
Abstract
Background
Vestibular disorders affect mobility, independence, and quality of life. Culturally adapted assessment tools are essential for accurate evaluation and effective treatment in diverse populations.
Objectives
To translate, culturally adapt, and evaluate the psychometric properties of the Vestibular Disorders Activities of Daily Living Scale (VADL) into European Spanish (VADL-ES).
Methods
The VADL was adapted following international cross-cultural guidelines. Psychometric testing included internal consistency (Cronbach’s α), test–retest reliability (ICC), content validity (CVI), convergent validity with the Dizziness Handicap Inventory (DHI), and discriminant validity (ROC analysis, Youden index). Floor/ceiling effects, standard error of measurement (SEM), minimal detectable change (MDC95), and structural validity (exploratory and confirmatory factor analysis) were also assessed.
Results
The VADL-ES showed excellent internal consistency (α = 0.978), test–retest reliability (ICC = 0.988), strong correlation with the DHI (ρ = 0.768), and high content validity (S-CVI = 0.93). ROC analysis yielded an AUC = 0.988 with 100% specificity. Factor analysis confirmed a three-factor structure explaining 72% of variance. No floor or ceiling effects were observed; MDC95 was 0.91.
Conclusions
The VADL-ES is a valid and reliable instrument for assessing functional limitations in Spanish-speaking patients with vestibular disorders, enabling standardized evaluation and longitudinal monitoring in clinical and research settings.
Keywords
Introduction
Vestibular disorders often cause symptoms such as vertigo, dizziness, and imbalance, which significantly hinder the performance of daily activities.1,2 These functional limitations translate into decreased autonomy and reduced quality of life. 3 Epidemiological data suggest that vertigo or dizziness affects approximately 20–30% of adults annually, with prevalence rising with age to affect up to 50% of those over 60 years old. 4 These conditions account for a high proportion of medical consultations, falls, and functional disability, especially in older adults.1,5
Vestibular dysfunction not only impairs balance and spatial orientation but also affects the individual’s ability to perform basic and instrumental activities of daily living, such as walking, cooking, bathing, or using public transportation. 6 This loss of independence may lead to major psychosocial consequences, including anticipatory anxiety, mobility restriction, social isolation, and depression. 2
To quantify disability and functional impact, several self-reported questionnaires have been developed. Among the most widely used are the Dizziness Handicap Inventory (DHI), 7 which evaluates perceived handicap due to dizziness, and the Activities-specific Balance Confidence (ABC) Scale, 8 which measures confidence in performing balance-related tasks. However, both instruments have limitations, as they do not explore in sufficient depth the specific daily activities affected by vestibular dysfunction, nor do they include important dimensions such as functional mobility or instrumental tasks. 9
To address these gaps, Cohen et al. developed the Vestibular Disorders Activities of Daily Living Scale (VADL), specifically designed to assess the impact of vestibular disorders on everyday activities. The VADL consists of 28 items grouped into three subscales (functional, ambulation, and instrumental), each rated on a 10-point scale from 1 (fully independent) to 10 (fully dependent). The original study reported high internal consistency (α ≥ 0.90) and strong test–retest reliability. 10
The VADL has since been translated, culturally adapted, and psychometrically validated in several international contexts. For example, Aratani et al. translated, adapted, and validated the VADL into Brazilian Portuguese, 11 Xu et al. conducted the translation, cultural adaptation, and validation into Chinese, 12 and Rao et al. into Kannada, a South Indian language. 13 Additionally, Mehrkian et al. validated the Persian version of the scale, 14 also demonstrating adequate reliability and validity. These international versions confirm the scale’s applicability and validity across diverse populations with vestibular dysfunction.
Despite these foreign versions, a Spanish-language adaptation of the VADL has not yet been developed. While several validated questionnaires in Spanish exist, the absence of a condition-specific scale aimed at evaluating functional performance in individuals with vestibular dysfunction limits diagnostic precision and therapeutic planning. 9 Therefore, it is essential to develop and validate a culturally adapted tool to assess daily activity limitations in this population.
We translated and culturally adapted the VADL into European Spanish and evaluated the psychometric properties of the resulting VADL-ES.
Materials and methods
Participants
This study was approved by an independent ethics committee and conducted in accordance with the Declaration of Helsinki. Between January 2024 and June 2025, a total of 226 individuals participated in the study.
Of these, 200 patients with a confirmed clinical diagnosis of vestibular disorder (Ménière’s disease, 15 vestibular migraine, 16 or benign paroxysmal positional vertigo 17 ), according to Bárány Society criteria and supported by objective vestibular testing, were recruited through purposive sampling 18 from patient associations, specialized clinics, and professional associations across Spain. The patient group comprised adults aged 18 to 75 years.
Additionally, a control group of 26 individuals without any history or symptoms of vestibular disorders, mostly relatives of patients and acquaintances of healthcare professionals, was included to assess the discriminative capacity of the VADL-ES.
All participants were fluent in Spanish and provided written informed consent prior to participation.
Inclusion and exclusion criteria
To ensure sample homogeneity, clinical relevance, and validity of the results, specific inclusion and exclusion criteria were established and consistently applied across all study phases.
(i) adults aged 18–75 years, Spanish nationality and residence in Spain; (ii) confirmed diagnosis of vestibular disorder established by an otolaryngologist or neurologist according to Bárány Society criteria; (iii) confirmation through objective vestibular testing (video Head Impulse Test, vestibular evoked myogenic potentials, caloric testing, and/or pure-tone audiometry); and (iv) ability to read, understand, and complete questionnaires in Spanish.
(i) adults aged 18–75 years, Spanish nationality and residence in Spain; (ii) absence of current or previous vestibular disorders, confirmed by clinical anamnesis; and (iii) ability to read, understand, and complete questionnaires in Spanish.
(i) multiple vestibular diagnoses or relevant neurological or psychiatric conditions that could interfere with functional performance or disability perception (e.g., epilepsy, Parkinson’s disease, psychotic disorders, and major depression); (ii) significant cognitive impairment; (iii) severe uncorrected visual deficits; (iv) inability to adequately read or understand Spanish.
(i) history of vestibular disorders or current vestibular symptoms; relevant neurological or psychiatric conditions; significant cognitive impairment or severe sensory deficits; (ii) inability to read or understand Spanish.
Sample size justification
Sample size was based on psychometric recommendations suggesting 5–10 participants per item for factor analysis, ensuring statistical stability and accurate estimates. Given that the VADL contains 28 items, the theoretical sample size ranged between 140 and 280.18–21 Additionally, samples exceeding 150 participants have been deemed adequate for evaluating reliability and validity in cross-cultural adaptations. Thus, a cohort of 200 patients was selected to meet methodological requirements and compensate for potential attrition.
During interviews, the principal investigator recorded any difficulties reported by participants and addressed them through strategies such as paraphrasing, illustrative examples, or direct inquiry. Semantic, idiomatic, and experiential equivalence were evaluated. According to methodological recommendations, if 20% or more of the participants (≥6 individuals) had difficulty with an item, it was to be revised.22,23
Measures
(a) Vestibular Disorders Activities of Daily Living Scale (VADL): The VADL is a 28-item self-report questionnaire assessing functional dependence on individuals with vestibular disorders. It includes three subscales: Functional, Ambulation, and Instrumental. Items are scored on a 10-point scale, where higher scores reflect greater disability. The scale has been validated in various cultural settings, demonstrating good reliability, internal consistency, and content validity. It is useful for both functional assessment and monitoring treatment outcomes.10–14 (b) Dizziness Handicap Inventory (DHI): The Spanish version of the DHI, used for convergent validity, comprises 25 items across functional, emotional, and physical domains. Total scores range from 0 to 100, with higher scores indicating greater perceived disability.
24
Translation and cross-cultural adaptation
The cross-cultural adaptation process followed the main steps proposed by Beaton et al., 22 including forward translation, synthesis, expert committee review, and pre-testing. The back-translation step, although recommended in standard cross-cultural adaptation guidelines, was not performed in this study and is therefore acknowledged as a methodological limitation.
The Spanish version of the VADL was developed following international guidelines for cross-cultural adaptation of patient-reported outcome measures. The process included four phases (Figure 1). Permission to use, translate, and adapt the original instrument, was obtained through the American Medical Association (License No. 6070660976043, issued and renewed on July 16, 2025). (a) Step 1: Independent forward translations. Two independent translations from English into Spanish were performed: one by a Spanish occupational therapist experienced in cross-cultural adaptations (TL1), and another by a professional bilingual translator without clinical training in vestibular disorders (TL2). Each translator rated item difficulty on a 0–10 scale (low: 0–3; moderate: 4–6; high: 7–10). (b) Step 2: Reconciliation and synthesis. The two versions were compared by both translators and a third researcher from the project team. Discrepancies were discussed, and a preliminary version (P-TL) was created based on linguistic clarity, conceptual accuracy, cultural appropriateness, and grammatical structure.22,23,25–27 (c) Step 3: Expert committee review. A multidisciplinary committee reviewed the original items, TL1, TL2, and the P-TL version. Items were rated as A (full semantic and conceptual equivalence), B (minor semantic modifications), or C (inadequate semantic equivalence). Disagreements were resolved by consensus (see Supplemental Table 1). The expert panel consisted of one otolaryngologist and five occupational therapists. Three of the therapists had clinical and academic experience in neurology and vestibular disorders, with prior involvement in the content validation of patient-reported outcome measures, one of whom also had expertise in cross-cultural adaptation and translation. All experts held doctoral degrees, except for the otolaryngologist and two occupational therapists, who held a Master’s degree in Health Sciences and were PhD students. Process of cross-cultural adaptation of the Vestibular Disorders Activities of Daily Living Scale (VADL) into Spanish. The process followed international guidelines and included independent forward translations, synthesis, expert committee review, and comprehensibility testing.
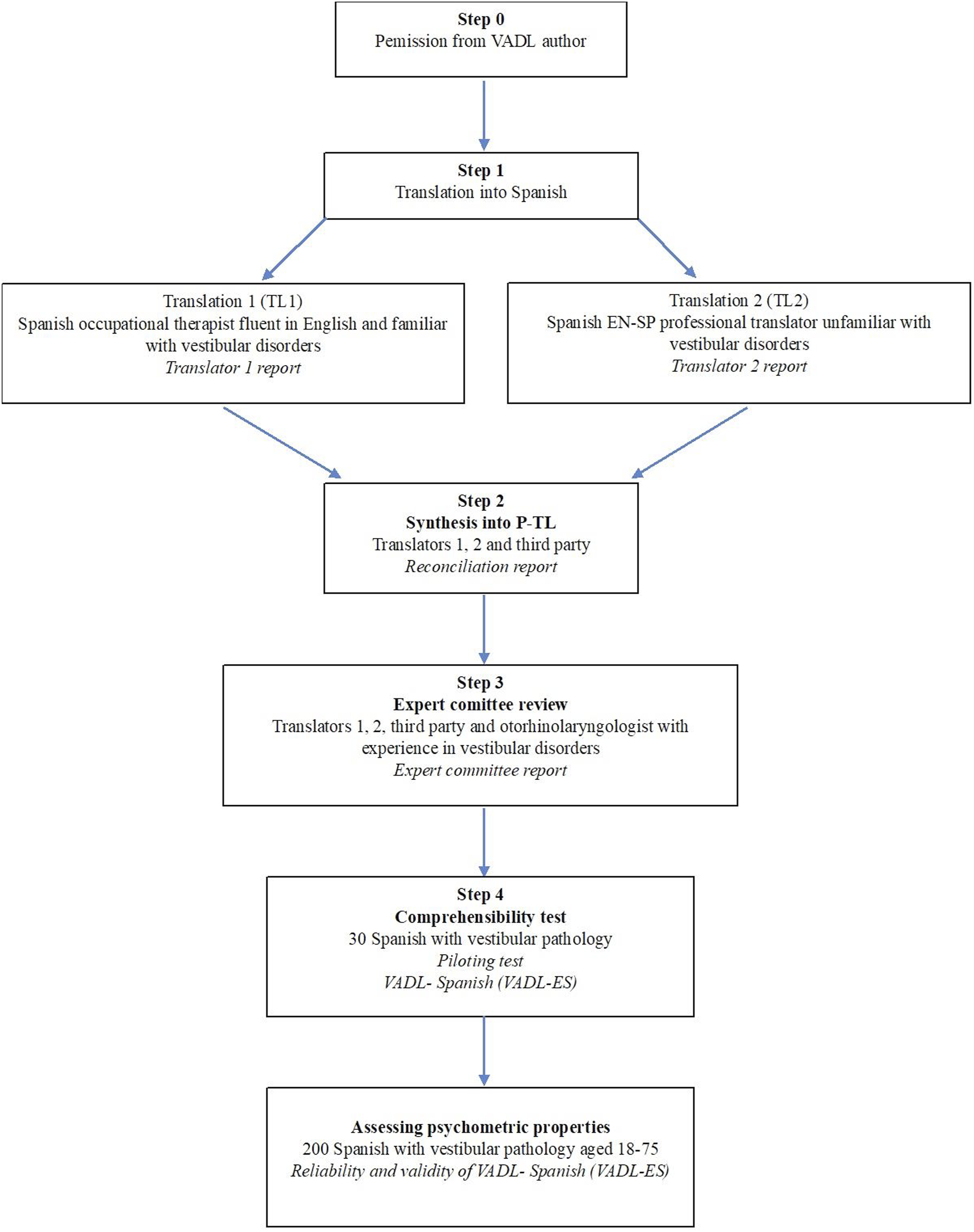
Translations were performed independently by translators with complementary profiles (one with clinical expertise and one with linguistic expertise). Subsequently, discrepancies between versions were addressed through a structured group discussion involving the translators and the expert committee. Consensus on the final version was reached based on predefined criteria of semantic, idiomatic, experiential, and conceptual equivalence. (d) Step 4: Comprehensibility testing. A pilot study was conducted with 30 individuals (18–65 years old) diagnosed with vestibular disorders using cognitive interviews. Participants were asked to read items aloud, comment on clarity, and provide related examples.22,23,25–27 No major issues were identified, and no items required revision. The final Spanish version (VADL-ES) is available in Supplemental File 1.
Statistical analysis
Participants with incomplete questionnaire data were excluded from the analyses (listwise deletion). Statistical analyses were conducted using IBM SPSS Statistics v28.0 and R software v4.3.1. Floor and ceiling effects were considered present when >15% of respondents achieved the lowest or highest possible score. 28 Internal consistency was assessed using Cronbach’s alpha, 29 and test–retest reliability using intraclass correlation coefficients (ICC, two-way mixed-effects model). 30 Content validity was evaluated using the content validity index (CVI). For structural validity, the sample was randomly split into two groups (n = 100 each) to perform independent exploratory factor analysis (EFA) and confirmatory factor analysis (CFA), minimizing overfitting and following psychometric best practices.31,32 EFA used maximum likelihood extraction with oblimin rotation, as recommended for continuous data and underlying latent constructs.32,33 Items with loadings ≥ 0.40 were retained unless theoretical relevance justified inclusion. 33 Sampling adequacy was verified using the Kaiser–Meyer–Olkin (KMO) index and Bartlett’s test of sphericity. 31 CFA used maximum likelihood estimation. Model fit was evaluated using SRMR (≤0.08) and CFI (≥0.97), with factor loadings ≥0.30 considered significant. 34 Convergent validity was assessed using correlations between VADL-ES and DHI scores.10,24 Discriminant validity was analyzed using receiver operating characteristic (ROC) curves, with optimal cut-off values identified via the Youden index.35–37 Finally, the standard error of measurement (SEM) was calculated from the baseline standard deviation and ICC, and the minimal detectable change at 95% confidence (MDC95) was derived from SEM. 38
Results
Participants
A total of 226 individuals participated in the study. Of these, 202 patients with vestibular disorders and 26 healthy controls were initially recruited. However, two patients were excluded due to missing sociodemographic data, resulting in a final sample of 200 patients included in the analyses.
A control group of 26 individuals without vestibular pathology was included for discriminant validity analyses.
Demographic and clinical characteristics of the study sample.
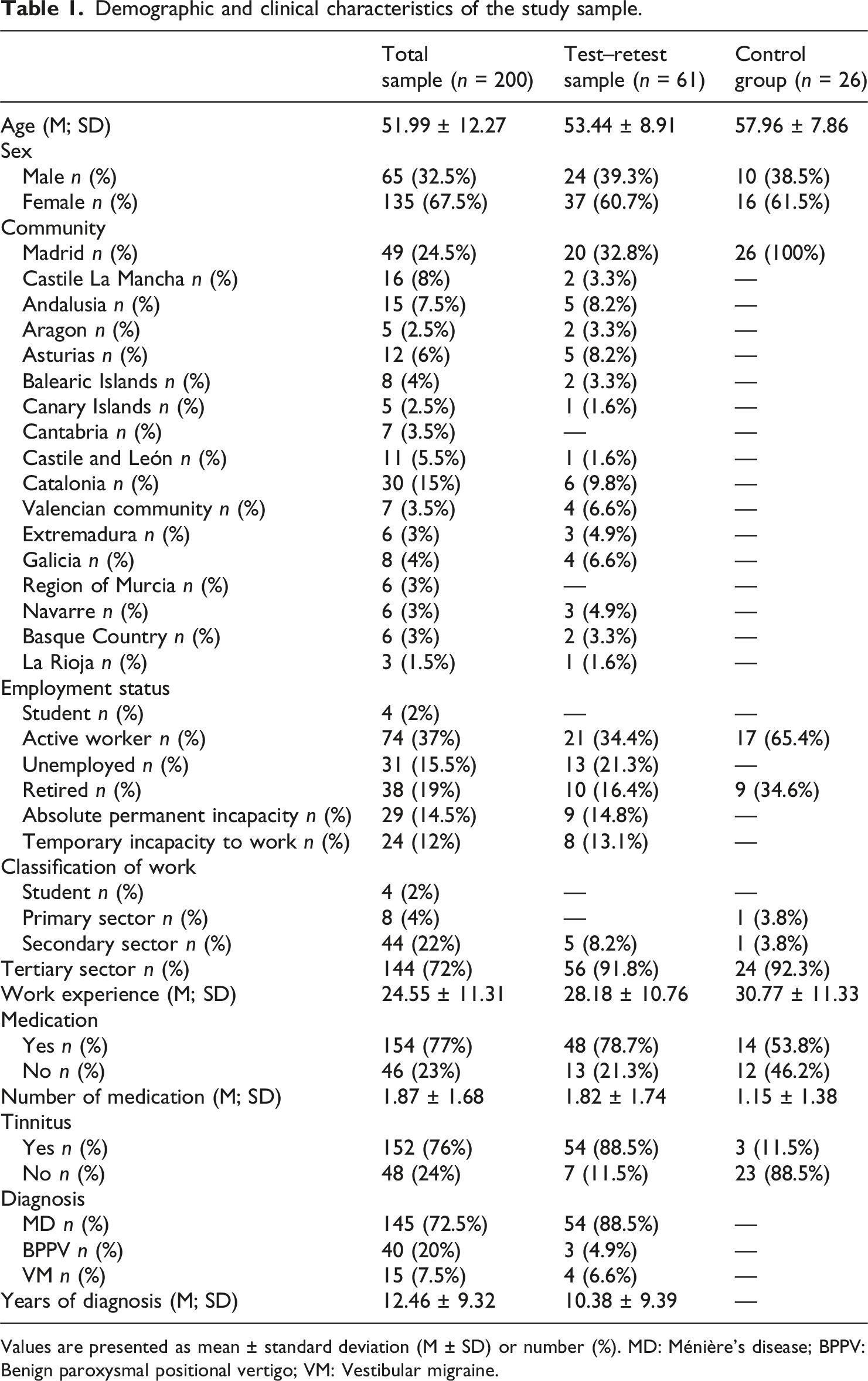
Values are presented as mean ± standard deviation (M ± SD) or number (%). MD: Ménière’s disease; BPPV: Benign paroxysmal positional vertigo; VM: Vestibular migraine.
Pre-test sample (cognitive debriefing)
A preliminary sample of n = 30 participants with vestibular disorders was used to evaluate the comprehensibility, clarity, and cultural adequacy of the translated version (VADL-ES) through cognitive interviews.
The sample had a mean age of 56.1 ± 8.2 years, with 60% women. Most participants were diagnosed with Ménière’s disease (90%), followed by vestibular migraine (10%), with a mean time since diagnosis of 15 ± 9.7 years.
Participants completed the questionnaire and were subsequently interviewed to identify potential difficulties in item interpretation. No relevant comprehension issues were detected.
Test–retest reliability sample
A subgroup of n = 61 participants from the main clinical sample (n = 200) completed the VADL-ES twice within a 4–8 h interval (mean = 6.1 h) to assess temporal stability.
This short interval was selected to minimize the potential impact of symptom fluctuation in individuals with vestibular disorders.
Psychometric validation sample
The main psychometric analyses, including internal consistency, structural validity (EFA and CFA), and construct validity, were conducted in a sample of n = 200 patients with vestibular disorders.
Additionally, a control group of n = 26 individuals without vestibular pathology was included to assess discriminant validity.
For structural validity, the clinical sample was randomly divided into two subsamples (n = 100 each) to perform independent exploratory and confirmatory factor analyses.
Content validity
Six experts rated item relevance using a 4-point Likert scale. The content validity index (S-CVI/Ave) was 0.93 overall, with subscale scores of 0.92 (Functional), 0.96 (Ambulation), and 0.93 (Instrumental), supporting high content validity.
Exploratory factor analysis (EFA)
To examine the factor structure of the VADL-ES, an exploratory factor analysis (EFA) was conducted on a random subsample of 100 participants, following Gorsuch’s recommendation for a minimum sample size. 39 Sampling adequacy was confirmed (KMO = 0.82; Bartlett’s test: χ2 = 6342.245, p < 0.001). Maximum likelihood extraction with oblimin rotation revealed a three-factor solution explaining 72% of the total variance. Factor loadings corresponded to the theoretical structure (Functional, Ambulation, and Instrumental), with an average item complexity of 1.6. Model fit indices were acceptable (RMSR = 0.04; RMSEA = 0.117, 90% CI: 0.107–0.129).
Separate EFAs for each subscale showed acceptable structure. The Functional subscale had KMO = 0.92, RMSEA = 0.283, TLI = 0.666, and CFI = 0.727, with SRMR = 0.086 and all loadings significant. Ambulation showed better fit (KMO = 0.92, RMSEA = 0.171, TLI = 0.88), while the Instrumental subscale also demonstrated structural adequacy (KMO = 0.84, RMSEA = 0.182, TLI = 0.84). In both, SRMR ≤ 0.08 supported the underlying dimensional structure.
Confirmatory factor analysis (CFA)
Confirmatory factor analysis (CFA) was conducted on the remaining 100 participants to test the original three-factor structure of the VADL using maximum likelihood estimation. The model yielded χ2 = 1362.876 (df = 347, p < 0.001), with a χ2/df ratio of 3.93. Fit indices were acceptable overall (CFI = 0.746, TLI = 0.723, SRMR = 0.063), although RMSEA was elevated (0.171; 90% CI: 0.162–0.181), possibly reflecting sample size limitations. All factor loadings were significant (p < 0.001), with most exceeding 0.60, particularly in the Functional and Ambulation subscales.
EFA and CFA Factor Loads of Items of VADL-ES and subscales.
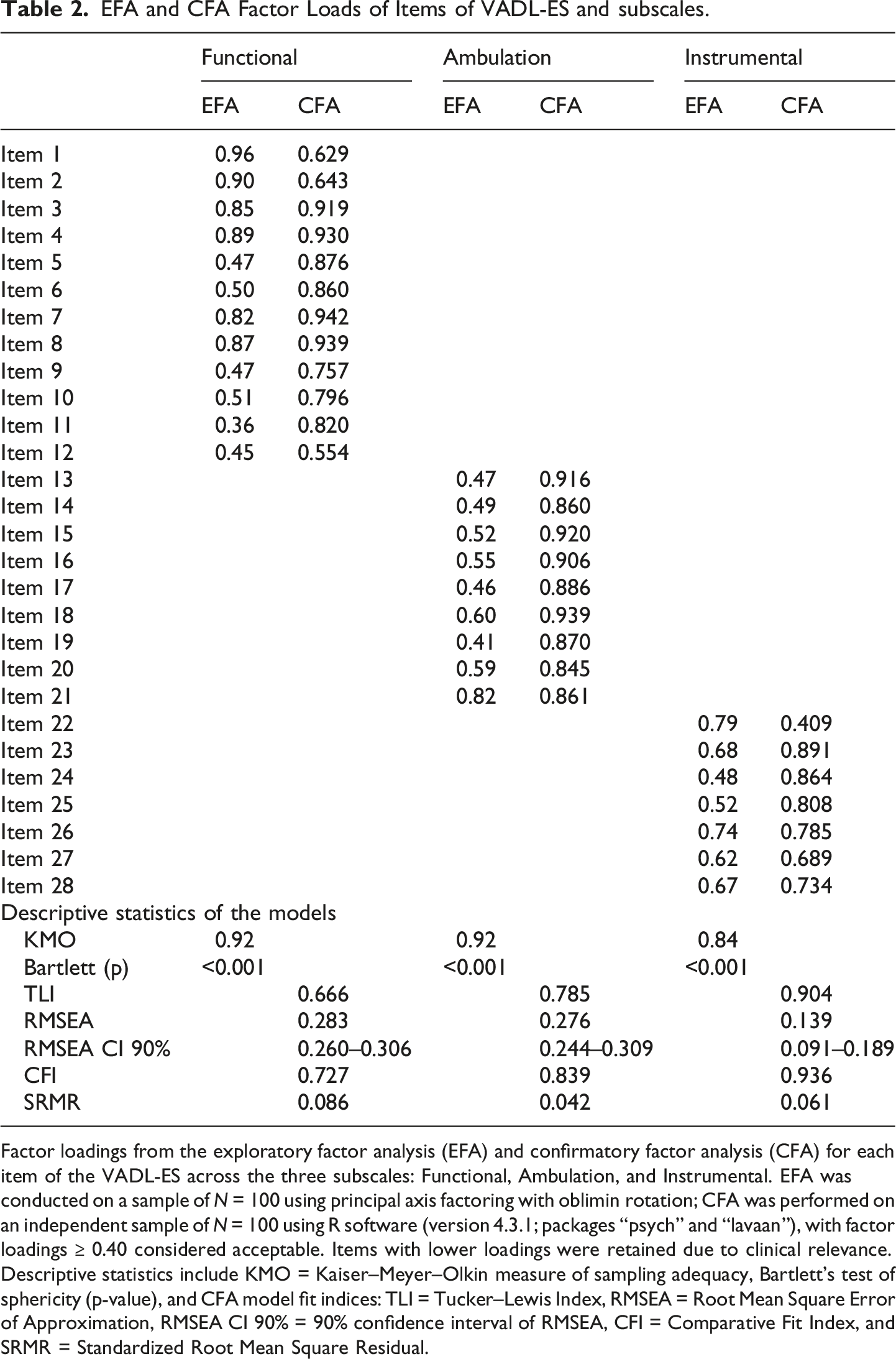
Factor loadings from the exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) for each item of the VADL-ES across the three subscales: Functional, Ambulation, and Instrumental. EFA was conducted on a sample of N = 100 using principal axis factoring with oblimin rotation; CFA was performed on an independent sample of N = 100 using R software (version 4.3.1; packages “psych” and “lavaan”), with factor loadings ≥ 0.40 considered acceptable. Items with lower loadings were retained due to clinical relevance. Descriptive statistics include KMO = Kaiser–Meyer–Olkin measure of sampling adequacy, Bartlett’s test of sphericity (p-value), and CFA model fit indices: TLI = Tucker–Lewis Index, RMSEA = Root Mean Square Error of Approximation, RMSEA CI 90% = 90% confidence interval of RMSEA, CFI = Comparative Fit Index, and SRMR = Standardized Root Mean Square Residual.
Internal consistency
Cronbach’s alpha was 0.978 for the total VADL-ES score, indicating excellent internal consistency. Subscale alphas were: Functional = 0.960; Ambulation = 0.964; Instrumental = 0.899.
Test–retest reliability
A total of 61 participants completed the VADL-ES twice within a 4–8-h interval (mean = 6.1 h), selected to minimize the potential impact of short-term symptom fluctuation, a known characteristic of vestibular disorders, while preserving clinical stability between measurements. The ICC for the total score was 0.988, indicating excellent reliability. Subscale ICCs were: Functional = 0.981, Ambulation = 0.981, and Instrumental = 0.940.
Convergent validity
Convergent validity testing of the VADL-ES with DHI.
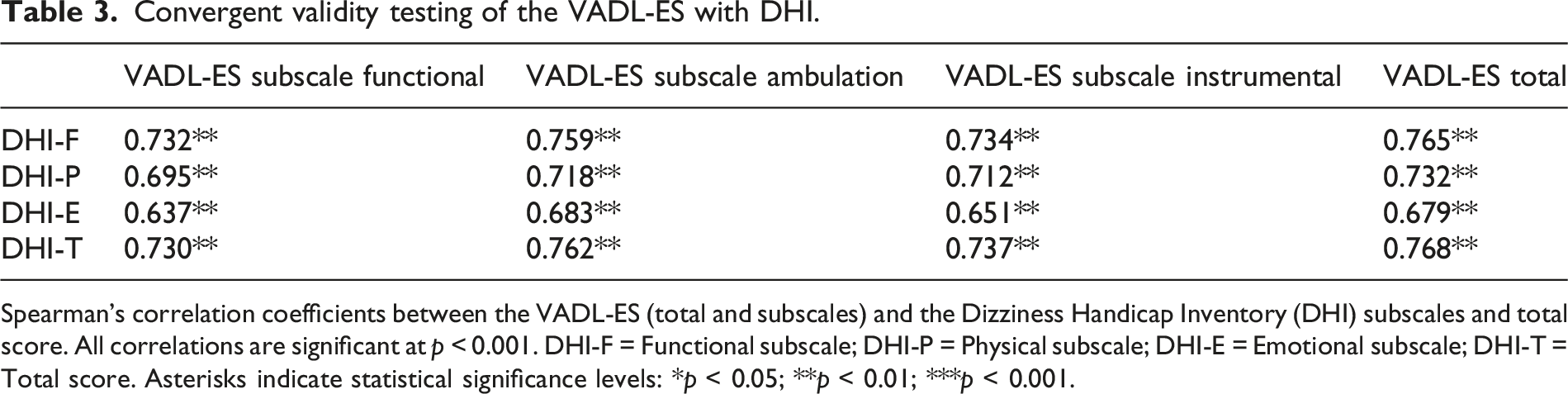
Spearman’s correlation coefficients between the VADL-ES (total and subscales) and the Dizziness Handicap Inventory (DHI) subscales and total score. All correlations are significant at p < 0.001. DHI-F = Functional subscale; DHI-P = Physical subscale; DHI-E = Emotional subscale; DHI-T = Total score. Asterisks indicate statistical significance levels: *p < 0.05; **p < 0.01; ***p < 0.001.
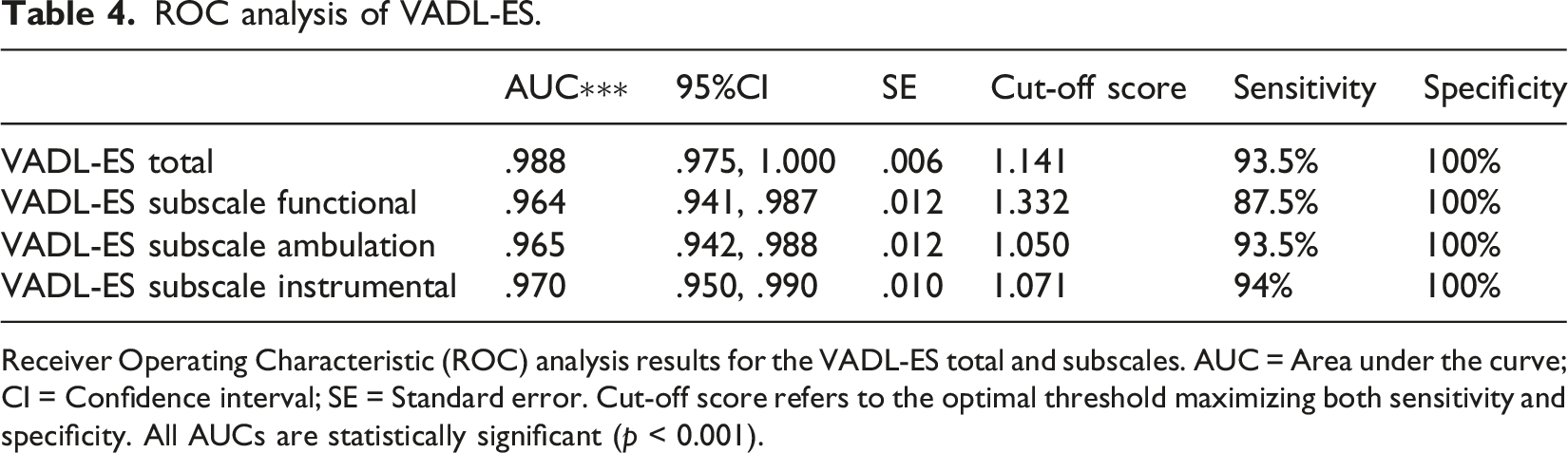
Discriminant validity
ROC curves are shown in Figure 2; results are detailed in Table 4. The AUC for the total VADL-ES score was 0.988. Subscale AUCs ranged from 0.960 to 0.970. All AUCs were statistically significant (p < 0.001) compared to the null value of 0.50. Optimal cut-off points determined by the Youden index were ≥1.141 (total), ≥1.332 (Functional), ≥1.050 (Ambulation), and ≥1.071 (Instrumental), yielding sensitivities from 87.5% to 94% and 100% specificity. ROC curves for VADL-ES total score and subscale scores between test group versus control group. The turquoise curved line indicates VADL-ES total score; the yellow curved line indicates VADL-ES Ambulation subscale; the red curved line indicates VADL-ES Functional subscale; the pink curved line indicates VADL-ES Instrumental subscale. The straight line indicates nondiscriminating characteristics of the test. ROC analysis of VADL-ES. Receiver Operating Characteristic (ROC) analysis results for the VADL-ES total and subscales. AUC = Area under the curve; CI = Confidence interval; SE = Standard error. Cut-off score refers to the optimal threshold maximizing both sensitivity and specificity. All AUCs are statistically significant (p < 0.001).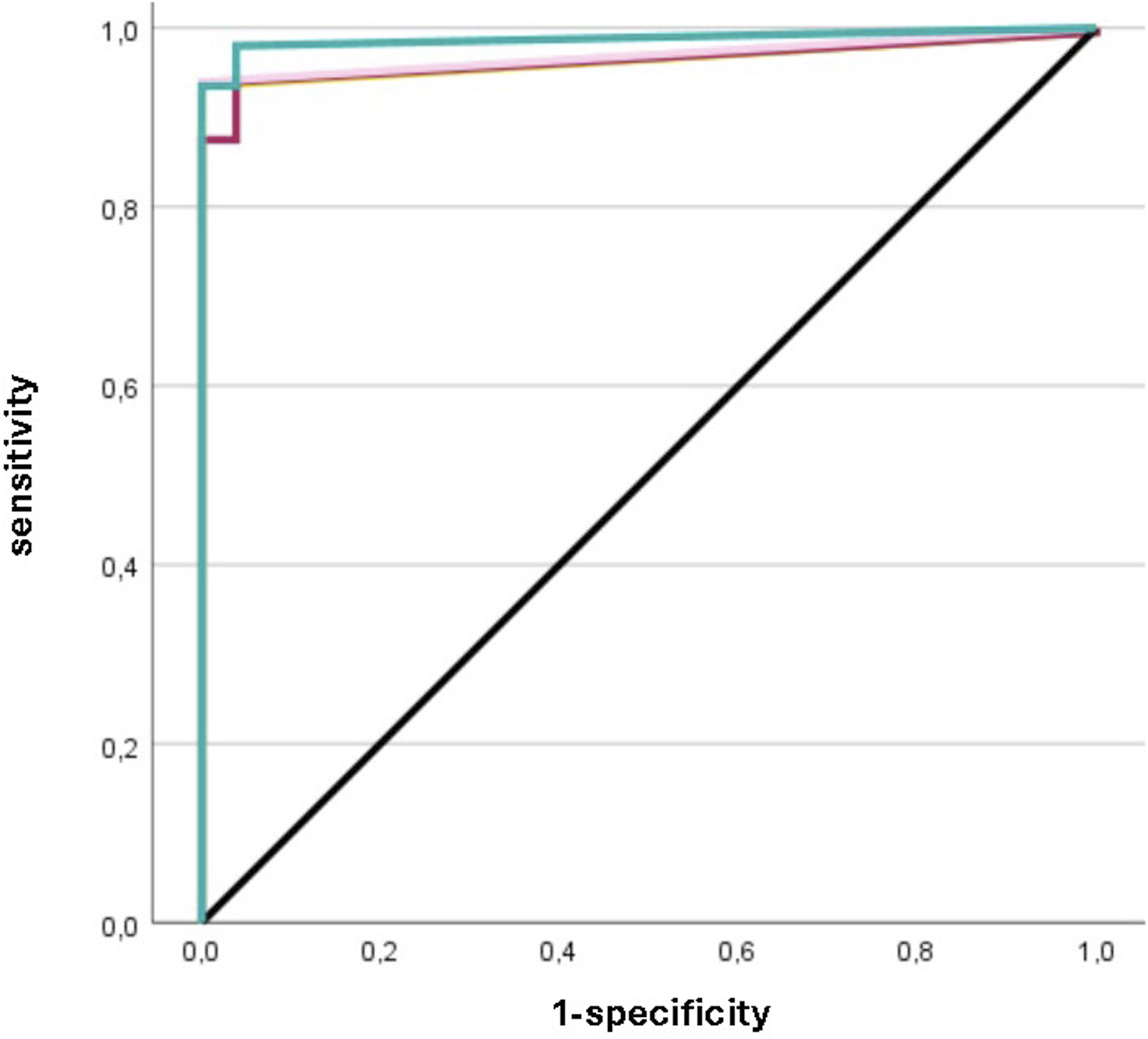
Measurement error, responsiveness, floor and ceiling effects
SEM was 0.328; MDC95 was 0.91, indicating high responsiveness. No floor or ceiling effects were detected (≤2% scoring extremes).
Discussion
The development of the VADL-ES adhered closely to internationally recognized guidelines for cross-cultural adaptation of health-related measurement tools, including those proposed by Beaton et al. and the ISPOR Task Force.22,23 This approach ensured both linguistic accuracy and cultural relevance, applying dual independent translations, expert committee review, and a reconciliation process based on pre-established decision criteria for semantic, cultural, and grammatical equivalence.25,27 Notably, this method aligns with the procedures used in other VADL adaptations, such as the Brazilian, 11 Chinese, 12 Kannada, 13 and Persian 14 versions, all of which followed structured, albeit slightly varied, translation and adaptation protocols.
Despite these shared methodological foundations, there are distinct differences that set the VADL-ES apart. One of the most noteworthy aspects is the detailed criteria used during the reconciliation phase, which prioritized not only fidelity to the original instrument but also comprehension across different literacy levels and cultural appropriateness of sensitive content. For instance, decisions regarding item terminology (e.g., “sexual activity” or “driving”) were evaluated for their acceptability and clarity within the Spanish cultural context, an approach echoed in the Kannada and Persian adaptations but executed with greater transparency and documentation in the current study.13,14
Furthermore, the VADL-ES team introduced a formalized rating system for item relevance and comprehensibility during the expert committee phase, where each item was evaluated according to semantic equivalence, cultural suitability, and clarity. This level of structured appraisal was not systematically reported in the Brazilian or Chinese adaptations, which instead relied more heavily on back-translation and consensus approaches.11,12 In contrast, the Spanish version leveraged both qualitative and quantitative input from bilingual clinicians and researchers to resolve discrepancies, particularly in items referencing contextually specific activities. An important methodological aspect of the VADL-ES adaptation is the omission of the back-translation step, which is traditionally recommended in established cross-cultural adaptation guidelines such as those proposed by Beaton et al. and ISPOR.22,23 Although back-translation is commonly recommended, its role should be understood within a broader framework that includes forward translation, expert committee review, and cognitive debriefing as complementary and interdependent steps. 26 Some methodological studies have reported variability in the implementation of these procedures across guidelines.40–42 Nevertheless, back-translation remains a key component of most standard cross-cultural adaptation protocols, and therefore its omission in the present study should be acknowledged as a methodological limitation.
In the present study, back-translation was not performed. Several complementary procedures were implemented to support semantic and conceptual equivalence, including independent forward translations, a structured reconciliation process, expert committee review, and cognitive interviews during pre-testing. However, these procedures do not replace the role of back-translation within the adaptation process. Therefore, its absence should be considered a methodological limitation when interpreting the results.
Therefore, the omission of back-translation was a deliberate methodological decision informed by emerging evidence and practical considerations, particularly the availability of a strong expert-based approach. Nevertheless, it should be acknowledged that most contemporary guidelines continue to recommend including all stages of the adaptation process, including back-translation, to ensure methodological rigor.22,23,27,42 Consequently, the absence of this step may be considered a limitation, and future studies are encouraged to incorporate it to further strengthen the cross-cultural validity of the instrument.
Additionally, a key linguistic adaptation involved the naming of the subscales. While the original VADL includes three subscales: functional skills (F), ambulation skills (A), and instrumental skills (I), the Spanish version adopted the terms “Habilidades funcionales” (F), “Habilidades de deambulación” (D), and “Habilidades instrumentales” (I). Notably, the term “ambulation” has limited usage in Spanish, particularly in Spain, where the more commonly accepted term is “deambulación.” Consequently, the abbreviation for the ambulation subscale was adapted from “A” to “D” to maintain linguistic naturalness and clarity for Spanish-speaking respondents.
Another important distinction lies in the treatment of culturally dependent activities. For example, in the original scale developed by Cohen et al., the item “driving a car” assumes a universal relevance that does not translate equally across all populations. 10 In the Spanish adaptation, this item was carefully reviewed due to variability in driving rates among older adults and individuals from urban centers who may rely more on public transport. Rather than removing or replacing the item, the VADL-ES clarified its definition to ensure it referred explicitly to operating a motor vehicle, not passive transport. Similarly, the item “sexual activity,” which is often a source of discomfort or non-response in certain cultural contexts, was retained in the Spanish version to preserve conceptual integrity. To enhance clarity and reduce response bias, the description was expanded within the item itself to specify that it refers to consensual sexual behavior, including intercourse, masturbation, and foreplay (“coito, masturbación y preliminares”). In contrast, the Kannada version omitted this item altogether due to anticipated cultural resistance. 13
In other instances, lexical modifications were made to enhance everyday comprehension. For example, “bathing/showering” was translated into two distinct Spanish verbs (“bañarse/ducharse”) to capture regional usage differences and improve clarity. The term “household chores” was adjusted to “tareas domésticas,” a more common and contextually appropriate phrase in Spanish-speaking populations. A clear example of this appears in the item “household chores,” which was initially translated as “quehaceres domésticos”. However, during the expert review, it was determined that “tareas domésticas” was a more inclusive and familiar term across different Spanish-speaking regions, especially among older adults and those with lower literacy levels. These nuanced adaptations aim to ensure the relevance of each item across diverse sociocultural and educational backgrounds, something not uniformly detailed in the Chinese or Persian versions.12,14 Additionally, the Spanish adaptation emphasized the importance of cultural roles embedded in certain items, such as “participating in social activities” and “engaging in occupational roles.” In Spain, occupational engagement in older adults can vary significantly due to socioeconomic and retirement policy factors. Therefore, the definition of “occupational role” was broadened to include volunteer work, caregiving, or community-based activities, an approach similar to that taken in the Brazilian version, but articulated more explicitly in the Spanish adaptation. 11
Taking together, these modifications reflect a deliberate and methodologically rigorous approach to cultural adaptation that goes beyond literal translation. By addressing semantic nuance, regional vocabulary, and cultural norms, the VADL-ES offers an instrument that is not only equivalent in construct but also optimized for contextual relevance. This level of attention to detail helps ensure that patient responses genuinely reflect their functional limitations, reducing potential biases introduced by misunderstanding or discomfort.
Regarding content validity, the VADL-ES demonstrated excellent conceptual clarity and item relevance. Expert evaluations confirmed that each item accurately reflected the functional limitations typically experienced by individuals with vestibular disorders. These findings are consistent with previous high-quality adaptations of the VADL, including the Chinese, Persian, and Kannada versions, which also reported strong item representativeness and semantic equivalence based on expert judgment.12–14 The consistency of these results across diverse linguistic and cultural contexts reinforces the utility of rigorous cross-cultural adaptation methodologies as outlined in established international guidelines.22,23
With respect to construct validity, the VADL-ES benefited from the combined application of exploratory and confirmatory factor analyses, a methodological strategy not commonly implemented in previous adaptations. This dual approach provided robust empirical evidence for the preservation of the original three-factor structure (Functional, Ambulation, and Instrumental subscales), as proposed in the original VADL. 10 In contrast, many previous adaptations, including the Brazilian and Kannada versions, focused primarily on reliability metrics without formally testing the underlying factorial structure.11,13 Our findings confirm the dimensional integrity of the scale and offer stronger construct validation than previously available, aligning with established psychometric guidelines.29,30,43
In terms of internal consistency, the Spanish version of the VADL showed remarkable coherence among items within each subscale and across the overall scale. This suggests that the scale’s items effectively capture consistent patterns of disability related to vestibular dysfunction. Compared to the original VADL, which already demonstrated excellent internal consistency, 10 the VADL-ES demonstrated even higher internal consistency coefficients. This enhancement may be attributable to a more homogenous clinical sample, improved item clarity through linguistic refinement, and the cultural relevance of daily tasks assessed in the Spanish population. Furthermore, while the Brazilian version showed strong consistency in most domains, it reported a notably lower value for the Instrumental subscale, 11 a limitation not observed in the Spanish version. These differences may reflect both cultural interpretations of activities and methodological rigor in translation and item selection.
The test–retest reliability of the VADL-ES was confirmed, showing highly stable scores when administered twice on the same day in participants with chronic and clinically stable vestibular symptoms. Although current methodological standards, such as COSMIN, recommend longer intervals (e.g., 24–48 h or up to 1–2 weeks) to minimize recall bias, 28 the choice of a short interval in the present study was primarily driven by the need to ensure clinical stability in a population characterized by symptom fluctuation.2,4
This approach is consistent with the original VADL validation, which used a similarly brief interval and reported excellent reliability. 10 Moreover, short test–retest intervals have also been applied in related vestibular instruments, such as the Dutch version of the Dizziness Handicap Inventory, which demonstrated very high reliability with same-day administration. 44 In contrast, other cross-cultural adaptations of the VADL have employed longer intervals (e.g., 1 to 2 weeks) and still reported high reliability coefficients,11–14 suggesting that the instrument is inherently stable across different temporal conditions. Importantly, consistency with previous studies does not, by itself, justify the methodological choice. Therefore, the selected interval should be understood as a trade-off between minimizing clinical variability and the potential risk of recall bias, as both factors are critical when determining appropriate test–retest intervals in clinical populations.
Therefore, while the short interval used in this study may have contributed to a slight overestimation of reliability due to recall bias, the consistency of findings across studies using longer intervals supports the robustness of the scale. To mitigate potential recall effects, methodological precautions were implemented, including ensuring clinical stability of participants and varying item presentation. 28 Nevertheless, the possibility of recall bias cannot be fully excluded. Future studies are encouraged to replicate these findings using longer intervals in line with COSMIN recommendations to further confirm temporal stability under more stringent methodological conditions. 28
When assessing convergent validity, the VADL-ES exhibited strong correlations with the DHI, supporting its relevance as a measure of perceived disability in individuals with vestibular dysfunction. This observation is consistent with findings from the Kannada and Persian versions.13,14 Interestingly, the original VADL validation did not assess convergent validity using the DHI or any related instrument. 10 This gap limits comparison with the initial psychometric foundation, making the current study an important contribution to the broader validation literature.
Notably, this study is the first to explore discriminant validity of the VADL through ROC curve analysis. The VADL-ES demonstrated a strong ability to distinguish between individuals with and without vestibular disorders. This property, along with the establishment of population-specific cut-off points, strengthens the instrument’s clinical applicability for both diagnostic and rehabilitative purposes. Earlier adaptations of the VADL, including the Chinese, Brazilian, and Persian versions, did not assess discriminant validity,11,12,14 making our findings a valuable addition to the evidence base.35–37,39
The responsiveness of the VADL-ES, measured through the SEM and MDC, adds further utility for clinical and research settings. These metrics, which were not reported in prior validations, allow clinicians to interpret whether observed changes in patient scores are meaningful or within the margin of error.41,42 Their inclusion positions the Spanish adaptation as a tool not only for diagnosis but also for tracking therapeutic progress and treatment outcomes over time.
When comparing the psychometric properties of the VADL-ES with previously validated versions, the Spanish adaptation demonstrates comparable and, in some cases, slightly higher values across several domains. For instance, the internal consistency of the VADL-ES (α = 0.978) is slightly higher than that reported in the original version (α ≥ 0.90), 10 as well as in the Brazilian and Persian adaptations, which reported values above 0.90 but generally lower than those observed in the present study.11,14 Similarly, the Chinese version also reported excellent internal consistency (Cronbach’s α > 0.90), supporting the consistency of the scale across cultural contexts. 12
Test–retest reliability in the VADL-ES (ICC = 0.988) is at the upper range of values reported in other versions, where ICC values typically ranged between 0.85 and 0.97.11–14 In line with this, the Chinese adaptation also demonstrated high reliability, with ICC values above 0.90, 12 indicating strong temporal stability across different populations. Convergent validity with the DHI (ρ = 0.768) is also consistent with findings from the Kannada and Persian versions, which reported moderate to strong correlations with related constructs.13,14
Overall, these findings are in line with previously validated versions across different cultural contexts, supporting the cross-cultural robustness of the VADL. However, these differences should be interpreted with caution, as variations across studies may be influenced by sample characteristics, methodological differences, and testing conditions (e.g., retest interval), rather than true differences in instrument performance.
Compared to most previous adaptations, which primarily focused on reliability and basic validity measures, the present study also includes analyses of discriminant validity, measurement error (SEM, MDC), and structural validity using both exploratory and confirmatory factor analyses. This more comprehensive psychometric evaluation strengthens the overall evidence supporting the validity and clinical utility of the VADL-ES.
Lastly, the absence of floor and ceiling effects in the VADL-ES indicates its ability to capture a broad range of functional limitations. This feature ensures that the scale remains sensitive across different levels of severity, avoiding clustering of scores at either end of the spectrum. This finding was consistent with the original scale’s design but is rarely reported in previous adaptations.10–14 Our results suggest that the VADL-ES maintains measurement precision across the continuum of vestibular disability.
Taken together, these psychometric properties affirm that the VADL-ES is a reliable, valid, and clinically relevant tool for assessing the functional impact of vestibular disorders in Spanish-speaking populations. Its methodological rigor, including dual-phase construct validation, stability testing, and sensitivity measures, positions it among the most comprehensive and robustly adapted versions of the VADL to date. In doing so, it not only facilitates accurate assessment in clinical practice but also contributes meaningfully to the global literature on vestibular health measurement tools.
Study limitations
The Spanish version of the VADL was culturally adapted to reflect the linguistic and conceptual context of Spanish-speaking populations. Although the Spanish version of the VADL demonstrated strong validity and reliability, supporting its use as a valuable tool to assess functional limitations in individuals with vestibular disorders in both clinical and research settings. Moreover, specifying the exact challenges patients face in activities of daily living may contribute to the development of more targeted rehabilitation programs. Nevertheless, several limitations should be acknowledged.
First, test–retest reliability was assessed using a short interval (4–8 h). Although this approach ensured that no relevant clinical changes occurred between measurements in a population with potentially fluctuating symptoms, it does not fully align with current methodological recommendations, which suggest longer intervals to minimize recall bias. 28 Consequently, the reliability estimates may be slightly inflated due to memory effects. While similar short intervals have been used in the original VADL and in other vestibular measures,10,44 this methodological choice should be interpreted with caution. Future research should prioritize longer retest intervals (e.g., 24–72 h or up to 1–2 weeks) to provide more conservative estimates of temporal stability.10,30
Second, the back-translation step, commonly recommended in cross-cultural adaptation guidelines,22,23 was not performed. While several complementary procedures, such as independent forward translations, expert committee review, and cognitive interviewing, were implemented to ensure semantic and conceptual equivalence, these do not replace the role of back-translation within standard methodological frameworks. Therefore, its absence should be considered a methodological limitation, potentially affecting the overall rigor of the adaptation process, and should be taken into account when interpreting the results.
Third, although a control group was included to assess discriminant validity, the control sample was relatively small and not matched to the clinical group in sociodemographic characteristics such as sex. This imbalance could affect external validity and limit the generalizability of the discriminant findings. Larger and demographically matched comparison groups should be considered in future studies to strengthen the interpretability of results.
Lastly, the clinical sample consisted predominantly of individuals diagnosed with Ménière’s disease. While this condition represents a substantial portion of the vestibular disorder population, the limited inclusion of other diagnoses, such as vestibular neuritis, benign paroxysmal positional vertigo, or vestibular migraine, may restrict the applicability of the findings across the broader spectrum of vestibular disorders. Further research validating the VADL-ES in more diagnostically diverse populations is warranted to ensure comprehensive utility.
Conclusions
The present study supports the VADL-ES as a reliable, valid, and culturally adapted instrument for assessing functional limitations in Spanish-speaking individuals with vestibular disorders. It demonstrated excellent internal consistency, high test–retest reliability, and strong discriminative validity, confirming its utility for both clinical assessment and research applications. The VADL-ES enables standardized evaluation of functional dependence across a range of daily activities, and its linguistic and cultural relevance enhances its applicability within the Spanish context. However, the short test–retest interval used may have led to a slight overestimation of reliability; therefore, results should be interpreted with caution until confirmed by studies using longer intervals. Further studies involving broader and more diverse clinical populations are warranted to strengthen generalizability and explore its responsiveness across different vestibular diagnoses.
Supplemental material
Supplemental material - Cross-cultural adaptation and psychometric properties of a Spanish-language version of the Vestibular Disorders Activities of Daily Living Scale (VADL-ES)
Supplemental material for Cross-cultural adaptation and psychometric properties of a Spanish-language version of the Vestibular Disorders Activities of Daily Living Scale (VADL-ES) by Aitor Yusta-Ceacero, Sergio Serrada-Tejeda, Patricia Sánchez-Herrera Baeza, Nuria Máximo-Bocanegra, Paula Obeso-Benítez, Joaquín Horna-Schlincker, Helen S. Cohen, Rosa M. Martínez-Piédrola, and Marta Pérez-de-Heredia-Torres in Journal of Vestibular Research
Footnotes
Acknowledgments
The authors sincerely thank the Asociación Síndrome de Ménière España (ASMES), Clínica Osteofels, and the Spanish Professional Colleges of Occupational Therapy for their collaboration in the recruitment of participants.
ORCID iDs
Ethical considerations
The study was approved by the Ethics Committee of Universidad Rey Juan Carlos (Approval Code: 0611202335623; Date: December 7, 2023).
Consent to participate
All participants provided written informed consent in accordance with the Declaration of Helsinki.
Author contributions
All authors read and approved the final manuscript and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Other identifying information
Permission to use the “Vestibular Disorders Activities of Daily Living Scale” was obtained through the American Medical Association (License No. 6070660976043, issued and renewed on July 16, 2025). Original source: Cohen HS, Kimball KT. Development of the Vestibular Disorders Activities of Daily Living Scale. JAMA Otolaryngology—Head & Neck Surgery.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.