
Abstract
Background
Patients with persistent postural-perceptual dizziness (PPPD) exhibit altered postural and gait dynamics, but development of these changes following precipitating illnesses is poorly understood.
Objective
To compare posture and gait metrics in patients with PPPD or subacute unilateral vestibulopathies (sAUVP) to healthy controls (HC).
Methods
Ten patients with sAUVP, nine with PPPD, and eleven HC completed the 10 Meters Walk Test (10MWT) (an eyes open task) and Fukuda Stepping Test (FST) (an eyes closed task). Gait stability, symmetry, and smoothness were compared among groups and correlated with Dizziness Handicap Inventory (DHI) scores.
Results
10MWT – Patients with PPPD had lower pelvis stability and gait symmetry than HCs. Patients with sAUVP had only lower pelvis stability. FST – Patients with PPPD and sAUVP had lower gait smoothness than HCs. Patients with sAUVP also had lower gait symmetry. Among patients with PPPD, DHI scores correlated positively with head stability.
Conclusions
PPPD and sAUVP caused abnormal pelvis stability when walking and gait smoothness when stepping but differed in effects on gait symmetry with the presence/absence of visual inputs. For PPPD, visual stimuli had destabilizing effects, whereas for sAUVP vision aided stability. Symptom severity in patients with PPPD was related to head stability.
Introduction
Persistent postural-perceptual dizziness (PPPD) is a chronic functional disorder characterized by persistent dizziness, instability, and non-rotational vertigo.1,2 The diagnostic criteria, established by the Barany Society in 2017, 3 include the persistence of vestibular symptoms for at least three months, exacerbated by upright posture, movement, and exposure to complex visual stimuli. While peripheral vestibular conditions are common triggers of PPPD, other conditions including vestibular migraine, central vestibular disorders, and mild traumatic brain injuries can also precipitate the disorder. 3 Recent clinical epidemiologic studies estimated the prevalence of PPPD among patients seeking treatment for dizziness to range from 14% in general internal medicine clinics, 4 to 20% in neurology clinics, 5 to over 40% in specialized dizziness centers, where it is often identified coexisting with other vestibular disorders. 6 Indeed, a significant number of individuals with chronic dizziness that were previously diagnosed with other conditions, are now considered to have PPPD. 7 PPPD-related handicap and sensitivity to exacerbating factors may be measured by patient reported outcomes such as the Dizziness Handicap Inventory (DHI) 8 and Niigata PPPD Questionnaire, 9 respectively.
Although PPPD is defined only by its symptoms, abnormalities in posture and gait, including stiffened posture with or without functional sway of the upper body and wide-based, shorter strides, have been measured in research studies of PPPD and related predecessors such as phobic postural vertigo 10 and chronic subjective dizziness. 11 Mechanisms responsible for the development of PPPD and these changes in posture and gait dynamics after precipitating events are incompletely understood. When triggering events are acute vestibular syndromes, the appearance of sensitivities to the three exacerbating factors of PPPD (upright posture, active or passive motion, and visual stimuli) in the subacute stage of illness (first 90 days) presaged later diagnoses of PPPD. 12 Although some patients with acute vestibular syndromes may develop PPPD, this is not an inevitable progression for all individuals. In studies predating the formal definition of PPPD, development of chronic PPPD-like dizziness after an acute unilateral vestibulopathy was predicted much less by the extent of peripheral vestibular damage than by the combination of visual dependence and heightened body vigilance. 13 The onset of stiffened posture with low amplitude, high frequency sway was reported in a single prospective case study of a patient who developed phobic postural vertigo following an acute unilateral vestibulopathy (vestibular neuritis). 14
Assessment of dynamic postural stability in patients with PPPD remains challenging. Recent developments in inertial sensors-based assessments allow for quantitative evaluations of gait disorders, potentially providing insight into fundamental mechanisms related to stability, symmetry, and smoothness of gait in people with different neurological disorders15,16 as well as in people with subacute unilateral vestibulopathy (sAUVP). 17 Furthermore, wearable sensor-based assessments enable participants to move freely with minimal spatial constraints, facilitating the evaluation of gait and posture in a more natural and flexible setting. The portability and ease of setup of wearable sensors allow for data collection in environments that better reflect real-world conditions, thereby enhancing the ecological validity of the assessment.
We hypothesized that an instrumental evaluation comparing patients with PPPD to patients with sAUVP and healthy controls would demonstrate an evolution of altered posture and gait dynamics from the subacute to chronic phases of illness. From a rehabilitative perspective, quantitative assessments of these differences might also allow clinicians to establish better tailored rehabilitative programmes for patients with PPPD, potentially starting during the sAUVP phase.
Thus, the primary aim of this study was to measure through an ecological sensor-based assessment any alterations in dynamic postural stability, symmetry, and smoothness of gait in patients with PPPD, patients with sAUVP, and healthy control (HC) participants to identify changes that might elucidate the underlying mechanisms of onset of PPPD. The secondary aim was to assess the correlation between the obtained sensor-based information and dizziness-related handicap.
Materials and methods
This cross-sectional study was carried out at the IRCCS Santa Lucia Foundation from July 2022 to February 2024. All procedures involved in this study adhered to the ethical standards outlined in the pertinent national and institutional guidelines for human experimentation, as well as the principles laid out in the World Medical Association Declaration of Helsinki. The study was carried out according to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. The Local Independent Ethics Committee of IRCCS Santa Lucia Foundation approved the study with protocol number CE/2024_021. Written consent was obtained from all participants for the publication of results obtained from their clinical examinations and instrumental tests. This study is part of a clinical trial registered with ID NCT05831618.
Participants
Participants were recruited by the Laboratory of Neuromotor Physiology of IRCCS Santa Lucia Foundation. The sample size was calculated using G*Power 3.1 Software. 18 We used the Cohen’s d effect size derived from a previous similar study 19 which used the same postural stability index as the present study. The effect size was estimated at a value of 1.23. Based on an alpha level of 0.05 and a power of 80%, the required sample size per group was determined to be approximately nine participants. The age for recruitment in the study was restricted between 18 and 70 years. Eligibility criteria for PPPD patients included a diagnosis of PPPD according to the diagnostic criteria of the Barany Society. 3 Patients were diagnosed by otologists and referred to the Santa Lucia Foundation unit, where they completed a video head impulse test (vHIT) and magnetic resonance imaging of the head. Patients with sAUVP met diagnostic criteria of the Barany Society for an acute unilateral vestibulopathy 20 no more than three months prior to enrollment and were still experiencing disturbances in static and dynamic balance that had an impact on the activities of daily living (ADLs), and had evidence of unilateral vestibular hypofunction on bedside examination and vHIT. Eleven HC were included after careful collection of their medical history to exclude those who reported the presence of disorders that could have influenced motor performance. Individuals with other neurological conditions, vestibular bilateral hypofunction, orthopedic, or cardiac comorbidities were excluded.
Demographic and clinic characteristics of the enrolled participants.
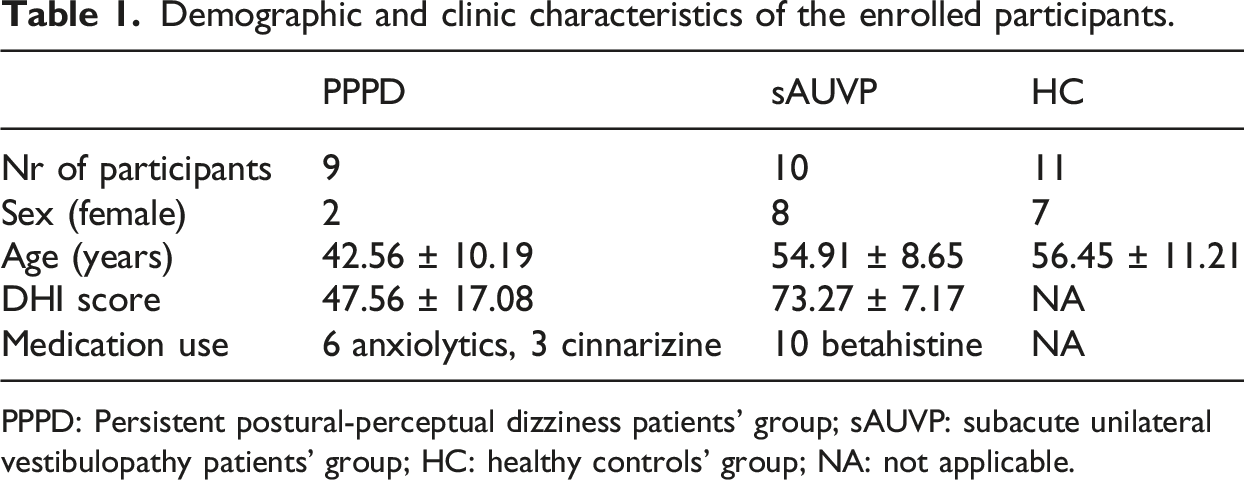
PPPD: Persistent postural-perceptual dizziness patients’ group; sAUVP: subacute unilateral vestibulopathy patients’ group; HC: healthy controls’ group; NA: not applicable.
Experimental protocol
Participants were evaluated while executing two motor tasks: the 10-Meters Walk Test (10MWT), and the Fukuda Stepping Test (FST).21,22 During the 10MWT, participants were asked to walk at their preferred speed along a 14 m linear path. Data at steady-state walking speed from the central 10 meters were analyzed, excluding the initial acceleration and final deceleration phases. The FST is a blindfolded march in place of one-minute duration. Figure 1 represents the study flow diagram along with a schematic representation of the 10MWT and FST. To the left: schematic representation of the tasks. 10MWT: participants were asked to walk at their preferred speed on a 14 m trail; FST: participants were asked to walk on the spot with eyes closed and arms lifted at 90° from the body. To the right: study flow diagram.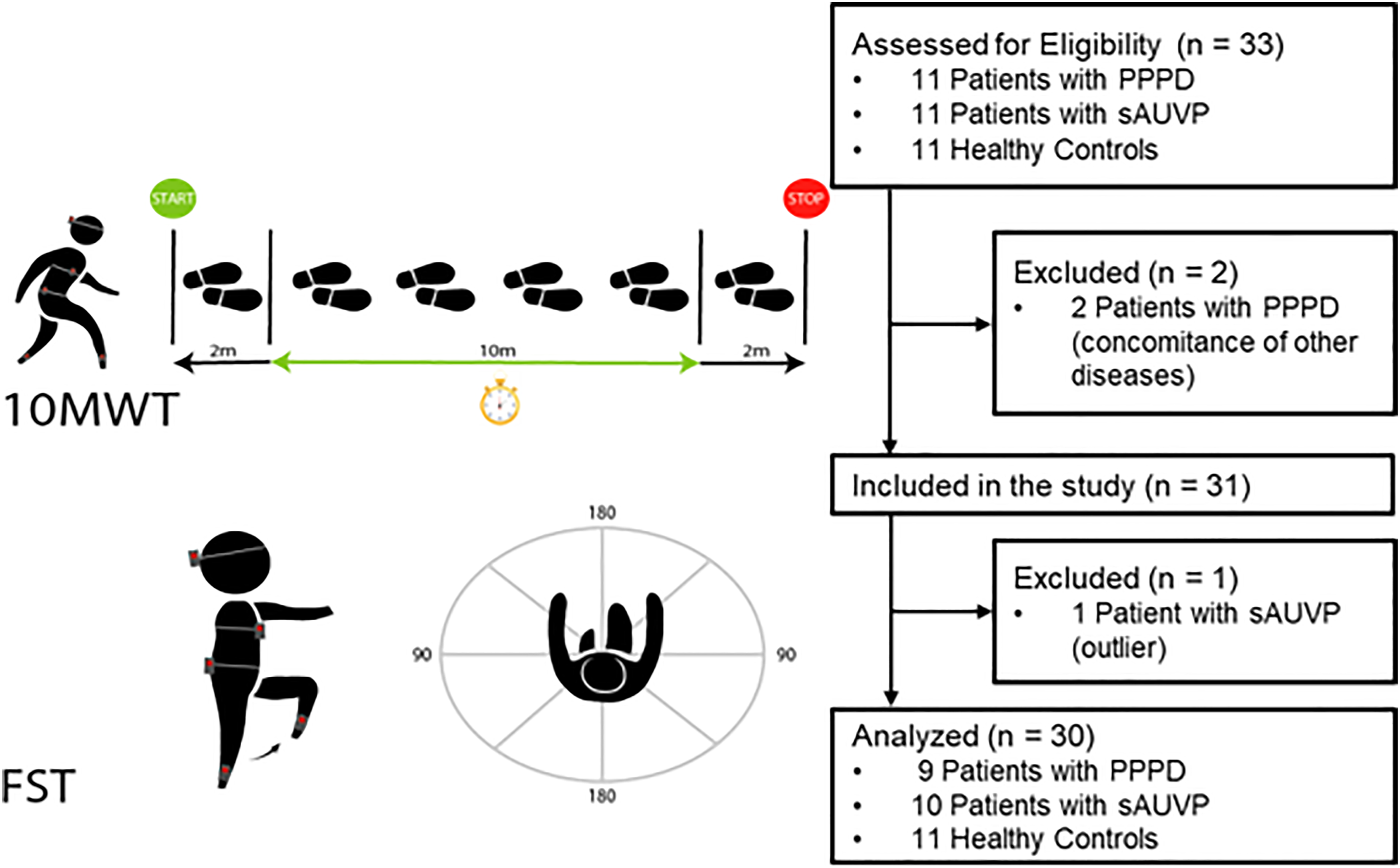
Participants belonging to the PPPD group and the sAUVP group were also asked to report their perceived handicap related to dizziness using the DHI, a scale that consists of 25 questions, scored 4 (always experienced problem), 2 (sometimes) or 0 (never), to assess the subjective perception of one’s balance. On average, sAUVP patients’ DHI scores reflected severe self-perceived handicaps, while PPPD patients’ score was associated with a moderate handicap.
Gait assessment
Instrumental assessment of the gait parameters was conducted using five wearable wireless inertial sensors (128 Hz, Opal, APDM, Portland, Oregon, USA), operating on internal batteries. Each inertial measurement unit (IMU) contains a triaxial accelerometer, measuring accelerations along three axes aligned with the sensor case, and a triaxial gyroscope, which measures angular velocities around the same axes. Three wearable sensors were positioned at the level of the occipital cranium bone, of the sternum, and at L4-L5 level and were carefully aligned with the antero-posterior (AP), medio-lateral (ML), and cranio-caudal (CC) anatomical axes of the participant’s body. Two sensors were placed at the tibias, near the lateral malleolus, and were used for step segmentation. Gait parameters were extracted from raw data by means of custom MATLAB® scripts (MATLAB R2022b, MathWorks).
Different gait spatiotemporal parameters were considered for the two tests: during the 10MWT we evaluated stride frequency, stride duration, and walking speed, whereas for the FST we considered the number, the frequency, and the duration of steps.
In addition, we used the inertial sensors data to assess postural stability, symmetry, and smoothness of gait using the following parameters, calculated over each segmented stride.
Postural stability
Normalized Root Mean Square (nRMS) values of each stride acceleration were obtained from the acceleration measured by IMUs placed at pelvis, trunk and head for the AP, ML, and CC components. This measure is an indicator of postural stability: high values have been associated with a decrease in postural stability because of the higher acceleration levels. It is calculated as: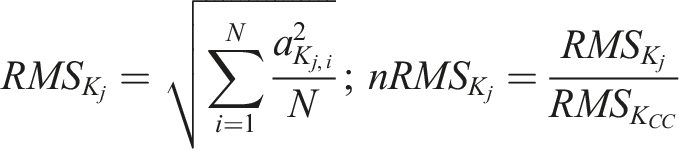
Symmetry
Improved Harmonic Ratio (iHR) was measured at the level of the pelvis, for each acceleration component (AP, ML, and CC). It was defined as the ratio between the power of the intrinsic harmonics (PI) over the total power of the signal (corresponding to intrinsic and extrinsic harmonics). The intrinsic harmonics are the even harmonics for the AP and CC components of acceleration, and the odd harmonics for the ML acceleration component; extrinsic harmonics are the odd harmonics for the AP and CC components of the acceleration, and the even harmonics for the ML acceleration component.
24
The result is a normalized index, ranging from 0 (total asymmetry) to 100 (total symmetry) according to the following formula: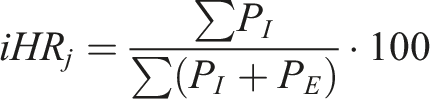
Smoothness
Log dimensionless jerk (LDLJ) is a measure of smoothness, obtained from the pelvic sensor data:

Lower LDLJ values closer to zero have been associated with higher levels of smoothness of translational/rotational movement. 25 We computed the linear and angular LDLJ using data from the accelerometer (LDLJa) and gyroscope (LDLJw) sensors, respectively.
Data collection
Inertial sensors were securely fixed to the relevant body segments using Velcro straps to minimize oscillations and thereby reduce motion artifacts. Two physiotherapists closely accompanied participants throughout the assessment to prevent falls, reiterating all instructions prior to each test administration. All collected data were electronically stored through an interface compliant with European (GDPR No. 679/2016) and Italian (D.L. 101/2018) data protection regulations. Personal data and contacts were safeguarded with a password, recorded in a separate dataset, and denoted via an alpha-numeric ID.
Statistical analysis
Descriptive and inferential statistical analyses were performed using the RStudio software (R version 4.3.2, RStudio: Integrated Development for R. RStudio, PBC, Boston). Statistical level of significance was set to alpha = 0.05.
We excluded from further analysis one sAUVP patient because several gait parameters differed more than 5 times the variance from the mean values of the sAUVP group.
We checked for normality of distribution of the estimated parameters using the Shapiro-Wilk test and we investigated differences among groups using the Kruskal-Wallis’ test. Post-hoc pairwise comparisons were performed using the Wilcoxon rank-sum test with Benjamini-Hochberg correction.
Results of the Wilcoxon rank-sum are reported as U-statistics, z-scores and corrected p-values (p-adj). For these tests, statistical level of significance was set to alpha = 0.05.
The correlation between gait indexes and DHI scores of the PPPD and sAUVP groups was assessed through the Spearman’s rank correlation coefficient (ρ). For these correlation analyses, statistical level of significance was set to a more restrictive alpha = 0.01, due to the small number of datapoints. Analysis of Covariance (ANCOVA) was performed to evaluate potential confounding factors such as age and DHI score. The ANCOVA with age as a covariate was conducted across all three groups (HC, PPPD, sAUVP), whereas the ANCOVA with DHI as a covariate was performed on the two patient groups (PPPD, sAUVP), as DHI was not applicable to the healthy control group.
Results
Eleven patients with PPPD were initially recruited for the study. The results of vHIT assessment were normal for nine patients (with a vestibulo-ocular reflex gain between 0.7 and 1.2 for vertical canals and between 0.8 and 1.2 for horizontal canals), while two patients had slightly sub-threshold gains (gains for the left-anterior canal were 0.65 and 0.67 for subjects A and B, respectively, and gains for the right-posterior canal were 0.63 and 0.52). These two patients were included in the study. One patient who showed a bilateral low gain in the vHIT was excluded. MRI scan did not reveal any concomitant neurological disease for 10 patients. However, one participant was diagnosed with a pineal cyst compressing the dorsal part of the superior colliculus and thus was excluded from the study. Among the nine remaining patients with PPPD, precipitant causes were vestibular neuritis (2 patients), vestibular migraine (2 patients), panic attacks (1 patient), delayed Ménière (1 patient), benign paroxysmal positional vertigo (BPPV) (2 patients), episode of vertigo of unknown cause (1 patient). Eleven people with sAUVP were recruited. Seven people were diagnosed with vestibular neuritis, 3 with Ménière disease and one underwent vestibular neurectomy. All sAUVP patients were tested in the subacute phase less than one month after the vestibular damage (less than 3 months for the patient who underwent vestibular neurectomy), so they didn’t qualify for the diagnosis of PPPD. As for patients with Ménière, one was tested less than one month after gentamicin treatment and the other two were tested less than a month after serious vertigo attacks. One sAUVP patient was excluded because of exceedingly altered gait and postural performance, according to outlier analysis.
This excluded participant showed values that differed significantly from the rest of the sAUVP group in several parameters measured during 10MWT and the FST. Data from the 10MWT showed reduced iHR values compared to the rest of the sAUVP group across all three axes (around 60 compared to average values of 85–95), while the nRMS measured at pelvis and trunk level along the ML axis was above 1.2, whereas average group value was below 1. Data from the FST similarly revealed reduced iHR values for this participant compared to the sAUVP group. We conducted a sensitivity analysis to assess the impact of excluding this participant on the main group comparisons, by applying the non-parametric Kruskal-Wallis test to two datasets: with and without the excluded participant. For all parameters investigated in the 10MWT, we found no change of significance in group comparisons, except for walking speed, which became significant by excluding the outlier. Regarding the FST, the parameters that showed statistically significant differences between groups were not affected by the exclusion of the participant. In both cases were registered small fluctuations of p-values that did not cross the 0.05 threshold, with the only exception being walking speed in the 10MWT (which already had a borderline p-value before the exclusion of the outlier). Although the analysis did not necessarily require the exclusion of the outlier due to the use of non-parametric statistical methods, we opted for removing the outlier participant as conservative measure. This allowed us to ensure that the results were not influenced by a single anomalous data point.
Statistical analyses were conducted on 9 PPPD patients, 10 sAUVP patients and 11 HC. Shapiro-Wilk tests on the distributions of the gait parameters indicated that data were not normally distributed and, therefore, we adopted non-parametric statistics. A significant overall difference among groups in walking speed during the 10MWT (Kruskal-Wallis χ2(2) = 7.12; p = 0.028) was found, but pairwise post-hoc tests failed to show significant differences between any of the subject groups after correction for multiple comparisons. There was a significant difference among groups with respect to the nRMS on the ML axis at the pelvis level (Kruskal-Wallis χ2(2) = 8.69; p = 0.013). Post-hoc pairwise comparisons adjusted for multiple comparisons revealed significantly higher values of nRMS for patients with PPPD (U = 20.00, z = −2.24, p-adj = 0.038) and sAUVP (U = 16.00, z = −2.75, p-adj = 0.014) than HC, indicating less postural stability in both groups of patients with respect to HC (Figure 2(a)). A significant overall difference among groups also was found for the iHR on the AP axis (Kruskal-Wallis χ2(2) = 6.86; p = 0.032), due to significantly lower values between PPPD and HC groups (U = 81.00, z = 2.39, p-adj = 0.048) and indicating decreased symmetry of gait only in patients with PPPD compared to HC (Figure 2(b)). Stability and symmetry parameters did not differ between patients with PPPD versus those with sAUVP. Gait smoothness parameters showed no significant differences among all three subject groups. (a) Normalized root mean square (nRMS) values on ML axis at pelvis level for the three groups during 10MWT; (b) Improved harmonic ratio (iHR) on the AP axis measured at the pelvis level for the three groups during 10MWT. AP: antero-posterior; ML: medio-lateral. Statistically significant differences between groups are indicated as: * (p < 0.05).
ANCOVA between groups showed a significant difference (p<0.01) in the DHI score, whereas the effect of age as a covariate parameter was not statistically significant. We conducted the ANCOVA on the parameters that were statistically significant in the Kruskal-Wallis test, namely “RMS ML Ios pelvis” and “iHR AP” for the 10MWT, and “iHR ML” and “LDLJw CC” for the FST, controlling for both age and DHI. Regarding the analysis with DHI as a covariate, we found a significant effect of DHI for the “iHR_ML” parameter (F = 5.554, df = 1, p = 0.033) from the FST data, while the difference between the PPPD and sAUVP groups was not statistically significant (F = 1.991, df = 1, p = 0.18). Thus, when controlling for DHI scores, the difference in “iHR_ML” between the two groups did not reach significance.
A significant overall difference among groups was found during the FST for iHR on the ML axis (Kruskal-Wallis χ2(2) = 9.22; p = 0.010) due to significantly lower iHR in patients with sAUVP compared to patients with PPPD (U = 12.00, z = −2.69, p-adj = 0.015) and HC (U = 91, z = 2.54, p-adj = 0.015), indicating less symmetric gait in the sAUVP group (Figure 3(a)). A significant overall difference also was found among groups for LDLJw on the CC axis (Kruskal-Wallis χ2(2) = 7.47; p = 0.024) due to significantly lower values for patients with PPPD (U = 80, z = 2.32, p-adj = 0.03) and sAUVP (U = 88, z = 2.32, p-adj = 0.03) compared to HCs, indicating lower gait smoothness in both patient groups (Figure 3(b)). (a) Improved harmonic ratio (iHR) on ML axis for the three groups during Fukuda Stepping Test; (b) angular log dimensionless jerk (LDLJw) on CC axis for the three groups during Fukuda Stepping Test. AP: antero-posterior; ML: medio-lateral, CC: cranio-caudal. Statistically significant differences between groups are indicated as: * (p < 0.05).
Tables with the results of the statistical tests applied to all parameters derived from the instrumental assessments are reported in the supplemental materials (Tables 2 and 3).
Handicap correlations
Finally, we examined correlations between DHI scores and gait and posture parameters in the PPPD and sAUVP groups. We found only one significant result. In patients with PPPD, DHI scores correlated positively with the nRMS at head level in the AP direction during the 10MWT (ρ = 0.90, p = 0.006). In patients with sAUVP, a borderline negative correlation was found between DHI scores and the nRMS at head level in the ML during the 10MWT (ρ = −0.77, p = 0.010), but datapoints displayed definite non-linearities. All correlation coefficients are reported in the supplemental materials (Table 4).
Discussion
In this study, we used ecological sensor-based assessments to identify potential alterations of postural stability, symmetry, and smoothness of gait in patients with PPPD and sAUVP versus HCs during straight walking with eyes open (10MWT) and during on-the-spot stepping while blindfolded (FST). We found decreased postural stability and a lower degree of gait symmetry in patients with PPPD with respect to HC during the 10MWT. Previous studies have reported that patients with phobic postural vertigo (PPV) 10 and chronic subjective dizziness, 11 two precursors of PPPD before its unifying definition, had an increase of high frequency/low amplitude sway activity and poor balance performance on posturography testing, respectively. Co-activation of anti-gravity muscles may be responsible for the increase seen in high-frequency/low-amplitude sway of patients with PPV. This motor strategy results in stiffening of the stance, perhaps aimed at achieving better control of the acceleration of the centre of mass. 26 Our results suggest that patients with PPPD might adopt similar strategies. Changes in postural stability in the AP direction at the level of the head correlated with severity of dizziness handicap suggesting that patients with PPPD may be particularly sensitive to forward-backward motions of their heads with their eyes open.
The sAUVP group had higher levels of dizziness handicap than the PPPD group reflecting severe impairment during the subacute period of their illnesses versus moderate longer-term impairment in patients with PPPD. According to the results of the ANCOVA test, DHI difference between the two groups is inherent to the group composition, as participants in the subacute phase perceive their symptoms as more severe than those in the chronic phase. There is a possibility that the DHI scores reported by the participants are a consequence of the differences in postural stability parameters between the groups.
Patients with sAUVP also had lower gait symmetry during the FST than both of the other groups indicating that they had more difficulty than the others in stabilizing movements with their eyes closed, which is expected given their deficits in peripheral vestibular functioning. Previous studies demonstrated that patients with sAUVP employed asymmetric strategies during blindfolded motor tasks 19 and that visual cues significantly improved their walking in well-lit environments versus darkness.27,28 Patients with PPPD were unaffected by the absence of visual cues on the FST indicating that they were able to adopt postural control strategies similar to HCs. They fared worse when visual stimuli were present during the 10MWT, which is consistent with criterion B of the diagnostic definition (exacerbation of symptoms with complex or moving visual stimuli). 3 Although this study appears to confirm the alteration of visual sensitivity in patients with PPPD, the two walking tests we used differ for the type of kinematic patterns involved. Because of this, differences between the tasks cannot be conclusively attributed to a sensitivity to visual stimuli. Our results, however, pave the way for further studies to assess the interference of visual stimuli through both open-eye and closed-eye conditions during the same motor task such as a standing march. It will also be possible to incorporate sudden visual stimuli or simulate crowded and chaotic environments through virtual reality to assess how patients with PPPD respond under these conditions.
From a rehabilitative perspective, our findings could offer significant insight into the management of PPPD, in agreement with what was reported in a previous review article. 29 The observed differences between patients with PPPD and sAUVP in postural stability and gait dynamics may enable rehabilitative professionals to consider the necessity of PPPD patients to overcome visual sensitivity and the different compensatory strategies that patients may adopt during the subacute stages of vestibular diseases compared to chronic dizziness. Although this aspect has been studied, 29 future clinical trials evaluating the effectiveness of rehabilitation training based on visuo-vestibular interaction in managing patients with PPPD will be valuable. Future research is necessary to confirm these findings and explore the effectiveness of tailored rehabilitative approaches for patients with PPPD.
Our ecological sensor-based approach also affords a potential avenue for use in well-designed clinical trials aimed at evaluating the effectiveness of tailored rehabilitative programs on aspects such as dynamic stability, symmetry, and smoothness during locomotion in PPPD.
Finally, it is worth noting the limitations of our study, particularly the small sample sizes of all groups. We may not have had sufficient statistical power to detect other important differences between groups. In addition, the small sample size may also increase the likelihood of overestimating effect sizes and reduce the probability that significant results reflect true effects. 30 Furthermore, we did not perform a psychological assessment as part of this study, which limits our ability to fully explore the impact of these factors on our findings. Considering the importance of personality traits and anxiety in postural control, 31 we think that further studies are needed to incorporate comprehensive psychological assessments to better understand the interplay between psychological factors and postural control in these patient groups. Furthermore, further studies should directly compare performance with and without visual cues during the same test to better understand these differences.
Nevertheless, while the differences noted between patients with sAUVP and PPPD suggest that deficiencies in posture and gait control evolve from the subacute to chronic phases, this cannot be definitively attributed to differences in chronicity alone, but also to the difficulties in integrating complex visual stimuli for those who develop PPPD. This merits future study as a potential avenue to better understand the complex interplay of factors that contribute to these observed differences and for developing tailored rehabilitative interventions for individuals with PPPD.
Conclusion
Patients with PPPD patients exhibited quantitative alterations of postural stability that differed from those of patients with sAUVP and HC in a pattern that emphasized differences in control of posture and gait in conditions with versus without visual information. Positive correlations between dizziness handicap and head stability with eyes open reinforce the sensitivity that patients with PPPD have processing complex or moving visual stimuli. Differences between patients with PPPD and sAUVP may be exploited to refine rehabilitative interventions.
Supplemental Material
Supplemental Material - Dynamic postural stability, symmetry, and smoothness of gait in patients with persistent postural-perceptual dizziness
Supplemental Material for Dynamic postural stability, symmetry, and smoothness of gait in patients with persistent postural-perceptual dizziness by Marco Tramontano, Gianluca Paolocci, Diego Piatti, Giuseppe Attanasio, Laura Casagrande Conti, Elena Bergamini, Leonardo Manzari, Francesco Lacquaniti, Jeffrey P. Staab, Gianfranco Bosco, Iole Indovina in Journal of Vestibular Research.
Statements and declarations
Footnotes
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Italian Ministry of Health (RF-2019-12369194 and IRCCS Fondazione Santa Lucia Ricerca Corrente), by the U.S. Department of Defense Congressionally Directed Medical Research Program W81XWH1810760 PT170028, by #NEXTGENERATIONEU (NGEU) funded by the Ministry of University and Research (MUR), National Recovery and Resilience Plan (NRRP), project MNESYS (PE0000006)–A Multiscale integrated approach to the study of the nervous system in health and disease (DN. 1553 11.10.2022), by #NEXTGENERATIONEU (NGEU), Ministry of Health, National Recovery and Resilience Plan (NRRP), PNRR-MCNT2-2023-12377870 and by #NEXTGENERATIONEU (NGEU), Ministry of University and Research (MUR), National Recovery and Resilience Plan (NRRP), PRIN 2022B42X54.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.