
Abstract
Noise pollution is a growing problem in hospitals. Noise is a common complaint among hospital staff, patients, and their families in hospitals. Research shows the negative impact of noise on patients. The common effects of noise on patients and staffs in hospitals are annoyance, irritation, high blood pressure, stress, poor mental health, and fatigue. But peoples are unaware about these effects. There are different noise sources in the hospitals e.g., medical equipment, talking of patient’s family members, staff conversation, opening-closing doors etc. There is need to control the noise level in the hospitals from the above noise sources. In this review paper, the noise effects on patients, noise sources in hospitals and noise controlling strategies are summarised and discussed. The aim of this review work is to increase the awareness about the noise effects on human health and show the actual condition of the hospital noise. Further, to increase the researcher’s curiosity to do in-depth research on noise pollution and control in hospitals.
Introduction
Noise pollution (sound pollution) is also known as environmental noise. This unwanted sound is increasing day by day and control over this is important aspect. Busch et al.
1
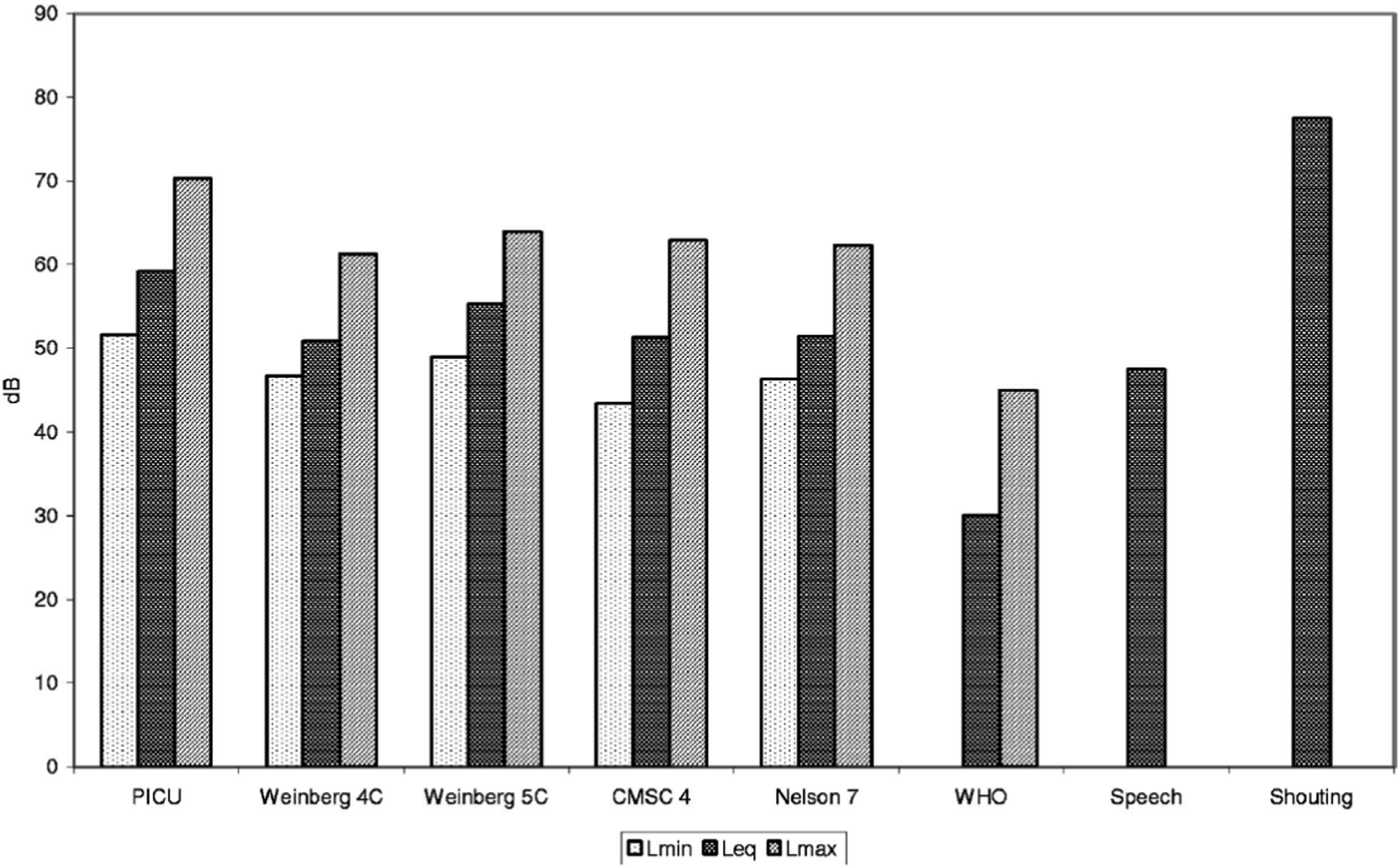
did the noise survey at Johns Hopkins Hospital (JHH) in Baltimore, MD, and measured noise level by considering equivalent sound pressure levels (SPL) as a role of frequency, location, and time of day. They found a serious problem at all locations and all times of day. There is no location where the noise level follows the current World Health Organization (WHO) Guidelines. The data in the review paper shows that this is the true condition of hospitals all over the world. Figure 1 shows the average SPL recorded in JHH and its comparison with WHO recommendations. Logarithmic average A-weighted SPLs in JHH compared with WHO recommendations and the levels for speech.
1
There are different effects of noise pollutions on human and animals. The common effects on human are hearing losses, ischemic heart disease, hypertension, annoyance, tinnitus, and sleep disturbance.2,3 Ising and Kruppa 4 studied the effects of noise pollutions on human health. They reviewed past 25 years literature and found out that the traffic noise is the most powerful source of annoyance. Hospital noise levels are somewhat lower than other locations such as airports, roads and construction sites. However, because of the nature of the environment with patients wanting rest and privacy, these relatively low noise levels are an issue. Noise not only affects the health issue but also decrease the employment due to noisier regions. 5
Many researchers did the study on hospital noise and its effects on human being. The literature shows that the noise affects are more serious in hospitals which is discussed in the below section. The effects on both hospital staff and patients are common as they are continuously with noise exposures. There are several equipment/devices installed in the hospital which make noise. Apart from these equipment/devices the movement and talking of family members of patients are general source of hospital noise. The hospital staff/nurses also make noise in the hospitals by movement and talking to each other and with patient/patient family members. These noise sources are also discussed. There are different noise controlling strategies and methods which are also discussed in detail. The last section summarises the literature work done so far and presented the scope for future research in the field of hospital noise.
Hospital noise effects
In hospitals, there are three types of people i.e. hospital staff, patient and family members of the patient. Generally, people ignore the noise pollution because of the lake of knowledge about its effects or due to noise exposer for a short duration. Due to this, the people think that it will not affect much. But in the case of hospitals, the patient who already undergoing with some disease can have chances to increase adverse effects of noise. A noise impact investigation in the ICU was conducted by Pugh et al. 6 particularly for the hard of hearing and elderly peoples. They found that noise may obstruct communication and reduce understanding. Noise may also create abnormalities in thought processing and behavior. There are several literatures available which shows the effects of noise on human in hospitals. Some are discussed here.
Noise effects on patient
Patients have more chances to be affected by noise exposure. There are many studies about hospital noise and its effects on patients.7,8 The noise level measurement and its analysis are the first step for the researchers. Hilton 9 collected twenty-five samples from different care units of three hospitals for the study of noise level and found the higher noise level than the normal range. Ising and Kruppa 4 studied the effects of noise on patient health. They reviewed past works and found out that the noise is the main source of annoyance. The annoyance problem due to noise is common in patients but it is also common in hospital staff and hospital visitors. 10 The study of Balogh 11 shows that ICUs is a major noise source for stress in patient. The annoyance problem was also observed in the patient. Their study also shows that the patient gets irritated due to alarms noise. The psychological response of patients, hospital staff, and hospital visitors are also affected by noise pollutions. 10 According to Madalena and Nelio, 12 hospital noise influences the subjective wellbeing of the human, and it was confirmed that some physiological dissemination in patients were related to hospitals noise. Some studies also show the anxiety and distress among patients. 13 Extreme noise also reduces healthcare quality and safety. Some other problems like stress, high blood pressure, sensitivity of pain and poor mental health were also observed. Noise level is responsible for reducing the speech intelligence of the patient and hearing losses are also observed in the patient. 14 There is other impact of noise on word identification by the patient after talking on speaker. 14 Allaouchiche et al. 15 studied the effect of noise pollution on anaesthesia recuperating patients. They considered the sources and noise intensity in the postanaesthesia care unit and found there was no discomfort in the patients although sound in the postanaesthesia care unit surpassed equivalent sound level of 40 dB-A the globally suggested intensity level. They also concluded that conversation among patients, family members etc. were the most common reason of high noise. Hsu et al. 16 wrote a review paper on hospital noise and its effects. Some of the papers were focused on noise pollutions which were related to patient’s problems such as lack of sleep-in patient, cardiac response, long hospital stays, healing problem, and physiological issues. The extreme noise in hospitals disturbs the communication and increase fatigue, annoyance, and irritation. 17 There are several effects of noise, some common type of effects of noise are discussed in detail in the next sections.
Sleep disturbance
Sleep disturbance due to noise pollution in hospitals is quite common among the patients. Many research papers have been published on this issue. Some papers are discussed here; the study of Badia 18 and Buxton 19 were focused on sleeping disturbance in hospitals. Sleep difficulties in hospitals are due to disruptions and can be understood how patients, hospital doctors, and nurses notice sleep disruptions. 20 The noise in hallway also is a key factor for sleep disturbance. 18 Elliott et al. 21 considered critically ill patients and defined two types of factors i.e., intrinsic, and extrinsic. These factors affect the sleep of the patients. Waye et al. 22 analysed ICU noise environment and found sleep disturbances. Their study shows that noise reduction from 64 to 56 dB is not enough to improve the sleep quality. The ICUs noise also weakens the sleep. However, the white noise also affects the sleep in ICU. 23 The peak noise and variation in sound level from reference line were investigated and found that if the white noise increases that would be able to minimise the amount of changing noise levels. According to this study, the peak sound levels were not the main reason of sleep disturbance in ICU. 23 Ding et al. 24 studied the ICU noise for patients’ sleep disturbances and recorded the perceptions and opinions obtained by patients, staff and surrogates. Simons et al. 25 studied the effect of noise on subjective sleep quality. Noise levels were found negatively related for male and positively related for female gender. Xie et al. 26 reviewed the sleep disturbances from ICU noise. Their review study suggests that the staff discussion and alarms were the main reason of sleep disturbance in ICUs. Nicholas et al. 27 analysed noise during sleep and found that this induces heart rate, peripheral vasomotor and electroencephalogram changes. Plummer et al. 28 studied high sound level related with sleep insufficiency and observed that it increases occurrence of delirium. Falk and Woods 29 observed that the noise levels stimulated the hypophyseal-adrenocortical axis of patients and posed a threat to incompatible with sleep. Aaron et al. 30 observed that environmental noise of sound peak greater than 80 dB-A is potentially responsible for sleep-disruptive. Margaret 31 studied the stress and sleeps due to noise in 105 female volunteers and found the sleep disturbances in the patients. The effectiveness of sleep care strategies and improving quality of sleep were also studied by the researchers. 32
Hearing loss
Hearing loss is mainly associated with high noise level or continuous noise level exposure. In hospital environment, continuous noise exposure generally occurs than the peak noise level. In industries, peak noise level is also a major problem. There are several research papers which show the reasons of hearing loss of hospitalised patient or hospital staff is due to noise pollution. The hearing loss can significantly influence the performance of the human. 14 Prabhakar et al. 33 used CEM DT-8851 industrial high-accuracy digital sound noise level meter data logger (CEM Instruments, Bengal, India) and studied the effects of noise on a surgeon’s hearing. The recorded noise level was analysed and compared. The maximum and minimum noise level was recorded during non-drilling and suction periods, and it was seen that the noise level exceeded 85 dB that was only in 0.04% of the time of test. Love 34 used Quest Q-300 Noise Dosimeter and Quest Calibrator (Quest Technologies, USA) and studied orthopaedic operating theatres surgeons and they were exposed to noise pollution produced by routine hospital instruments and found the hearing loss risk among the surgeons. Nassiri and Golbabai 35 studied the noise level related with air-turbine drills that were used in dental hospital. They observed the average value 69.1 dB-A for the high-speed drills. In the high frequency range around 6000- 8000 Hertz, the maximum energy level was found. Audiological assessment shows that the hearing damage occurred at 6000 Hertz range for all groups in dental practice which had a connection with the sound level in this frequency. They also observed that hearing loss is different in female and male groups and greater hearing loss found in the female group. Girard et.al 36 studied noise pollution for male workers in hospital and exposed him to a greater than 80 dB-A noise level, which showed a hearing loss due to high noise level. Falk and Woods 29 studied hospital noise levels in acute-care unit (ACU), recovery room and infant incubators. The measurements were made for 24 hours and it showed a threat to hearing loss in patients. Purnami 37 studied hearing loss due to reactive oxygen species on risk workers at the hospital. The hearing loss may be due to increased reactive oxygen species (ROS) but in the study there was no correlation between ROS and hearing loss. Shukla et al. 38 review study was focused on age-related hearing loss mainly on older aged adults and concluded that noise level affects hearing loss of older aged patients significantly.
Newborn children healing
The noise pollution affects many patients in the hospitals, but it also affects newborn children in hospitals. There are some literatures that gives the overview of noise effects on newborn child and during hospitalized. Adatia et al. 39 studied the noise level in maternity ward and suggested that how to control noise level in room of maternity ward because the noise is observed dangerous to the healing process for both mothers and their new-borns. They suggested to the healthcare decision-makers that it is needed to reduce the noise level. This study also gives provisions on how to minimise the noise pollution or at least maternity ward should have less noise level. There were some studies that related to the noise level in university hospital centre. These studies about the noise effect on mother and new-born children. 40 The impact of noise levels in children admitted in hospital for treatment were also studied. 41
Noise effects on hospital staff
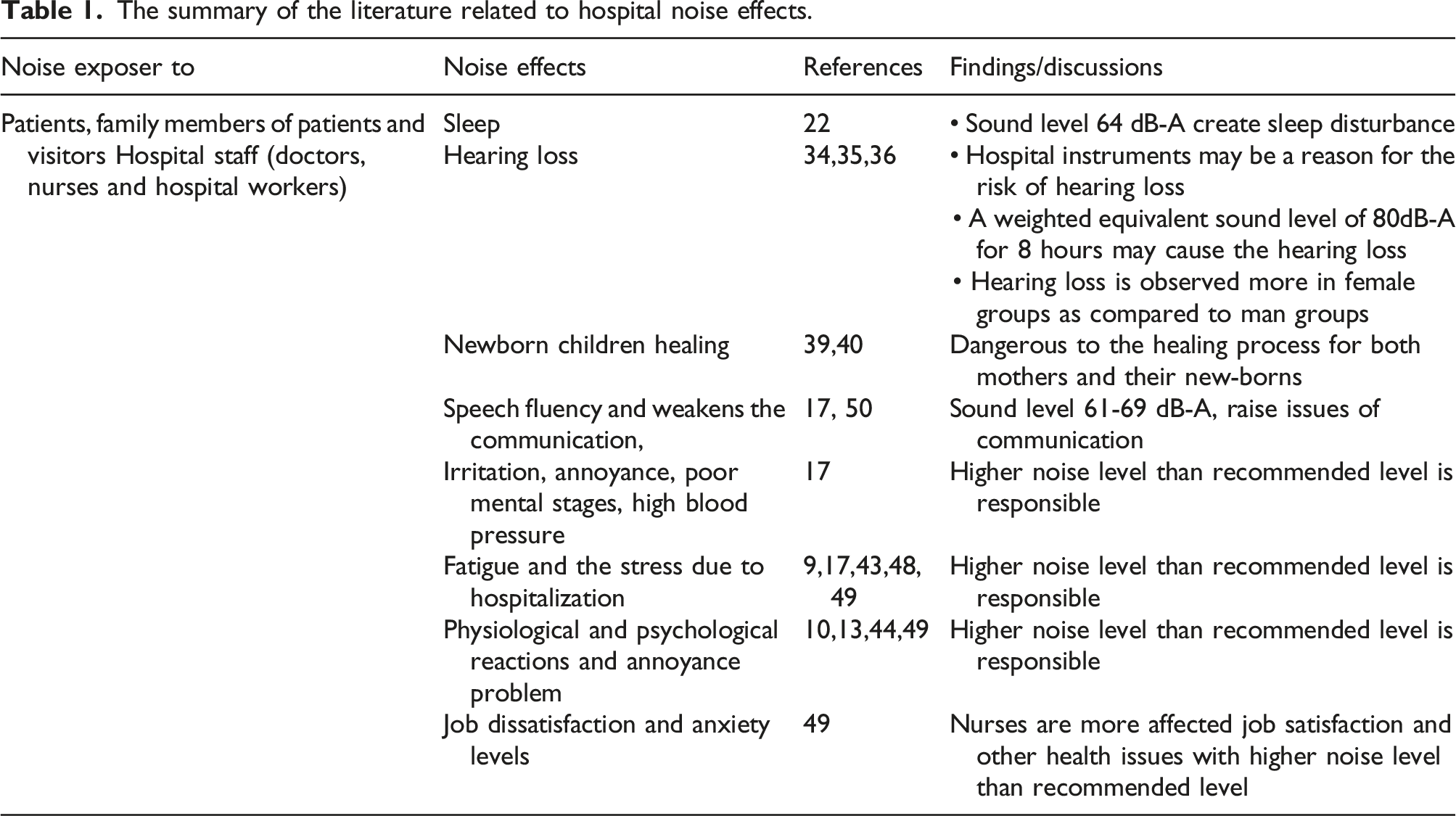
The summary of the literature related to hospital noise effects.
Hospital noise sources
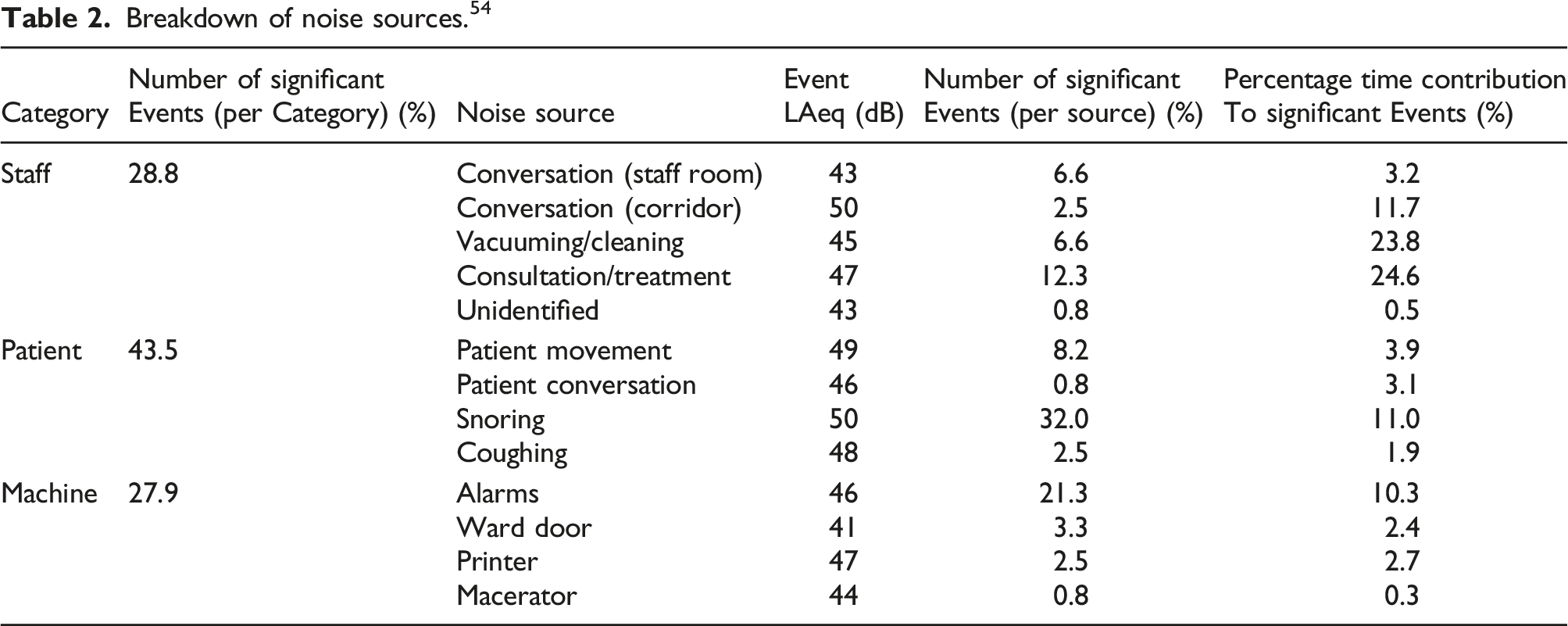
Breakdown of noise sources. 54
The literature related to different noise sources are discussed in the below sections.
Noise from hospital equipment/instrument
There are many hospitals equipment that are responsible for generating high level noise i.e. surgical instrument, instrument used in ICUs, power generating units, fans, printers/scanners etc.
According to Chen et al. 55 some irregular activities can produce noise more than 90 dB-A e.g. drilling or powered surgical instruments, surgery activities and clean up. According to Sellers 56 communication system is a noise pollution source that should be a very serious consideration before the installation of any communication system. Madalena and Nelio 12 studied and found that subjective well-being is more concerned for hospital noise and specially the noise from clinical source e.g. infusion pump, monitor and other equipment. Falcke et al. 57 studied the noise from various components of the equipment by frequency analysis and found that the noise level was high during routine work and low in dangerous situations. Gray and Philbin 58 studied the sound measuring instruments which are also the noise sources while using them. The objective is to give informal training on how to use these different devices and understand their measurements. Orellana et al. 50 studied hospitals noisy environments, the noise level was observed higher in an emergency department where the moving equipment was the main source of noise. Jue and Roberts 59 studied noise sources and found that the most of the patient’s disturbances are created by the machines. There are increasing medical equipment in ICUs which makes the noise and a major source of noise. In which the alarms create the most irritating noise. 11 Most of the nursing staff members talk to the visitors/other staff members or family members of the patients and to each other is the main noise source; however, conversation to the family members of the patient or visitors and noise from game playing by children are the two main sources of noise. 10 However, maximum visitors and patients requested that opening and closing of doors and patients crying or moaning are also the two main noise sources inside the wards. Other noise sources outside the wards are renewal of hospitals, conversation of visitors or patient’s family members, shouting of nurses and opening or closing of doors. 10 Sellers 60 studied the hospital noise levels in workstations and clinical laboratory. They found that the laboratory instrument creates the noise, so the specification of the instruments should be kept in such way that the noise level be minimum as possible.
Noise from impact on floor
There are presently no norms that deals with impact noise in rooms from falling stuffs that may be a more concern than walking noise. 61 Noise is generated in the rooms due to walking on floors in buildings. 62 Hee 63 examined the noise effects on people using two methods e.g. psychological and physiological. The impact noise on floors was generated by a standard impact ball and five other actual impact sources like footsteps of human and dropped stuffs.
Noise in ICUs
Generally, the noise levels are found high in the ICUs. World Health Organization (WHO) guidelines suggest that the hospital noise levels should be around 35 dB-A during the daytime and 30 dB-A at nighttime. 64 The noise in the ICU is the current research area for the researchers of different fields like equipment/instrument design, tools design used in the ICU and ICU design. Many studies were done for hospital noise measurement in the ICUs to know the sources of noise and their effects.65–67 According to Khademi 68 the sound level was maximum in the most of wards in the hospital which was around 85-86 dB and found 94 dB in the ICU just in single measurement. The average sound level in all wards was 60.2 dB. The average sound levels in ICU and emergency wards were recorded higher noise level than the standard. MacKenzie and Galbrun 69 did a complete and systematic analysis of sound sources and levels which was carried out in two ICUs. In this analysis many noise sources were found. Their research shows that 34% of these noise sources are completely avoidable and 28% are avoidable to some extent. Konkani and Oakley 70 examined ICUs noise to know the sources and the effects. In their review article, they analysed 29 existing investigations related to ICUs noise. Their study shows vital prospects to improve methods to study of the noise levels and to reduce the ICU noise. Tsiou 70 investigated noise level and their sources in the ICU of six beds in Athens, Greece. He specifically designed questionnaires and ten patients in which six males and four females completed the task. The questionnaires were conducted, and no reliable information was obtained. The ICU noise levels were found greater than the recommended hospital levels. Balogh 11 studied the increasing number of medical devices in ICUs. These devices make noise as a major stressor. Also measured the noise level of the alarms of various appliances. Sound level was approximately equal during the daytime but at night it was around 60-65 dB-A and peaks up to 96 dB-A. Most alarms noise was recorded as 60-70 dB-A but some exceeded 80 dB-A. During teaching rounds, the level exceeded 65 dB-A. Johansson et al. 71 studied noise level in an ICU for two objectives first was quantitative and second one was qualitative. Akansel and Kaymakçi 72 measured the noise in the ICU at certain locations and determined the disturbance to patients. The investigation was carried out with patients of 35 coronary artery bypass graft surgery. Their results show, noise levels recorded and found a mean of 65 dB (A). The peak noise levels were measured as 89 dB-A. The noise levels measured at different locations were not varied significantly. Stanchina et al. 23 studied the noise in ICU and found that peak noise was not the main basis of sleep disturbance in ICU. Different alarm systems of medical devices in ICU were investigated for noise measurement and analysis.73,74 Bitan and Connor 73 studied different sensors data to predict the alarm value in ICU. According to Darbyshire and Young 75 noise was measured in the five adult ICUs. They applied a strategy and collected sample values to record sound levels produced by equipment/apparatus and outside noise in a vacate side room of ICU. The average sound levels value was 45 dB-A however for 50% of the time the sound level exceeded and found between 52 and 59 dB-A in individual ICUs. According to Duarte et al. 43 the ICU key noise source was the own team and found that the sound levels were greater than the recommended. The paediatric intensive care units pay to poor sleep due to noise and may increase the danger of rising delirium. 76 Milette 8 measured baseline of the noise level in an NICU and compared it to the approvals of international bodies. Stafford et al. 77 measured noise in ICU and discussed about the main source of noise. According to Terzi et al. 49 ICUs have noisy atmospheres, which may have adverse effects on nurse’s psychology. Christensen 45 measured, investigated and compared the noise levels in a 9-bedded general ICU. His findings of noise level analysis indicate the average value 56.42 dB-A within this clinical area with serious peaks of 80 dB-A. The lowest noise level reached was that of 50 dB-A. Due to high technology and activity, noise level in the ICU is increased. 78
Noise in operating room/dental practice
Generally, the operating rooms work with high noise exposer due to the instruments in the operating room. This may carry hearing loss risk for the surgeons. 34 Nott and West 79 studied orthopaedic theatre noise and found its major health effects. McLaren and Armstrong 80 measured noise level on three wards A, B, C, and a surgical unit. The frequently of the noise exceeded 80 dB (peak reading) on all the wards during the day. Their results exceed the WHO guidelines at all times. Nassiri and Golbabai 35 studied the noise levels and related problems with the use of air-turbine drills in dental practice. The results show that the noise level produced by the high-speed drills was 69.1 dB. ZT et al. 81 used Dual-channel, handheld analyzer and sound level meter (Type 2270; Bruel & Kjaer, Naerum, Denmark), and conducted a survey of questionnaire and noise measurements in the dentistry clinics in Hong Kong. Sound pressure level was acquired at sixty places around the hospital working areas and sound spectrum analysis was done. The mean values of noise were observed 62.6 dB-A and 67.7 dB-A in the dental clinics and laboratories respectively. These equivalent continuous sound pressure levels were observed below the limit of 85 dB-A (e.g. 8 h/working day without any hearing protection) for affecting the hearing loss”. Prabhakar et al. 33 studied the effects on a surgeon’s hearing. The measured noise levels were analysed and found that noise levels exceeded 85 dB. Yarar 82 studied noise level for three days namely on Tuesday, Friday and Saturday at the different locations such as operating room, clinic and outpatient departments. Their result shows the noise level 81.25 ± 3.21 dB which was the highest average noise level at the hospital and the 52.51 ± 2.37 dB was the lowest noise level. Further, the outpatient department had the higher noise level than operating room and clinics. Akansel and Kaymakçi 72 measured the noise levels at some places of an ICU and found that the noise level was not varied significantly. The most alarming noise sources were the noise produced by patients, patients coming from emergency room/operating room into ICU, alarms, and staff talk/conversations. Kracht et al. 83 studied the noise level in the operating room. They monitored sound pressure levels at different intervals e.g. before, during, and after operations. The data were analysed to measure sound levels at background, frequency distribution, average equivalent sound pressure levels, and peak sound pressure levels. After averaging sound level data of many surgeries, an orthopaedic surgery had the maximum equivalent sound level of approximately 66 dB-A. The other surgeries e.g. Neurosurgery, cardiology, urology, and gastrointestinal surgery had the sound pressure levels from 62 to 65 dB-A.
Noise from alarms in hospital
Now a days in every hospital, alarm systems are installed for many purposes. Balogh 11 studied about the rising numbers of technical devices used in ICUs. It was observed that SPL roughly recorded almost same throughout the day/night, between 60-65 dB-A and peak values were obtained up to 96 dB-A. Bitan and Connor 73 studied data obtained from various sensors to predict the alarm noise value in ICU. Imhoff et al. 74 studied the smart alarm devices in ICU and observed the noise effects on patients. Hasanain et al. 84 studied the effects of alarms on auditory systems of humans. Edworthy and Hellier 85 studied the effects of medical alarm on behaviour of human. Edworthy et al. 86 studied the hearing problems due to alarms and established the medical device standards.
Noise control in hospitals
Noise can be controlled by applying different strategies that are suggested by researchers. Generally, noise is controlled at source or in the path of sound travel. The noise on a maternity ward is harmful to the healing process for mothers and their new-borns. In this case, the healthcare providers need to develop the atmosphere for these patients.
Adatia et al. 39 studied how to control maternity ward noise level and their study also offers recommendations on how to minimise the noise levels on a maternity ward. Gallo 87 studied the noise source in neonatal hospitalization environment and developed a noise control system. Engleman et al. 88 measured the noise and analysed the effect of the program conducted in a paediatric operating theatre for noise-reduction. Noise pollution effects were observed in the theatres. Sound level measurement was carried out in the theatres by adopting the guidelines, providing educations and using technical devices before and after a noise-reduction program. Monazzam and Nassiri 89 investigated on the acoustic performance of diffuser barrier. The whole performance was improved by the above diffusive barrier and was predicted 5.8 dB-A less than its other diffuser barrier known as rigid equivalent barrier. Ahamed et al. 90 did quality improvement research and their objective was to reduce the average noise level of a neonatal ICU by 10% during a year from the baseline. The average sound level was reduced from 62.4 dB to 56.1 dB and the peak value of sound level was reduced from 115 dB to 76 dB during a year. Kawai et al. 76 studied noise pollution in paediatric ICU. The aims are to build up a delirium bundle to reduce noise level and to measure the effect of the delirium bundle on nocturnal noise pollution. Delirium bundle is the bundle approach of delirium risk factor reduction by delirium monitoring or management, which includes reorientation, improving sleep and wakefulness, as well as reducing hearing and/or visual impairment, etc. The utilization of the paediatric delirium bundle managed to a significant noise level drop. The aim of Kol et al. 91 was to evaluate the efficiency of noise reduction approaches in the ICU. The sound pressure levels were determined before and after applying noise reduction strategies and found as 67.6 dB-A and 56 dB-A. The reduction strategies were effective in getting down the noise in ICUs. Konkani and Oakley 67 examined noise level in ICUs to find the noise sources and their effects. For reducing the noise level, they described best practices and common problems related with noise level reduction. Luetz et al. 92 analysed sound pressure level and reduced to some extent. By seeing all available studies, they redesigned the two rooms of the ICU with the goal of examining the noise level for reduction. They presented the possible solution of sound pressure levels reduction using architectural modifications. Wang et al. 93 studied and compared sound levels in dB. The sound-activated noise meters look effective in decreasing sound pressure levels in patient regions. Jue et al. 59 studied noise reduction in hospitals. Their objective is to do investigation on noise level reduction strategies such as suggestions, staff training and design improvement of hospitals. Hasegawa et al. 94 investigated difficult noise sources and gave a plan for controlling hospital noise which was less related to specific noise source. Oleksy 95 suggested refining the soundscape that can start by staff training for noise decrement, implementing noise reduction plans, alarm re-design and increasing research to estimate the parameters which produce noise on the soundscape of the hospital. The objective of Gallo 87 was to present an application of a noise control system that covers training parts to control the certain sources of noise in hospital. For this, they implemented number of strategies e.g. surveys, observations, procedures, electronic control devices and a training program. After that all sources were recognized but some of them can be eliminated. Noise control device was designed and installed, and training was provided to the staff for this noise reduction program. According to Chen et al. 55 measured sound pressure level shows that some activities at irregular intervals can produce sound pressure levels beyond 90 dB-A i.e. preparation for surgery, powered surgical instruments (drilling) etc. They suggested some methods during purchasing the instruments of noise level measurements. The noise exposures can be reduced by powered surgical instruments using preventive maintenance. Other methods to reduce interventions of noise level are playing music at a low volume and using some devices for hearing protection. Sellers 56 indicated that the noise pollution should be a very serious consideration before the installation of any communication system. They also like to encourage the vendors to agree to take responsibility when placing the equipment in the hospitals and set the specifications. Iyendo 96 studied the impact of sound disturbances on mental health. Their study shows that pleasant sound can protect mental health e.g. ocean waves and singing birds revealed benefits of stress recovery in patients and staff. Kahn et al. 97 modified the ICU design for noise levels reduction. 98 Their study also shows that it is possible to decrease the sound levels in an ICU greatly through a behaviour modification program. The baseline sound level in the NICU continuously exceeds the guidelines, but optimum design of NICU and noise reduction approach is needed to decrease the noise levels. 99 It is also important to increase the knowledge of nurses and increase their awareness regarding noise problem.99,100 Karen et al. 101 suggested to the health care providers, and hospital administrators of NICUs to identify the changes and optimize the implementation for reducing the noise level.
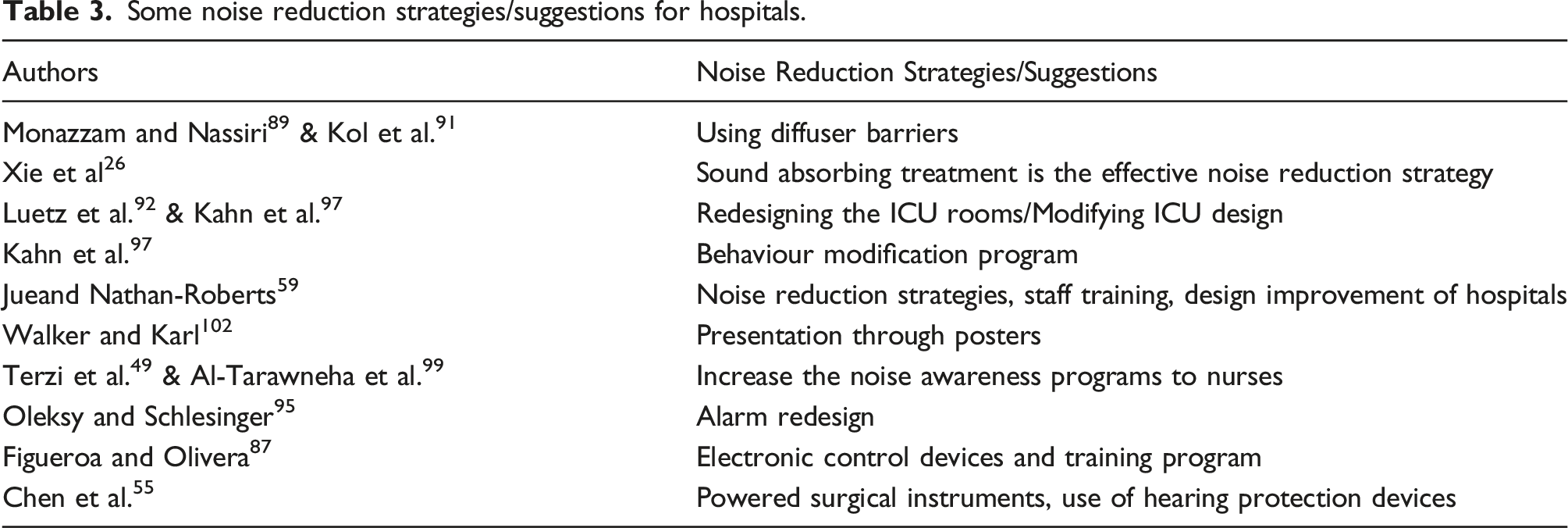
Some noise reduction strategies/suggestions for hospitals.
Conclusions and future research scope
This review paper concludes the aspect of good hospital design for low noise level, survey of noise levels in hospitals, different noise sources in hospitals, effects of hospital noise on human and noise control strategies for hospital environments.
It is concluded that the noise is responsible for many effects on human that are stress, hearing loss, annoyance, sleep disturbances, physiological dissemination, anxiety, comfort, fatigue, high blood pressure, poor mental health, fluency of speech and communication, recovering from anaesthesia and effects on newborn children.
There are numerous hospital noise sources such as noise from hospital staff, family members of the patients, walking sound of hospital staff and patient’s family members, hospital equipment, surgery equipment, alarm system, elevator bell sound, generator sound, opening and closing of doors, fans etc.
There are some noises controlling strategies that suggested by many researchers such as installing noise controlling system, organise noise reduction programs i.e. staff education about noise, rules, technical devices, noise isolation barriers, hospital soundscape, change alarm design and quit posters on wall. However, Hospital site selection, building design and room design is the first step for low noise level hospital.
The noise level is higher at daytime than nighttime and the high noise locations in the hospitals are reception area and corridors. However, ICU noise level is also observed beyond the limit that should be minimised.
The future research on noise pollution in hospitals are needed for controlling the noise in hospitals by redesigning hospital equipment, surgery equipment, sound absorbing system, alarms, hospital specific elevators and provide education to staff, patients and patient’s family members about noise pollution and its effects on human. An active noise control system design could be a good solution to control the hospital noise.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.