 1723: 44–5, original emphasis)
Such observations reflect an agreement among physicians of an abnormally hot brain being the cause of a mad mind, and the brain being susceptible to the beneficial effects of shock and prolonged pouring of cold water on the head. While the description of the hot brain would change over the following century, the principles of the ‘fall of water’ would remain largely unchanged.
Towards the end of the eighteenth century, physicians pinpointed the blood vessels in the brains of the insane as the specific site of disorder. 3 The brains of lunatics, having been opened up and examined, had shown signs of inflamed and distended vessels (Haslam, 1798; Rowley, 1793). The movement of blood within the brain had been hypothesized to be subject to the passions and focus of the mind; ‘Madness is commonly caused by a gradual, slow, and continued determination of the blood to the brain from pathemata animi, 4 or meditation on one subject, until the fluids of the brain become, and continue, vitiated’ (Rowley, 1793: 13). The ‘hot brain’ came to be described as ‘inflamed’, and congestion within its blood vessels or nerves was viewed as either caused by or causing the chaotic mind. The science of hydropathy observed that cold water could counteract inflammation of the joints, ears, eyes, navel, mouth, throat, skin, intestine, abdomen, and around broken bones and other wounds; reduce the heat associated with fevers; cure headaches and toothache; and prevent congestion of the blood (Claridge, 1842; Forbes, 1848; Stock, 1805). Physicians hypothesized that cold water’s natural qualities of constricting blood vessels would redirect blood away from the brain and towards the internal organs (Hartshorne, 1847) in order to reduce the unseen inflammation and congestion.
Therapeutic practices to reduce inflammation and congestion included bleedings, blistering, purges, and application of cold through baths and showers (Morison, 1828). It was now thought that the location of madness was within the vessels of the brain, so the practice of plunging the whole body into water came to be seen as primitive and uninformed. Knowledgeable physicians now sought to design treatments that could target the particular site of disorder (see Figure 1 5 ).

Morison’s douche bath (Morison, 1828: 167).
The different parts of an apparatus for giving the Douche, consisting of a bucket, from which a stream of water is made to fall on the head of the patient from different heights, regulated by a rope and pully, — by the cock inserted into the lower part of the bucket, the size of the stream is regulated; in this Plate is likewise exhibited a perpendicular section of a warm bath, with the position of the patient in it,— the form of spring-straps to fasten him, if necessary,— the cover of the bath, with space for the patient’s neck, and a wax-cloth tippet to carry off the cold water. (Morison, 1828: 163–4)
In Morison’s fall of water (which, reflecting its European origins, he named a ‘douche’), the patient’s body and head are arranged according to the physician’s prescription; the body is stripped, tied down, sealed in and immersed in water. The head, separated off by a collar, endures the fall of water. The physician uses the device to harness the natural forces of water, cold and gravity to reach into and reorder the brain of the patient. 6 The apparatus and body are thus employed by the physician to carry out his prescription with measured precision.
Showers for the obstinate will
The douche of cold water … directed upon the head, as well to diminish vascular activation in the brain as to repress violence, to overcome obstinacy, and to rouse the patient when indolence or stupor prevails. (Morison, 1828: 44–5)
Alongside the effect on the brain, the cold shower was argued to exert therapeutic benefit on the more ethereal aspects of insanity. 7 In the eighteenth and early nineteenth centuries, there was a close connection between the passions, the will and madness. Excitement or anger could take control of the mad mind, taking hold of attention and imagination: ‘the distraction of the mind is the result of our blind surrender to our desires, our incapacity to control or to moderate our passions’ (Sauvage, as quoted in Foucault, 2001: 85). Passions ‘assume a kind of additional power which ultimately renders it irresistible even to the most concerted efforts of the will’ (Foucault, 2001). An unbridled will could fail to moderate the passions, which could then take control of the mind and, having taken hold, overpower any potential taming influence of the will.
Cold-water showers designed to shock (henceforth referred to as cold-water shock showers) were thought to exert an influence on the will. Passion was thought to subdue passion: ‘Fear being a passion that diminishes excitement, may therefore be opposed to the excess of it … In most cases it has appeared to me necessary to employ a very constant impression of fear’ (Cullen, 1784: 153–4). Pinel’s moral treatment proposed in 1794 – that ‘one of the major principles of the psychologic management of the insane is to break their will in a skilfully timed manner without causing wounds or imposing hard labour’ (Pinel, as quoted in Weiner, 1992: 732) – sounds innocuous. However, he continues, ‘Rather, a formidable show of terror should convince them that they are not free to pursue their impetuous wilfulness and that their only choice is to submit’ (p. 732). Fear, like cold, was thought to transmit a beneficial effect on the disordered brain. 8 Fear was aroused in the patient by the shower in two ways. First, the shower started unexpectedly, and second, the shower would continue for as long as the patient could endure, thus creating in them the fear of death. The animal heat and passion of the mad were seen as power and strength rather than weakness, hence the mad could go without the basic needs of man, such as food and warmth, could demonstrate uncommon muscular strength and be considered in good health (Crichton, 1789; Pinel, 1806b). The cold-shock fall of water was therefore prescribed for an extended time, and made to fall with force in order to break down the unusually strong will of the insane. Once the passions were subdued, the weak or wild will could submit to the will of the physician, allowing a cure to be realized.
Dr Patrick Blair (1725) gives an early example in his description of his ‘fall of water’ from an abandoned 35-foot-high water tower, under which he placed a bath tub: A married woman … became mad, neglected every thing, would not own her husband nor any of the family … I ordered to her to be blindfolded. She was lifted up by force, plac’d in and fixt to the Chair in the bathing Tub. All this put her in an unexpressable terrour especially when the water was let down. I kept her under the fall 30 minutes, stopping the pipe now and then and enquiring whether she would take to her husband butt she still obstinately deny’d till at last being much fatigu’d with the pressure of the water she promised she would do what I desired on which I desisted, let her go to bed … A week after I gave her another Tryal but adding a smaller pipe so that when the one let the water fall on top of her head the other squirted it in her face or any other part of her head neck or breast I thought proper. Being still very strong I gave her 60 minutes this time when she still kept so obstinate that she would not promise to take her husband until her spirits being allmost dissipated she promised to Love him as before … I gave her the 3d Tryal of the fall and continued her 90 minutes under it … I threatned her with the fourth Tryal, took her out of bed, had her stript, blindfolded and ready to be put in the Chair, when she being terrify’d with what she was to undergo she kneeld submissively that I would spare her and she would become a Loving obedient and dutifull Wife for ever thereafter. I granted her request provided she would go to bed that night with her husband, which she did with great cheerfulness … it appear’d that in 90 minutes there was 15 Ton of water let fall upon her. (Blair, as quoted in Ingram, 1998: 74–5)
In this example, the fall of water was used to produce fear, weakening the will of the patient, making it more liable to submit to the will of the physician, and subsequently to the will of her estranged husband. The removal of clothing, binding to the chair and blindfolding, along with the fall of water, are all carried out with the intent of instilling terror, fatigue and dissipated spirits. The physician threatened further falls of water for increasing lengths of time until the patient’s will was broken, and she became the submissive, obedient and dutiful wife he would have her be. Blair’s treatment precedes the discovery of the brain as the locus of insanity. Although the treatment was directed towards the body, the target was based on the desires of the physician (as he saw proper). Blair’s shower aimed to diminish the patient’s spirit and will. She was strong, and wilfully disobedient. Blair exposes her body by stripping, blinding and binding her, and subjects it to his will. He employs large quantities of water that can provide the time and pressure needed to wear down her strength and her will (effectively dissolving her resolve). Blair’s shower aimed to tame the patient and ensure that she returned to her duties, in order to maintain the social order.
A century after Dr Blair’s patient agreed to be an obedient wife, physicians continued to employ the force and duration of the fall of cold water to treat their patients. For example, Dr Benjamin Rush (1835), in his Diseases of the Mind, advised complete government over maniac patients. As such, strapping the patient to a chair (the ‘tranquillizer chair’), applying the shower bath for 15–20 minutes and finally threatening the patient with death were considered effective strategies for resistant cases. While Blair had relied on a naturally available supply of water, later advocates of the shower such as Rush were designing buildings to suit their purposes. In the early nineteenth century throughout Europe and North America, physicians were writing on the use of architecture in the treatment of the insane (e.g. Dr Conolly (1847) on The Construction and Government of Lunatic Asylums; see also Gualandi, 1823; Guislain, 1826). They sought to design buildings and landscapes in which therapeutic practices could be built into the walls, windows, vents, gardens, bathrooms and treatment rooms of the building.
9
Under the direction of Dr Rush, the Pennsylvania insane hospital wing included a novel (and seemingly one-off) design for administering shower-baths: In a wing of the hospital, particularly appropriated to the reception of insane patients, a space, about three feet square, was left in the flooring of the galleries communicating with the cells on each story. This space was occupied by a strong wooden lattice, or grating, divided into spaces of about an inch square. As these lattices were placed in an exactly perpendicular direction, one over the other, it was easy for the medical attendant to subject the patient to any degree of impression required, by directing the water to be thrown from a height of one, two or three stories. (Stock, 1805: 152)
The physician could thus increase the force of the water (or ‘degree of impression’) on the patient by prescribing greater heights for the water to be thrown from, but simultaneously decrease it by disrupting the flow with the lattice. The building was thus employed by the physician to improve the ease with which treatment could be prescribed and administered.
While Rush’s building aided physicians in their control over the fall of water, it is unclear how the supply of water (and thus the important aspect of duration) was addressed. This issue is resolved in Guislain’s (1826) design, which enlists the roof of the building into the prescription of the cold-shock shower. The roof of the building gathers and stores the water, and the height that the water falls from is set in stone (see Figure 2). In Guislain’s shower, wood, leather, copper and bricks partake in the prescription of the shower. In 1826, patients remained bound to a chair and the attendant was positioned out of sight so that the patient would be surprised by the shower’s start and end. Various objects allowed the physician to prescribe the amount of force and duration of the treatment. The barrel provided the option of submersion in water, which could be warm or cold. The affusion shower bath (Figure 2) could be used if a more violent application were sought. Water poured in and drained away through the structure of the building, solidifying the place of the cold shower in the manufactured treatment of the insane.
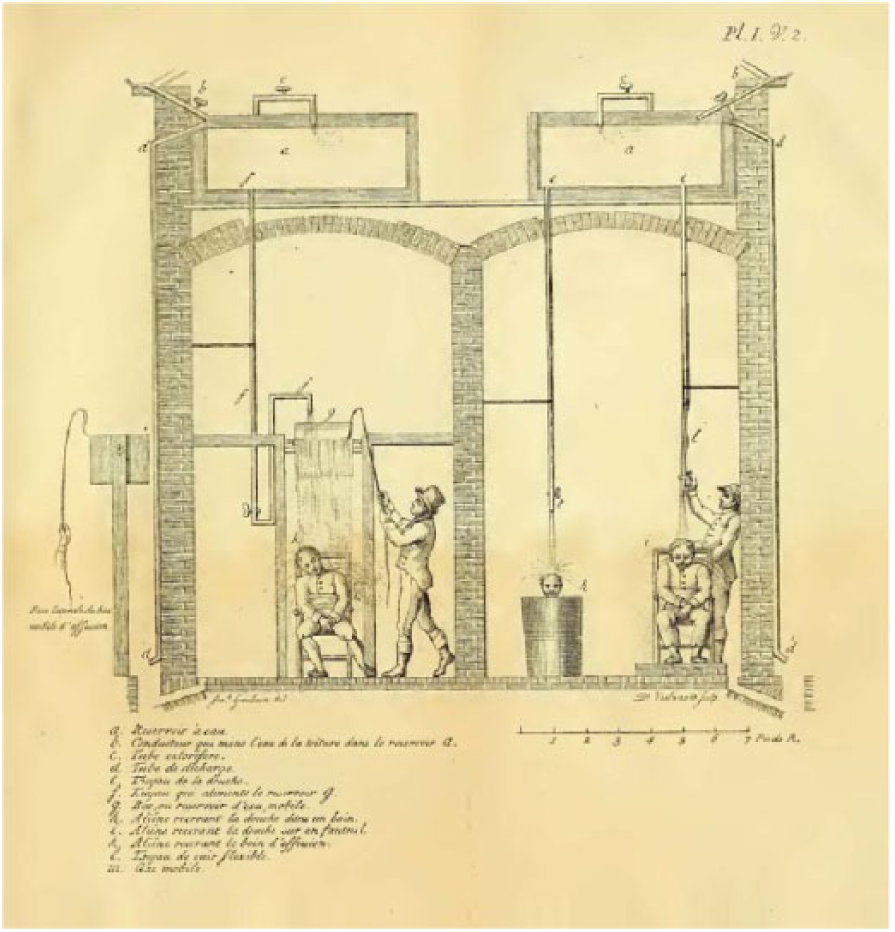
Guislain’s asylum shower designs (Guislain, 1826: 38).
The fall of water, douche and shower-bath of the eighteenth and early nineteenth centuries were born at a time when medical science had connected insanity, the will and the spirits to the body. It was thought possible that a mechanical device could harness natural forces to counteract the effects of the disease, and to diminish the patient’s will and spirit. The promise of returning the insane to being healthy, productive members of society justified building fearful devices into the walls that housed them, or bringing such devices into their homes.
The death of the cold-shock shower
The shower was the habitual punishment of the ordinary police tribunal that sat permanently at the asylum. (Foucault, 2001: 266)
The problem of wilful disobedience was of concern not only to physicians. Alongside the significant shifts in management of the insane, the mid-nineteenth century was a time of major penal reform. Although attempts were made to separate the insane from criminals through the construction of asylums and large state prisons, the distinction between insanity and criminality remained blurred. As Foucault points out, from the early nineteenth century: Every crime and even every offence now carries with it, as a legitimate suspicion, but also as a right that may be claimed, the hypothesis of insanity, in any case of anomaly. And the sentence … bears within it an assessment of normality and a technical prescription for a possible normalisation. (Foucault, 1995: 20–1)
Therapeutic devices such as the cold shower were used in prisons, to treat both the ‘obstreperous lunatic’ and those not insane (see e.g. McElwee, 1835). In the early nineteenth century, penologists were taking an interest in the corrective methods of medicine, as across Europe ‘punitive practices had become more reticent. One no longer touched the body, or at least as little as possible, and then only to reach something other than the body itself’ (Foucault, 1995: 11). The use of the body for productivity was connected to a disruption in relationship between punishment and inflicting wounds. Prior to this ‘the human body, has neither the utility nor the commercial value that are conferred on them in an economy of an industrial type’ (p. 54). As most corporal punishments were falling out of favour, punishments were sought to affect the mind, ideas and conscience of the criminal. Alongside solitude, 10 technologies such as the shower provided both physicians and prison administrators with a way to inflict ‘unpleasantness’ on the body without leaving the marks of the whip. 11
However, unlike the heat associated with inflammation of the brain and its vessels, the impetuous will was not so easily connected to a particular part of the body. While physicians argued that the soul, will and nerves were somehow connected, ‘human knowledge has not yet discovered, nor perhaps never may discover, what the soul is, how it operates on the body by means of the nerves, or how the nerves operate on the soul, and convey our will or sensations’ (Rowley, 1793: 14). This lack of connection between the mind and the body brought into question practices that targeted the body to influence the will. Although the cold-shock shower was acceptable within the original moral treatment, a new form of moral treatment emerged in the mid-nineteenth century that no longer accepted bodies being subjugated in order to induce fear.
Showers as barbaric form of torture
Aligning crime and punishment with abnormality and treatment meant that practices using violent physical force could be carried out with apparently benign intent. While Pinel (1806b) advocated the use of fear, this did not mean that the physician should be seen as a tyrant. He suggested that ‘to render the effects of fear solid and durable, its influence ought to be associated with that of a profound regard … coercion must always appear to be the result of necessity, reluctantly resorted to’ (p. 67). With the shower employed as an intermediary, the physician could act with a measure of kindness while the cold water inflicted calculated brutality: We profit from the circumstance of the bath [shower-bath], remind him of the transgression, or of the omission of an important duty, and with the aid of a faucet suddenly release a shower of cold water upon his head, which often disconcerts that madman or drives out a predominant idea by a strong and unexpected impression; if the idea persists, the shower is repeated, but care is taken to avoid the hard tone and the shocking terms that would cause rebellion: On the contrary, the madman is made to understand that it is for his sake and reluctantly that we resort to such violent measures; sometimes we add a joke, taking care not to go too far with it. (Pinel, quoted in Foucault, 2001: 267)
It was argued that, under the control of the physician, the power of the shower could be regulated, and the physician himself could moderate the suffering. However, the shower itself was not benign. While some physicians maintained that the benefit of the shower was in its potentially harmful effects,
12
the occurrence of shower-related deaths led to charges that those using the cold-shock shower were outdated and ignorant. The problem of the ignorant physician had been a concern of the state since ancient times, and legislation regulating practitioners had been passed throughout the centuries prior to the misuse of the cold shower (Barrett, 1905). By the time the 1858 Medical Act gave the UK General Medical Council support to control the education of physicians and to prosecute those deemed ignorant (Glover and Davidson, 1858), the legitimacy of hydropathy was being questioned. In defence of the practice, statements by gentlemen lecturers, the ‘most eminent among the present heads of the profession of medicine’, and works of ‘stupendous labor and research’ were used to argue that hydropathy ‘undoubtedly includes powerful therapeutic (healing) agents’ (Johnson, 1854: xxi). Nonetheless, Johnson declared that: Indiscriminate … douchings for almost unlimited periods of time may be tolerable perhaps by the phlegmatic German. But a country like England … is not likely to furnish very numerous constitutions which would bear, either with advantage or safety, the daily hammering of so powerful an engine as the douche. (p. 81).
Newspaper articles published a short time later reported deaths of the inmates of an asylum and a prison. The shower was deemed ‘frightening’ (Anon., 1866), and a ‘fearful’ example of the mismanagement of publicly funded institutions (Anon., 1858: 808). The death of a prisoner during a shower-bath punishment was used to illustrate the horror, and the shower subsequently fell out of favour (see Figure 3).
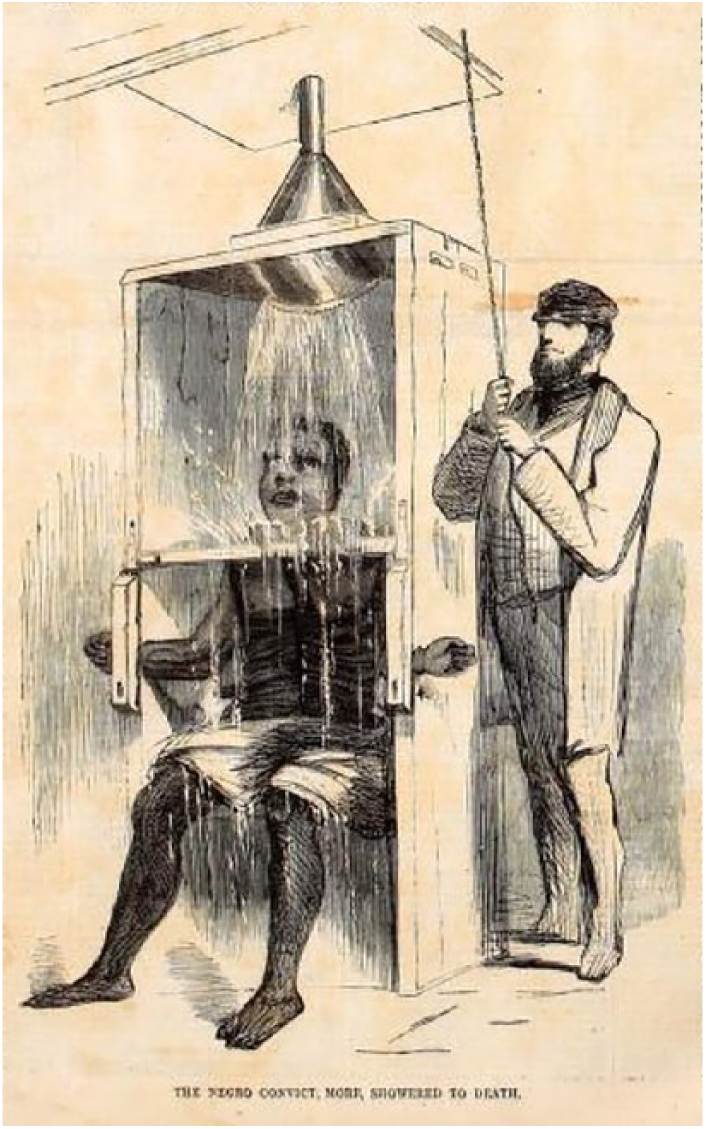
Harper’s Weekly illustrating the mismanagement of prisons (Anon., 1858: 808).
Just as plunging had been connected to the uninformed physician, showers were to become a feature of the unintelligent: ‘The efficiency of punishment depends exactly upon its tendency to increase or diminish the self-respect of its victim … Hence the growing abhorrence among intelligent philanthropists for the use of the cat, the shower bath, the ball and chain … etc. etc.’ (Prison Association of New York, 1845: 245, original emphasis). Practices that would wear down or diminish the spirit of the prisoner or the patient were looked upon in disdain: ‘Cruelty … drownings … were resorted to … to quench the spirit, to frighten men into their senses, to subdue and train, to overcome and tame the passions … we shall say little more of what is worthy of being called the Immoral Treatment’ (Browne, 1864: 4, original emphasis). By the mid-nineteenth century the inducement of fear had turned from being a therapeutic tool to a destructive aspect of the cold-shock shower: ‘the shower bath, as a means of repression or punishment would probably be destructive, by the feelings of fear or dislike which it would inspire, of all the benefits likely to be derived from their use as therapeutic agents’ (Worthington, 1851: 210). Shower-baths were occasionally used, but the purpose now was to produce ‘tranquillity’ (Winslow, 1855: 313). 13 The functions of the cold-shock shower, its ability to induce fear and to wear down the will and spirit were no longer thought of as therapeutic, meaning that practices such as Blair’s were relegated to the immoral.
The cold-water shower was abandoned by all but a few asylums (Granville, 1877). In prisons, the shower-bath was deemed ‘a relic of barbarism, a connecting link between the outrages of the inquisition and the inhumanities of the slave-pen, a process of gradual strangulation by drowning, whose existence is a blot upon the fair escutcheon of our state’ (Wines and Dwight, 1867: 166). In 1872, at the International Penitentiary Congress, the shower-bath was reported to be forbidden (‘amongst other modes of torture’; p. 26) in most prisons, but still practised in some (Wines, 1873). Despite these criticisms, showers not only endured, but their use spread and they became an ‘essential’ part of daily living.
Showers reborn in an economy of cleanliness
For the 150 years that the fall of water was used to treat and punish, the use of cold water distinguished them from something that could be used to wash a person’s body. 14 Although the possibility of using a shower to wash someone was apparent to those who used them, there was no reason to do so when warm baths were available. 15 While the 1872 International Penitentiary Congress signalled the end of showers as a form of punishment, an interest in prison hygiene expressed at this same event transformed showers from devices that touched the brains, will and ideas of lunatics and prisoners, into devices that acted upon their skin.
In society at large, the benefits of bathing were being debated during the nineteenth century, but regular bathing was generally avoided (Bichart, 1824; Webster, 1861). At the same time, enforced cleanliness was argued to be a necessary part of the system of governing patients and prisoners. Both the insane and the criminal were thought to have a particular need for washing: for insane patients, frequent washing was necessary so that ‘the peculiar odour of the insane, so often described, does not permeate every ward’ (Conolly, 1847: 40). 16 In prisons at that time, for the large majority of individuals, hygiene was said to be an almost unknown virtue, or in any case, a disagreeable practice (Delabost, 1888: 219).
However, just as cold water could reach in to modify the inflamed brain and wear down the spirit, warm water and the resulting cleanliness could also permeate into the body and exert an influence on the mental, moral and self-worth of the bather. Warm baths could soothe, refresh and allay excitement (Worthington, 1851). Washing the body had long been connected to ‘mental and moral faculties’ and was employed to improve health and self-respect: The moral influence of a habit of personal cleanliness is neither slight nor unimportant … the bath is not so absolutely necessary in cool as in hot weather; yet it is, at all times, refreshing, invigorating, healthful. Many of the employments in prisons are of such a nature that the frequent use of the bath is demanded as well to insure self-respect as to promote health; for who so degraded as not to feel a deeper degradation from personal uncleanliness? … cool water will produce a feeling of refreshment; but water, moderately warm, with soap and the brush, or even a rough towel, really restores. (Wines and Dwight, 1867: 245–6, original emphasis)
It was, however, a shift in focus to skin as the locus of disease that saw it become the primary target of washing.
In the mid-nineteenth century, the ‘modern period of dermatology’ started, and connections were established between the skin and a multitude of diseases (McCaw, 1944). Mania could be identified in the skin: ‘In those cases of maniacal excitement … functions of the skin … are greatly perverted, the surface of the body and the extremities being in most cases cool, and either moist or excessively dry and harsh, and presenting to the eye an earthy or dusky appearance’ (Worthington, 1851: 208–9). Physicians argued that skin benefited from the application of warm water to remove impurities, 17 and skin washing became an important part of managing personal health. 18 ‘Personal cleanliness is also afforded by each patient having a warm bath once a week. Where these regulations prevail, the skin of insane patients loses its most repulsive and unwholesome aspect; general health is promoted, and with health, comfort, and cheerfulness’ (Conolly, 1847: 40).
While washing was argued to benefit the health and well-being of the insane and prisoners, this institutional interest in their health and well-being was in its connection to labour viewed as a therapeutic tool within asylums (Conolly, 1847; Delabost, 1888; Pinel, 1806b; Rush, 1835). 19 Healthy skin would enable asylum inmates to work, while work would also improve the health of their skin. Worthington (1851: 201) suggested that perspiration from labour ‘seems the grand means appointed by nature to insure the healthy action of the skin’. The inability of the insane to work was thought to account for the ‘altered condition of the cutaneous surface’ (p. 201) and consequently the large number of the incurable insane that suffered fatal chronic disease. Hygiene, health and work were thus connected. 20
While good health was used to advocate for washing, the link between productivity and health had the added benefit of contributing to the economy of the institution. The good health of the inmates or prisoners allowed them to work, thus diminishing the cost of incarceration (Conolly, 1847; Delabost, 1888: 219; Pinel, 1806b; Wines, 1873). Prisoners were compelled to be clean, healthy and productive, and a ‘want of cleanliness’ was considered a punishable offence within a number of prisons. Despite the link to productivity giving reason for regular bathing, bathing was often not attended to in asylums (Conolly, 1847) and many prisoners bathed infrequently, as little as four times a year (Wines and Dwight, 1867).
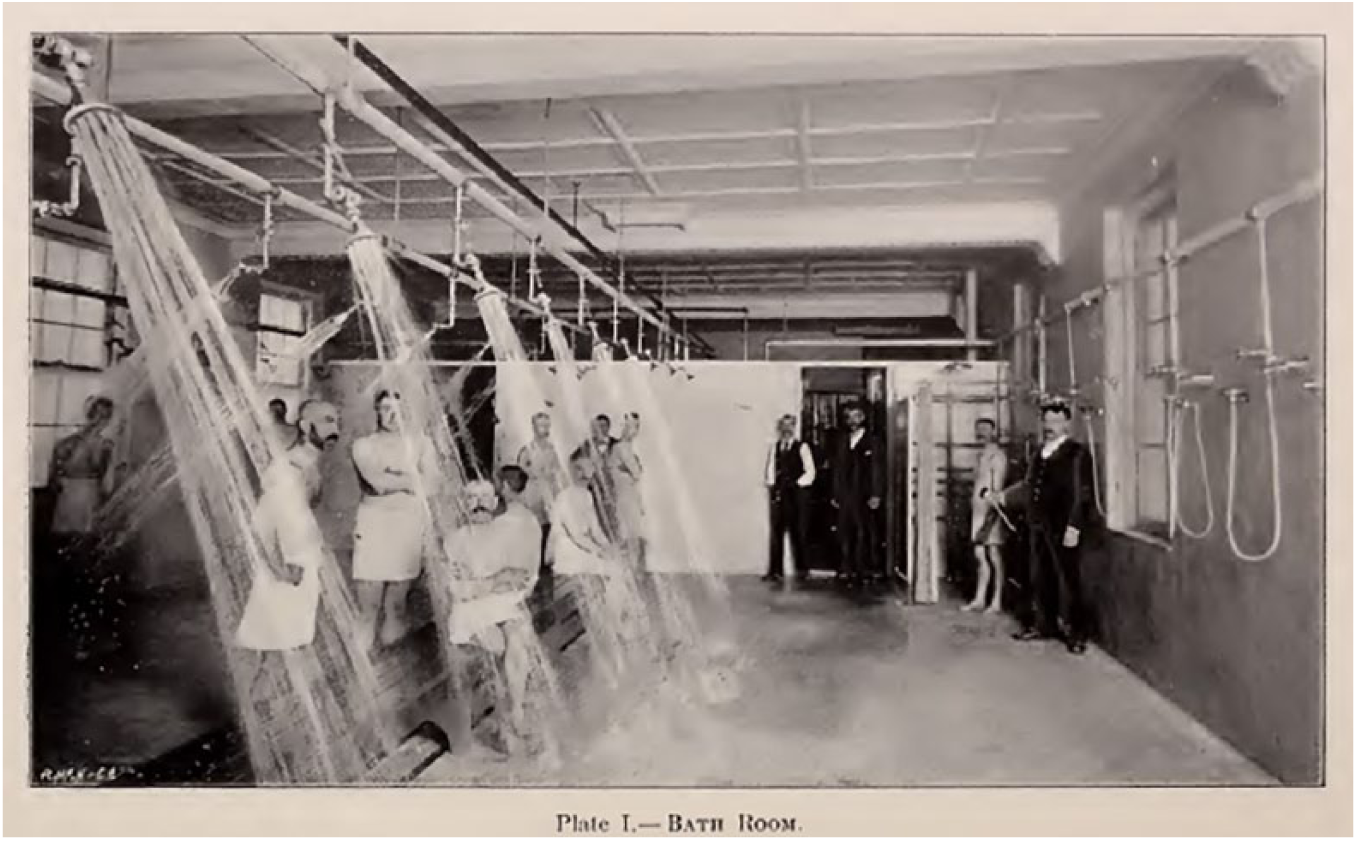
Dr Merry Delabost, a French prison physician, is credited with conceiving the idea of showers for washing. 21 Following the 1872 International Penitentiary Congress, the French government asked prison doctors what could be done to improve the cleanliness and hygiene of prisoners (Delabost, 1875). Delabost had been attempting, without success, to have cold showers installed for the purpose of hydrotherapy at the Rouen prison. 22 He proposed that the use of warm water, poured over the heads and bodies of prisoners, would be an efficient and effective way to promote hygiene. 23 The shower was reported to encourage the prisoners to scrub (with the assistance of soap), thus detaching impurities that the water (running over the surface of the body) would then take away (p. 115). He employed a cellular design (see Figure 4), which prisons had been using for some time to separate prisoners and improve the ease and efficiency of surveillance. It was argued that guard surveillance was necessary during washing, as most prisoners, through laziness, not caring or existing uncleanliness, neglected to scrub sufficiently to be clean (p. 114). The shower was proposed to have several advantages in this respect; in particular, the guards had an unobscured view of the body, and washing large numbers of bodies could be performed in less than five minutes (a population of 900–1200 could be showered within two days), using only 25 litres of water per person. Furthermore, the shower was reported to be very agreeable.
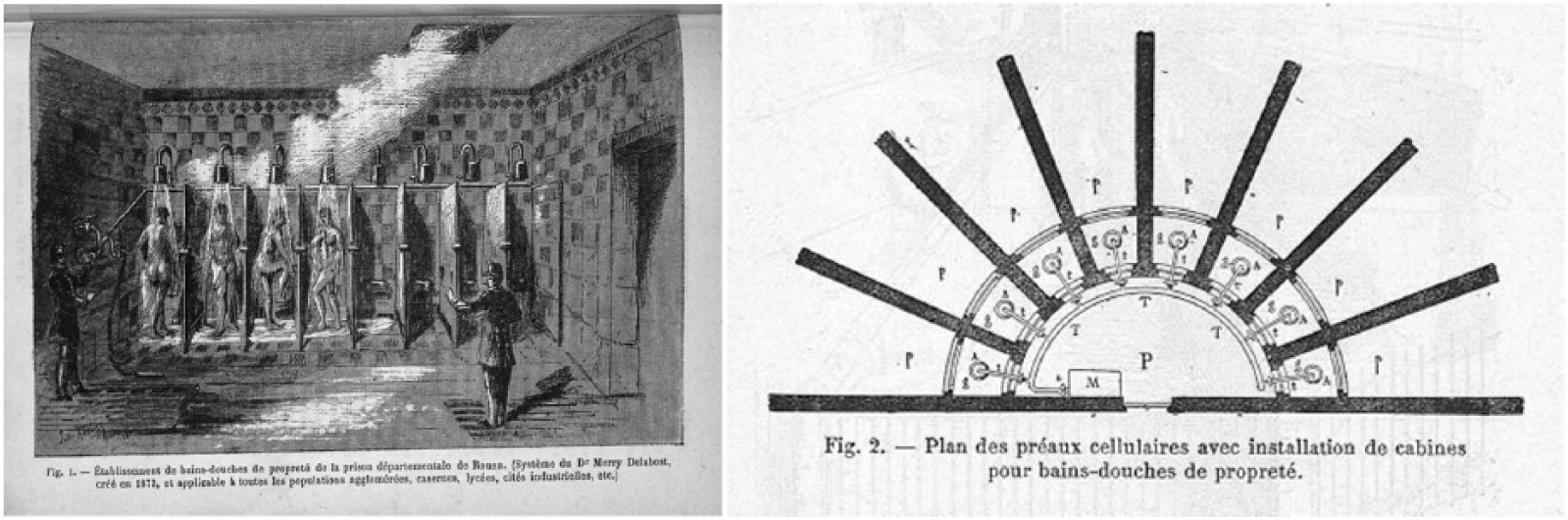
Delabost’s prison shower designs (Delabost, 1888: 223, 227).
In Delabost’s ablution system, the skin covering the bodies of the prison population was washed to ensure health and productivity; the shower functioned to wash away impurities with the greatest economy of time, water, heating and surveillance. Delabost’s efforts to improve the health of the prison population through hygiene measures drew on broader societal discourses regarding public health and productivity. Towards the middle of the century, strategies to encourage personal hygiene habits were employed as part of public health reforms. 24 The hygiene shower was a shower for the masses, and less than a decade after Delabost’s invention, Dr Lassar promoted a shower block (‘the people’s baths’) of near identical design 25 as an economical way of supplying public bathing to the poorer classes (Anon., 1896a) (see Figure 5).
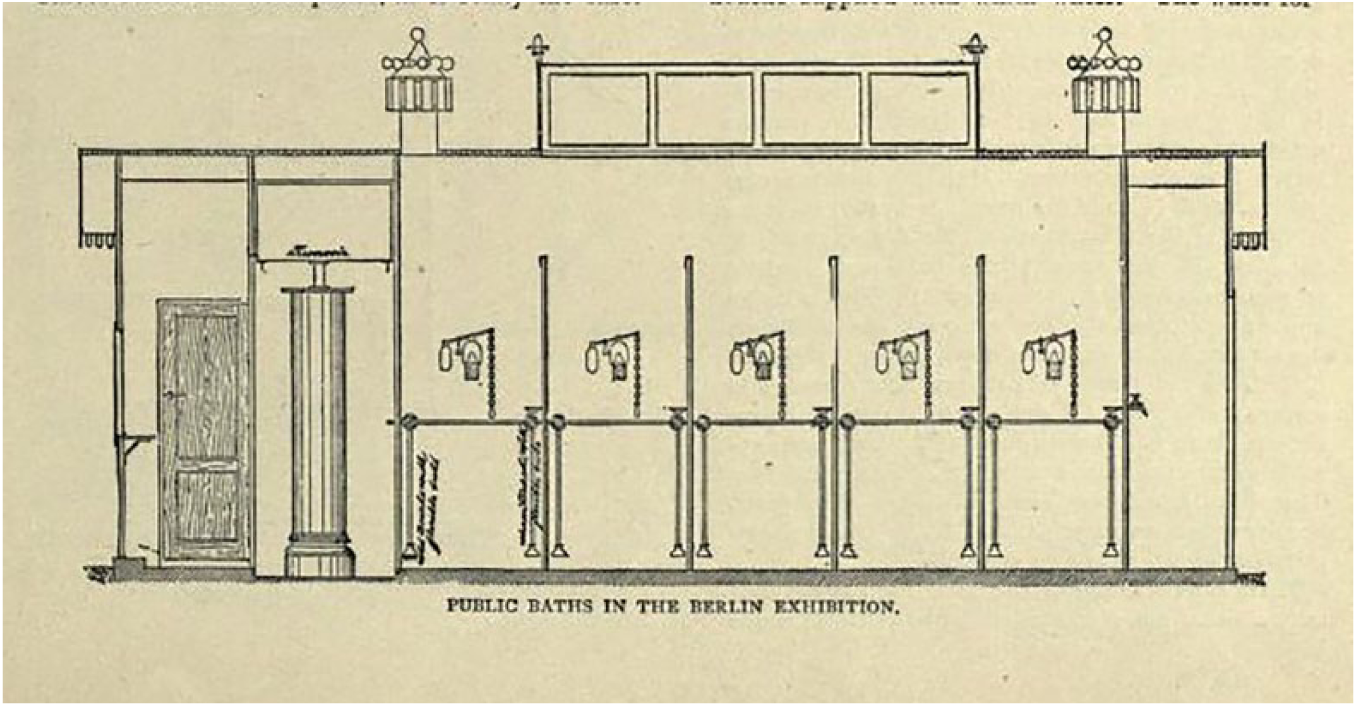
Showers for the poorer class at the 1883 Hygiene Exhibition (Anon., 1896a: 197).
By the end of the century, hygiene showers had proliferated and become a common feature of public baths across Europe (Wright and Weaver, 1897), in army barracks (Billings, 1875; Delabost, 1888), schools and factories, on ships (Gerhard, 1894b), and in athletics clubs and schools (Anon., 1896b). Showers were also available in the British colonies (Anon., 1892).
The hygiene shower, as an object of economy rather than therapy, became the domain of the engineer rather than the psychiatrists, with showers installed in asylums according to engineering plans and specifications (Gerhard, 1894b). Indeed, Gerhard (1895) argued that baths were now the enemy of the asylum and should be abandoned as they were costly to maintain, time-consuming to use, dirty, harmful, wasteful of water and dangerous (in terms of spreading disease, scalding, being used for suicide). At this time, showers of various designs appeared for washing the insane, including the ‘needle bath’, ‘hand sprays’ and ‘rain baths’ (Gerhard, 1895). The rain bath, in which the shower head was angled on the incline that is familiar to us today, was said to be the desirable option, as it could avoid ‘the shower striking the head of the bather, which to many persons is quite disagreeable’ (Gerhard, 1894a). The shower, once designed to be unpleasant and to target the head, could be used without the head getting wet at all, and thus avoid any unpleasantness! Furthermore, the rain bath would avoid the need for an attendant to assist with showering, and would avoid the undesirable impression that patients might be showered against their will (Gerhard, 1895) (see Figure 6). Such showers were vastly transformed from the fall of cold water that Dr Blair had employed to cure a wayward wife. The sudden shock, the fear and unpleasantness, and the cooling effects on the maniacal brain were all exchanged for agreeable, efficient application of warm water and soap, for the purposes of clean skin and health.
Bathroom of the Utica Psychiatric Centre (Gerhard, 1895: 34).
Conclusion
Shifts in knowledge through the nineteenth century made the shower thinkable, first as a device to aid in the treatment of the insane, and later to wash the skins of the masses. The well-informed physician’s understanding of the brains, minds and wills of the insane led to the manufacture of an artefact that would induce therapeutic cold, shock and fear. The ideas that governed the practices of the physicians and the lives of their patients materialised in the various shower designs, and in their construction, the ideas were made durable and could proliferate. However, when the cold fall of water fell out of favour, the shower was reborn. Connections were formed between skin, health and productivity, and the failed hydropathic shower was transformed into an effective and efficient machine for bringing hygiene to the masses. The ‘dosage’ of an hour and a half was reduced to five minutes and 15 tons of water reduced to 25 litres. The shower now served the good of the nation by washing away the impurities of the masses with the minimum of expense. The shower went from being a device intended to inflict unpleasantness to one that was very agreeable. So agreeable, in fact, that the following century would see populations calling for showers to be provided for them, and the mass production of shower units that people could purchase for their own homes.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.