
Abstract
The so-called ‘Kirkbride Plan’ is a type of mental institution designed by the American psychiatrist Thomas Story Kirkbride. The Kirkbride-design asylums were built from 1848 to the end of the nineteenth century. Their structural characteristics were subordinated to a certain approach to moral management: exposure to natural light, beautiful views and good air circulation. These hospitals used several architectural styles, but they all had a similar general plan. The popularity of the model decreased for theoretical and economic reasons, so many were demolished or reused, but at least 25 of the original buildings became protected places. Over the years, surrounded by a legendary aura, these buildings have become a leitmotif of contemporary popular culture: ‘the asylum of terror’.
Introduction
During the nineteenth century, the USA was a mosaic of rural enclosed communities. Face-to-face relationships and social solidarity prevailed. In this context, disease was seen as a community problem which, when it affected a family also affected the group. Insane asylums did not exist, so the care of a mentally ill patient was a family matter. It was common, therefore, for villages to subsidize families with a mentally ill member; and when the family unit – or the community – was unable to support them, they inevitably ended up in a poorhouse, a jail, or an inappropriate almshouse (Grob, 1973: 10–11; see also Howard and Aleguas, 2019). In these conditions, the situation of abandoned mental patients became serious, and in 1766, guided by enlightened principles and driven by a growing popular demand, the authorities began to think about the problem. The Royal Governor for the Colony of Virginia, Francis Fauquier (1703–68), proposed the creation of a hospital whose sole purpose was to treat ‘idiots’ and ‘lunatics’. Thus, the first North American mental institution, the Eastern Lunatic Asylum of Virginia, or Eastern State Hospital (Figure 1), was founded in Williamsburg in 1773 (Osborn, 2009).
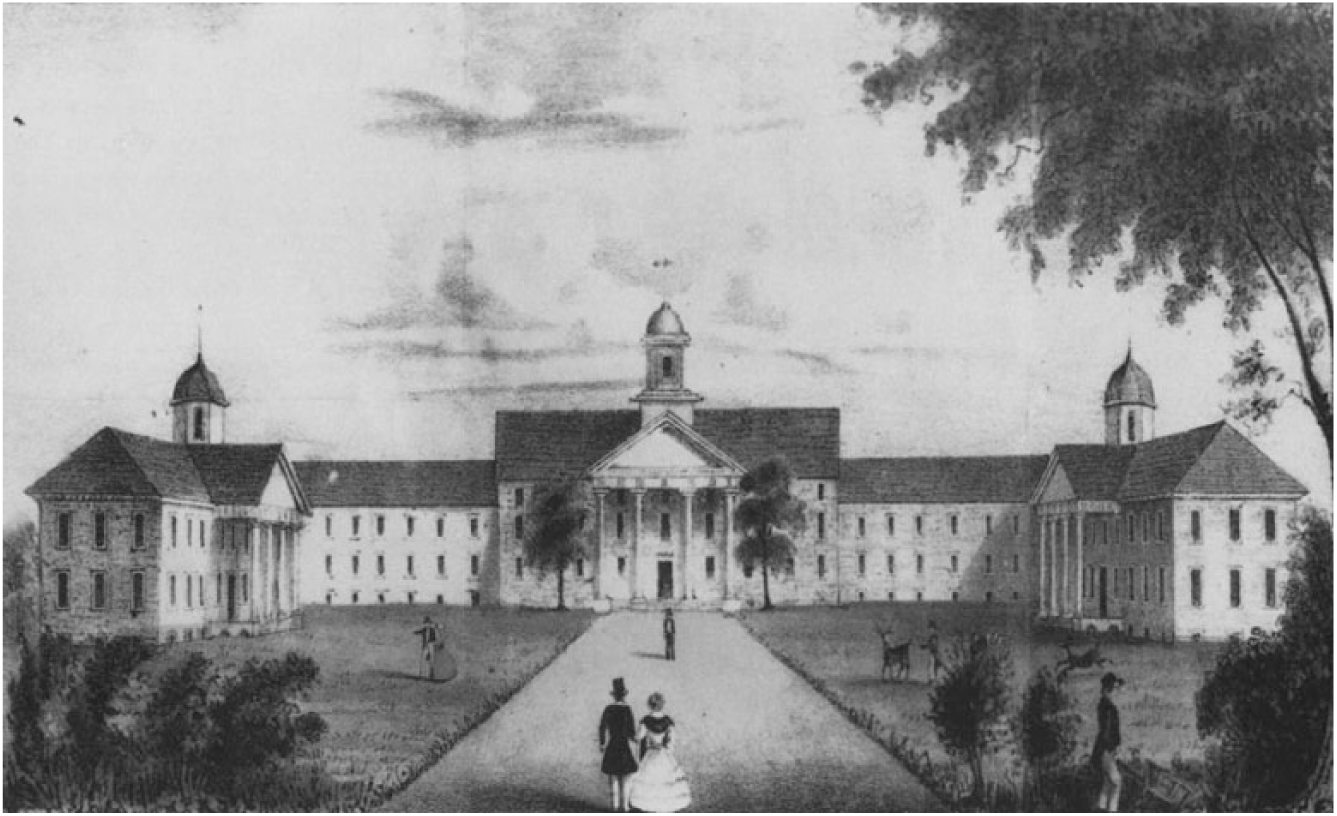
North view of the Eastern Lunatic Asylum, Williamsburg, VA. Lithograph by T.C. Millington, ordered in 1845 by John M. Galt, II, Superintendent. Galt Collection (source: Gibbs and Rowe, 1974/1990: 379).
Between 1783 – the effective year of the independence of the USA – and 1820, there was a rapid modernization of the country. It changed from a model of rural life to one with an exponential growth of cities, factories and businesses, which caused a progressive separation of family life and work. In this context, family care for the insane, and for any relative affected by a chronic disease, became a problem that was hard to resolve. There was a shortage of public hospitals, and for this reason the authorities started to set up health institutions throughout the country. In a nation that was experiencing a powerful demographic and economic explosion, the role of families in the care of their sick members had to be drastically redefined (Osborn, 2009). In the case of insane asylums, therapeutics was not a well-defined topic among the medical profession, so patients continued to be kept in prisons and care institutions (Grob, 1973: 1–34; Yanni, 2007: 11). Benjamin Rush (1746–1813) was important in promoting a substantial change in medical care in the USA; when he was chief medical officer of the military hospital of the Central Continental Army Department, he wrote a controversial letter to George Washington in 1777, giving details of the inhumane treatment of prisoners and the deplorable conditions of the sick (North, 2000).
Thomas Kirkbride
Thomas Story Kirkbride (1809–83) (Figure 2) was born into a wealthy Quaker family in Morrisville, Pennsylvania. He began his medical studies in 1828 at the University of Pennsylvania, graduating in 1832. In the same year he became the youngest resident physician on the staff of Friend’s Asylum, a Quaker mental institution that was a pioneer in the application of the so-called ‘moral treatment’; he worked there until 1840 (Cherry, 1989: 167–70). In that year, being a figure of increasing popularity in the field of American psychiatry along with his contemporary Pliny Earle (1809–42), he was appointed Superintendent of the Pennsylvania Hospital for the Insane (Tomes, 1994: 44–89). This centre, originally conceived as a general hospital, had opened in 1756 with money contributed by the local high society. However, its material conditions quickly deteriorated, and the recovery rate was only 17%; it collapsed and was temporarily closed for a few months and then, under Kirkbride’s control, it reopened again in January 1841 (Osborn, 2009; see also Howard and Aleguas, 2019).

Thomas Story Kirkbride: portrait painted in 1898 by the artist Howard Russell Butler (source: Chapin, 1898).
In 1844 Kirkbride was one of the founding members of the Association of Medical Superintendents of American Institutions for the Insane (AMSAII). Later, he would become secretary, treasurer and finally, between 1862 and 1870, President (Kelly and Burrage, 1920). His most influential work was published in 1854 and reissued as a book in 1880 with the title On the Construction, Organization, and General Arrangements of Hospitals for the Insane. This text is considered to be a key contribution to the consolidation and development of a new therapeutic philosophy in American mental institutions. His detractors, however, dismissed his ideas as overly idealistic and counterproductive to the genuine progression of medical science. In his 1854 publication, Kirkbride defended the theory that if mentally ill patients were given proper treatment they could even be cured. Indeed, after the death of his first wife, Ann West Jenks (1812–62), he married one of his former patients, Eliza Ogden Butler (1835–?). In the Pennsylvania Hospital for The Insane report for the year 1846, Kirkbride is clear about his ideas for mental health therapy (Cherry, 1989: 163). He thought that insanity was curable, in proportion to how soon the patient was given treatment, and that a rapid separation from the family scenario was usually desirable. In fact, he was convinced that at least 80% of patients could recover in a substitute home – an adoptive family – in which patients could be resocialized.
Kirkbride’s best known contribution was the architectural and organizational model that he implemented for mental hospitals, which was eventually used in many of the psychiatric hospitals built in the USA and Canada during the nineteenth century. In his opinion, the architecture of the asylums should follow a series of special guidelines that would improve the accommodation and conditions of the inmates and, consequently, contribute to their psychological improvement in an efficient manner. This model became popularly known as the ‘Kirkbride Plan’ or ‘Kirkbride Model’, and the many buildings that were based on it as ‘Kirkbride buildings’ (Hardman, 1999: 13). Each construction had its own architectural individuality, but they all contained a series of elements which made them very characteristic, for example their plan in the form of ‘bat wings’ joined to a central block (Figure 3) (Yanni, 2007: ch. 2).
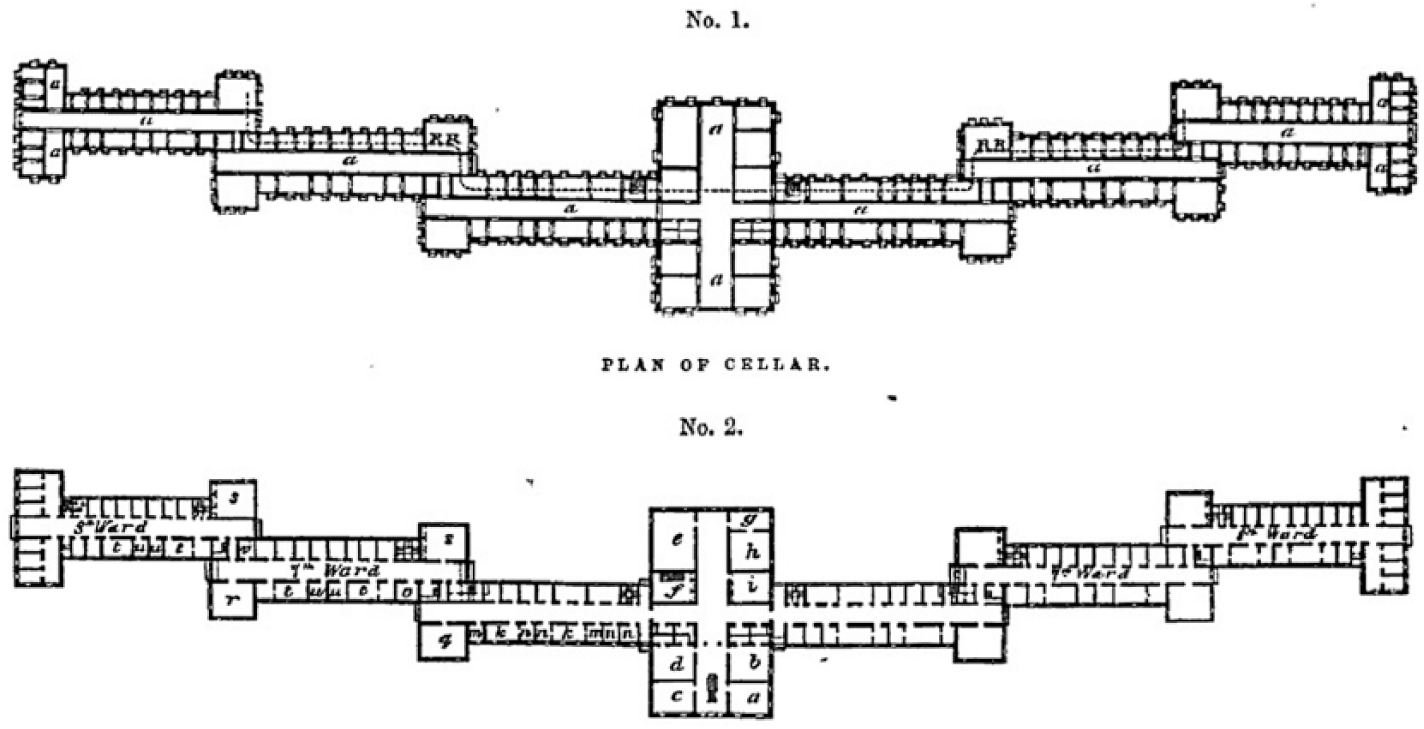
A plate from the original Kirkbride Plan project plans (source: Kirkbride, 1854).
The first building of this type erected in the USA was the New Jersey State Lunatic Asylum of Trenton, where building began in 1848; it was later renamed Trenton State Hospital. It was followed by another 72, the last being inaugurated in 1910, when the star of the Kirkbride Plan was already declining among the medical community. However, before the AMSAII certified the Kirkbride model as the best and most meticulous way to organize a mental institution, some of Kirkbride’s theoretical proposals were already in operation. They had been applied to a large extent by Samuel B Woodward (1787–1850), another co-founder of the Association and its first president; he was a convinced supporter of moral treatment, which he used at the Worcester Lunatic Asylum in Massachusetts where he was Director from 1832 (Osborn, 2009).
Principles of moral treatment
The fundamental change that led to the emergence of new therapeutic schools in the field of mental health came in the early nineteenth century, when there was a new medical attitude to insanity: that people with mental problems had moments of lucidity. They were not, therefore, irrational animals who could be treated as mere cattle (Peloquin, 1989). In fact, the torture and mistreatment that this type of patient had suffered when crowded into mental institutions – or prisons – were not designed specifically to inflict pain, but as a mere control method.
One of the first debates on the subject in the USA was stimulated by Doctor Eli Todd (1769–1833), the Superintendent of the Hartford Retreat Center in Connecticut. He questioned who should direct this new type of institution; the early superintendents were not necessarily graduates in medicine, but managers who would ensure the best conditions for the institution. In this situation, all the therapeutic emphasis was placed on moral treatment, while medical therapy was relegated to the background, since the resident physicians only dealt with bodily health. Todd, who supported an organic confrontation of insanity, increased the use of substances such as morphine and opium as a complement to moral treatment. At the same time, he campaigned to ensure that the superintendent was a qualified doctor. This debate attracted supporters to each point of view – medical model versus only administrative and moral model – and provoked several discussions, but concluded in 1850, when Todd’s criterion was imposed within the AMSAII. Thus, there emerged a second generation of asylums run by specialists who placed both types of therapies, moral and medical, on an equal footing (Scull, 1981: ch. 1). For these psychiatrists who were inspired by the philosophy of moral treatment, this second generation was defined as removing the insane from the family home and their old lifestyle, and providing respectful and kind treatment in all circumstances and, in most cases, with manual labour, attendance at Sunday religious services, establishment of regular habits of self-control, and moving the mind away from morbid thoughts (Brigham, 1847).
The idea of ‘removing’ the insane from the social environment made a lot of sense in the USA at the time. The country experienced much institutionalization, in response to a sustained population increase, but also an enormous migration to the large urban centres. The authorities made enormous efforts to build hospitals and clinics in anticipation of serious public health problems. At the same time, the pre-war circumstances extended throughout the Atlantic coast states, generating political and administrative problems at all levels, and these inevitably affected health institutions and the communications between their directors. Understandably, these difficulties also affected the theoretical and practical scope of mental health, to the point that the problems were seen as one of the reasons for the increase in the number of people with psychiatric problems. Some professionals stated that many of their patients showed moral disturbances related to the will and emotions, while their intellectual faculties remained intact. Such disturbances could be attributed to the new social tensions and the community chaos (Rothman, 2002: ch. 5).
The asylums were understood as a reasonable space, which was away from that chaos and which would contribute to improving the conditions of the patients. In fact, one of the great preoccupations of the psychiatrists assigned to the AMSAII was to replace the old ‘penitentiary’ style of language and behaviour in relation to the psychiatric centres with new ‘familiar’ terminology and rules. This not only served as a ‘cleansing’ of the image and reassurance for families and patients, but also extended to all institutional customs: the inmates could wear ordinary clothes and never uniforms; did not have to have special haircuts, identification tags or numbers; and there were no organized queues, formations or marches for the exercise of habitual tasks (Hardman, 1999: 14). From 1850, AMSAII members were inspired by the regeneration demands of the movement led by Dorothea Lynde Dix (1802–87); one of their main concerns was to improve the public image of both the psychiatric profession and the mental institutions, and this dominated many of the annual meetings of the association (McGovern, 1976).
There were great controversies about the use, in some centres, of cage beds and isolation cells, which was widely condemned by Kirkbride and others, although some people, such as Horace Buttolph (1815–98), Superintendent of Trenton, defended their use for extreme cases. The most scrupulous defenders of moral treatment also scrutinized and censured other activities, such as the use of cold water enemas to avoid nocturnal incontinence (McGovern, 1976). The idea that moral treatment could only work if it was accompanied by adequate medical treatment justified the modification by US psychiatrists of the original Pinelian theory, in order to proceed with medical interventions (Scull, 1981: ch. 1). A leading figure in the AMSAII, Amariah Brigham (1789–1849), argued that any moral disturbance was basically a brain ailment that could have been originally caused by exogenous causes, but that ultimately also required adequate medical treatment (Brigham, 1844). In short, regardless of the therapeutic emphasis, any kind of dementia was linked to an organic pathological course.
These considerations only seemed to benefit the middle and upper classes. The poor, usually imprisoned in jails and charitable institutions, very rarely experienced the advantageous conditions of moral treatment (Peloquin, 1989; Tomes, 1984: 202–3). It was argued that beggars and vagabonds, who had been exposed for a long time to disturbing environments, would have suffered severe and chronic organic damage, and therefore moral treatment would have little success. Thus, the community of excellent mental asylums that drove the theory of moral treatment became the preserve of elite upper- and middle-class physicians providing for the therapeutic needs of elite patients from the upper and middle classes (Peloquin, 1989).
The Kirkbride Plan: origin and development
The standards developed for private asylums became a model for public institutions which suddenly joined the race to attract ‘curable patients’ (Peloquin, 1989). In the mid-nineteenth century, the USA was facing a real human drama in relation to the treatment of the mental health of the most disadvantaged population groups. This situation was denounced by Dorothea Dix before parliamentarians of the legislature of New Jersey in 1844, and it was the first state to address the problem by creating a specific centre that tried to gather and use the latest advances in relation to the treatment of mental pathologies (Sheth and Imbroglia, 1999). The model public mental hospital in the USA was the Pennsylvania Hospital for the Insane, directed by Kirkbride and, considering his influence along with that of Woodward within the AMSAII, it was logical that the state of New Jersey opted to follow this innovative model (Yanni, 2007: ch. 2). The measure was applauded because the problem of poor patients was very difficult for superintendents. The old model of the insane asylum versus charitable institutions and prisons was changed to a new one: private versus public asylums (Peloquin, 1989). The example spread in such a way that in the USA the second half of the nineteenth century was a real ‘age of asylums’ (Hardman, 1999: 5). More than 70 Kirkbride buildings were constructed and, in total, 140 mental hospitals were erected throughout the country (Osborn, 2009).
Guided by the principle of environmental determinism, Kirkbride thought that the construction plan of the centres should be a basic ‘curative’ factor: only from an orderly and rationalized environment could one ‘heal’ – reorder, restructure – the mind of the patient (Rothman, 2002: 149). In his opinion, the ideal would be a linear building, with two huge tiered wings connected to a large central block that would be used for reception functions, administration, kitchens, the superintendent’s house (for Kirkbride, it was essential that he lived there), as well as other general services. This would achieve uniform illumination and adequate ventilation, while allowing a good distribution of patients according to their peculiar state and pathology, and ensuring that each of the blocks maintained a certain degree of privacy and independence from the rest. In fact, suitable classification of patients was essential for moral treatment, and this should be perfectly reflected in the physical structure of the building (Peloquin, 1989).
Nosological classifications were not clear at this time, and in general, the doctors organized the mental patients from a basic diagnostic criterion that catalogued them as manic, melancholic or demented. Subsequently, and depending on the specific manifestations of the pathology of the patient, they introduced suitable adjustments to each case. There were also criteria for the separation of inmates, such as gender, their habitual behaviours or their possible physiological ailments. On the other hand, there was a tendency to separate the noisy patients from the silent ones, and the seriously ill from the mild cases. In addition, it was expected that social class would also be taken into account for all purposes, from the quality of the accommodation to the type of tasks and occupations that would be assigned to the patient; in this way, the status of the person within the institution would reflect, in some way, their background. Logically, this implied several levels of treatment, and these criteria were applied to all possible aspects of institutional life (Tomes, 1994: 44–89).
The building should therefore have the latest technologies and be decorated according to ‘good taste’. As befits the aesthetic canon of the time, the Victorian institutional ideal would be followed: large, voluminous and ornate (pp. 44–89). Kirkbride’s ideas were restricted to therapeutic issues, and did not impose artistic criteria. Therefore, among the many new buildings of this type, the stylistic appearance was very variable, reflecting the American architectural tastes of the time, such as neo-Gothic, Edwardian and Richardsonian (Kirkbride, 1854a: 11; Howard and Aleguas, 2019; Verderber, 2010: 26). The truth is that a complete material endowment was required, with a great economic cost, to the extent that the centres were designed for extended stays; this was because the patient’s cure required, among other things, that the physical and psychic climate remain constant to keep him or her calm, balanced and away from the usual psychophysical changes outside the asylum.
Kirkbride was of the opinion that a standard psychiatric building should have at least eight pavilions in which it could accommodate, for operational reasons, no more than 250 inmates in total (Kirkbride, 1854a: 4). Each pavilion or section had to have independent nursing and guard posts, as well as its own living room, bathrooms and dressing rooms; it also had its own forklift truck and a communication system that allowed orders to be sent and materials to be moved easily between the different buildings. The arrangement of the patients had to be perfectly rationalized. The most excitable, dangerous or unpredictable had to occupy the pavilions farthest from the central body of the building – at the ends of the wings – and, progressively, patients should be placed in pavilions towards the centre, so that the calmest, the recovered and the stable occupied the blocks closest to the centre.
In order to avoid the temptation to put too many patients in a space as large as the one offered by this type of construction, Kirkbride recommended that the rooms should be spacious – for example, ceiling height should be around the 3.70 m – but not excessively, thus guaranteeing enough comfort for a single person, without allowing space for too many beds. He thought a minimum area of around 8.90 m2 for each room seemed reasonable for a maximum of two patients (pp. 15–16).
The importance of rural life was emphasized, so it was necessary to have extensive and fertile landscaped spaces, as well as a variety of landscape perspectives visible from all angles. This meant that the area for the facilities of the centre should not be less than 40 hectares and was, by necessity, far from the nearest urban nucleus (pp. 6–7). In fact, the gardens and farmland of the asylum could provide an excellent form of occupational therapy for patients who, in their lives outside the asylum, were used to this type of work (Verderber, 2010: 26).
Regarding the staff, Kirkbride determined that the standard template for this type of centre should be 71 people, parity of men and women being very important; this assumed that patients in better conditions could be used in the performance of all sorts of minor tasks. Most of the staff had to live in the psychiatric centre itself or in facilities built nearby for this purpose; their accommodation was provided free (see Table 1). The superintendent should always live in a house intended for that purpose in the central part of the building, or in a house attached to it (Kirkbride, 1854b: 125).
Minimum annual economic benefits for the employees of an asylum according to the Kirkbride Plan (based on Kirkbride, 1854: 137–8).

Apart from counsellors and the Treasurer, all employees were provided with lodgings (for Superintendent, see note 2). In the USA there was no basic salary, and interstate differences were very marked. In 1850, the average salary of an agricultural worker, for about 10 hours of work per day, was about $9.7 per month; it varied, e.g. from $7.7 in South Carolina to $12 in Texas. This means that the average annual salary of a farm worker was around $116, $92 or $144, respectively. In many places, salaries were lower because they did not include daily maintenance (Lebergott, 1960). It can therefore be said that, in spite of the obvious salary differences of men and women, and bearing in mind that the expenses of residence and food were borne by the institution, the basic or minimum remuneration stipulated by Kirkbride was generous: he was convinced that a low-paid psychiatric worker would not comply with the demands of good treatment demanded by the therapeutic plan.
The first figure was the salary of the Superintendent if his family resided in the same building, and the second if he was forced to look for comfortable accommodation for the family unit outside the facilities.
These figures are a purely explanatory gross conversion, and do not take into account the obvious economic considerations – inflation, purchasing power, monetary value changes, cost of living and so on – that would undoubtedly change them markedly.
At each guard post there should always be at least two assistants carefully selected by the superintendent, as an extension of himself, since he felt that the duties of the assistants, when carried out in an appropriate manner, could be exasperating, especially when the patients were excitable. Therefore, they should be guaranteed a certain degree of comfort (pp. 128–9).
Occupational therapy
Pinel (1809) discovered by chance that when patients who were usually idle were engaged in some sort of task, silence and concentration prevailed at Bicêtre’s asylum. American supporters of moral treatment therefore turned the routine of daily work into a central element of therapy. For this reason, it was necessary to increase the cost of staffing the insane asylums in order to provide farms, workshops and other facilities that would allow this kind of work. This extra investment yielded, in the medium term, excellent therapeutic results: ‘grant a man permanent employment, treat him with kindness and respect in any case and, as crazy as he may be, little can be feared him, with the exception of indolence or some mischief’ (Galt, 1846/1973: 50).
In line with the above, Kirkbride actively stressed to his patients – and the psychiatric professionals – the importance of occupying the patients’ time by doing something; he considered idleness to be one of the worst enemies of mental health. The important thing was to be busy because it regularized habits and behaviours, which had immediate beneficial effects for the patient and, in the long term, contributed to recovery (Rothman, 2002: ch. 9). It was important, moreover, that the work was not compulsory but done willingly, and that the patient had an occupation similar to the one he or she had performed prior to admission (Osborn, 2009). The occupations, meticulously programmed, were assigned according to the classification of the patients and were complemented with regular religious and physical exercises, as well as other group activities (Peloquin, 1989).
The kind treatment, the individualized care, and the use of non-radical psycho-physiological therapies were of paramount importance. With certain exceptions, narcotic-based treatments replaced the use of emetics, purgatives and bleeding that were common in many centres at the time. Doctors had to visit all patients daily and know them personally, and if possible, the concession or withdrawal of rewards and privileges replaced traditional punishment systems based on immobilization, beatings, unpleasant tasks, etc. (Galt, 1846/1973; Pérez-Fernández and Peñaranda-Ortega, 2017). This explains why Kirkbride considered that a centre could not operate well if the number of inmates exceeded 250; indeed, some, such as the Hartford Retreat, did not house more than 40 patients (Deutsch, 1937: 115). As one of the premises of moral treatment was the avoidance of overcrowding, it was necessary to have smaller, well-equipped mental hospitals, and therefore the number of asylums in the USA increased between 1850 and 1900.
The decline
The moral treatment achieved success very quickly after it was introduced in private asylums during the 1830s. The statistics seemed indisputable: for example, between 1833 and 1842 the Worcester Lunatic Asylum showed a recovery rate among newly admitted patients of 70–75%, and a clear improvement in the general condition of 3–8% of the remaining patients (Bockoven, 1963). These encouraging figures, which were one of the main reasons for the acceptance of the Kirkbride Plan as an official model by the AMSAII, were repeated in all the insane asylums based on the model. There was a combination of three elements in the use of moral treatment: (1) the homogeneous nature – psychosocial, cultural and economic – of the patients admitted to these centres, and their small number; (2) the therapeutic atmosphere of these institutions, fuelled by the enthusiasm of the superintendents in a kind of self-fulfilling prophecy; and (3) the close and optimistic interpersonal relationships that were established within these small and isolated therapeutic communities (Grob, 1973: 168–9).
However, at the end of the nineteenth century, moral treatment began to decline, due to a wide range of socio-economic and scientific factors. Theories about the healing of mental patients were already being widely discussed by a medical community imbued with a new pessimism. Also, long-term mental hospitals, many of them originally private centres that had passed into public hands, began to receive less money than was necessary to maintain an optimal level of functioning. Although politicians applauded the idea of building insane asylums to alleviate the problem of the growing mental population, there was a general failure of the public model when it came to paying for the expenses generated by the newly created institutions, and these were soon in a desperate economic situation. Certainly, the centres had originally been designed to maintain a certain degree of self-sufficiency, but they still required funding to pay for common expenses such as employee wages, coal that fed boilers, medicines and electricity (Osborn, 2009).
The regeneration movement had required the extension of good psychiatric treatment to all kinds of patients, regardless of their social background, their financial situation, or whether good public treatment was available locally. At first, the movement succeeded. Public administrations began to send thousands of mental patients to asylums, ignoring the advice of professionals (Peloquin, 1989). However, at this time there were serious economic problems resulting from the Civil War (1861–5), which prevented both the increase in budget allocations for public centres, and the construction of new ones at the necessary rate. As a result, mental hospitals became overpopulated and the rate of chronicity increased, with a consequent decrease in the numbers discharged; staff were overwhelmed, and slowly the situation degenerated towards the suppression of moral treatment and the resumption of previous custodial methods: punishments, isolation, restriction of movement, shock therapies and so on.
The dream promoted by Dorothea Dix became a nightmare. From 1870, the progressive legislations of the states mandated the admission of dangerous mental patients to the available asylums. All persons previously admitted to prisons and charity homes ended up in mental institutions. Over a short period, superintendents had to admit large numbers of patients to facilities designed for smaller and more homogeneous groups. The superintendents failed in their protests against this massive influx, as well as in their demand to be able to segregate the most violent patients and those who were incurable. In all US states, public regulations were strict, limiting the autonomy of institutions, and restricting the possibility of denying admissions (Gamwell and Tomes, 1995: 121).
Some calculations help us to understand the magnitude of this problem: the population of the USA in 1860 was 31.4 million inhabitants, of which 8500 were mentally ill; in 1890 the population of the country reached 63 million, and mental patients around 75,000 (Baxter and Hathcox, 1994: ch. 5), that is, almost nine times more. A simple division brings us closer to the number of patients in each asylum in the country: on average, about 530. In the case of the Kirkbride Plan buildings, this was more than double the number prescribed in principle by Thomas Kirkbride for an adequate application of moral treatment. The truth is that some centres had three times the number of inmates than provided for in the original design (Osborn, 2009).
In the second half of the nineteenth century, the other great conflict was really a medical one. Assuming that superintendents had to be graduates in medicine implied a focus on medicine in the cure of the patient; as a result, discussions on the potential of the moral treatment model to heal patients were slowly abandoned in favour of more invasive therapeutic techniques. In fact, the last third of the century saw a resurgence of hereditary and somatic theories about mental illness that simply turned moral treatment, especially after 1870, into a chimera that was gradually confined to the domain of private asylums (Dain, 1964: 169). Their supporters were accused of artificially swelling his statistics in order to sell as efficient therapy what was no more than a philosophical position: the unproved belief in what was described, maliciously, as some kind of ‘“mysterious” therapeutic influence to be found behind your walls and locked doors’ (Mitchell, 1894: 427). Other critics simply argued that madness, by the end of the nineteenth century, had become more complex and resistant because of the progressive complication of socio-economic conditions, and therefore needed another kind of more aggressive or simply more empirical treatments (Bockoven, 1963: 20–31).
Even within the AMSAII, moral treatment had not been completely accepted or imposed in a definitive way instead of other current trends such as phrenology, archaic methodologies such as the use of bleeding and purgatives, and even explanatory theories of altered states of the consciousness as ‘spiritual manifestations’. In fact, various details of moral treatment were discussed at the annual meetings, resulting in some friction between the superintendents (McGovern, 1976: ch. 6). Given that the American version of moral treatment adopted a pragmatic, discretional approach, Kirkbride himself recommended a certain degree of therapeutic invasiveness for extreme cases; this contravened his ethical principles to some extent, and led to the debates within the AMSAII (McGovern, 1976: ch. 6; Osborn, 2009).
On the other hand, and despite the existence of a theoretical link with the movement of Dorothea Dix, this relationship was more formal than real. It must be taken into account that the AMSAII was a very elitist association, admitting only the superintendents of the asylums and excluding most of the psychiatric profession (Berthoff, 1971: 258; McGovern, 1976: ch. 7). Thus, while there was some nominal recognition of the figure of Dix (some members such as Buttolph and Charles Henry Nichols were intimate friends of Dix), the AMSAII never granted her any honour. In addition, there was a radical confrontation between the Association and the American Medical Association, and there were also internal and external ideological problems resulting from the context of the Civil War. Inevitably, Kirkbride’s moral treatment and ideas, at the first real setback of bad recovery rates, entered the spiral of controversy (McGovern, 1976: 180–1).
This change of paradigm had a decisive effect on the insane asylums built according to the model of the Kirkbride Plan. As already mentioned, by 1910 up to 73 buildings had been erected in the USA that scrupulously followed Kirkbride’s specifications, and other buildings were based, more or less, on them. Over the years, some of them were reused as general hospitals, university centres, commercial buildings and even hotel complexes, but the vast majority were dysfunctional buildings erected according to medical and hospital management criteria that were now clearly ‘outdated’. They were gradually demolished, or abandoned to their fate. In recent years, however, a historicist and socially aware movement has emerged to try to rescue the remaining Kirkbride buildings from abandonment, ruin or misuse. These structures represent an age of mental health provision that, although not always seen in a positive light, was unique in its theoretical details, as well as in its architectural style – in fact, the Kirkbride buildings were unique constructions in the context of American history (Hardman, 1999: 112–15).
However, this type of initiative has had serious detractors, not only in the USA but also in many of the countries where there were moves to preserve these ‘historical’ structures – although the the detractors lacked economic and/or revisionist criteria to justify their opposition. Nowadays, the concept of ‘asylum’ is a subject of great controversy and is associated with the negative connotations that the earlier therapy of mental illness acquired over time, and that the medical profession has not been able to throw off. In fact, historiography faces the permanent dilemma between positive therapy and mere custody; in general, this is simplified as the clash between the mental institution which was ‘moral’ and driven by humanitarian criteria, and the penitentiary structure which was radically destructive, with the sole purpose of monitoring madmen (Osborn, 2009).
Mental health and popular culture
In the early twentieth century, the medical profession began to speak of ‘mental hygiene’, assuming that it was easier to prevent the incidence of mental disorders among the general population than to treat and try to cure the insane within an institutional setting (Grob, 1994: ch. 6). The return to the imprisonment model generated a serious debate in a North American society that was very sensitive to the problem. Discussions were sparked by the widespread publicity for cases like that of the reporter and ‘false patient’ Nellie Bly, whose real name was Elizabeth Jane Cochran (Pérez-Fernández and Peñaranda-Ortega, 2017). She was admitted to a New York asylum without a diagnosis and without suffering any physical or mental illness, simply because she was a woman who presented herself as a ‘deviant’ person (Bly, 1887). Another such case was that of the patient Clifford W. Beers who, after he recovered, was one of the founders of the movement for mental hygiene.
Beers, who published a famous book with a descriptive title, A Mind That Found Itself (1908), managed to enlist the support of William James (1842–1910) and Adolf Meyer (1866–1950) to found the National Committee for Mental Hygiene (NCMH). Its purpose was to combat the mistreatment to which patients were subjected in insane asylums, while protecting their rights and improving the quality of care they received. Unfortunately, the impact of these proselytizing actions was reduced among public institutions because the NCMH lacked a viable plan that could be accepted by the authorities (Osborn, 2009). The situation degenerated at a dizzying speed: the number of institutionalized patients was 75,000 in 1890, and increased to about 187,800 in 1910, and 425,000 in 1939. In the days before World War II there was, on average, a ratio of 1 nurse for every 500 inmates and a specialized doctor for every 1320; in these conditions, the daily needs were hardly met, so very few care plans or effective treatments could be applied (Grob, 1994: ch. 7).
Between 1890 and 1930 – perhaps because of the unstoppable institutional degeneration towards the reclusion model, perhaps after the excuse that this process provided – the American psychiatric profession began to promote all sorts of radical therapies of dubious validity; publicity about them generated strong rejection or simple fear. Previously, patients assigned to the old insane asylums in which the moral treatment was prescribed had expressed all kinds of resistance to admission, especially because they did not know when they would leave the institution. So it was not surprising that those about to be admitted to the modern psychiatric centres of the first decades of the twentieth century were aware of their situation and felt pure panic. In fact, there were serious controversies among psychiatrists themselves about the theory and efficacy of insulin treatment, electroconvulsive therapy and lobotomy, to name some notorious examples. Understandably, this public controversy fostered a progressive discrediting of mental institutions (Osborn, 2009).
Woodward, Kirkbride and his colleagues at the AMSAII had been aware of the importance of maintaining a good public relations policy to give prestige to the activities of mental health centres; however, this was the battle that their successors lost. There was a general silence among the psychiatric profession around the daily routine of the asylums. Instead, public opinion was based on texts such as the successful 1946 autobiographical novel The Snake Pit by Mary Jane Ward. The author uses terms that would become common among the public to describe the conditions of some hospitals, for example ‘back-wards’, in the figurative sense of regression to the worst possible state. She meant that many of the more problematic and violent patients were simply left to their fate in the pavilions farthest from the rest of the hospital; ‘warehousing’ referred to the mere ‘storage’ of patients who received little or no treatment (Osborn, 2009). Two years after Ward’s novel was published, it was made into a film by the director Anatole Litvak, featuring the actress Olivia de Havilland. It was a very successful movie which received many awards and acknowledgements (Vera Poseck, 2007).
Influential books such as A Mind That Found Itself and The Snake Pit created an interest in this kind of literature. For this reason, the American film industry started to produce films on all sorts of topics – the police, terror, social denunciation – in which mental institutions became central, or at least one of the principal scenarios. The films projected a terrible image of the centres themselves, and of the professionals who worked in them. For example, two films contemporary with Litvak’s The Snake Pit were High Wall (1947), directed by Curtis Bernhardt, and Behind Locked Doors (1948), by Budd Boetticher. These films created a popular image of mental health which did not help to improve the asylums. Also, of course, it generated confusion around the problem of mental health, as well as in relation to its diagnosis, therapy and prognosis. This contributed substantially to the stigmatization of the patient who needed to ‘be saved’ from the institutional disaster. At this time, it was a common topic in films, for example, to identify mental illness with telling lies, and to imagine it was easy to deceive psychiatrists and that, therefore, mental pathology was not a ‘real’ disease, but an excuse or deception used by many criminals to avoid punishment (Byrne, 2009: 5).
From the middle of the 1950s, American psychiatry made great efforts to offset this failure of its public image by applying and publicizing new psychological and pharmacological therapies. In addition to this movement for the humanization of mental health, in 1960 the Supreme Court of the United States approved for the first time a measure aimed at the social integration of the mental patient: a patient could be hospitalized only if there were no alternative treatments (Levinthal, 2005: ch. 14). In fact, it is often forgotten that progress in the socialization of the mental patient was possible because of advances in psychopharmacological therapies. But the damage was already done, and the image of mental health that had been transmitted in popular culture ignored genuine cases and treatment. Instead, it always depicted disorganized and unhealthy hospitals where chaos reigned and the staff were out of control. The films constantly repeat images and clichés that were already part of the subgenre: the brutal application of immobilization techniques or torture of the madman; the patient who resists the nurses; crowded dining rooms and corridors where each patient gives free rein to their peculiar form of madness. Moreover, the psychiatrists are inept – or even real criminals, unable to discern between madness and sanity; they are portrayed as evil doctors who make the situation worse for the patient in order to increase their power both inside and outside the institution (Vera Poseck, 2007). The next step was then to turn the mental institution into an optimal scenario for contemporary horror films: a dangerous place full of dreadful lunatics – including its director – who harboured (or had done so in the past) monsters of the worst kind.
A perfect example of this tendency is found in the two existing versions of the film House on Haunted Hill. The first was made in 1959 and directed by William Castle, starring Vincent L. Price, an iconic actor of the genre. The second, directed in 1999 by William Malone, is more gimmicky visually, but less interesting in cinematic terms than the first. In both, an eccentric millionaire organizes a party in a sinister mansion that, in reality, is an old abandoned psychiatric hospital with a terrible history. The story ends, as usual, with a bloody tragedy.
So the abandoned asylums of the Kirkbride Plan, scattered throughout the USA, gradually developed the same negative image that psychiatric care was acquiring in popular culture; they became sinister buildings. As well as locations for horror films, they were places of urban legends of all kinds, and therefore they became a magnet for ghost-hunters and myth-seekers. In other words, they were a complete perversion of the humanist ideology on which they were based, designed and constructed. Some of them were saved by universities, hospitals, political authorities, companies or other institutions, and have been protected and remodelled, but this has not freed them from their folk image. Thus, for example, the Trans-Allegheny Lunatic Asylum, located in Weston, West Virginia, became a general hospital and later it housed three museums, but it was abandoned in 2004 because it violated fire regulations. For years, it had the reputation of being one of the ‘most haunted’ buildings in the USA, so it was then acquired by a hotel company which attracts tourists by saying that it is ‘full of ghosts’, and offering guided tours of the cells, basements, dungeons and alleged torture chambers. The building has starred in several reality shows about the paranormal: Ghost Hunters, from the SyFy channel; Ghost Stories and Ghost Adventures, both from the Travel Channel; and Paranormal Lockdown, from the Destination America channel. These shows have turned it into a true icon of the genre.
Another icon is the Danvers State Insane Asylum, Massachusetts, which was also converted into a hospital. Although it was later largely demolished, much of the central building was preserved, as it is a protected project of the American architect Nathaniel J. Bradlee. This building, with a long tradition of ‘ghosts’, ‘hauntings’ and ‘possessions’, has inspired, among others, the writer Howard P. Lovecraft in the writing of his story The Shadow over Innsmouth, and later, the cartoonist Bob Kane in the design of the gothic Arkham Asylum where Batman always locks up the psychopathic Joker. It also became the stage for the development of different game levels in successful video games such as Painkiller (DreamCatcher Interactive, 2004), and was the setting for two psychological horror films: Home Before Dark or After the Storm (1958) by Mervyn Leroy, and Session 9 (2001) by Brad Anderson.
Final thoughts
The Kirkbride buildings, perhaps because of their unique architecture, have remained indelibly associated in popular culture with the insane asylum: that massive, dark, terrible mansion with long corridors and gloomy recesses in which the person enters, but from which it is impossible to leave, and in which the patient, visitor, employee on duty is exposed to all sorts of iniquities. It is easy to find countless horror films, television series and amusement parks whose mysterious and enchanted mansions have a unique resemblance to the peculiar architecture of the Kirkbride Plan. Indeed, this could save some of these historic buildings from demolition. One example is Fergus Falls State Hospital, which was designed by the architect Warren Dunnell (1851–1931) and built in the town of Fergus Falls, Minnesota, in 1895.
After a random history of reconversions, this asylum was reused as Fergus Falls Regional Treatment Center until 2005, when it was abandoned. In 2007 the state sold the land to the Fergus Falls City Council (Cartwright, 2012). The municipal authorities were going to demolish it and reuse the land, even though it had been on the National Register of Historic Places since 1986. However, the building was generally in good condition, so since 2013 several filming teams have made substantial payments to the municipal coffers in order to use it for various productions related to horror movies or ‘paranormal research’, for example The Control Group (2014, directed by Peter Hurd), and Geist (2015, directed by Eric Daniel Dunn). This has not only increased public interest in the building, but has also led to its new status of historical uniqueness, as well as some money for Fergus Falls. This has motivated municipal and academic authorities to consider a construction rescue and also its official preservation (Tellers, 2015a, 2015b).
So it may be that popular culture comes to the rescue of a historical heritage that the peculiar scientific development of psychiatry was about to destroy. But Kirkbride and the American followers of moral treatment would not have been able to understand this situation, which is now so far from their real interests.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.