
Abstract
The use of markets and market mechanisms to deliver care services is growing in both liberal and social democratic welfare states. This article examines debates and policies concerning the marketisation of eldercare and childcare in Sweden, England and Australia. It shows how market discourses and practices intersect with, reinforce or challenge traditions and existing policies and examines whether care markets deliver user empowerment and greater efficiency. Markets for eldercare and childcare have developed in uneven and context specific ways with varying consequences. Both politics and policy history help to shape market outcomes.
Introduction
The use of markets and market mechanisms to deliver care is one of the most significant and contentious ways in which welfare states have been transformed (Gilbert, 2002). The establishment and extension of public services (or publicly subsidised non-profit services) was central to post-war welfare states. Since the 1960s, the demands of women’s movements and other actors for ‘recognition, rights and redistribution’ of care responsibilities were focused squarely upon the state (Williams, 2010). In the last quarter of the 20th century, enthusiasm for neo-liberal ideas about competition and choice, together with increasing pressures on public finances, have led many governments to adopt policies that foster markets in care and encourage for-profit providers. Market-oriented policies construct care users as consumers and care as a commodity to be bought and sold. In this new political imagery, the citizen (associated with politics and the public realm) is overshadowed by the consumer (assumed to be a self-interested individual embedded primarily in economic relationships) (Clarke et al., 2007).
In this paper we seek to illuminate the discourses, processes and outcomes of care marketisation by exploring the arguments that have been deployed and the policies that have been introduced to bring about varying degrees of marketisation of childcare and eldercare in Sweden, England and Australia. Childcare and eldercare are critical domains of contemporary social policy closely connected to the ‘new social risks’ confronting welfare states as more women enter the labour force and populations age in post-industrial economies. In these three countries – one social democratic and two liberal – childcare and eldercare have contrasting histories and patterns of provision, enabling us to identify variations in how markets have been promoted, defended and criticised in each domain.
Sweden is a Nordic social care regime characterised by extensive public provision for children and older people based on a commitment to universalism (Anttonen, 1990). Market principles and private for-profit providers represent a major challenge to Sweden’s traditions. Although England and Australia are both liberal welfare regimes, they have quite distinct histories of care provision. Australia has a strong tradition of delivering eldercare and childcare through publicly subsidised non-profit organisations; in England, local authority provision dominated eldercare until the early 1980s, while childcare did not reach the national agenda until the late 1990s. These contrasting histories illustrate salient variations across both domains of care within the liberal group.
Care markets for children and adults operate alongside other systems of service allocation and delivery; rarely if ever are they the ‘only game in town’. Building on the analysis of home care developed by Burau et al. (2007: 31) we observe four ‘logics’ in eldercare and childcare, each based in a particular set of institutions, which correspond to the four points of Razavi’s (2007) ‘care diamond’: the logic of market provision concerned with profit-seeking through competition; the logic of state provision to meet citizen’s social rights operating through formal/public institutions and state bureaucracies; the logic of associations working through formal/private/non-profit bodies whose rules originate in ethical norms and codes; and the logic of informal, private family provision whose rules and practices are embedded in moral/personal obligation and emotional/social relations.
We explore the growing influence of market provision and market thinking in eldercare and childcare in all three countries, showing that the arguments deployed for marketisation, and its impact, depend upon the balance between the different logics of care prevailing in each country and each sector. In the following sections we outline the different ways in which markets in eldercare and childcare have been introduced, the discourses and policy objectives used to justify them and the outcomes to date. We locate these developments within broad national traditions and cultures of care and consider the extent to which marketisation is shaped by the scale and strength of other forms of provision such as state-provided care and services provided by non-government organisations.
We begin by defining marketisation and outlining the arguments made for markets as well as some criticisms of those arguments. With the theoretical terrain established in the second section, the third section describes the processes of marketisation, separately for elder- and childcare, locating the arguments deployed to support markets in each domain within national political and policy contexts. The fourth section then links our findings to the theoretical issues raised in the second section and assesses whether care markets are delivering what has been claimed for them. Finally, we offer some conclusions about variations in the arguments put forward for marketisation in childcare and eldercare across our three countries. We show that marketisation takes root in particular ways in each sector and country (cf. Sipilä et al., 2003). Even when marketisation is oriented to similar policy goals, the arguments used to promote it and the mechanisms by which it is implemented are influenced by local histories and practices (Pavolini and Ranci, 2008).
Care markets
We use the term marketisation to refer to government measures that authorise, support or enforce the introduction of markets, the creation of relationships between buyers and sellers and the use of market mechanisms to allocate care. Marketisation takes a variety of forms including contracting service delivery to private providers (both for-profit and non-profit), financing users to purchase services in the market, mandating insurance against social risks such as the need for long-term care, and providing cash allowances or tax concessions to enable the employment of carers in the home. Subsidies and instruments are often designed to shape consumer behaviour. For example, vouchers may be redeemable only from certain kinds of providers, or their value may be set so low that recipients turn to low-paid workers, including migrants or continue to rely on family carers. In some cases, service users may be permitted to top-up public subsidies by purchasing additional, or higher quality, services through private financial contributions.
The promotion of markets in care is part of a broader suite of changes in state–society relations. Using the arguments of neo-classical economics, proponents suggest two main types of benefits that should flow from delivering services through markets (Blank, 2000; Greener, 2008). First, giving service users (or their agents) purchasing power should empower users by enabling them to exercise consumer sovereignty. Second, this should improve the quality of services and reduce costs to purchasers, by forcing providers to compete for business. Thus, markets should ‘compel producers to serve the public interest by providing goods and services that are efficiently produced, of reasonable quality, and at prices that are close to costs’ (Cleveland, 2008).
Market provision promises empowerment through the exercise of choice and more efficient provision; higher quality services delivered for lower cost to the consumer, and ultimately to the taxpayer if services are funded wholly or partially by the state. For markets to function in this way, however, certain conditions must be met: information about the price and quality of competing suppliers must be freely available to consumers; the costs of changing supplier must be low; and suppliers must operate in a competitive market. These conditions do not all apply to markets in care (Land and Himmelweit, 2010).
To be empowered, consumers must be able to assess the price and quality of services and make choices on the basis of their assessments. In practice, consumers find it difficult to make accurate judgements about the quality of care (Morris and Helburn, 2000; Vincent and Ball, 2006) and there are many reasons why they may not be able to act on the basis of their assessment. Decisions about purchasing childcare or eldercare are made infrequently, often at short notice and under pressure. The same frailty and dependence that creates the need for care may limit consumer sovereignty (Eika, 2009).
Quality differences are inherent in market provision; indeed it is through such differences that markets are supposed to promote efficiency. However, making use of market information requires skills that are not equally distributed: an increased focus on choice favours those with more resources and education, who have considerable advantages in navigating the system (Eika, 2006). Where the market provides for both privately and publicly funded care, or care recipients are expected to top-up public funds through their own resources, those with greater resources will be able to purchase higher quality. Markets almost inevitably therefore lead to increasing inequality in the quality of care.
Further, for quality control through the market to work, consumers must be able easily to switch poor quality providers for higher quality ones. However, continuity of care is important both for children and older people, particularly in residential care, so that exit can be too costly a strategy when quality is found to be inferior. This critically limits the effectiveness of market mechanisms in ensuring care quality (Eika, 2006; Plantenga, 2010).
In recognition of these problems, governments may seek to aid transparency and effective choice through regulation, accreditation and the provision of information about how individual services perform against standards. Inevitably, such standards capture the most easily quantifiable aspects of care rather than the less tangible, relational features that are of such importance to care recipients and their families (Wærness, 1984). Because these intangible aspects of care are difficult to measure, monitor and regulate, they are likely to be sidelined by providers in the pursuit of cost control (Gilbert, 2002).
Finally, for markets to deliver high quality services and reduce costs, suppliers must operate in a competitive market. However, not only are there economies of scale in care provision, government policies may encourage provider consolidation and market concentration to reduce the costs of regulation and accreditation per unit. Where markets become too concentrated, competition no longer improves efficiency (Scourfield, 2007). Providers with too much market power can set their own prices, raising costs to government and to service users.
Since the wages of care workers form a high proportion of the costs of care, competition lowers costs only if staffing ratios are reduced or less qualified staff are employed, both of which tend to reduce quality. However, quality considerations may be more easily put aside in care markets than in markets where quality is more easily observable. This raises important issues for the labour market (see Williams, 2012). Since care markets deliver efficiency at the expense of workers’ pay and conditions, care workers tend to be drawn from more vulnerable groups in society: traditionally women and, increasingly in eldercare, migrants (Shutes and Chiatti, 2012).
These are the main arguments that have been debated by market enthusiasts and their critics when the issue has been the benefit of private over public provision. In some cases, marketisation has also meant encouraging the entry of for-profit providers into sectors previously dominated by, or reserved for, non-profits. The latter, by definition, are motivated by norms other than profit. Providing opportunities to make a profit from care provision will not necessarily generate supply by non-profits since they may be unwilling to offer care for a subsidy that is too low to cover the quality that they find acceptable. In such situations, provision can be expanded more cheaply by allowing for-profit providers into the market. For a commodity such as care, whose quality is hard to assess without direct experience, non-profits are likely to be more trusted to use higher fees to produce higher quality. Where the market is sufficiently differentiated that there are some purchasers willing and able to pay for higher quality care, that higher quality care tends to be provided by non-profits, while for-profits provide lower quality care for lower prices (Cleveland, 2008).
Governments have increasingly promoted the ‘logic of the market’ in eldercare and childcare. However, marketisation is a highly context specific process: it had a distinctive starting point and was designed to bring about particular effects in each sector and country. In the next section we examine the arguments used to justify the marketisation of eldercare and childcare and the processes by which it was advanced.
Processes of marketisation
Eldercare
England was the first European country to marketise social care services. After patchy success in encouraging local authorities to contract out home-care services voluntarily, in 1990 the government forced the creation of a market (Pavolini and Ranci, 2008: 251). This resulted in most public provision being contracted out to the for-profit, rather than the voluntary, sector (Land and Himmelweit, 2010: 11). In 2011, as Table 1 indicates, three-quarters of England’s residential care facilities and home-care services were run by for-profit providers (Care Quality Commission, 2011).
Eldercare provider mix: Australia, UK and Sweden, latest available figures (2010/11)
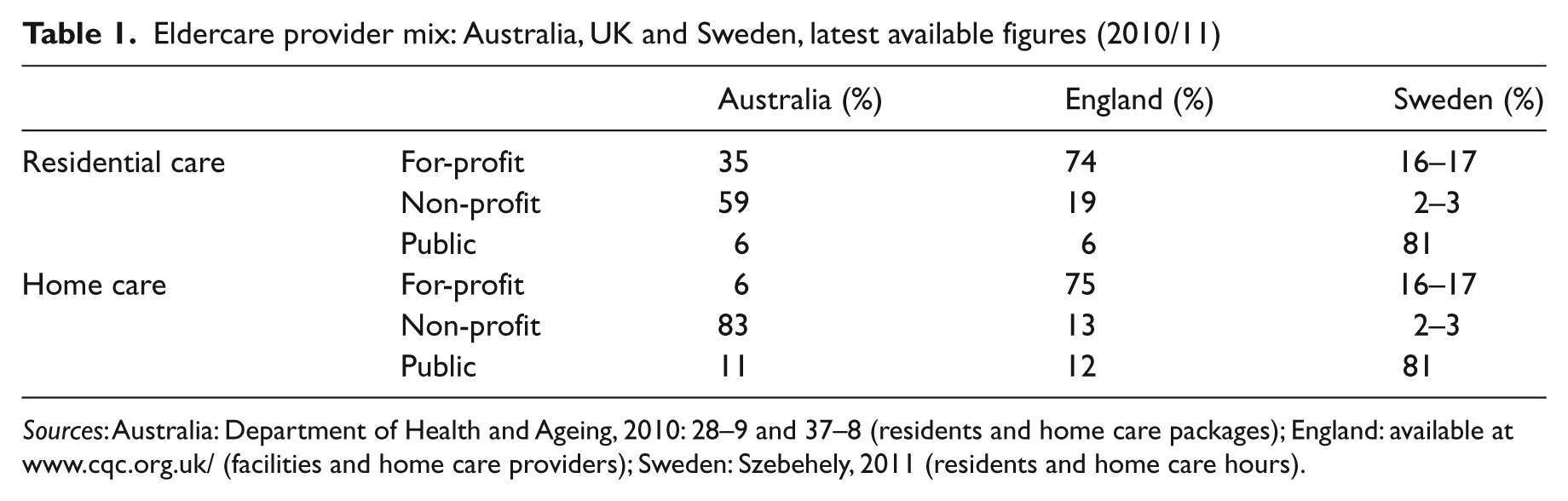
Sources: Australia: Department of Health and Ageing, 2010: 28–9 and 37–8 (residents and home care packages); England: available at www.cqc.org.uk/ (facilities and home care providers); Sweden: Szebehely, 2011 (residents and home care hours).
After 1997, increasing numbers of service users had the option of receiving direct payments to purchase their own care, but take-up remained low, especially among older people (Baxter at al., 2011). In 2007, the Government announced the roll-out of individual budgets to be controlled by users even if not taken in the form of cash, for everyone in England eligible for publicly funded adult social care. The post-war state logic of local authority provision was thus superseded by a nationally mandated shift towards constituting service users as consumers exercising choice (Baldock, 2003; Baxter at al., 2011). While located in the discourse of giving those dependent on the public purse the same rights to consumer choice, empowerment and service flexibility as those who purchase services privately, this policy also favoured market mechanisms as the best route to cost containment and increased quality of care.
In England, the framing of care users as consumers has added the personal dimension of quality to arguments for the introduction of market mechanisms centred on provider competition delivering value for money. Therefore, the logic of marketisation, involving a shift from public to market provision, is paradoxically accompanied by strong advocacy for users’ and carers’ social rights (Burau et al., 2007: 166), including rights for the publicly supported to make consumer choices.
Marketisation of eldercare services started later in Sweden, but drew upon similar arguments. Sweden’s post-war tradition of class solidarity made public provision more difficult to dislodge; most services are still publicly financed and publicly provided (see Table 1). Nevertheless, the introduction of a new Local Government Act in 1991 allowed municipalities to outsource some services, including tax-funded eldercare, to both for-profit and non-profit organisations. The arguments for marketisation focused initially on improving quality, but, with the recession of the early 1990s, they moved more to cutting costs through price competition (Blomqvist, 2004).
While for-profits provided less than 1 percent of Swedish eldercare at the beginning of the 1990s, that sector now accounts for 17 % the non-profit sector remains marginal at 2–3 percent (Szebehely, 2011). Behind these national averages there are large local variations: more than 50 percent of eldercare in and around Stockholm is provided by private for-profit firms, while a majority of the municipalities have no for-profit providers. As a result of generous funding and light regulation, the Swedish care market has become very attractive to investors. Two corporations owned by international private equity companies own half of Sweden’s private eldercare market (Meagher and Szebehely, 2010). That marketisation in Swedish eldercare started with competitive tendering for large nursing homes and geographical areas of homecare, rather than with a customer choice model, is important in explaining the oligopolistic structure of private sector provision.
Partly as a response to the tendency towards oligopoly, an ‘Act on Free Choice Systems’ was introduced in 2009. Encouraged by state incentives, by 2010 more than half of Sweden’s municipalities had decided to introduce customer choice models in eldercare, compared with less than 5 percent in 2003. Despite the strong tradition of highly independent municipalities, the Swedish centre-right government is considering legislation, similar to that passed in England, to compel all municipalities to introduce private alternatives and user choice by 2014 (Szebehely, 2011). The government continues to express strong hopes for the positive effects of choice by asserting the right of users ‘to choose and choose again’.
In contrast to Sweden and England, Australian home and residential eldercare services have been provided mainly by non-profit organisations (religious, community-based and charitable), whose associational logic of care provision has been dominant since the latter part of the 19th century (Murphy, 2011: 29) (see Table 1). Australian governments have mainly been funders and regulators rather than service providers, determining the number of places to be operated in particular geographical areas and letting tenders for non-profit providers to run them. For-profit providers have been important players in residential eldercare since the 1960s, through their ownership of high-care nursing homes, a sector they continue to dominate (King and Martin, 2009). Australian governments have progressively increased the role of market mechanisms in the provision and allocation of residential care places (Howe and Healy, 2005) and competitive tendering through regulated markets has become the core mechanism for home-care services (Fine, 2007).
Care purchased directly by consumers using government-provided payments or entitlements is less prominent in eldercare in Australia than in England or Sweden (Fisher et al., 2010), but a strong consumer movement and powerful official voices, particularly the Australian Government Productivity Commission (Australian Government Productivity Commission, 2011), now argue for its introduction. They rely strongly on the argument that empowerment through consumer choice among competitive independent providers is most likely to ensure adequate, flexible, high quality supply.
To sum up, increased penetration of the discourses and processes of marketisation is evident in eldercare in all three countries. In Sweden and England, policy priority is given to greater consumer choice, with service users increasingly constituted as consumers demanding higher quality service (market logic), rather than citizens bearing social rights (state-provider logic) (Burau et al., 2007: 149). These consumer-centric arguments are situated in a political context calling for greater efficiency and cost containment in the expenditure of public funds. Australia has no history of social rights to services and limited reliance on publicly provided eldercare services. Opening up a quality-regulated market through contracting-out, tendering and commissioning, by allowing competition between for-profit and non-profit providers has been promulgated as expanding the supply of services, controlling costs and more latterly providing flexibility, higher quality services and consumer choice.
Childcare
With ‘ever more children at ever-earlier ages and for ever-longer hours’ participating in early childhood education and care (ECEC) (United Nations Children’s Fund, 2008: 3), the contending logics of state, market, family and non-profit provision are in constant tension in this policy domain. Governments’ growing interest in delivering services through market mechanisms emerged at the same time as recognition of the benefits of high quality ECEC in providing cognitive, emotional and social benefits for children, especially those from disadvantaged backgrounds (Organisation for Economic Co-operation and Development, 2006). Yet there has been little debate about the compatibility of these goals.
Sweden’s ‘educare’ system is internationally renowned. Gender equality is an important foundation of the system, as are the needs and rights of children. Municipalities must provide a full-time childcare place for all children whose parents are working or studying, while children of unemployed parents and those whose parents are on leave are eligible for 15 hours of childcare per week. In keeping with Sweden’s commitment to universalism, children from immigrant backgrounds and those whose parents are poorly educated use tax-funded services to the same extent as children from more privileged families (National Agency for Education, 2007). As noted below, however, this does not necessarily mean that children from all backgrounds use the same services.
Despite its strong history of public provision, Sweden was the first of the three countries to debate the marketisation of childcare. In 1983, as part of a broad challenge to publicly provided services, the Swedish Employers Federation proposed setting up for-profit childcare centres. Social democrats responded that for-profit care would threaten quality and lead to class-based segregation; they introduced legislation to render for-profit childcare ineligible for taxpayer subsidies. Prime Minister Palme described for-profit childcare as ‘part of the attack on the joint and democratically steered sector of our society’ (Government Bill, 1983/84: 7).
In 1991, a newly elected centre-right government proclaimed a ‘freedom of choice revolution’ and permitted extension of taxpayer subsidies to for-profit childcare providers, if agreed to by the municipality. In a break with Sweden’s egalitarian traditions, private childcare providers were permitted to charge higher fees than their public counterparts and to offer places to children not on the municipal waiting list (Government Bill, 1991/92). The Social Democrats returned to power in 1994 but did not repeal this legislation, and so since 1991 there have been no restrictions on for-profit providers in childcare, schools, eldercare or care for disabled people within Swedish tax-funded welfare services. National legislation in 2006 has further entrenched private provision as the municipalities lost their right to prevent private companies setting up publicly subsidised childcare centres.
Compared with eldercare, for-profit providers have a more limited role in Swedish childcare: 8 percent of childcare places are operated by private, for-profit organisations and 11 percent by non-profit providers, mainly parental or staff cooperatives (see Table 2). As with eldercare, there is significant local variation. Further, private services are being used more by better-off families, potentially undermining the solidarity of the Swedish system (National Agency for Education, 2007). Thus, despite its relatively small scale, marketisation in Sweden has introduced cracks in a decades-long tradition of childcare as ‘a meeting-place for children with different ethnic, cultural and social backgrounds’ (Government Bill, 1999/2000: 8).
Childcare provider mix: Australia, UK and Sweden, latest available figures (2010/11)
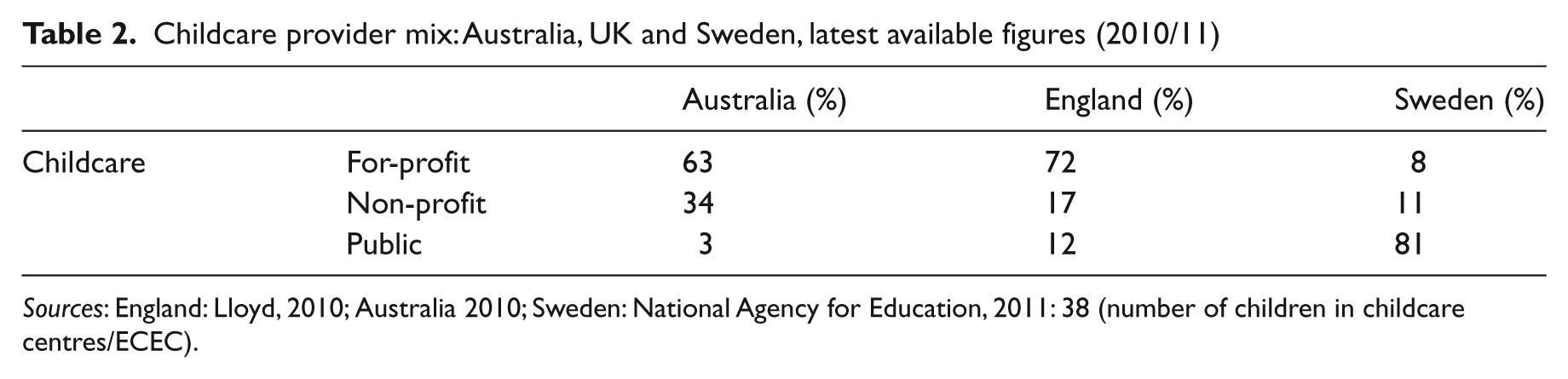
Sources: England: Lloyd, 2010; Australia 2010; Sweden: National Agency for Education, 2011: 38 (number of children in childcare centres/ECEC).
In England, by contrast, the introduction of market principles into ECEC has served primarily to expand supply. Until the late 1990s, with the exception of local authority nursery care for children deemed needy or vulnerable, childcare was regarded as a private, family responsibility. From 1997 to 2010, there was rapid policy development and substantial investment in ECEC services. The Childcare Act 2006 required local authorities to ‘close the gap’ between the most and least well off children by providing early years education and care. Firmly based in the logic of the market, the Act stipulated that priority must be given to private providers, with local authority provision a last resort (Lloyd, 2010: 6).
Means-tested tax credits were used to encourage a market of private, voluntary and independent providers. For low–middle income parents in employment, 70 percent of the costs of childcare up to a limit are refunded, and there are tax breaks for better-off employees. England experienced a 70 percent increase in private, for-profit childcare between 2002 and 2010 (Lloyd, 2010). For-profit services now account for 72 percent of UK early education and care (see Table 2). Before the recession, there was strong market consolidation with a number of nursery chains listing on the stock market either as ‘stand alone’ companies or elements of diversified corporations. Recently, concerns have been raised about the capacity of England’s mixed economy to deliver universal, high quality provision (West et al., 2010) and to address the priorities and values of black and minority ethnic communities (Focus Institute on Rights and Social Transformation, 2004). A recent study notes that even ‘skilled and privileged middle-class consumers’ find the system difficult to navigate and ‘have to deploy the full range of capitals available to them, economic, cultural and social, to achieve their purposes in this market’ (Vincent and Ball, 2006: 162).
The marketisation of childcare in Australia, as in England, was primarily designed to expand supply, rather than to increase consumer choice. The logic of associations whose ethos was service to the local community, not profit, had been the dominant logic of Australian childcare. Throughout the 1970s and 1980s the Australian government expanded the supply of non-profit services through a mix of capital grants to providers and fee subsidies to parents. Families who used for-profit services were not eligible for government assistance. In 1990, the Australian government extended fee subsidies to users of for-profit childcare arguing that this would, in the long term, reduce the burden on government since capital for new services would be provided by businesses rather than taxpayers.
The government’s strategy was to encourage competition between commercial and non-profit providers by subsidising consumer demand through a voucher (an entitlement to a given level of subsidy based on income and other family circumstances). Such subsidies greatly stimulated demand and opened up business opportunities. The voucher was seen as ‘a bonanza for business’ and ‘a license to get rich’ (Ferguson, 1996). Several childcare providers listed on the stock exchange and one of these, ABC Learning, rapidly took over its local rivals before expanding into overseas markets. At its peak, ABC owned 25 percent of all Australian childcare centres and was the largest publicly listed childcare provider in the world (Brennan, 2007). The company collapsed in 2008, putting at risk the care of 120,000 children and the livelihood of 16,000 staff in Australia alone. The future of the centres hung in the balance for over a year until they were purchased by a consortium of non-profit providers (Ellis, 2009). In the interim, the Australian government spent tens of millions of dollars keeping them open. Following the sale, the proportion of centres owned by non-profit providers rose from 22 to 34 percent (Australian Government, 2010).
As this brief survey shows, marketisation and the encouragement of for-profit childcare have had different goals, meanings and impacts in each country. Marketisation, while intensifying in each of the three countries (see Table 2), has been shaped by pre-existing patterns of provision or ‘policy logics’ (Burau et al., 2007). In Sweden, marketisation was introduced to challenge a public monopoly and extend choice. For-profit childcare still represents only a small proportion of the Swedish system, although its long-term impact is potentially significant in rupturing the logic of state provision. In England, subsidised parental choice in a market of private providers has been the vehicle to promote service expansion. In Australia, the aim of marketisation was to reduce the direct costs of service expansion faced by government by encouraging for-profit providers to enter the sector.
Applying market logic to care services
Have markets delivered the promised benefits of empowering users through increased choice and promoting more efficient care provision in the three countries?
Empowering users
Evidence emerging from the UK and Sweden suggests that consumer choice and individual budgets have not universally empowered frail older people (Glendinning, 2008; Svensson and Edebalk, 2010). Indeed some English research suggests that choice may be more of a burden than a means of empowering older people (Glendinning et al., 2008; Yeandle and Steill, 2007; Yeandle et al., 2012). Data on user satisfaction shows lower scores among elderly users than younger disabled people for both ‘improvements in mental well-being’ and ‘getting the support they need’ from using personal budgets (National Audit Office, 2011: 19, Figures 8 and 9). The quality of support available to personal budget users was found to be variable, with only around half finding it easy to get information and advice, and less than half finding it easy to choose care services or change providers (Public Accounts Committee, 2011). The same research found wide variations in the support offered to users by different local authorities. Nearly a third of respondents found the experience of being an employer daunting or difficult to cope with: ‘Whilst some users welcome having choice, many did not want the responsibility of organizing and coordinating their own care, and they were therefore prepared to trade off choice in favour of convenience’ (National Audit Office, 2011: 21).
As private providers have entered the field, home care tasks have become increasingly regulated, leaving the user with less rather than more latitude. The Eldercare Ombudsman in Stockholm notes that home care recipients who criticise their home-care provider to the local authorities may be asked to change provider. Since very few older people actually do change provider, consumer choice could leave older and frail users less rather than more empowered (Szebehely, 2011).
Consumerism and choice have had different consequences for different social groups and therefore constitute a challenge to Swedish universalism. Universalism is further challenged by the interplay between consumer-choice models and tax deductions for household services, introduced in 2007. Private providers of tax-funded home care services are allowed to offer extra services, enabling high income older people to top-up their needs-assessed home care services with services from the same provider, benefiting from the tax deduction and thus increasing inequalities in eldercare (Szebehely, 2011). Those with more educational resources have a greater chance of finding the best services; this, in turn, may amplify differences in the quality of care (Barnes and Prior, 1995; Eika, 2006; Swedish Agency for Public Management, 2009).
The slower take-up of market ideas in relation to eldercare in Australia may be related to the strength and visibility of a variety of non-profit providers, which provide the perception of choice. In reality, since the mid-1980s, the exercise of choice by older people and their carers has been limited by supply-side constraints on service provision and block-funding arrangements under competitive tendering and contracting. Although the Home and Community Care programme offers some service flexibility to meet individual needs, community care packages for very frail aged people, delivered by funded providers, are less flexible, with limits on both supply and funding. Market processes of competitive tendering have not at this stage increased older people’s opportunities for choice of service provider, either in home care or residential care. This is the policy terrain which the Australian Government Productivity Commission seeks to reform through expanded marketisation, bringing additional and diversified providers, including for-profit providers, into the arena and at the same time expanding the coverage of consumer-directed funding (Australian Government Productivity Commission, 2011).
In childcare, the rapid growth of for-profit providers in Australia, and especially the dominance of a single company, reduced the capacity of many families to choose a service of their preferred type. Previously, services were grounded in their local communities and managed by parents and staff. But the diverse non-profit childcare sector that predated marketisation gave way to a smaller number of commercial providers. Families increasingly face a market in which the main decisions are made not at the local level but in corporate headquarters. The situation is different in England where childcare services scarcely existed before the late 1990s and market mechanisms are associated with expanded service provision. However, in England, as well as Australia, the fundamental decisions about the direction of childcare policy are made by governments and providers, with little input from families and communities (Lloyd, 2010). For all the talk about ‘choice’ there has been a ‘remarkable absence of parental voice in the recent expansion of childcare’ (Vincent and Ball, 2006: 36).
In the Swedish context of full coverage of childcare it can be argued that parents have been empowered as they have got a greater scope for choosing between childcare centres with different auspices, but there is no empirical evidence that parents value such choice. Most parents choose a childcare centre close to the home irrespective of provider or profile, often with the argument that the child then will have friends in the neighbourhood. Some, often highly educated parents, want to be more engaged in the daily life of the childcare centre and therefore choose a parental cooperative, while others who cannot or do not want to spend time in the centre have to choose other alternatives (Bergqvist and Nyberg, 2002).
Promoting efficiency
Efficient provision of care means producing high quality at the lowest possible cost, thus making best use of limited resources. The logic of the market relies heavily upon the consumer to exercise quality control and to promote efficiency through choice and exit. This logic, however, does not take account of the ways in which care differs from other ‘products’. The transaction costs of switching eldercare and childcare providers are too high for many users to make market information useful; perversely, consumers can be locked in to continuing with a provider even when they have concerns about quality (Plantenga, 2010). This reduces the effectiveness of the market in promoting efficiency. Further, where publicly funded services are limited, choice is not always available. This is particularly problematic for low-income users who may lack the skills and resources necessary to make effective choices around quality. If those with more resources gain the best services, those with fewer resources are left with inferior services; for them the quality of services may actually decrease (Eika, 2006).
Large providers, including stock-market listed companies, have become dominant in many sectors of the care market by merging and buying up smaller providers. The Australian childcare market remains highly concentrated, even after the collapse of ABC Learning (Australian Government, 2010). As noted above, in Sweden, half the private eldercare market is in the hands of two corporations owned by international private equity companies. In England, too, the residential care sector is increasingly concentrated with recognised problems of dominance in some geographical areas (National Audit Office, 2011: 26/7). The childcare market is increasingly concentrated as well (Lloyd, 2010). When large providers fail, significant numbers of children or adults can be left without care, a moral hazard that governments cannot ignore. This happened when ABC Learning, the Australian-based childcare provider, failed. Over-confidence in an expanding market that came to an abrupt halt with restrictions in state funding for social care was the key factor in the collapse of Southern Cross, the largest provider of care homes in the UK, with 30,000 frail elderly residents across 750 homes. The National Audit Office (2011: 30) noted the absence of any policy to prevent or deal with future failures and their consequences for frail elderly people.
Little empirical data with respect to eldercare in the three countries support the hopes for cost containment expressed by market enthusiasts. Increased marketisation did not stop eldercare costs rising in England; there was an increase of 3 percent in real terms in the average cost of residential care for older people in 2008–2009 and 2009–2010 (Health and Social Care Information Centre, 2011: 18, Table 6.2). In Sweden after the first years of competitive tendering, costs do not seem to have fallen. Interestingly, many municipalities that have introduced choice models do not track whether competition has reduced public expenditure. As the Swedish Competition Authority (2009: 19) notes, this failure to collect information could be because the aim of introducing competition is often ‘political rather than economic’.
Does marketisation improve quality? Studies of eldercare in the US, Canada and the UK have shown that staffing ratios are lower in for-profit residential care than in non-profit facilities (Comondore et al., 2009) and the same has been found in Sweden (Stolt et al., 2011). The UK regulator, the Care Quality Commission (CQC), rated 13.4 percent of social care services provided by the private sector as ‘poor or adequate’, while only 8.1 percent of voluntary sector and 6.7 percent of local authority provision received such a low rating (Care Quality Commission, 2010: 39, Table C4). Similarly, in Australia an analysis of the health and care workforces in the residential aged care sector for 2003 notes that for-profit facilities had small but significant differences from others: fewer aged care workers per bed than non-profits and government-operated facilities, higher staff turnover and higher use of private agency staff (Martin, 2005). Martin attributes this partly to the fact that the for-profit services were predominantly high care facilities which tend to have these staffing characteristics, however, this finding is consistent with the view that creating profit from residential aged care tends to require that labour costs are minimised.
Evidence about quality in childcare also shows that non-profit services are generally of higher quality than those offered by for-profit providers. An evaluation of the UK Neighbourhood Nurseries Initiative (a programme aimed at expanding childcare provision in the 20 percent most disadvantaged wards in England) reported that ‘maintained’ nurseries (that is, those funded by local authorities and not run for profit) had the highest level of quality (Mathers and Sylva, 2007: 55). Evaluation of the UK initiative, Effective Provision of Preschool Education (EPPE) revealed that outcomes for children attending private day nurseries were lower than for children attending other service types. A report on childcare quality in the Millennium Cohort Study (a multidisciplinary research project following the lives of 19,000 children born in the UK in 2000/2001) showed that services maintained by local area authorities offered ‘higher quality provision in almost all dimensions measured’ (Mathers et al., 2007: 8).
An Australian study that measured childcare quality partly by the willingness of staff to place their own child in a service of a similar standard, suggested that quality is highest in non-profit services and lowest in those provided by large corporate providers, with independent for-profits in the middle, but closer to non-profits (Rush, 2006). Swedish evidence also suggests lower quality in private childcare facilities, in particular a lower proportion of qualified pre-school teachers: in public childcare centres more than half the staff (52 percent) are pre-school teachers with a university degree compared with 37 percent in private childcare centres. The data do not differentiate between for-profit and non-profit private centres. However, as for-profit childcare has displaced parental and staff cooperatives, staff qualifications in private childcare have declined significantly (National Agency for Education, 2011: 47).
Conclusion
This paper has drawn upon the analytical framework of four ‘logics’ in eldercare and childcare, each based in a particular set of institutions: the logic of market provision concerned with profit-seeking through competition; the logic of state provision to meet citizen’s social rights operating through formal/public institutions and state bureaucracies; the logic of associations working through formal/private/non-profit bodies whose rules originate in ethical norms and codes; and underpinning all, the logic of informal, private family provision whose rules and practices are embedded in moral/personal obligation and emotional/social relations (Burau et al., 2007). This analysis has been concerned with the dynamic and shifting interplay of the first three logics, those that are implemented in the arena of public provision, rather than private, familial provision.
We have explored the growing influence of market provision and market thinking in eldercare and childcare in England, Sweden and Australia, demonstrating that the arguments deployed for marketisation and its impact depend upon the balance between the different logics of care prevailing in each country and in each sector. Arguments for the marketisation of eldercare and childcare have been broadly similar in the three countries, but differently inflected. Resting on different institutional bases, and influenced by local histories and practices, the arguments for and processes of marketisation have developed at different speeds, depending on the political context and the problems that marketisation was expected to solve. Marketisation is therefore path-dependent with the initial balance of logics in each domain and in each country continuing to shape its form and pace.
The paper has explored arguments drawn from neoclassical economics, which proposes two main types of benefits that should flow from delivering services through markets: empowering service users by giving them purchasing power to support consumer choice; and reducing the costs of services, often focused on ensuring more cost-effective use of taxpayer funds, while simultaneously improving the quality of services through providers competing for business.
In exploring the ways in which these arguments have played out in the three countries, we found that in Sweden and England, and to an increasing extent in Australia, policy priority is given to greater individual choice in both elder and childcare markets, with service users (or their parents or carers) increasingly constituted as consumers. Market advocates claim that consumers demand greater choice of provider and higher quality services which can only be met by increased provider competition (by for-profit, non-profit and public providers, with emphasis on for-profit providers) and user co-payments to restrain costs to the state. We identify an ‘elective affinity’ between the consumer-centric and cost-containment arguments positioning market processes as the most cost-effective and efficient way to expand services. However, there is no firm evidence that either increased quality or lower costs have resulted from increased competition, marketisation and the increased penetration of for-profit services in childcare and eldercare.
Despite these common themes, there are differences between elder and childcare. In the sphere of eldercare, increased penetration of the discourses and processes of marketisation is evident in all three countries. In Sweden and England, policy priority is given to greater consumer choice, with service users increasingly constituted as consumers demanding higher quality service (market logic), rather than citizens bearing social rights (state-provider logic). These consumer-centric arguments are situated in a political context calling for greater efficiency and cost containment in the expenditure of public funds. Australia has no history of social rights to services and limited reliance on eldercare services directly provided by government, since services have been largely provided by the non-profit sector, albeit funded by governments. Opening up a quality-regulated market through contracting-out, tendering and commissioning, by allowing competition between for-profit and non-profit providers has been promulgated as expanding the supply of services, controlling costs and more recently, providing flexibility, higher quality services and consumer choice.
In childcare, marketisation and the encouragement of for-profit childcare have had different goals, meanings and impacts in each country, reflecting pre-existing patterns of provision or ‘policy logics’. In Sweden, marketisation was introduced to challenge a public monopoly and extend choice. For-profit childcare still represents only a small proportion of the Swedish system, although its long-term impact is potentially significant in rupturing the logic of state provision. In England, private markets have been the vehicle for governments to promote service expansion while reducing publicly provided care. In Australia, the aim of marketisation was to reduce the direct costs of service expansion faced by the government by encouraging for-profit providers to enter the sector. The intense market concentration that resulted revealed a major weakness in the application of market models to care.
To some extent, differences in marketisation trends in eldercare and childcare have been differentially influenced by a model of social investment, applied only to provision for the early years of life as the rationale for expanding supply in early childhood education and care. An emphasis on social investment in the later years of life has not been applied to eldercare in these three countries: priority has been given to expanding choice and cost-effective supply.
What is important is that increasing marketisation has exacerbated inequalities among service users in both sectors. Considerable evidence shows the difficulties experienced by consumers in making informed decisions about care, and indicates that not all social groups have the same capacity to exercise choice, based on their command of information and other resources. Increased focus on consumerism favours those with more resources, who have an advantage in navigating the system. In the case of eldercare, market-generated inequalities have been exacerbated, since service users with high levels of private resources are in the best position to benefit. In childcare there is mounting evidence of quality variation, with quality higher in non-profit than for-profit services.
Despite its problems, in all three countries marketisation is increasingly adopted as the policy of choice.