
Abstract
Background
Vestibular neuritis (VN) has faced various diagnostic challenges despite years of clinical use. This study analyzes 65 cases based on diagnostic criteria for acute unilateral vestibulopathy/vestibular neuritis (AUVP/VN) 2022.
Method
Through medical history, physical examinations, and vestibular function tests, including the caloric test, video-head impulse test (v-HIT), and vestibular evoked myogenic potentials (VEMPs), we thoroughly tested vestibular receptor dysfunction of AUVP/VN cases. Patients were divided into two groups: total vestibular nerve branch dysfunction (tVND) and partial vestibular nerve branch dysfunction (pVND). The tVND group was defined as involving all receptors innervated by the superior and/or inferior vestibular nerve. The pVND group was defined as involving any other combination pattern of vestibular receptors (at least one). Sociodemographic and clinical characteristics were analyzed. All patients were followed up for 6 months. Changes in DHI scale scores and residual or new symptoms were investigated.
Results
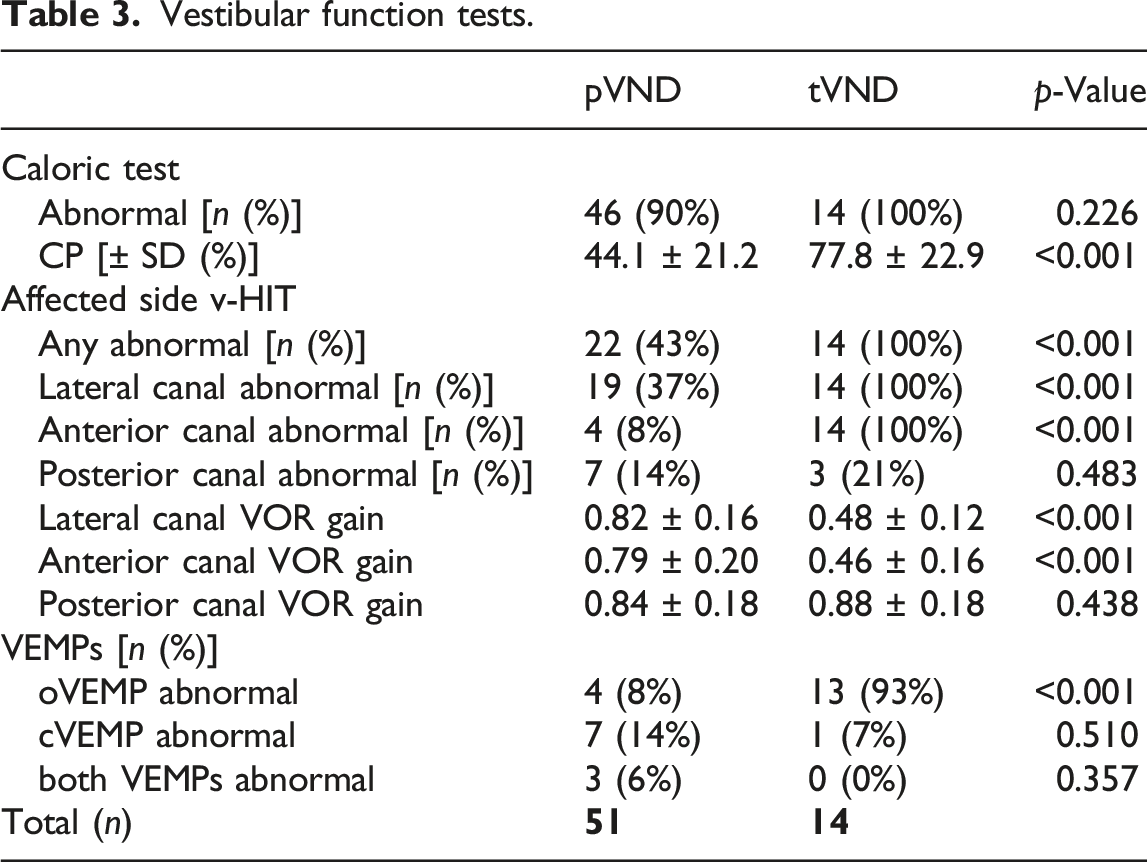
A total of 65 AUVP/VN patients with vestibular receptor dysfunction were included. There were 51 cases in the pVND group and 14 in the tVND group. Compared to the pVND group, the tVND group showed longer vertigo duration (p < 0.05), higher rates of postural symptoms (p < 0.01), higher rates of abnormal caloric tests (p < 0.05), higher canal paresis values (p < 0.001), and higher rates of deficient vestibulo-ocular reflex (VOR) gain in v-HIT (p < 0.001). After a 6-month follow-up, the pVND group showed lower DHI scores (p < 0.001) and higher cure rate (p < 0.001).
Conclusions
In general, patients in the tVND group showed a more severe disease and worse prognosis than those in the pVND group. The substitution of the term AUVP for VN is appropriate and aligns with the clinical characteristics of the cases. However, the diagnosis of AUVP should be further developed to include otolith organ dysfunction.
Introduction
Acute unilateral vestibulopathy (AUVP), as a synonym for vestibular neuritis (VN), is an acute peripheral vestibular syndrome defined by an acute unilateral loss of peripheral vestibular function without evidence for acute central neurological or acute audiological symptoms or signs.1,2 Various terms have been used to describe this condition, such as vestibular neuronitis, acute vestibular neuropathy, and acute vestibulopathy.3–5 In April 2022, the Barany Society established the AUVP/VN diagnostic criteria, including four diagnostic categories. 2 Given that a viral etiology cannot be fully demonstrated, the criteria formally recommended AUVP as a preferred synonym for VN. The established AUVP diagnostic criteria include (A) acute or subacute onset of sustained spinning or non-spinning vertigo of moderate to severe intensity with symptoms lasting for at least 24 hours; (B) spontaneous peripheral vestibular nystagmus with a trajectory consistent with the affected canal and enhanced by visual fixation removal; (C) evidence of a clear reduction in vestibulo-ocular reflex function in the direction opposite to the fast phase of nystagmus; (D) no acute central nervous system or auditory symptoms; (E) no acute central nervous system signs; and (F) symptoms not better explained by other diseases. AUVP in evolution (eAUVP) reduces the duration requirement to 3–24 hours and probable AUVP (pAUVP) includes patients with insufficient evidence of vestibulo ocular reflex (VOR) impairment. History of acute unilateral vestibulopathy includes patients with previous episodes of AUVP. The change in terminology from neuritis to vestibulopathy is more consistent with clinical features.
The widely accepted etiology of VN is reactivated herpes simplex virus (HSV).6,7 The patient may have a history that suggests the reactivation of a neurotropic virus, such as a recent bacterial or viral infection, fever, distressing family events, severe perimenstrual discomfort, or sleep deprivation. However, the lack of compelling structural evidence for a viral infection still raises doubts. 8 Meanwhile, neither history nor blood tests support a recent viral infection in approximately half of patients with AUVP, raising questions about the evidence for a vestibular nerve lesion. 6
The lesions of AUVP may be located not only in the vestibular nerve but also in specific vestibular receptors. Thus, comprehensive vestibular tests are important for the diagnosis and classification of AUVP. However, the recent Barany Society criteria do not include evidence of otolith dysfunction provided by vestibular evoked myogenic potentials (VEMPs), which may be helpful in localizing the lesion.
In this prospective cohort study, VEMPs were used as a criterion in addition to caloric testing and v-HIT to divide patients into different groups based on patterns of impaired sensory receptor distribution. Groups included those with total vestibular nerve branch dysfunction (tVND) and those with partial vestibular nerve branch dysfunction (pVND).
Methods
Patients diagnosed with AUVP from June 1, 2022, to June 1, 2023, at the China Air Force Medical Center’s Vertigo Center outpatient and inpatient departments were included in this study. The study had a prospective design and received local ethics committee approval from the hospital. Patients were evaluated by a neurotologist from the Vertigo Center for a new complaint of vertigo. All of the data at the first visit were acquired during the episode of acute vestibular symptoms.
After obtaining informed consent, the following information was obtained: sociodemographic characteristics, presence and duration of vertigo, occurrence of dizziness, positional symptoms, nausea, vomiting, fecal incontinence, tinnitus, ear fullness, self-reported hearing loss, headaches, photophobia, phonophobia, and recent viral infection history. Before vestibular function tests, spontaneous nystagmus without visual fixation, optokinetic nystagmus, gazeholding function, smooth pursuit, and saccades were investigated to exclude central lesions, and pure tone audiometry, tympanometry, and acoustic reflex measurement were conducted to exclude cochlear lesions.
All patients with excluded cochlear and central lesions underwent the caloric test, video-head impulse test (v-HIT), ocular vestibular evoked myogenic potentials (oVEMP), and cervical vestibular evoked myogenic potentials (cVEMP), assessing function of semicircular canals, utricle, and saccule. The caloric test used 30°C and 44°C water for stimulation. Canal paresis (CP) above 20% indicated unilateral ultra-low frequency VOR dysfunction in the lateral semicircular canal. In v-HIT, VOR gain values below 0.80 for the lateral semicircular canals and below 0.70 for the anterior and posterior semicircular canals indicated high-frequency VOR dysfunction. In the VEMP tests, absence of unilateral waveforms or bilateral asymmetry above 30% indicated otolith dysfunction.
A clinical diagnosis of AUVP was based on the current Barany Society criteria for AUVP/VN. All patients included in this study met the criteria of AUVP or eAUVP according to the diagnostic categories. 2
The tVND group included patients with vestibular receptor organ dysfunction of all of the organs innervated by one or both vestibular nerve branches. To be more specific, the tVND group had dysfunction of the utricle, the lateral semicircular canal, and the anterior semicircular canal, and/or dysfunction of the saccule and the posterior semicircular canal. The pVND group included patients with dysfunction of at least one receptor organ for any other combination. Based on the receptors involved, patients in the tVND group were divided into superior tVND (stVND), inferior tVND (itVND), and total tVND (ttVND). Patients in the pVND group, who showed heterogeneity according to the receptors involved, could be divided into canal pVND (cpVND), otolith pVND (opVND), and canal-otolith pVND (c-opVND). Demographic features, symptoms, signs, and results of vestibular function tests were subjected to statistical analysis.
The treating physician formulated the treatment plan, including drug therapy and vestibular rehabilitation, and the dose was adjusted according to the results of the return visit and follow-up. Drug therapy was mainly used for anti-inflammation, improving microcirculation, and nerve nourishment, such as dexamethasone, betahistine, ginkgo biloba, and mecobalamin.9–11 Antiviral agents were sometimes used in patients with a clear history of recent viral infection. The vestibular rehabilitation and subsequent guidance were carried out by a full-time vestibular rehabilitation therapist. According to the baseline evaluation, the program and dosage were determined, including gaze stabilization exercises, balance and gait training, and walking for endurance. 12
Follow-up was initiated after the initial visit for outpatients or discharge for inpatients at 2 weeks, 1 month, 2 months, 4 months, and 6 months. Additional visits could be performed according to the changes of the condition. Primary outcomes measured changes in DHI score at 6 months. Secondary outcomes included recurrence of persistent vertigo and occurrence of secondary BPPV during the 6 months follow-up. Cure was defined as DHI score less than 30 and 2 consecutive months without vestibular symptoms, including vertigo, dizziness, posture symptoms, or vestibular-visual symptoms. Remission was defined as a decline in DHI grade and patients reporting a reduction in chief complaint symptoms. Otherwise, the treatment was considered ineffective.
Statistical analysis was performed using IBM SPSS Statistics 27.0.1.0. Each analysis between subgroups in the same primary group was reported. Normality was evaluated using the Kolmogorov–Smirnov test, and homogeneity of variance was evaluated using Levene’s test before intergroup comparisons. Statistical analyses were conducted using the chi-square test, one-way analysis of variance, and Wilcoxon–Mann–Whitney U test. A p-value less than 0.05 was considered statistically significant.
Results
Sociodemographic characteristics.

Symptoms.

Vestibular function tests.
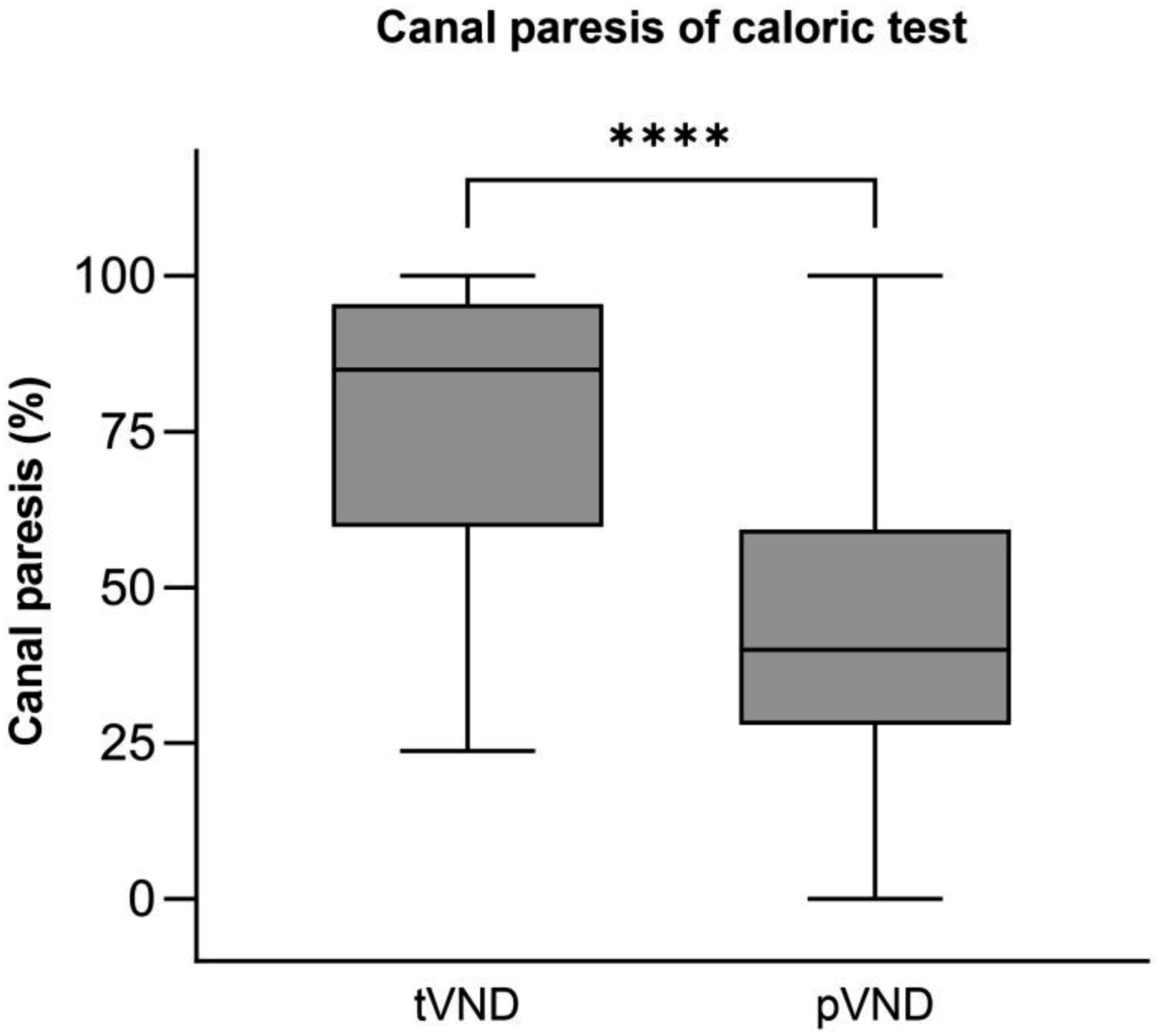
Box-and-whisker plot showing CP values of caloric tests by the tVND and pVND groups. The top bar denotes the maximum value, the upper edge of the box denotes third quartile (75%), the middle bar inside the box denotes the median (50%), the lower edge of the box denotes first quartile (25%), and the bottom bar denotes the minimum value. A t-test demonstrated that the CP values of patients in the tVND group were significantly higher than in the pVND group (p < 0.001).
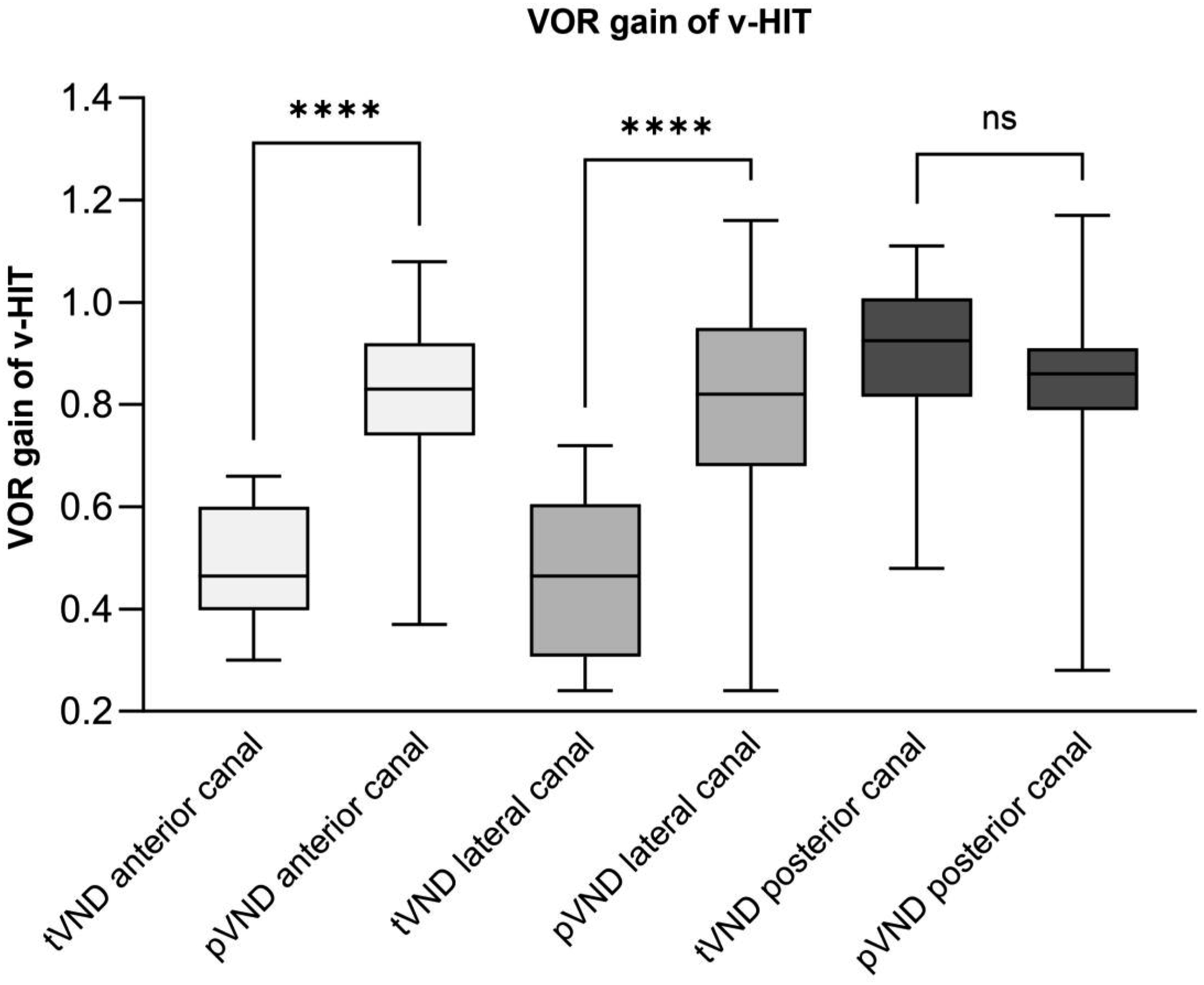
Box-and-whisker plot showing VOR gain of v-HIT by the tVND and pVND groups. t-Tests demonstrated that VOR gain in lateral and anterior canals of patients in the tVND group was significantly lower than in the pVND group (p < 0.001), while the posterior canal showed no significant difference (p > 0.05).
Follow-up and outcomes.
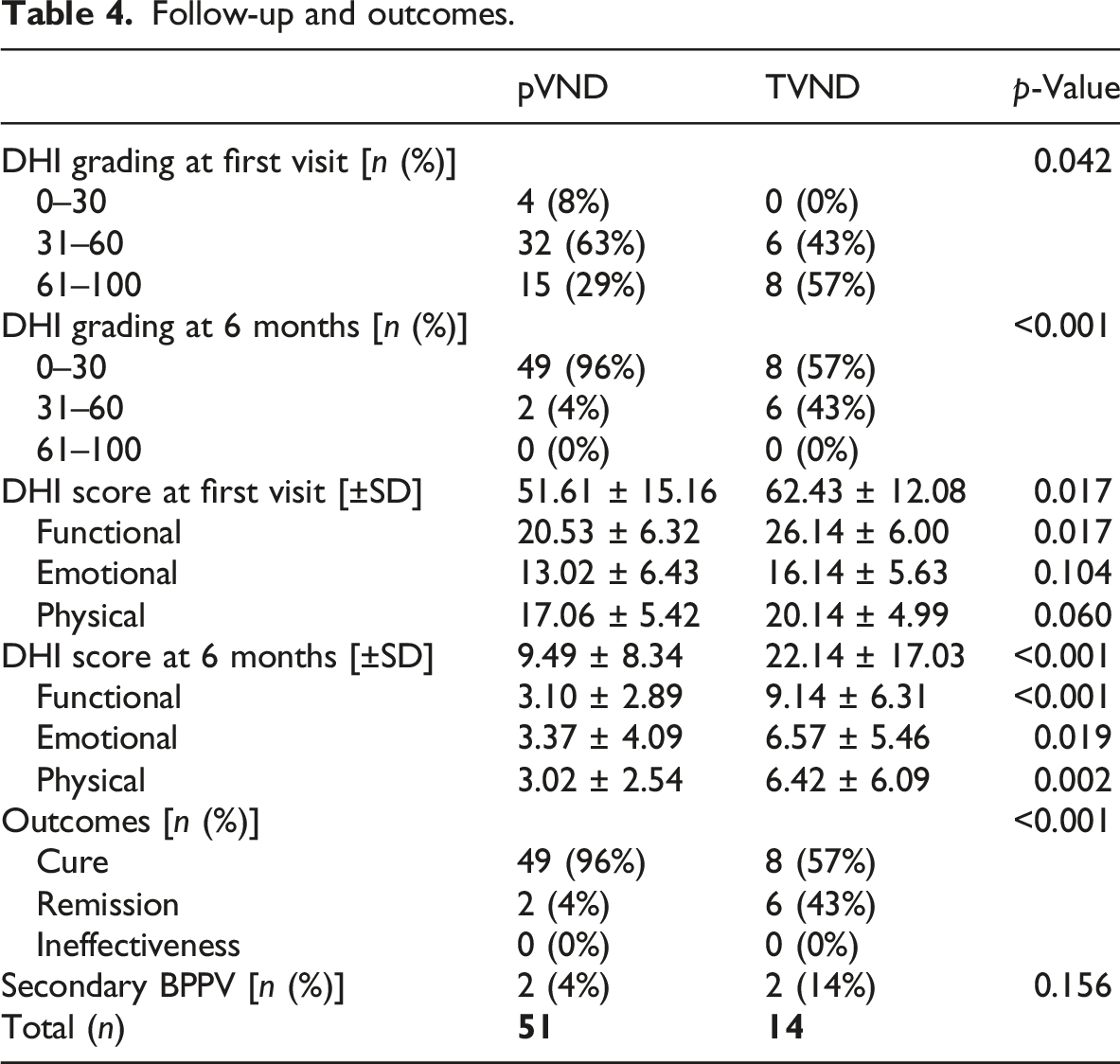

Box-and-whisker plot showing total DHI score by the tVND and pVND groups. The pVND group showed significantly lower scores than the tVND group at first visit (p = 0.012) and at 6 months (p < 0.001).
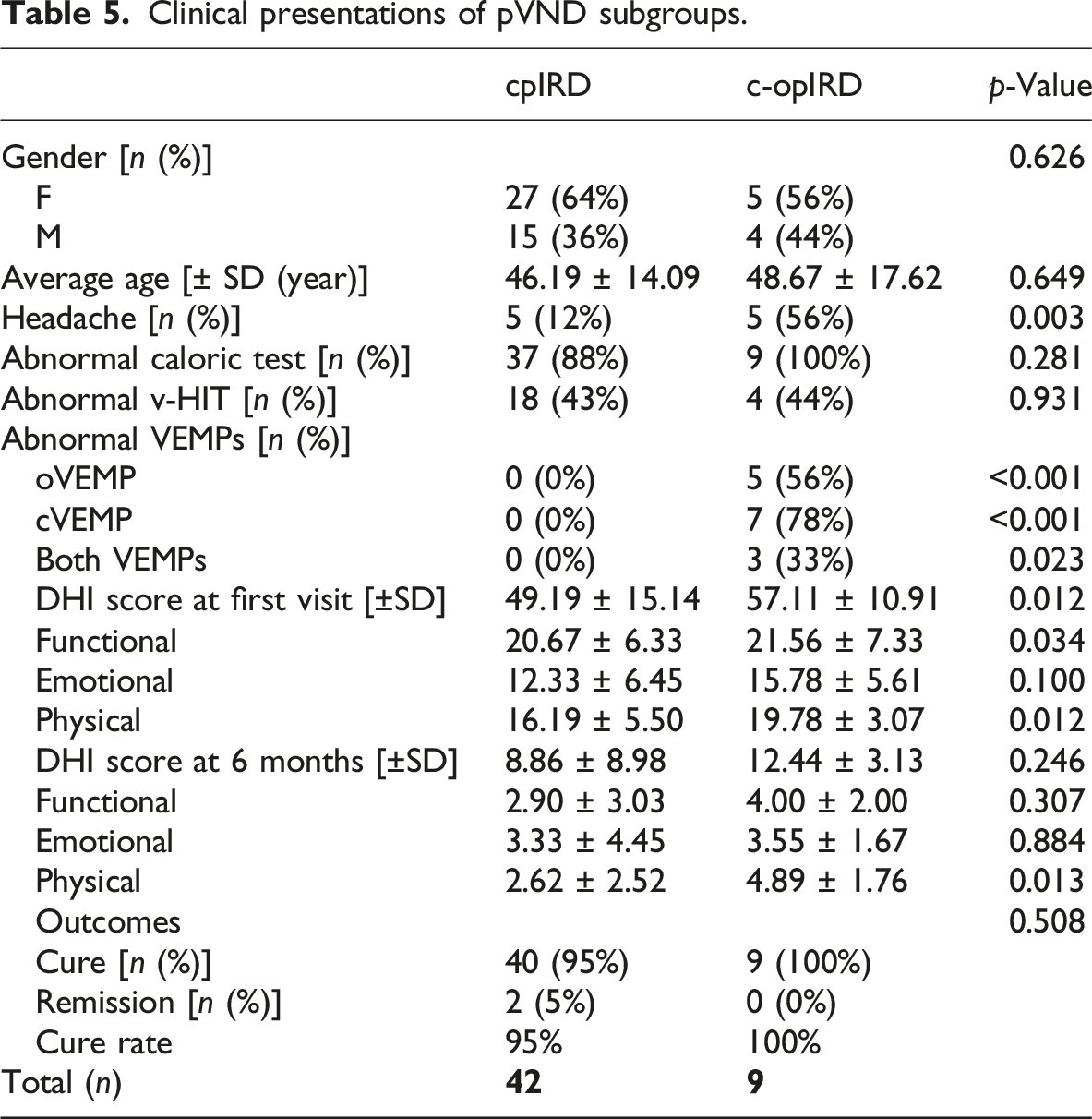
Figure 4 illustrates the distribution of the subgroups based on the affected vestibular receptors. There were 42 cases of cpVND, 9 c-opVND in the pVND group, and 13 cases of stVND, and 1 itVND in the tVND group. The number of tVND patients was too small to compare the data of subgroups. Table 5 summarizes the clinical characteristics of pVND patients by subgroups. There were no significant demographic differences between the two subgroups of pVND. In terms of symptoms, the rate of patients with headache in cpVND subgroup was significantly lower than in the c-opVND subgroup (p = 0.003), while there were no significant differences in other vestibular-related symptoms between the two subgroups (p > 0.05). In terms of results of vestibular function tests, there were no significant differences in the abnormal rate of caloric test and vHIT between the two subgroups (p > 0.001); the abnormal rates of oVEMP and cVEMP in the cpVND subgroup were significantly lower than in the c-opVND subgroup (p < 0.001). At the first visit, cpVND subgroup showed lower DHI score than c-opVND subgroup, while there were no significant differences in DHI score after the 6-month follow-up and outcomes between the two subgroups (p > 0.05). Histogram showing the distribution of the subgroups. cpVND was more common than c-opVND, and stVND was more common than itVND. Clinical presentations of pVND subgroups.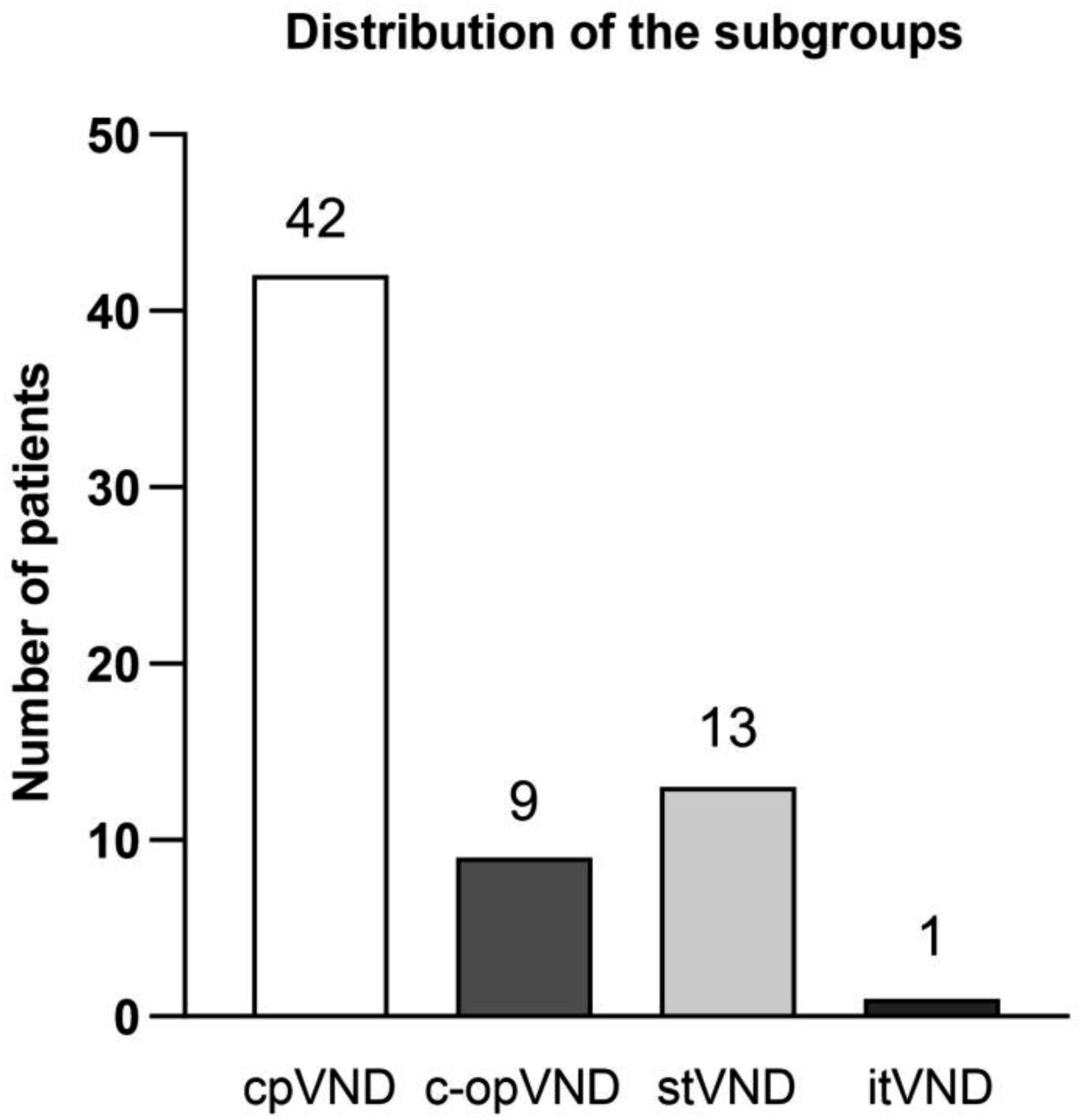
Discussion
In previous clinical work, there was no unified and clear diagnostic criterion for VN, which was ambiguously diagnosed based on persistent vertigo and dysfunction of unilateral lateral canal shown by caloric test. 7 With advancements in vestibular function test techniques and improvements in vestibular medical theory, v-HIT was used to assess the high-frequency VOR function of all three pairs of semicircular canals, and VEMPs to assess the utricle and saccule, providing complementary methods for evaluating the function of vertical canals and otolith organs. 8
The AUVP/VN diagnostic criteria published by the Barany Society proposed AUVP as a synonym for VN. The term AUVP was recommended, especially in the absence of evidence of vestibular nerve involvement in viral infection. 3 This perspective aligned with the view that the disease manifests as “vestibulopathy” rather than “neuritis.”
The criterion refers to the classification of superior, inferior, and total vestibular neuritis, which is the way to locate the lesion using v-HIT and VEMPs.2,13–15 However, there is still room for improvement. As AUVP is suggested as a synonym for VN, classification should get close to the concept of vestibulopathy. Perhaps the results of vestibular tests can be used as a basis for classification. Thus, it is necessary to study whether there are differences in the clinical presentations as well as prognosis among patients with different distribution patterns of vestibular receptor dysfunction.
For example, in this study, 24 cpVND cases showed only abnormal caloric test results, and 13 stVND cases showed abnormal results in caloric test, anterior canal, lateral canal VOR gain and oVEMP. However, all these 37 cases were appropriate for superior vestibular neuritis. Due to the varying range of vestibular receptors affected, their clinical presentations may vary greatly. The same logic applies to inferior and total vestibular neuritis. In this study, as an attempt, patients were divided into pVND and tVND groups.
Patients in both groups met the diagnostic criteria for a certain category of AUVP, not only showing similarities in case characteristics but also significant differences. All 14 patients in the tVND group met the AUVP criteria, while in the pVND group, 36 met the AUVP criteria and 15 eAUVP. According to the DHI score, the tVND group suffered more severe vertigo than the pVND group at the first visit. The incidence of balance disorders in the tVND group was significantly higher than in the pVND group. However, both groups showed no statistically significant differences in dizziness, gastrointestinal symptoms, and other related symptoms, demonstrating similarities except major symptoms and vestibular function test results. Although some patients showed headache, tinnitus, photophobia, and phonophobia, similar to vestibular migraine (VM), no persistent vertigo attack was found again during the 6-month follow-up. According to the VM diagnosis requirement of recurrent vestibular symptoms, it is more appropriate to consider these patients as AUVP rather than the first attack of VM. 16
After a 6 months follow-up, the cure rate of the tVND group was significantly lower than that of the pVND group (p < 0.001). Although no more vertigo episodes occurred, six tVND patients and two pVND patients remained with dizziness or balance disorder, with over a 31 DHI score (p < 0.001). This suggests that the establishment of vestibular compensation is more difficult in tVND group. Two patients in each group were proved to have secondary BPPV. Peripheral vestibulopathy might lead to utricular macula lesion resulted in detachment of otoconia. 17 Results above showed worse baseline status and outcomes of patients in tVND group. The classification method of the subgroups in this study also retained more detailed localization information of pVND and tVND.
pVND subgroups
Based on the affected peripheral vestibular receptors, patients in the pVND group were classified into cpVND and c-opVND subgroups, showing strong similarities in symptoms and signs. Regarding results of vestibular function tests, there were significant differences in abnormal rates in oVEMP and cVEMP, which were obviously related to the method of classification. DHI score at the first visit in the cpVND was lower than in the c-opVND subgroup, but DHI score at 6 months and cure rate showed no significant difference. However, it should be noted that the number of c-opVND cases in this study was limited. Thus, further research is needed to explore the case characteristics of each subgroup. Our team has been committed to collecting patients with peripheral unilateral vestibular dysfunction no matter the diagnosis, in order to explore the difference between pVND subgroups and various causes. For the same reason, it is difficult to compare 1 itVND and 13 stVND patients. Nonetheless, patients in stVND group accounted for the vast majority, which is similar to the results of previous studies on inferior vestibular neuritis.1,14,15
VEMPs and acute vertigo
VEMPs can serve as an auxiliary examination for AUVP. Abnormal oVEMP suggests utricle dysfunction, associated with superior vestibular neuritis, while abnormal cVEMP suggests saccule dysfunction and inferior vestibular neuritis. 13
VEMP uses 500 Hz non-physiological acoustic stimuli and gives us just a normal/abnormal result. Although these factors may lead to the presence of some false negative results, clear abnormal VEMP in patients with normal pure tone audiometry do provides evidence of impaired otolith function.
AUVP in evolution
Among 15 patients with eAUVP, 3 patients in the cpVND subgroup developed definite AUVP during the course and 12 patients did not persist for 24 hours (10 cpVND subgroup; 2 c-opVND subgroup). These 15 patients had remission of vertigo after treatment and had no further episodes during 6-month follow-up. The duration of subjective vertigo did not exceed 24 hours. This may be due to the early medical treatment, including promethazine and dexamethasone. However, vestibular-related dizziness, nystagmus, or balance disorder lasted for more than 24 hours, and these patients did not have a recurrence of vertigo during the 6-month follow-up. Referring to 3.4.1 Notes 5 and 6 of the AUVP criteria, we believed that it was more appropriate to consider these patients as AUVP, 2 but not the first attack of VM. In view of this result, it is appropriate to diagnose such patients as eAUVP and carry out intervention as early as possible.
Etiology
Considering that a temporary decrease in immunity is critical for the reactivation of latent neurotropic viruses, it is important to investigate significant events preceding the recent onset of vertigo.18,19 Out of the total cases, seven had pathological and psychological factors that could cause decreased immunity, with five in the tVND group and two in the pVND group. Statistical analysis revealed a significantly higher rate in the tVND group (p < 0.001). This result suggests that previous studies on the HSV-VN relationship might be more closely related to the characteristics of patients in the tVND group, implying an etiological difference between the two groups. However, the small number of tVND patients in this study necessitates further investigation to confirm any etiological differences between the two groups.
Conclusion
Overall, in our opinion, the term AUVP instead of VN is appropriate, and the concept of vestibulopathy fits the characteristics better. On this basis, the possibility of using VEMP as an auxiliary test for AUVP diagnosis can be considered, as well as the improvement of location-based classification, to fit the conceptual development of AUVP from neuritis to vestibulopathy.
Statements and declarations
Footnotes
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.