
Abstract
Since the diagnostic criteria of benign paroxysmal positional vertigo (BPPV) were published in 2015 by the Bárány Society, many new ideas and observations have been introduced concerning the diagnostic methods, classification and related theories of pathomechanisms of this most frequent vestibular disease. The aim of the authors was to review new diagnostic methods, classification, hypothetical pathomechanisms of the recently introduced BPPV variants. To look for answers to the “Questions for the Future” published in the Consensus Document (2015) of the Committee for Classification of Vestibular Disorders of the Bárány Society, the authors reviewed the publications listed in PUBMED since 2015 on “diagnosis,” “classification,” “pathomechanism,” of BPPV in the light of their own studies. The questions were:
1. The possible role of loose otoconia within the short arm of the semicircular canals.
2. Coexistence of canalithiasis and cupulolithiasis.
3. Mechanism of “pseudospontaneous” nystagmus and the theory of “canalith jam”.
4. Mechanism of persistent geotropic direction-changing positional nystagmus and the theory of light cupula.
5. Anterior canalithiasis and the posterior cupulolithiasis.
New research results contribute to our understanding of previously unclassified symptoms and examination results. As a conclusion it can be stated that the newly defined entities are important for topodiagnosis and successful treatments by physiotherapy.
Keywords
Introduction
In 2015, the Committee for Classification of Vestibular Disorders of the Bárány Society formulated the diagnostic criteria for benign paroxysmal positional vertigo (BPPV). 1 While the classification of BPPV in those criteria reflected up-to-date knowledge on the pathomechanisms of BPPV at that time, the authors also anticipated that growing understanding of the disease will lead to further developments. 1
Besides presenting a clear scientific framework on the diagnosis of BPPV in their Consensus Document, the authors also summarized the questions to be solved in the future. These concerned: (1) The possible role of loose otoconia within the short arm of the semicircular canals (on the utricular side of the cupula) (2) The possible coexistence of canalithiasis and cupulolithiasis (3) The possible mechanism of “pseudospontaneous” nystagmus in BPPV and the theory of “canalith jam” (4) The mechanism of persistent geotropic direction-changing positional nystagmus in the supine lateral head positions in the absence of central neurologic signs and the theory of light cupula (5) Under the heading of “controversial and emerging syndromes,” they discussed the anterior canalithiasis, the posterior cupulolithiasis (to be examined using the half Dix–Hallpike maneuver, performed with the head turned 45o toward the side to be tested and resting slightly raised from supine; about 30o in flexion).
Indeed, since then many new publications have been published on these questions and about BPPV in general, its pathomechanisms, prevalence, diagnosis, and therapy.
The aims of the current study are: (1) To review clinically relevant new publications listed in PUBMED since 2015 on the above questions. (2) To review new evidence on the pathomechanism of BPPV gained from three-dimensional inner ear reconstructions and from results with different therapeutic maneuvers
‘A priori’ principles
When considering BPPV, one should keep in mind that, when dislodged from the utricular macula, freely moving otoconia may migrate into any semicircular canal (SCC) or be attached to the cupula of any SCC on either utricular or canal side, thereby causing canalithiasis and/or cupulolithiasis of the individual SCC. Additionally, BPPV can be caused by either light or heavy cupula, possibly due to metabolic causes.2–4 Also, when theorizing evoked nystagmus in BPPV variants, it is first necessary to consider the location of the debris in the starting position, before examination, which is sitting (in case of vertical canal BPPV elicited by Dix–Hallpike position) or supine position before turning the head sideways (in case of horizontal canal BPPV). In our framework, debris should always be in the most inferior part of the fluid compartment in the starting position (the utriculus and the SCCs); then, in the provocative position it sinks into the most inferior part of the compartment than has been changed from the previous dependent position by the positioning maneuver. Therefore, the debris may be in the vestibule, or the short arm or long arm of the SCC, and be attached to the cupulae. Free moving debris should cause a stronger crescendo–decrescendo pattern of nystagmus (which abates when the debris reaches the most inferior portion of the fluid compartment); debris attached to the cupula or light cupula should cause a less strong, more persistent nystagmus pattern.
Hypothetical classification of peripheral positional nystagmus according the patterns of induced nystagmus during Dix–Hallpike maneuver (carried out from sitting) or supine head roll test (carried out from supine position)(5). Accepted classical BPPV variants printed bold.
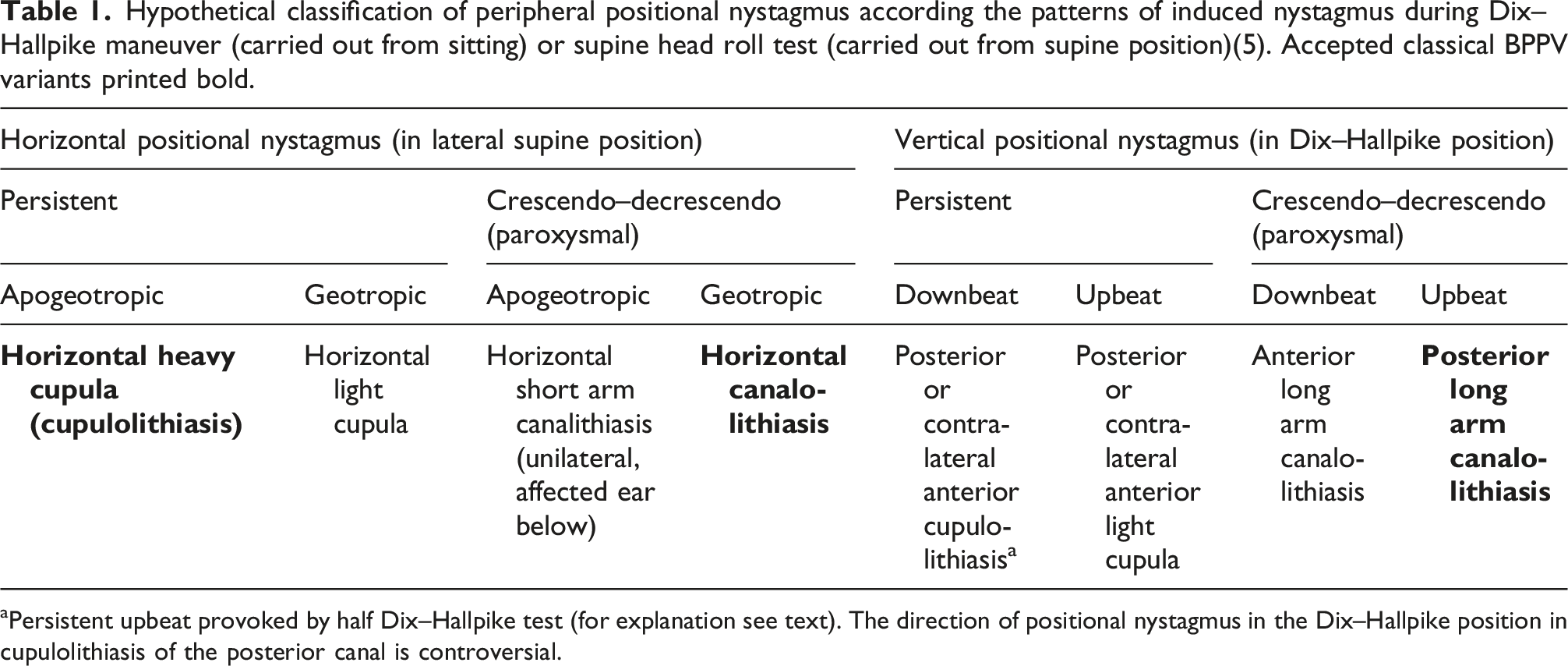
aPersistent upbeat provoked by half Dix–Hallpike test (for explanation see text). The direction of positional nystagmus in the Dix–Hallpike position in cupulolithiasis of the posterior canal is controversial.
Classification of peripheral positional nystagmus according to the involved canal and plausible mechanisms (5). Accepted classical BPPV variants printed bold. The resulting nystagmus types listed are evoked by Dix–Hallpike maneuver (carried out from sitting) or lateral supine positions (carried out from supine position).
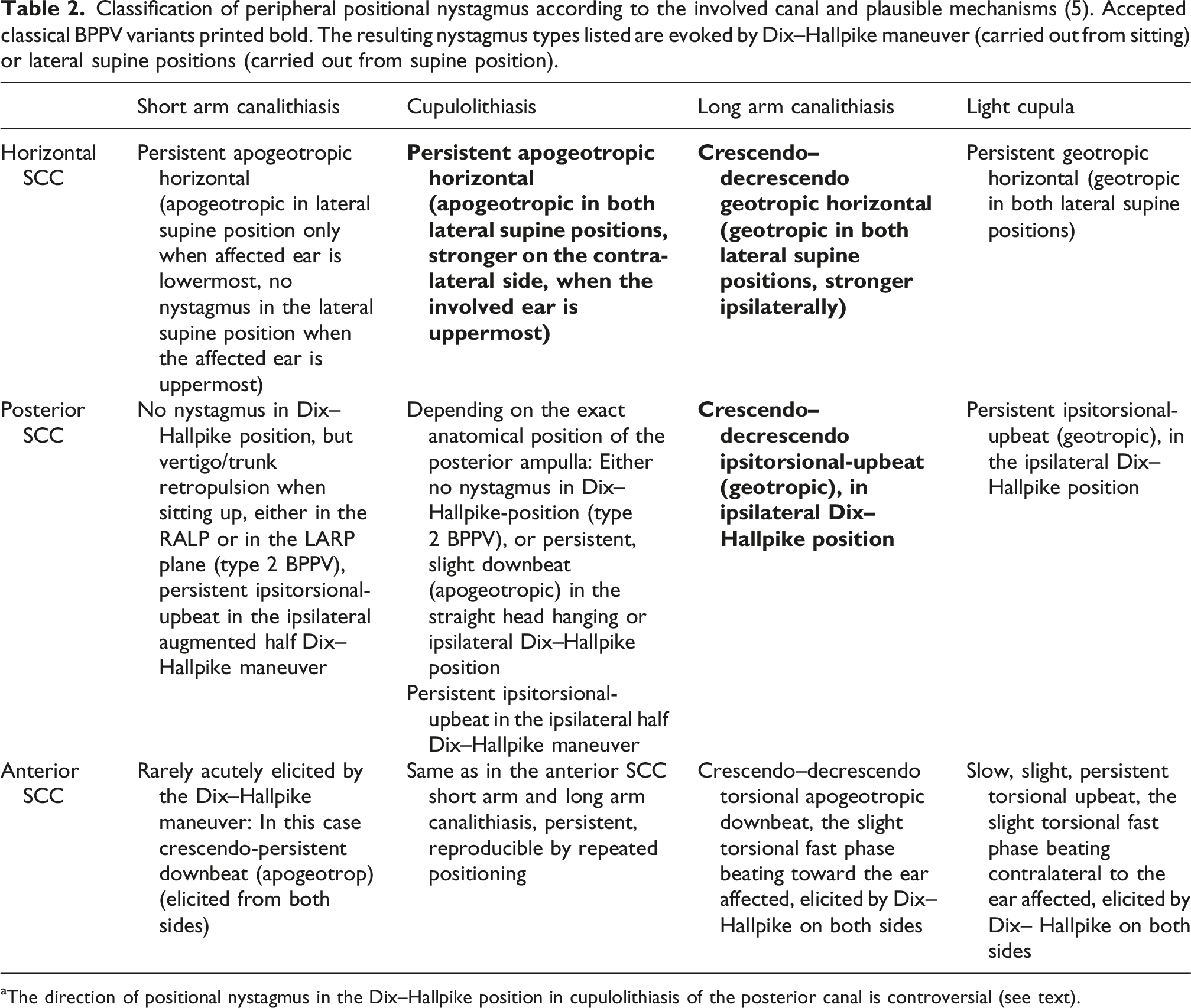
aThe direction of positional nystagmus in the Dix–Hallpike position in cupulolithiasis of the posterior canal is controversial (see text).
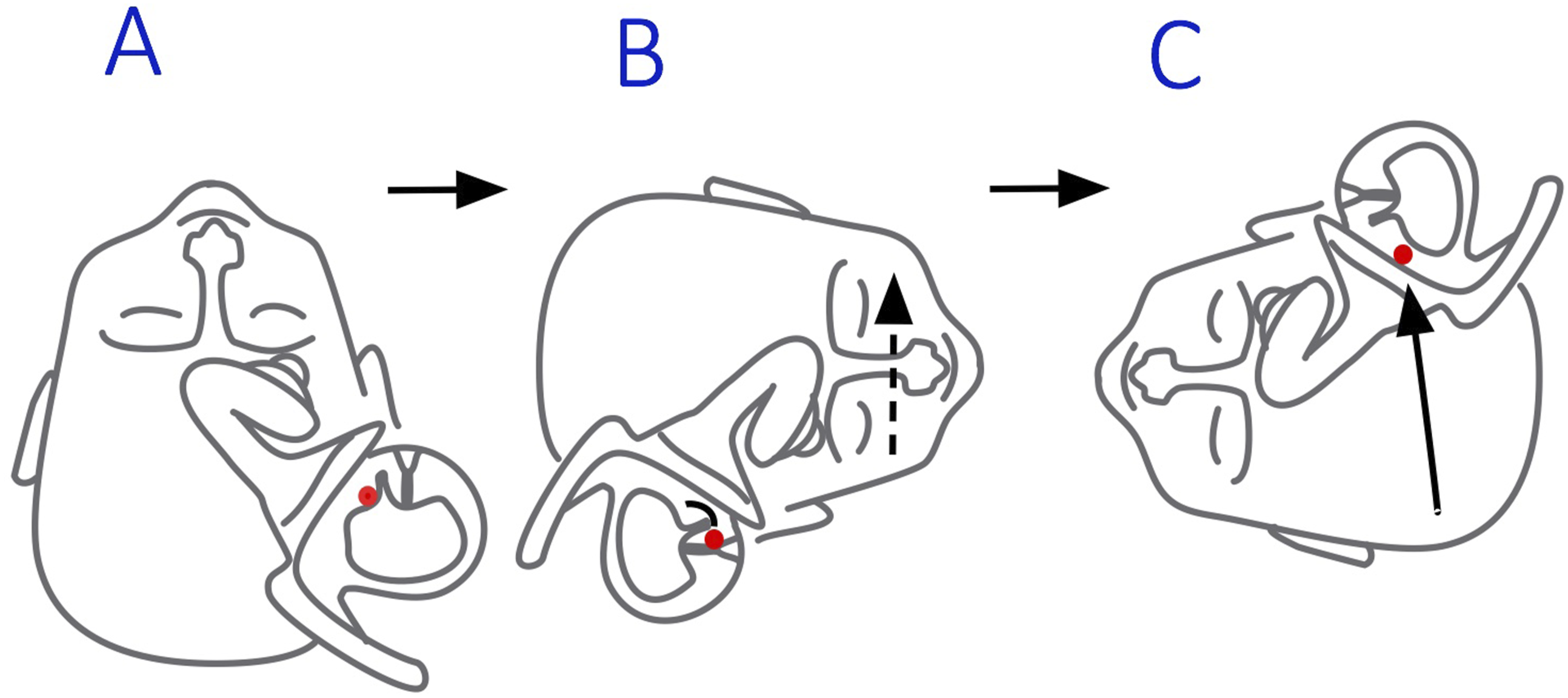
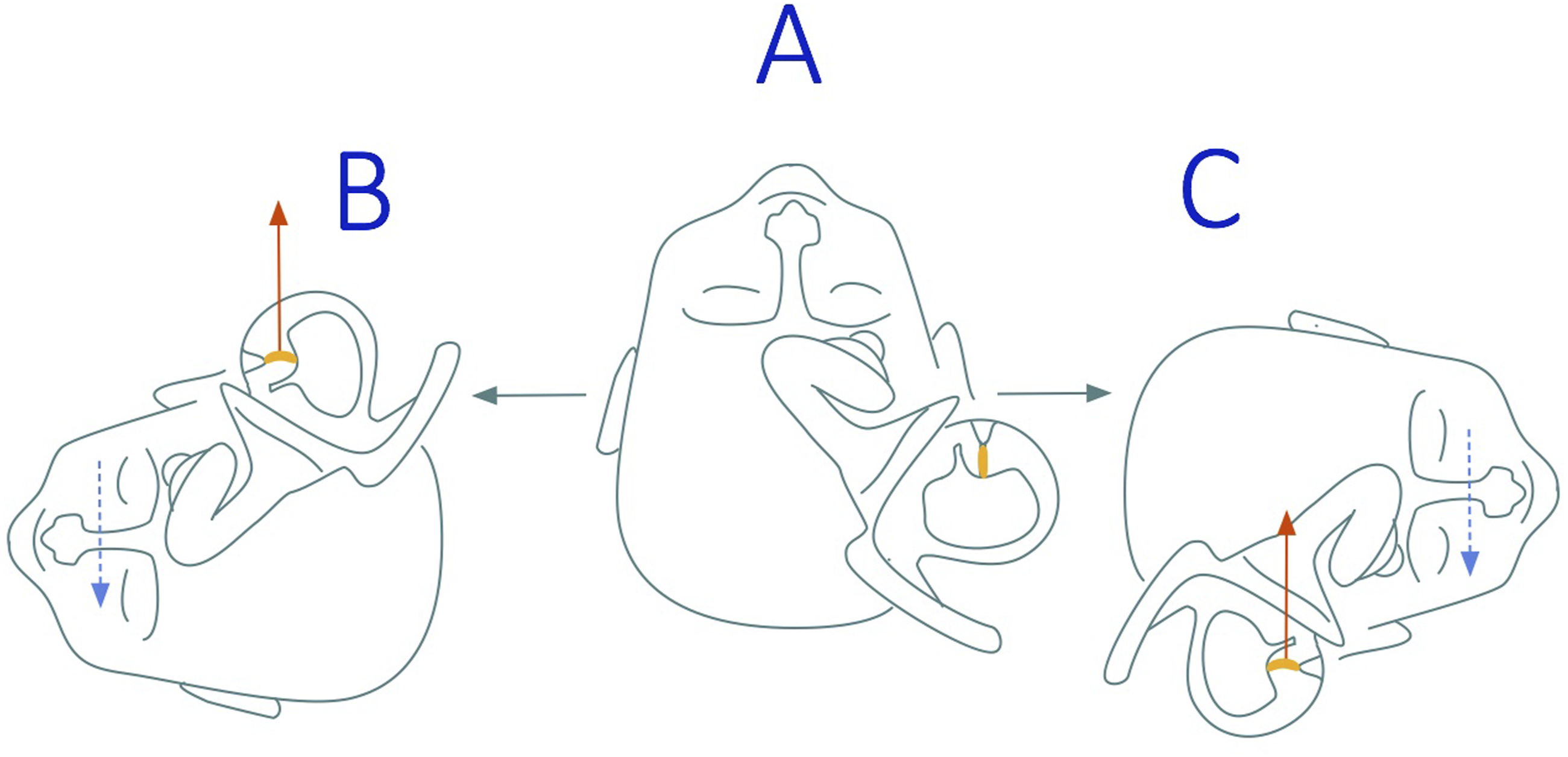
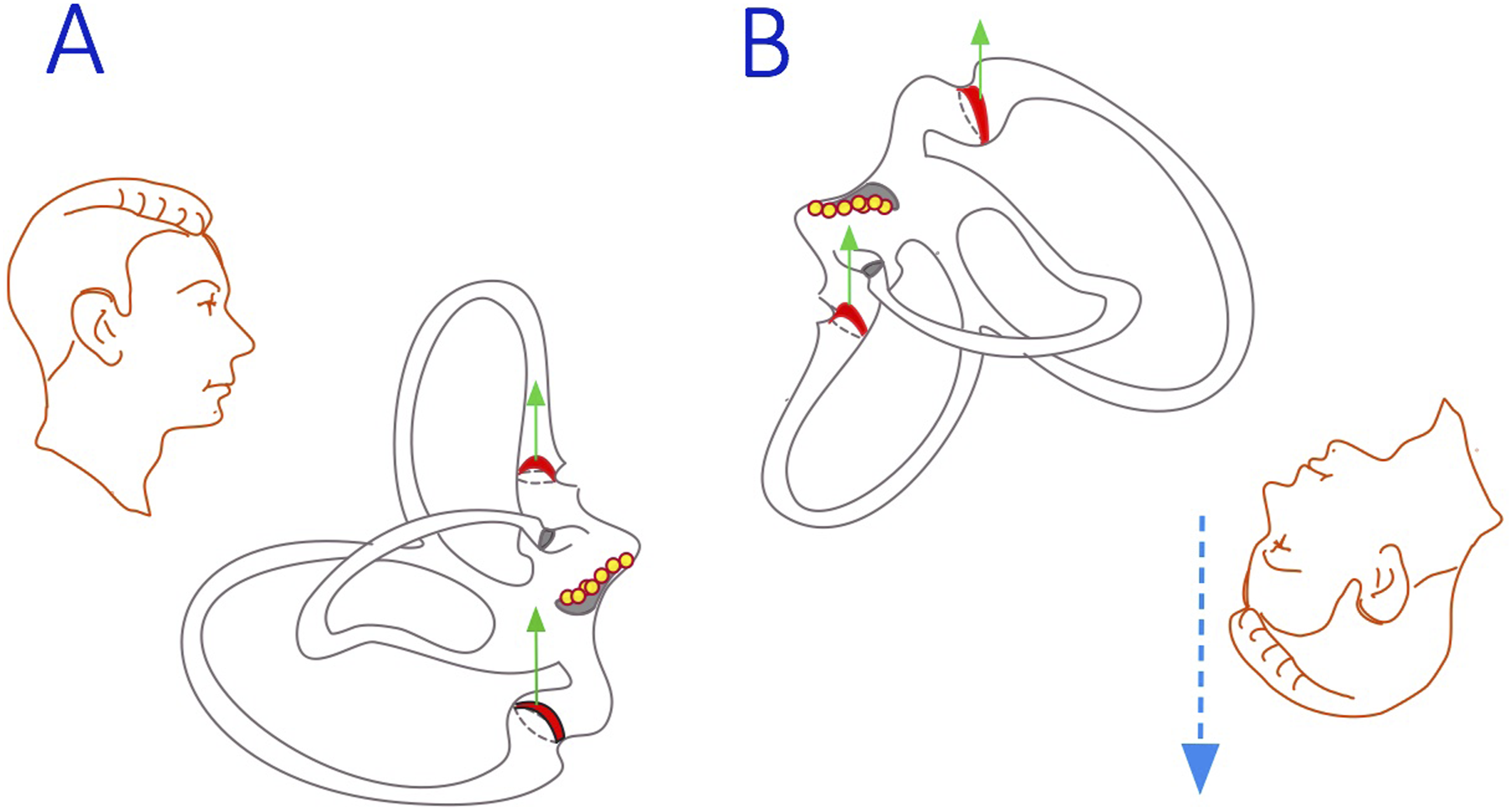
Next, we review research performed since 2015 on the controversial topics introduced by the Committee of the Bárány Society (see also Introduction) (Figures 1–4). Principle of the half Dix-Hallpike test (a) In posterior short arm canalithiasis or cupulolithiasis in the conventional right Dix-Hallpike position, the axis of the posterior canal cupula is aligned with the earth vertical and nystagmus may not be elicited by the positioning; (b) In the half Dix-Hallpike position, the cupular plane of the posterior semicircular canal is oriented perpendicular to the direction of gravity (arrow), thereby maximally deflected by the gravitational force inducing a persistent upbeat and ipsitorsional beating nystagmus with no or a minimal latency. Hypothetical mechanism of the horizontal short arm canalithiasis ‘A’: in supine position otoconial debris in the right utricle; ‘B’: in right lateral position the debris falls onto the right horizontal cupula, causing a persistent horizontal apogeotropic nystagmus (dashed arrow); ‘C’: in left lateral position the debris (arrow) falls out of the short arm into the utricle without a nystagmus. Hypothetical mechanism of the horizontal light cupula (arrow: buoyancy force) Hypothetical mechanism of the vertical light cupulae.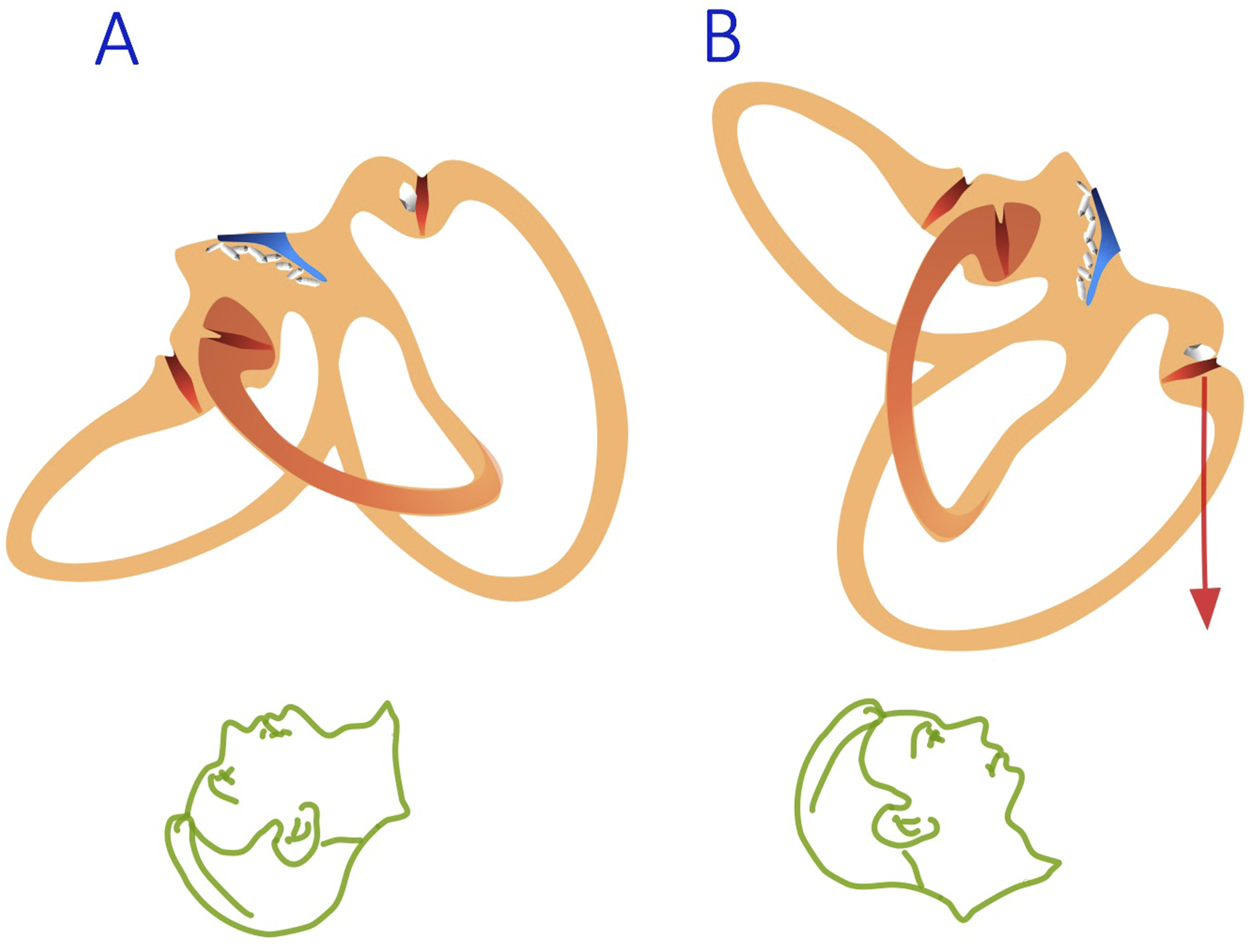
Results of literature search
The possible role of loose otoconia within the short arm of the semicircular canals (on the utricular side of the cupula)
In 1992, Epley published his observations and suggested a reposition procedure
9
for the most frequent variation of BPPV, the posterior canalithiasis. Until then there existed several hypotheses as to the exact mechanisms of positional nystagmus, but the success of this maneuver helped to develop a universally accepted theory. A few years later, based on anatomic considerations, Buckingham published his hypothesis on the fate of the otoconial debris during and after repositioning
10
and Oas followed with similar observations.
11
Buki et al. applied these principles to explain sitting up vertigo and positional vertigo without provoking nystagmus by short arm canalithiasis and/or posterior cupulolithiasis.
12
By now other authors also use this theoretical framework in discussions concerning subjective/atypical BPPV.4,13–16 Some of these authors suggested the “augmented half Dix–Hallpike maneuver” which is performed with the head turned 45◦ toward the side to be tested and slowly raised until it is flexed at 30 degrees after maintaining the conventional Dix-Hallpike position for a while.4,14 This procedure is regarded optimal because it shifts the otoconia from the lowermost dependent position onto the tip of the cupula and aligns the affected cupula perpendicular to gravity, thereby allowing a maximal deflection by the gravitational force. As was suggested by Epley,
17
this position is reportedly best suited to bring the affected cupula to be maximally deflected by the gravitational force. Harmat et al.
18
evaluated patients with BPPV that manifested as sitting-up vertigo. They used the definition of “type 2 BPPV” coined by Büki et al. for typical complaints of BPPV, no nystagmus in Dix-Hallpike positions but short vertigo spell while sitting up from one side, but not from the other.
12
In their outpatient ambulance out of all patients presenting with positional dizziness/vertigo, one-third met the criteria for type 2 BPPV; the remainder had a typical posterior or horizontal SCC involvement. The symptoms from type 2 BPPV were of longer duration and responded favorably to physical therapy (repetitive sit-ups). Upon repeat testing, 19 patients treated for posterior canalithiasis developed a weak persistent positional downbeat nystagmus in the Dix–Hallpike position, which the authors proposed as an evidence that the otoconia entered the short arm of the ipsilateral posterior SCC after having traveled through the utricle and attached themselves to the posterior cupula (posterior cupulolithiasis). In Dix–Hallpike position, in the case of a more inferiorly attached ampulla, the cupula may be pulled toward the utriculus by the weight of the otoconial debris, causing a slight, prolonged downbeat nystagmus (see also Figure 5(b)).
19
Hypothetical mechanism of peripheral downbeat nystagmus: posterior cupulolithiasis may cause either downbeat nystagmus or no nystagmus in Dix-Hallpike position depending on the angel of the positioning and on the anatomical position of the posterior ampulla which varies.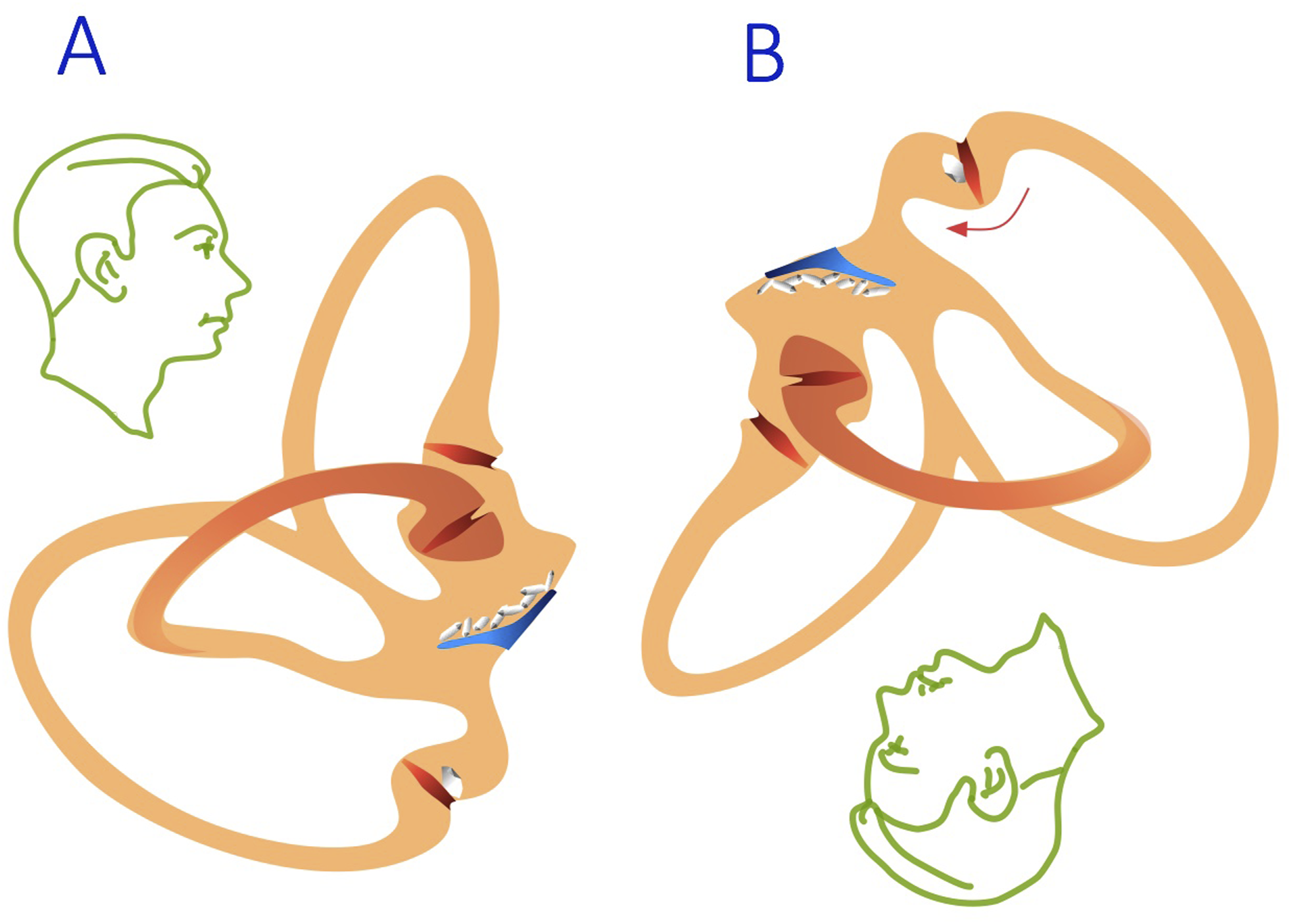
According to that study, type 2 BPPV appeared to be a treatable form of vertigo, more common than previously thought. In cases of posterior and horizontal canal canalithiasis, the otoconia that are repositioned into the utricle may subsequently cause canalithiasis in the short arm of the posterior canal, which can be diagnosed with the augmented half Dix-Hallpike maneuver. This observation supports the hypotheses proposed in previous studies. 20
Short arm canalithiasis of the horizontal SCC could cause a unilateral horizontal apogeotropic nystagmus probably only during supine head roll to the affected side. In this position, the otolithic debris would fall out of the utricle and rest onto the lowermost horizontal SCC cupula. 4 (Fig. 2).
The possible coexistence of canalithiasis and cupulolithiasis
Canalithiasis evokes usually a crescendo–decrescendo nystagmus with a short duration (mostly no longer than 30 s), in contrast to cupulolithiasis that goes with a longer, more persistent, and less intense nystagmus. 21 The examiner may suspect coexistence of canalithiasis and cupulolithiasis when the position of the debris is such that there is a spontaneous inversion of positional nystagmus without a positional change. In such cases, the initial nystagmus may be driven by canalith-induced endolymph flow, whereas subsequent cupular deflection may predominate, often leading to a reversal in nystagmus direction. 22 There are more data on this phenomenon concerning the horizontal SCC.22–25 However, alternative mechanisms, such as short-term central adaptation and endolymphatic reflux, have also been proposed to explain this phenomenon 23 . When the canalithiasis causes a nystagmus in the same direction as in the cupulolithiasis (such as in concomitant short arm and long arm canalithiasis of the posterior canal), it may be difficult to discern the two by the temporal dynamics of nystagmus alone.14,26 According to the pathophysiology and the location of otoconial debris, the posterior canal BPPV can be classified into four distinct types: (a) canalithiasis in the long arm, (b) canalithiasis in the short arm, (c) cupulolithiasis in the long arm, and (d) cupulolithiasis in the short arm. In clinical practice, various patterns of posterior canal BPPV may emerge as a result of different combinations of these subtypes. 26 This classification carries important implications for accurate diagnosis and tailored therapeutic strategies. The observation of ipsicanal conversion from cupulolithiasis to canalithiasis within the same canal and on the same side, in conjunction with application of the Dix–Hallpike, reversed Dix–Hallpike (in which the head is bent forward 90° from the upright position after being turned 45° toward the tested side), half Dix–Hallpike, inversed Half Dix–Hallpike (in which the head is rotated 180° away from the half Dix–Hallpike maneuver), and augmented half Dix–Hallpike maneuvers, can provide diagnostic clues for coexistence of canalithiasis and cupulolithiasis. 26 These cases may pose a difficulty for differential diagnosis because lesions of the vestibulocerebellum may also cause a direction-changing positional nystagmus.27–29 In general, it can be stated that, unless there is a typical upbeat-geotropic nystagmus in the Dix–Hallpike position which can be eliminated by Epley maneuver, it is not possible to differentiate between BPPV and central positional nystagmus only based on latency, horizontal direction of nystagmus, fatigability, and the crescendo–decrescendo pattern of nystagmus. 30 Central origin has to be assumed for purely upbeat, downbeat, and pure torsional nystagmus. In particular, positional downbeat nystagmus should alert the examiner to a possible central pathology although it may also be caused by posterior cupulolithiasis (Figure 5(b)).18,19,31 A weak spontaneous nystagmus may also be confused with a positional one if it is missed during examination in sitting posture because the spontaneous nystagmus may be amplified in Dix–Hallpike or lateral supine position. From a practical point of view, it is recommended to search for a central cause of positional vertigo (including brain MRI), especially if either the pattern of nystagmus does not fit one of the typical BPPV types and the treatments for BPPV is ineffective. 32
The possible mechanism of “pseudo-spontaneous” nystagmus in BPPV and the theory of “canalith jam”
We speak of pseudo-spontaneous nystagmus when spontaneous nystagmus, usually horizontal, is observed in sitting position, and is not explained by a sustained asymmetry of the vestibular discharge in the afferent vestibular pathways, but is in fact provoked by a gravity-dependent cupular deflection. It is dependent on head position, usually because of debris moving in the horizontal SCC or being attached to the horizontal SCC cupula, or by light cupula.
Nystagmus also can be caused by debris jamming a semicircular canal. This kind of spontaneous nystagmus persists independent of head position, usually caused by bigger otolithic particles obstructing and jamming the horizontal canal. Especially the latter can be misdiagnosed as genuine spontaneous nystagmus.
Position-dependent pseudo-spontaneous nystagmus
A typical scenario for a horizontal canal positional nystagmus which can be mistaken for spontaneous nystagmus involves leaning the patient’s head backward in sitting position. If the debris moves into the posterior part of the horizontal canal and thus inhibits the affected canal, then the evoked nystagmus would beat toward the healthy ear. In contrast, if it is attached to the horizontal cupula, then the nystagmus would beat to the involved side. 4 In this latter case, the nystagmus lasts longer, beat toward the upper ear while supine head turning (apogeotropic), and disappears when the head is turned toward the affected ear by 10–25o (“zero or null point”). 33 The mechanism of this position-dependent pseudo-spontaneous nystagmus seems to be clear, and its significance lies in its lateralizing value.
Position-independent pseudo-spontaneous nystagmus
Occasionally, positional tests or repositioning maneuvers lead to sudden appearance of strong spontaneous nystagmus that is unaffected by changes of head position. 17 In these cases, an ipsilateral canal paresis may be present. 34 These cases are rare and thought to be caused by the so called “canalith jam,” in which dislodged otoconia get hypothetically stuck in a narrow part of the canal or somewhere around the cupula, keeping the cupula slightly deviated. 17 Schubert et al. formulated the typical features of possible horizontal canalith jam based on two cases 35 : 1. Direction-fixed spontaneous nystagmus (seated or supine) with fixation removed. 2. Direction-fixed spontaneous nystagmus that does not change direction with positional testing 3. Velocity of the nystagmus and intensity of vertigo depend on head position. 4. Conversion of unidirectional nystagmus into geotropic nystagmus.
If the canalith jam is complete, it is not surprising that an ipsilateral canal paresis may coexists with these symptoms. 36 Schwarz et al. presented a case concerning the horizontal SCC in which, without a canal paresis, the horizontal pseudo-spontaneous nystagmus (which was observed in sitting position) could be modified by supine head roll (there was a bilateral apogeotropic horizontal nystagmus) but not by head positioning in the pitch plane. 37 Based on three dimensional reconstructions of the cupula, the authors suggested that this constellation of symptoms might be explained by the attachment of otoconia to the inferior part of horizontal cupula, at a location where it could cause gravity-dependent hair cell deviation in a sitting position.
Bronstein et al. described two cases in which a hypothetical transient canalith jam could be induced by vigorous head shaking (head-jolting); one of them showed a filling defect in the posterior limb of the left horizontal SCC on MRI that appeared to move with head shaking. 38 In this case, the symptoms ceased immediately after surgical plugging of the horizontal SCC. In the discussions concerning canalith jam, the size of the hypothetical particles responsible for the symptoms is a recurring topic because the size of human otoconia (between 1–30 µm 39 ) is in average less than one tenth of the narrowest part of the lateral canal ( in average 270 µm 40 ). This indicates that, for jamming the canal, a substantial bulk of otoconia has to be dislodged perhaps even with parts of the otolithic membrane. This may be indeed the case described by Kao et al. who found broken-off fragments of the utricular otolithic membrane with attached and detached otoconia during a surgery of the posterior SCC. 39 Apparently, this is not as frequent as the dislodgement of small quantities of otoconia, and therefore the canal jam is rarely documented.
The persistent geotropic direction-changing positional nystagmus and light cupula
Epley’s discovery of a simple otoconial repositioning maneuver 9 suddenly illuminated the possible mechanism of canalithiasis for the researchers because it was so effective and its effectiveness could be used as a proof for the hypothesis. Even before that, there already had been efforts to widen the horizon of positional vertigo syndromes; in 1985 McClure 41 and in 1989 Pagnini et al. described the involvement of the horizontal SCC. 42 The most conspicuous constellation was the horizontal long-arm canalithiasis diagnosed by crescendo–decrescendo type of geotropic nystagmus in both supine lateral positions (left and right); the evoked nystagmus was more intense when the pathological ear is lowermost. 43 With time, the resolution of the observations increased and patterns emerged with otoconia hypothetically located at different positions inside the horizontal SCC. First, the diagnosis of horizontal canal cupulolithiasis was born with an apogeotropic nystagmus that is more intense when the affected ear is uppermost. 44
Then, a less frequent variant was described with a persistent bilateral geotropic direction-changing positional nystagmus in the supine lateral head positions in the absence of central neurologic signs. 45 Later other authors also verified these initial findings. 46 To study the hypothesis that this phenomenon could be caused by a light cupula of the horizontal SCC, this group adopted the model of positional alcohol nystagmus (PAN). Soon after ingestion (PAN1), alcohol reaches the cupular matrix even before it saturates the endolymph. Therefore, the density gradient between the cupula and endolymph transforms the SCCs into gravity-sensitive receptors. This is because alcohol has a lower density than the endolymph (“buoyancy hypothesis” 47 ). To simulate the light cupula phenomenon using PAN1, the authors required patients with a unilateral deafferentation of the vestibular organ 48 because alcohol would influence both sides. Vestibular dysfunctions were commonly found in caloric and utricular function tests and 40% of the patients suffered from migraine. 49 Based on the findings of model experiments and clinical observations, the authors concluded that the cause of this persistent geotropic nystagmus is most probably due to a light cupula phenomenon involving the horizontal SCC, perhaps caused by a reversible metabolic disturbance.
Later it was also found that during PAN1 the light cupula phenomenon can also be elicited in the vertical canals. 5 In this respect, the authors proposed the terminology of “peripheral positional vertigo and dizziness” (PPVD) to embrace the persistent types of positional vertigo and nystagmus. Although these mild, longer lasting variants come with less severe symptoms, however, they make the patients ill enough to see a doctor. They may wait longer until seeking help but are grateful for the effective physical therapy. 18
Under the heading of controversial and emerging syndromes, the authors of the Bárány Committee Consensus Document 1 discuss the anterior canalithiasis and posterior cupulolithiasis
As listed in our Table 2, when the debris is on the cupula in the anterior canal ampulla and it falls into the long arm during the Dix–Hallpike positioning, anterior canalithiasis should cause a crescendo–decrescendo torsional downbeat nystagmus with a slight torsional fast phase beating toward the affected ear. The nystagmus may be elicited by the Dix–Hallpike maneuver on either side. The direction of the positional nystagmus during Dix–Hallpike maneuver should be the same either when the debris is attached onto the anterior cupula and remains on it (in this case of anterior cupulolithiasis the nystagmus is more persistent) or when the debris floating out of the utricle falls onto the anterior cupula (short arm anterior canalithiasis): in these latter cases, a crescendo-persistent downbeat nystagmus ensues. Kim et al. discuss this entity in their paper on “less talked of variants of benign paroxysmal positional vertigo” and remark that it is rarely observed. 4
When discussing the posterior canal cupulolithiasis among the controversial and emerging entities, the consensus diagnostic criteria by the Barany Society suggest that it should be examined using the half Dix–Hallpike maneuver (performed with the head turned 45o toward the side to be tested and raised from supine about 30o). 1 Several authors indeed found this test useful; in hypothetical posterior cupulolithiasis, this maneuver elicits positional nystagmus, after a brief latency, beating upward and ipsitorsionally (the upper pole of the eyes beating to the affected ear).4,13 Other authors also suggested that posterior cupulolithiasis causes either downbeat nystagmus or no nystagmus in Dix–Hallpike position, only a short vertigo spell when elevated from the head-hanging position (“sitting-up vertigo”),12,13,18,50,51 depending on the anatomical position of the posterior ampulla, which varies. 52 In the literature, others had already published evidence of positional downbeat nystagmus in the absence of a central vestibular pathology. 53 Theoretically, spontaneous nystagmus should occur in the sitting position in posterior canal cupulolithiasis because the otoconia would exert a stimulatory ampullofugal gravitational vector on the cupula in this position.31,50 However, previous studies have described no spontaneous nystagmus in the sitting position in cases of posterior canal cupulolithiasis diagnosed with the half Dix-Hallpike maneuver. 31 This absence of spontaneous nystagmus can be explained by set-point adaptation that serves to stabilize vision in the neutral position.31,50,54 Recent studies reported that nystagmus may not be elicited even in the half Dix–Hallpike position in posterior canal cupulolithiasis, thus suggesting that set-point adaptation may also operate in head positions other than the neutral one. 55 The set-point adaptation is indeed powerful enough to cancel out the maximal deflection of the cupula caused by the gravitational force during the half Dix–Hallpike maneuver. 55 These findings imply that the half Dix–Hallpike maneuver alone may not be sufficient for diagnosing the cupulolithiasis of posterior canal.26,55 Thus, for secure diagnosis of posterior canal cupulolithiasis, additional maneuvers that would deflect the cupula in the ampullopetal direction, such as the reversed Dix–Hallpike maneuver and the inversed half Dix–Hallpike maneuver, should be performed. For a more refined diagnosis of cupulolithiasis, it is necessary to assess whether nystagmus disappears at the null point of each semicircular canal cupula. 56 The null point is defined as the head position where the cupula affected by cupulolithiasis is aligned with gravity, so in this position the positional nystagmus should cease.
Further studies, however, are required to determine and define the precise null point for each canal. According to Harmat et al. 18 cases with the symptoms of BPPV but without nystagmus are rather frequent. In this study, one-third of the patients met the criteria for type 2 BPPV; the remainder had typical posterior or horizontal SCC involvement. As discussed earlier under the point 1. Short arm canalithiasis, upon repetition of testing, 19 patients treated for posterior canalithiasis developed a small persistent positional downbeat nystagmus in the Dix–Hallpike position, which was interpreted by the authors as post-repositioning posterior cupulolithiasis (see also Figure 5(b)). The symptoms from type 2 BPPV were longer in duration yet responded favorably to physical therapy. The authors completed three-dimensional reconstructions of the posterior ampulla and cupular plane based on cadaver histological sections and suggested that the type 2 BPPV is caused by either short-arm canalithiasis or cupulolithiasis of the posterior SCC. The most important message of this publication was that although the average duration of symptoms was 2 months in type 2 BPPV, 86% of patients showed improvement of symptoms at the 1-week follow-up visit and 54% reported a complete resolution with home exercises that consisted of 10 Dix–Hallpike positions to the affected side 3 times a day.
In summary, the direction of positional nystagmus in the Dix–Hallpike position in cupulolithiasis of the posterior canal is yet controversial. The most important message is that positional downbeat nystagmus may be of central but also of peripheral origin. If it is elicited in Dix–Hallpike position as a post-repositioning nystagmus after a posterior canalithiasis then it is probably peripheral, because during the maneuver the otoconial debris falls through the utricle and may attach itself to the utricular surface of the posterior cupula. In other cases, a possible central pathology should be excluded. Further studies of post-repositioning nystagmus using video nystagmography also recording torsional components may help to refine the diagnostic criteria of the posterior cupulolithiasis.
Conclusions
As predicted by the five points of the Bárány Committee Consensus Document, indeed there have been new observations on the possible role of loose otoconia within the short arm of the semicircular canals (on the utricular side of the cupula), on coexistence of canalithiasis and cupulolithiasis, on the “pseudo-spontaneous” nystagmus (position dependent and independent) and the theory of “canalith jam,” on the persistent geotropic direction-changing positional nystagmus in the supine lateral head positions (horizontal light cupula), and on the anterior canalithiasis and posterior cupulolithiasis. In our interpretation, these new results are important concerning topodiagnosis in the absence of central neurological and vestibular signs or pathologies. Apart from acute and severe positional vertigo due to classic forms of BPPV such as posterior canal canalithiasis, these new entities are important because they may cause less conspicuous, but more protracted symptoms that may be successfully treated by physiotherapy.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of article: The author Bela Büki appreciates the contribution of NÖ Landesgesundheitsagentur, legal entity of University Hospitals in Lower Austria, for providing the organizational framework to conduct this research and also would like to acknowledge support by Open Access Publishing Fund of Karl Landsteiner University of Health Sciences, Krems, Austria. Ji-Soo Kim was supported by a Seoul National University Bundang Hospital Research Fund (No. 13-2016-0005).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.