
Abstract
This article studies the University of Tartu psychiatric hospital and its patient population in the Russian Baltic Province of Livonia in 1881–95, using the hospital’s admission registry book as the primary source. Although it was a university clinic following the German academic tradition, both upper- and lower-class patients were admitted (25 and 75 per cent, respectively, of 2,184 hospitalizations), with a median stay of 70 days. Admission and length of stay often depended on a family’s or community’s financial capabilities. Considerably more men and unmarried patients were admitted, and 139 hospitalized women were diagnosed with female-specific illnesses. This study argues that gender and social class should be jointly analysed, as admission and discharge outcomes are influenced by both factors simultaneously.
Introduction
The strange behaviours and disturbed inner worlds of people deemed ‘mad’ by their contemporaries as well as by themselves have always existed (e.g. Ingram, 1997; Peterson, 1982; Schreber, 2000). The problem plaguing those who suffered from mental illnesses in previous centuries, just as now, was the absence of unchallenged and universal biomarkers that clearly indicate disturbances in mental faculties. There are therefore only two ways to recognize a mental disorder: first, by basing one’s knowledge on a first-person narrative of the diseased and, second, observing their behaviour, or both. Either approach is highly susceptible to the observer’s subjective interpretations and to pretence on the part of the ‘sufferer’. This means the justification for institutionalization or any other type of medical intervention has potential problems at its very core. For example, it can lead to accusations of wrongful confinement in mental institutions. 1
Many questions in the history of psychiatry arise from the fact that the patient population in mental institutions rose rapidly in the late nineteenth and early twentieth centuries. The first scholars who tried to explain the explosion in patient numbers claimed these institutions were instruments whereby the unconventional, the poor and women could be socially controlled (Foucault, 1972/2006: ch. 2; Showalter, 1987: ch. 3). These mid- and late-twentieth-century researchers have had their arguments disputed by later studies which have shown that the problem is not as straightforward as it first seemed (Busfield, 1994; Porter, 1987: ch. 1, ch. 3; Wright, 2004). For example, instead of looking at the question of gender from only a woman’s perspective, these studies have introduced other factors, such as class, into the equation, thus providing an analysis of the complex matrixes of gender–class relationships through the lens of mental illness (Hide, 2014; Michael, 2004; L Walsh, 2003). In addition, historians have shown how institutionalization, at least in the Anglo-American world, has not been controlled by medical men, but rather by a patient’s family or community – lay people, not those educated in psychiatry (Wright, 1997: 143). This means that potentially wrongful institutionalization was not so much the abuse of power by psychiatrists, who now claimed to have sole expertise in this regard, but rather decisions made by family members who, due to changes in family relationships and everyday life, could or would no longer care for a mentally ill family member (Shorter, 1997: 50). Although the majority of studies in English on the institutionalization of the insane are obviously in the context of Anglo-American psychiatry, this trend has begun to change, and international audiences can read discussions on gender or class in psychiatry in other parts of Europe (e.g. Pietikäinen and Kragh, 2020).
One way to study the institutionalization of the insane in the context of gender and social class is to analyse large datasets of hospital admission registers. These usually contain patient diagnostic and demographic data as well as admission and discharge information. This type of large dataset allows analysis of the patient population of a given hospital, enabling us to see how different variables, such as diagnosis, social class or gender, influence admission and discharge. Many studies in have used asylum registers to analyse patient populations, one of the first being by William Parry-Jones (1972). 2
In order to contribute to the debate of how both social class and gender influenced admission to, diagnosis and discharge from mental institutions, this article provides an example from the Russian Baltic Provinces, analysing data extracted from the University of Tartu 3 psychiatric hospital admission registry book in the period 1881–95. 4 Although the hospital was founded in 1877, the first registry book starts from January 1881 and ends in December 1895. 5 Analysis of this particular patient population provides a somewhat different insight, since previous studies have mostly looked at rural asylums and private madhouses (e.g. MacKenzie, 1992). University psychiatric hospitals have generally received less attention, especially in English-language studies, which is not surprising given that the UK, for example, only acquired its first university psychiatric hospital in 1923 (Shorter, 1997: 90). The present study gives an example from the Russian Empire, a region that has so far received scant attention from historians of psychiatry. The article argues that, although the admission, diagnosis and discharge of patients was significantly affected by gender, this cannot be viewed separately from social class which, as this study shows, had just as great an influence as gender. For this reason, all analyses for this study use a fourfold matrix that considers both social class (upper, lower) and gender (male, female), showing that the patterns of institutionalizing the mentally ill in Tartu were similar to those in Western Europe, since more men and unmarried patients were admitted. Admission was connected to the purchasing power of the patient’s family or community, so periods of institutionalization were relatively short (median: 70 days). As a result, mortality rates were high only for wealthy men, most of whom probably died from neurosyphilis. Though possible social control cannot be deduced from data based on a hospital registry book, the voluntary admission of some patients and the relatively small proportion of elderly patients would indicate that admission could have offered peace of mind to both patients themselves and their families that was not achievable at home. Yet, that a few patients escaped, and that discharge was very often at the hands of family members, would indicate that some admissions may not have taken patients’ opinions into account, but this could be argued with certainty only by analysing their case records and other accounts, for example diaries, if possible.
Historical outline
Before analysing the patient population, a brief outline of the historical context and situation of mental institutions in the Russian Baltic provinces is needed. Following the Great Northern War in the early eighteenth century, the Baltic provinces of Estonia and Livonia, and later Courland, became part of the Russian Empire. What distinguished these provinces from others was that the local nobility were Baltic-Germans and the majority of peasants were Estonians and Latvians – in other words, social class ran along ethnic lines. In addition, the Baltic provinces had their own separate legal system: Landesstaat. However, though the topic has been relatively little studied, it seems that social welfare policy was applied from St Petersburg uniformly across the empire (Seppel, 2019: 190).
At the beginning of the nineteenth century, after serfdom was abolished in the Baltic provinces, the legal responsibility for caring for the sick in rural municipalities started to shift towards the rural communities themselves. In the 1860s, a new law stipulated that rural communities had to ensure the availablity of various welfare services, including taking care of individuals with mental problems (Sirotkina, 2002: 11). The same law was issued in the Estonian language in 1866. 6 Hence, by the time Tartu’s hospital was founded in the 1870s, the legal responsibility for the welfare of mentally ill peasants lay with their own families and rural communities.
Additionally, in the late eighteenth century, both Livonian and Estonian Boards for Social Care (Livländische/Estländische Collegium für Allgemeine Fürsorge) were founded. One of their many tasks was to establish and supervise welfare institutions, including insane asylums. An asylum was opened in Riga in 1786 (Kuzņecovs, 2013: 83) and a general hospital with special wards for the mentally ill in Tallinn (‘Reval’ in German) in 1796 (Gustavson, 1971: 127). A new mental hospital called Alexandershöhe was opened in 1824 in Riga, and all mentally ill patients were transferred there from the Livonian Board’s facility (Kuzņecovs, 2011: 272). Thus, the beginning of institutional care for the mentally ill was initiated by the government in St Petersburg.
The exact number of mental hospitals in the Baltic provinces before 1877, when the hospital in Tartu was founded, remains uncertain and requires further research. Besides the Alexandershöhe in Riga and the Tallinn general hospital, there was a private asylum, Rothenberg, in Riga, which was later sold to the City of Riga; there were also the Deaconess’ Institution in Tallinn and a small temporary private institution (Familienpansionat) in Valmiera (Wolmar) (Laehr, 1875: 141, 182–3; Laehr and Lewald, 1899: 231, 234). In addition, mentally disturbed patients were also held in military and general hospitals (Laehr and Lewald, 1899: 187; see also Kuzņecovs and Loseviča, 2019: 39). Contemporaries estimated that in 1861 in all three Baltic provinces there were 697 insane people (Irren) and 1,375 people with mental retardation (Idioten): 1 per 554 inhabitants in Estonia, 1 per 857 in Livonia, and 1 per 998 in Courland (Schulz, 1863: 389). Later, together with the official 1881 census, mentally ill people were also counted. Here the numbers were worse – 1 per 241 in Livonia and 1 per 230 in Estonia. The ratio of mentally retarded to insane was similar: in Estonia there were 46.98 “idiots” to 53.02 insane, in Livonia 45.05 to 54.95 (Dehio, 1890: 77). At the same time, before the establishment of Tartu Hospital, there were an estimated 260 beds (Laehr, 1875: 172), indicating far more potential patients than there were beds.
Thanks to private initiatives and donations, an insane asylum (Irrenasyl) was opened in Tartu, Estonian-speaking Northern Livonia, on 4 March 1877 (Von Wahl, 1878). For its first three years, as a private institution, it only accommodated female patients – 12 the first year, then 16 and 21 (Von Wahl, 1878, 1879, 1880). The institution was meant as a study centre for university medical students from the outset, but bureaucracy took time and the hospital was bought by the university in 1880, when a Chair of Psychiatry was also established. In 1881, a new 50-bed hospital building was ready to admit patients (Saarma, 1981: 349–351). At first, it was called a psychiatric hospital (Psychiatrische Klinik), then from 1882 onwards the Hospital for Mental and Nervous Diseases (Klinik für Nerven- und Geisteskranke). 7
University of Tartu Hospital for Mental and Nervous Diseases
Hospital patient populations had traditionally been poor people for whom hospital was the last ray of hope. This started to change in the late nineteenth century with improvements in antisepsis, asepsis and diagnostic techniques. University hospitals and asylums cared for the lower classes, but Tartu Hospital admitted patients from all social classes. Since there were very few establishments for upper-class patients, it had to serve as an institution for those in the higher social strata. In its second year, in 1878, the hospital accommodated two ‘higher status’ (höherem Stande) women (Von Wahl, 1879). The hospital admission registry book had a separate section noting whether admitted patients paid for a Class I, II or III ward. Those in a Class I ward had a private room, a two-course breakfast and a three-course lunch; those paying for a Class II ward had to share a room with one other patient and received a two-course lunch; Class III patients shared a big ward and ate ordinary hospital food (Mikhelson and Chizh, 1891: 14).
During the period under observation (1881–95), 25 per cent of the 2,184 hospitalizations 8 paid for either Class I or II beds, meaning they were at least relatively wealthy. At that time, around 90 per cent of the whole population in the Baltic provinces were peasants whose purchasing power was considerably lower than that of the remaining 10 per cent (Vahtre, 2010: 60). In towns, however, the class division was different. According to the Tartu 1897 census, only 69.8 per cent of the population belonged to the peasant class (Berendsen and Maiste, 1999: 113). The upper- to lower-class ratio in the hospital was therefore similar to that in the town itself. However, because the hospital had to provide for all the provinces, it can be argued that the upper-class patients were somewhat over-represented among the patient population.
To appeal to higher-paying patients, the name of the hospital had to be attractive. A diagnosis of insanity almost always caused stigmatization, and was therefore to be avoided. As a result, in Europe, middle- and upper-class patients were often diagnosed with ‘nervous illnesses’ instead of insanity, even if their symptoms were identical to those of poorer patients. Cures for ‘nerves’ were offered in private institutions, often run by physicians (Shorter, 1997: 113, 118). Perhaps in order to attract these higher-paying patients, the hospital name included a reference to ‘nerves’, so that upper-class families could avoid the fear of stigmatization when one of their relatives was institutionalized. In fact, the hospital did admit patients whose ailments today would be classified as neurological: 144 hospitalizations were diagnosed with epilepsy, 60 with paralysis (e.g. hemiparesis) and 76 had some sort of brain disease or brain trauma. Nevertheless, these patients made up only a minority of all diagnoses. In addition, during the nineteenth century, epileptic patients were still treated and discussed by psychiatrists, as it was only from the 1880s that neurology slowly started to emerge as an independent subject (Hirschmüller, 1999: 405). In Tartu, the Hospital for Nervous Diseases was not separated from the psychiatric hospital until 1920 (Kaasik, 2000: 7).
The hospital belonged to the University of Tartu, whose scientists were deeply connected with German universities and thus their academic tradition. The hospital had to serve as a clinical base for teaching medical students and research. Its aim of using patients as teaching material was also highlighted in the hospital’s management report (Mikhelson and Chizh, 1891: 14). Although upper-class patients were not used for teaching or research (Kraepelin, 1983/1987: 40; Laehr and Lewald, 1899: 68), some psychiatrists in the hospital – one of them being Emil Kraepelin who was in Tartu during 1886–91 – found it easier to talk to upper-class patients because they shared a common language (German), whereas in order to talk to Class III ward patients, psychiatrists needed an interpreter (Kraepelin, 1983/1987: 40). 9 In addition, doctors communicated more easily with upper-class patients because they were educated and therefore often more articulate (L Walsh, 2003: 250). Thus, upper-class patients played an important part in helping psychiatrists further develop their understanding of mental disorders.
The subjects of research at the hospital were sometimes not patients but assistant medical students who worked at the hospital. Its assistant doctor Eduard Michelson (1861–1944), for example, conducted his innovative PhD research on sleep periodicity under Kraepelin’s supervision, using himself and three colleagues as subjects: Heinrich Dehio (1861–1928), Leon Daraszkiewicz (1866–after 1926) and Albert Berh (1860–1919) (Weber and Burgmair, 2009: 381–2). All three also did their dissertations on experimental psychology and were supervised by Kraepelin.
Lower-class patients were used for education and research. This was pointed out by Kraepelin (1983/1987: 40), who mentioned that ‘the majority of the patients suitable for teaching purposes only understood Estonian’. In other words, only Class III patients could be used for demonstrations at lectures and for bedside teaching during ward rounds. Although language barriers could have been an issue, there was no lack of suitable patients, with 75 per cent of hospitalizations in Class III wards. In addition, until the end of the nineteenth century, hospitals played an important part in poor relief, so the main target groups were poor patients (Tröhler and Prüll, 1997: 169). This was also the case in Tartu: when donations were collected for establishing the hospital, both Estonian and Livonian nobility (Ritterschaft) contributed on condition that the hospital would provide beds for patients from these provinces. It had to have 15 Class III beds for patients from Livonia and 4 Class III beds for patients from Estonia, although the patients were still expected to pay an additional Class III fee of 15 roubles per month for their stay (NAE: EAA.402.5.930, 101; see also Laehr and Lewald, 1899: 68). In comparison, a carpenter, for example, earned on average 2 rubles per day (Küng, 2015: 15). It therefore seems that it was possible for at least some lower-class people to afford such care for their relatives.
As medical practice in Tartu followed German academic traditions, research was highly valued (Tröhler and Prüll, 1997: 172). Keeping this in mind, the head of the hospital could admit interesting cases free of charge (Mikhelson and Chizh, 1891: 209). During the period 1881–95, 26 patients were admitted free of charge, all of them in Class III wards. It may be significant to note that 22 of these patients were admitted during Kraepelin’s directorship, which could indicate his dedication to research, although perhaps the next director, Vladimir Chizh (1855–1922), found sufficient interesting cases among the increasing number of patients.
What kind of diseases did psychiatrists diagnose in their patients in Tartu? First, it should be noted that a significant number of patients received multiple diagnoses, so there were many more diseases listed than there were hospitalizations. It is also noteworthy that many disease diagnoses had a question mark attached, indicating an uncertain diagnosis. Such hesitation was noted in 268 of the 2,184 hospitalizations, meaning that in over 10 per cent of cases doctors were not sure what they were dealing with. This uncertainty was one of the greatest problems in late nineteenth-century psychiatry, and was clearly seen as problematic by contemporaries as well. When writing the hospital report in 1891, hospital doctors Michelson and Chizh pointed out the diagnostic differences between the previous hospital directors – Hermann Emminghaus (1845–1904), the first director, and his successor, Kraepelin (Mikhelson and Chizh, 1891: 221–2). Already within these 10 years of activity, the differences in diagnoses were clearly visible. Considering Kraepelin’s work, for example, Kenneth S. Kendler has analysed in a series of articles how his disease categories of different psychotic illnesses developed at the turn of the century (Kendler, 2018, 2020a, 2020b, 2020c; Kendler and Engstrom, 2020). However, while Kraepelin was in Tartu, his taxonomy was not yet fully developed; for example, no patient between 1881 and 1895 received a diagnosis of dementia praecox. Nevertheless, this period early in his career certainly influenced Kraepelin’s later understandings of psychiatric illnesses.
This still-developing disease taxonomy was the reason for the vast differences in the names of mental ailments. The diagnoses patients received in Tartu clearly belonged to the end of the nineteenth century. We see diagnoses that have a remarkable history over two millennia (melancholy, mania, hysteria), but there are also relatively new diagnoses that were just being introduced during this time (neurasthenia, hebephrenia, catatonia, morphinismus). Yet other diagnoses were more general in nature (Blödsinn, Primare Verrücktheit). Degeneration as a diagnosis was also noted and indicates a growing fear of a deterioration in the quality of human beings. However, an in-depth analysis of the disease taxonomies used by Tartu’s doctors would go beyond the scope of this article, requiring a detailed reading of patient case histories, so this very interesting topic must await further research.
Finally, it should be noted that patients also suffered from somatic non-neurological diseases, such as tuberculosis, ulcers or arthritis. 10 This comorbidity was noted in a minority of patients, and very few were diagnosed solely with somatic ailments.
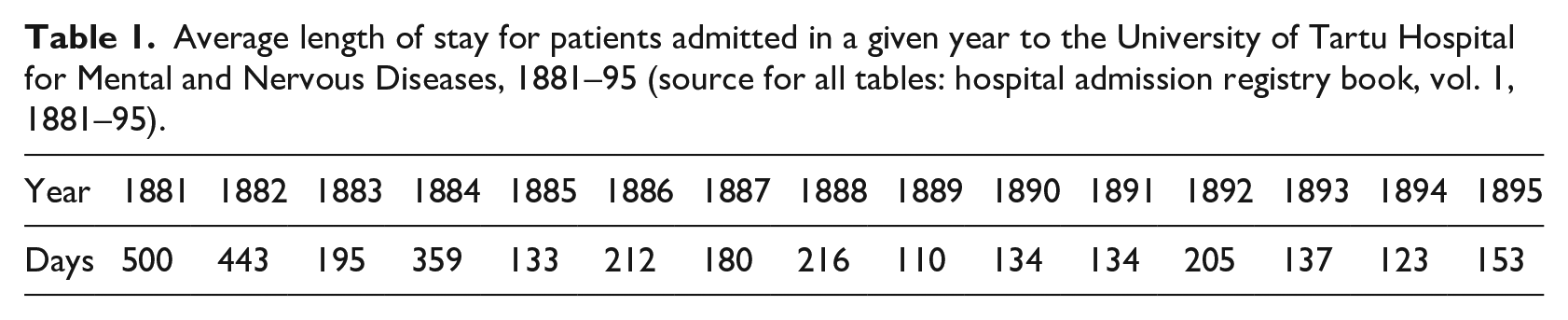
Length of hospital stay
When talking about using nineteenth-century asylums as ‘Victorian bins . . . for society’s unhinged and unwanted’ (Scull, 2006: 107), it has often been argued that patients spent unjustifiably long periods in mental institutions. Based on the data from Tartu, I would suggest this was not the case there. The median length of stay in Tartu Hospital was 70 days, while the average length of stay was 189. Based on this, it is impossible to argue that the hospital was filled with chronic incurable patients who were doomed to spend the remainder of their lives incarcerated, especially if compared with, for example, Pamela Michael’s study on an asylum in Wales, where the average length of stay was nearly 500 days (Michael, 2004: 100). However, as David Wright points out, when long-term patients started to occupy more and more beds, then new admissions would have had to stay for a shorter period of time (Wright, 1997: 143–4). In Tartu, the average length of stay did decrease but not infinitely (Table 1). Thus, it cannot be argued that long-term patients in Tartu made up ‘a repository of dead souls’ (Scull, 2006: 108). Yet, as Scull suggests, even short-term hospitalizations could be used as a means of social control (p. 108). Further study and thorough analysis of case records would be required in order to prove that some patients were institutionalized because they were ill or just unconventional. In addition, the length of hospitalization may not indicate whether the patient’s condition was considered chronic or not, since chronic patients might just have lacked the necessary funds to remain in hospital for a long period of time and might have received further outpatient treatment at home.
Average length of stay for patients admitted in a given year to the University of Tartu Hospital for Mental and Nervous Diseases, 1881–95 (source for all tables: hospital admission registry book, vol. 1, 1881–95).
Long-term patients need a more detailed analysis. Of the 2,184 hospitalizations, 188 remained longer than a year (Table 2). When comparing long-term patients with the overall average (Table 3), we can see similar but even more pronounced patterns: many wealthy men died in the hospital, and improvement rates were better for women than for men. However, figures that differ from the averages are those for the remarkably higher death rate and the lower improvement rate for long-term patients. These results might be explained by the severity of their symptoms, making these patients unable to cope with everyday life, thus leading to long-term institutionalization. In addition, unmarried patients were much more likely to experience long-term institutionalization than the average; this difference is especially remarkable in both upper- and lower-class women, but is clear in men as well. The probable reasons were that unmarried people lacked the social support a spouse provided, and there was reluctance to hospitalize a spouse. Thus, in analysing the socio-economic status of long-term patients, similar conclusions can be drawn as from the hospital’s overall average numbers: the same patterns are evident but are even more pronounced, possibly because of these patients’ more severe symptoms.
Long-term patients who were hospitalized for longer than a year in the University of Tartu Hospital for Mental and Nervous Diseases, 1881–95 (source: see Table 1).

For two women, no class was given.
Patients and their demographic data from the University of Tartu Hospital for Mental and Nervous Diseases, 1881–95 (source: see Table 1).
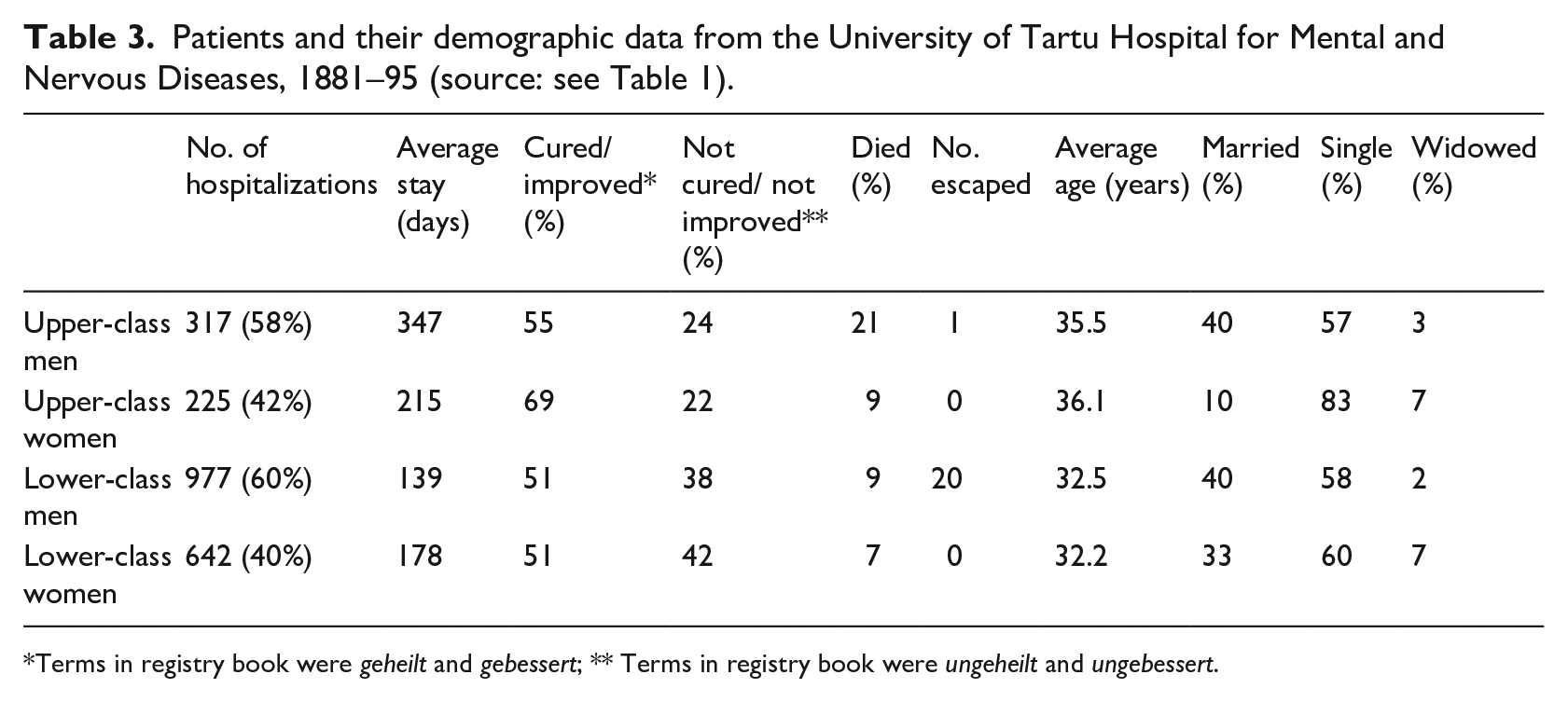
Terms in registry book were geheilt and gebessert; ** Terms in registry book were ungeheilt and ungebessert.
Possible social control
During the second half of the nineteenth century, the number of mental institutions and their patient populations rose rapidly, both in Europe (Shorter, 1997: 46–7) and the Russian Baltic provinces. When the hospital was established in Tartu in 1877, there were only a few other mental institutions, in Riga and Tallinn, but by 1904 there were 16 different institutions specifically caring for the mentally ill (Kuzņecovs and Loseviča, 2019: 36–45). One reason suggested for the increase in asylum numbers was the belief among medical and lay people alike that the institutions themselves were curative, since they provided a controlled environment different from home (Shorter, 1997: 18). In Tartu, there were 70 hospitalizations in 1881 and 234 in 1894. This rate of increase in admissions, especially when considering there were just 12 patients during its first year, is noteworthy. At least initially, the increase in admission numbers can be explained by the establishment and then growth of a new institution. But the fact that the number of admissions grew shows that there was indeed a pressure of numbers, just as elsewhere in Europe. However, the increase in patient population in itself does not clearly indicate that a new psychiatric establishment was used as a means of social control, as some scholars have argued. 11
The section in the admission registry book containing the address of the patient’s representative (Adresse des Vertreters des Kranken) may indicate who took the initiative to admit someone to hospital. From 1881–95, 129 patients admitted were recorded as representing themselves (Vertritt sich selbst). 12 Although the number is quite small compared with the total number of hospitalizations (2,184), it still indicates voluntary admission by some people. Of these, 78 (61 per cent) patients were paying for Class I and II wards (40 men, 36 women) and 50 (39 per cent) for Class III wards (34 men, 15 women). 13 Perhaps the reason poor men were more likely to seek medical help than poor women was that, as breadwinners, they felt under pressure to restore their ability to work. What is also worth pointing out is the voluntary patients’ relatively short length of stay: 45 (or nearly one-third) stayed less than 30 days and only 12 stayed for longer than 200 days. 14 In addition, 57 patients were diagnosed with neuroses that possibly had relatively mild symptoms, while 52 had either neurological problems or addiction. Thus, it seems that people who came to the hospital voluntarily were hospitalized for only a short while and needed either a different environment from home or help with their severe conditions. Nineteenth-century lay attitudes to insanity in Baltic provinces would require its own extensive research, but these voluntary admissions could suggest that, at least for some, insanity (or at least ‘nervous disorders’) had been medicalized. As a result, belief in a cure provided by the hospital itself, or specialized therapy provided by psychiatrists, may have reached the public, despite the virtual complete lack of local asylums.
Counterbalancing the figures for voluntary admission is the fact that 21 hospitalized male patients did try to escape, some escaping several times. They were diagnosed with severe diseases such as alcoholism, mania and paranoia, and, not surprisingly, none of them had been admitted voluntarily. All but one patient had a representative noted: one patient was represented by the police, four were represented by local tax boards (Steuerverwaltung), and the rest by a family member or a community. This would suggest that the immediate family or community had decided to admit them. Escaping would indicate that the patient could be difficult to manage at home or in the community and had therefore been put in the care of medical professionals. To what extent these men were actually a threat to themselves or others, and to what extent they were incarcerated out of malicious intent, might be answered by further reading of their case records.
The number of patients with spouses or family members as representatives cannot be provided with certainty, as often only the representative’s name and address were given, not their relationship to the patient. However, in 485 cases a family member (parent, brother, sister) was mentioned as representing the patient, but even when the title ‘Frau’ is given, it does not necessarily indicate that the representative was the patient’s wife. A community was noted as representative in 592 hospitalizations. In a small but still notable number of instances, 53 hospitalizations were represented by a local tax board (Steuerverwaltung). While in such cases it was an official who decided that a certain administrative department should pay for hospitalization, it was probably a family member who asked for this help.
Admission to the hospital was therefore decided in most cases by the patient’s family or community, and in Tartu their discharge was also in the same hands. Kraepelin (1983/1987: 37) noted that: ‘The patients had to stay until they were fetched by their relatives or until they could stay somewhere else.’ The admission registry book sometimes mentions who ‘withdrew’ the patient from the hospital, for example: ‘by husband withdrawn, cured’ (vom Mann zurückgenommen, geheilt). 15 Sometimes it was added that a patient was discharged because the family, or less often the community, lacked the funds to keep them in hospital for longer: 16 9 wealthy patients and 106 Class III patients were noted to have been discharged for this reason. In some instances, hospital staff found it important to mention that the patient was withdrawn against a doctor’s advice, 17 which was the case with 18 upper-class and 56 lower-class patients. Taking this into consideration, it seems that the psychiatrists, like their patients, were at the mercy of a family’s or community’s whims and financial situation in relation to both admissions and discharges.
In Tartu Hospital, therefore, it was often the family or community who paid for patients, and it was also they who discharged them. Thus, it seems that the length of stay was connected with the ability to pay and not doctors’ wishes. So, if social control did exist, it came from families and not doctors. However, when considering patients who represented themselves, it seems that it was not only the family or community who decided which thoughts and behaviours were considered improper, but that the patients themselves might also have considered their inner world unconventional and requiring treatment. The evidence suggests that patients who were not capable of taking care of themselves had to be discharged by a relative to ensure their safety, but those considered capable of reason could discharge themselves. For example, patient No. 1785 was noted to be ‘Discharged. Taken to train station with Andrei. Cured.’ (Entlassen. Mit Andrei auf den Bahnhof geschickt. Geheilt.), 18 or No. 1790 who ‘Travelled home himself. Taken to train station with head guard. Improved.’ (Fuhr selbst nach Hause. Mit Oberwärter zum Bahnhof geschickt. Gebessert.). 19 The question of the extent to which hospitalization was used as a means of social control cannot be answered with certainty from an analysis of a patient admission registry book. However, the facts that numbers increased and that patients were only discharged into the care of their relatives cannot be seen as unequivocally indicating a wish to incarcerate the unwanted. What can be argued is that the service provided by Tartu Hospital was considered necessary by increasing numbers of people in the Russian Baltic Provinces, attracting patients from as far away as St Petersburg.
Gender differences
As nineteenth-century psychiatry viewed men and women differently according to their perceived tasks in society, examining the effect of patient gender in admission and discharge can help us further understand this gendered approach. In Tartu, fewer women were institutionalized than men. From 1881 to 1895, 40 per cent of all hospitalizations were women and 60 per cent were men. 20 This ratio was very similar for both upper and lower classes. While considering this, it should be taken into account that men and women were in different wards, so no new patients could be admitted until an appropriate bed became available. Thus, based on Table 3, I would argue that the reason more men were admitted was that men in Class III wards spent considerably less time in hospital than Class III women, thus allowing new male patients to be admitted more often. More men were also admitted in Riga and Tallinn as well. In 1897 in Rothenberg Hospital (Riga), the male to female ratio was 191:150 (56 per cent to 44 per cent), in Alexandershöhe (Riga) 75:66 (53 per cent to 47 per cent), and Tallinn 22:14 (61 per cent to 39 per cent) (Laehr and Lewald, 1899: 230, 234–5). Similar male to female ratios seem to be the case elsewhere in Europe (O Walsh, 2003: 72). Two possibilities have been suggested for this: first, that families may have been more willing to pay for men’s health care because of their greater economic importance for the family (p. 73); second, women’s insanity may have been more manageable at home (p. 74). The latter proposition could be supported by the fact that during the period 1881–95, no women escaped from the hospital (Table 3).
An important variable that affected patient admission numbers was marital status, although it was noted in only about half of the hospitalizations. Unmarried people, men and women in both classes, were more likely to be admitted (Table 3). It has been suggested that the reason was a reluctance to commit a spouse to an asylum (Wright, 1997: 151). There is, however, a remarkable gender difference. While for male patients there was no obvious connection between social class and marital status, there definitely was for women: the proportion of married women in both upper- and lower-class wards was lower than was the case for men, and the difference was even more considerable when we compare wealthy and poor women. The fact that only 10 per cent of upper-class women admitted to the hospital were married raises questions. One possible reason (among many) is changes in family models in the late nineteenth century, where unmarried female relatives were increasingly perceived as a family burden. In the Baltic provinces, as elsewhere, family finances were handled by men. Consequently, husbands were more likely to provide care for their sick wives at home (being reluctant to hospitalize a spouse) than, for example, an unmarried sister – the man, as the head of the household, would be responsible for her and might think institutionalization was appropriate, if it was economically feasible (Anepaio, 2019: 10). In addition, when an upper-class woman exhibited symptoms of mental illness during her early years, she was usually unable to marry and was destined to be depend on her brother or her sister’s husband after her parents died (p. 12). Taking all this into consideration, I suggest that the higher hospitalization rates for single upper-class women were due to a lack of willingness as well as means to care for unmarried female relatives at home. However, at least some wealthy women were admitted voluntarily and stayed for a long time. For example, patient No. 347 was admitted on 2 January 1885. She was 34 years old, from St Petersburg, paid 85 roubles per month for a Class I ward, and was recorded as having represented herself (Vertritt sich selbst). Diagnosed with neurasthenia and hysteria, she left in the summer of 1887 as ‘improved’ (Gebessert entlassen). Cases like this clearly show that, in at least some cases, personal agency was involved, and there is no evidence of any direct coercive measures. However, only further reading of case records could reveal with more certainty what variables influenced the different admission numbers for married and unmarried women.
The diagnosing of women with gender-specific illnesses could indicate the extent to which stigmatization may have occurred. In Tartu, such illnesses were diagnosed in a small but significant number of female patients. Only 14 women were diagnosed with some sort of puerperal insanity, indicating that this gendered diagnosis was not systematically used to wrongfully institutionalize great numbers of women at the end of the nineteenth century in Tartu. Similar results were found by David Wright (2004: 165), who analysed records for an English county asylum. Additionally, it has been pointed out that female sexual behaviour outside the aim of reproduction was considered abnormal, possibly pathological, at the end of the nineteenth century (Neve, 1997: 243). In Tartu, there were in total six patients, all female, whose diagnoses were related to sexual behaviour or ideas. Three were diagnosed with ‘Nymphomania’, all in Class III wards and aged between 24 and 35. 21 Two were diagnosed with ‘Masturbatio’, both in Class II wards and aged 10 and 20. 22 One was diagnosed with ‘obsession of religious-sexual character’ (Zwangsvorstellungen religiose-sexuellen Character); she paid for a Class II ward and was 46 and single. 23
Based on these few cases, it would appear that these women’s social class was connected with perception of their sexual conduct. However, a pattern of gross misconduct involving the pathologizing of female sexuality with the help of the medical profession cannot be presumed based on these six patients. At the same time, all those diagnosed based on their sexual conduct were women, indicating that it was their sexuality, not men’s, that drew the attention of their families and community, and concerned them sufficiently that they were willing to pay for their cure and run the risk of stigmatization. Hysteria, the most famous, even infamous, nineteenth-century female ailment, was diagnosed in total of 137 hospitalizations. However, male hysteria as a diagnosis had started to receive more attention around the time the hospital was established (Micale, 1990: 365), and of the 137 patients diagnosed, 18 were men.
However, the data based on 139 female-specific diagnoses does not allow a definite conclusion to be drawn about the extent to which these women were victims of new classifications invented by psychiatrists attempting to redeem the failure of their therapeutic promises (Scull, 2006: 119). Nevertheless, there seemed to be a tendency in Tartu to associate women (and not men) with problems related to the reproductive organs or sexual conduct; a further analysis of their case histories should provide us with more detailed information, especially taking into account the fact that men with hysteria-like symptoms may have received a diagnosis of neurasthenia (Micale, 1990: 379).
Patients’ health status at discharge differs when gender and class variables are considered. First, high mortality among wealthy men stands out (Table 3), and I suggest that a diagnosis of late-stage syphilis was the reason; 28 per cent of the wealthy men in Tartu Hospital had neurosyphilis, meaning that they were in the disease’s terminal stages. 24 At the same time, 17 per cent of men in Class III wards had neurosyphilis. Also noticeable was the high proportion of wealthy women discharged as cured or improved, and the duration of their hospitalizations was noticeably less than for their male counterparts. This could be explained by the high proportion of upper-class women diagnosed with neuroses: 31 per cent were diagnosed with hysteria, neurasthenia or hypochondria, compared with only 11 per cent of Class III female patients. Patients suffering from ‘nerves’ or ‘neuroses’ often complained of fatigue, anxiety and vague physical symptoms undetectable by physicians (Rosenberg, 1962: 247). In an American context, it has been argued that neurasthenia makes ‘discomfort and unhappiness seem like abnormal conditions – medical symptoms that required therapeutic treatment’ (Schuster, 2011: 2). As such, these symptoms, and diseases for that matter, could be easily managed by changing the environment or just using a placebo, thus possibly explaining higher improvement rates and shorter stays for upper-class women. A conclusion can therefore be drawn, based on the state of patients’ health at discharge: class influenced gender differences more than the other way round. Patients’ state of health at discharge was very similar for men and women in Class III wards, while a gender difference among wealthy patients is clearly noticeable; health at discharge also varies when comparing wealthy and poor patients of the same gender. All this shows that gender and social class must be analysed together; any analysis of one that does not take the other into account yields incomplete results.
Elderly patients
Shorter (1997: 51) has suggested that changing family sentiments was one reason for the increasing institutionalization of the mentally ill as well as the demented elderly. They were once tolerated and part of the family, but by the end of the nineteenth century more and more families felt they needed help to manage such individuals. Do we see a disproportionately high number of elderly patients in Tartu Hospital? The average age of the patient population (Table 4) shows that during the study period only 4 per cent were patients aged over 60. In comparison, based on the 1897 census, 9.7 per cent of the population were over 60 (Palli, 1998: 29). However, a higher percentage of wealthy patients in that age group is seen in the hospital records: compared with the average of 25 per cent of hospitalizations being upper class, around half the seniors paid for Class I or II wards. Two conclusions can be drawn from these results. First, the low number of elderly patients compared with the average population shows that the hospital was not extensively used as a nursing home for the demented elderly by families no longer wishing to care for them. Second, the relatively high percentage of wealthy patients in this age group would suggest that wealthy families were more willing to seek a cure for their elderly than were poor patients and their communities. The poor, especially poor peasants, probably had somewhere to stay when they were too old to work, such as their own family’s farmhouse or in a ‘sauna’ (type of small dwelling) belonging to their landlord. Members of the nobility with a title but inadequate financial resources probably did not have a comparable social network that would ensure they could spend their old age in peace, especially in the case of women. But when we look at the gender differences in Tartu (Table 5) we see that wealthy older women (Classes I and II), possibly without family support, were not in a majority. Instead, there were more poor men whose institutionalization was deemed necessary by their families and communities. Perhaps the reason was again that women patients were easier to manage at home or that for men there was hope that hospitalization would restore their ability to work.
Age of the hospitalized patients in the University of Tartu Hospital for Mental and Nervous Diseases, 1881–95 (source: see Table 1).

For age ranges 0–19, 20–39, 40–59 and 60–89 years.
Gender of patients over 60 years old in different wards of the University of Tartu Hospital for Mental and Nervous Diseases, 1881–95 (source: see Table 1).

The fact that people aged 60–69 spent on average nine months longer in the hospital than their older counterparts requires an explanation. It would be reasonable to assume that the shorter stays of people in their 70s could be due to significantly higher mortality, but this cannot be supported by the figures: 24 per cent of patients in their 70s and 20 per cent in their 60s died in the hospital. Looking more closely at the details, we see that 15 out of 69 patients in their 60s were in hospital for over a year; six were diagnosed with dementia. 25 At the same time, no patient in their 70s with a diagnosis of dementia stayed longer than almost four months. From this, I suggest that in a very few cases wealthy families may have used the hospital as a nursing home for their elderly, but it was definitely an exception rather than the rule, and these patients may have been difficult to manage at home. In addition, families of patients in their 60s might have had some hope of a cure being achieved; families of patients in their 70s might have had lower expectations of the effectiveness of a long-term hospital stay.
Conclusion
Institutionalization of the insane in the second half of the nineteenth century has long interested medical historians. An example from the Russian Baltic Provinces is provided by this study of the patient population in the University of Tartu Hospital for the Mental and Nervous Diseases between 1881–95. The evidence shows that patients were institutionalized for relatively short periods, the median length of stay being 10 weeks; only 188 hospitalizations out of 2,184 lasted longer than a year. Although even short-term institutionalization could be used as a means of social control by families or communities, possible deviant behaviour, at least in the case of Tartu, did not result in long-term loss of freedom. Some records of voluntary admissions and of patients discharging themselves suggest at least some patient agency in regard to both admission and discharge. The fact that a number of patients escaped from the hospital suggests that some coercive measures were being used, the justification for which is not yet certain.
Analyses of patients’ admission, diagnosis and discharge show that gender and social class must be viewed together, as outcomes differed when these variables were combined. Women in upper-class wards had remarkably different outcomes compared with wealthy men and with women in lower-class wards. For instance, upper-class women were far more frequently diagnosed with neuroses than lower-class women, indicating that the more ambivalent symptoms exhibited in the case of neuroses were more specific to the upper classes. Women-specific diagnoses were also used in Tartu, for example puerperal insanity, but only in 14 cases; this is insufficient to allow for a conclusion of extensive stigmatization of women, because postpartum psychosis, for example, is an actual mental health problem affecting new mothers nowadays as well.
Sexual dysfunction was only diagnosed in women, and hysteria was recognized mainly in women, but 10 per cent of patients with the hysteria diagnosis were men, thus showing a change in the disease paradigm. This study demonstrates that although the Russian Empire has often been considered backward and economically underdeveloped and thus dissimilar to the rest of Europe, the pattern of the hospitalization of the mentally ill seems to have largely followed that of late nineteenth-century Western Europe: increasing numbers of mental hospitals and patients as well as upper- and middle-class women receiving special attention from psychiatrists. The Tartu case study also shows how the German academic tradition resonated there, a region on the periphery of both Europe and the Russian Empire.
Following on from these findings, further studies might focus on more specific issues, such as the extent to which coercion and discrimination were relevant factors or how exactly psychiatrists arrived at their diagnoses. These are topics that could be further enlightened by studying the individual patient case records from Tartu Hospital in more detail than was possible for this study, which primarily focused on the admission and discharge details.
Footnotes
Acknowledgements
I am indebted to my supervisor, Dr Martin Seppel, for his feedback, advice and encouragement. I would also like to thank Alex Savolainen and Yaroslav Stadnichenko for their help with the data analysis and translations, respectively.
Correction (Jan 2023):
Article updated; for further details please see the Article Note at the end of the article.
Declaration of conflicting interests
The author declares that there are no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Eesti Teadusagentuur [PRG318].
Article Note
The following updates were made to the patient numbers this article:
Page 429, abstract, line 6: “…139 hospitalized women …”
Page 439, line 3: “…137 hospitalizations”
Page 439, line 5: “…137 patients …”
Page 439, line 6: “… 139 female-specific diagnoses …”