
Abstract
Differences in welfare attitudes of Eastern and Western Europeans have often been explained in terms of legacies of communism. In this article, we explore evaluations of healthcare systems across European countries and argue that East–West differences in these evaluations are explained by differences in the current institutional design of healthcare systems in the two regions. The empirical analysis is based on the fourth round of the European Social Survey, applying multilevel and multilevel mediation analysis. Our results support the institutional explanation. Regional differences in healthcare evaluations are explained by institutional characteristics of the healthcare system, that is, lower financial resources, higher out-of-pocket payments, and lower supply of primary healthcare services in Eastern compared to Western European countries. We conclude that specific aspects of the current institutional design of healthcare systems are crucial for understanding East–West differences in healthcare evaluations and encourage research to further explore the relevance of institutions for differences in welfare state attitudes across socio-political contexts.
Introduction
Analysing welfare attitudes has become increasingly relevant in the context of the recent economic crisis and austerity, which have intensified debates about the legitimacy and future of the welfare state (see Farnsworth and Irving, 2011). In an era of fiscal constraints and increasing pressures for welfare state reforms, it is important for both academics and policymakers to better understand public opinion towards welfare programmes and services. Some of the recent studies have, however, stressed that more research on welfare attitudes is needed as these attitudes are multidimensional (Roosma et al., 2013, 2014), and findings concerning public opinion towards the welfare state can differ depending on the type of attitude analysed. Scholars investigating normative attitudes, such as those related to views on redistribution or expectations towards government involvement in different social policy sectors, often find strong public support for the welfare state. In contrast, evaluative attitudes, which focus on the performance of the welfare state and have been much less systematically researched, are found to be far more negative (Roosma et al., 2013, 2014; van Oorschot et al., 2012; van Oorschot and Meuleman, 2012).
In this article, we analyse attitudes towards a specific welfare sector, healthcare, and compare these attitudes between Eastern and Western Europe. While attitudes towards welfare, and healthcare more specifically, have been well explored in Western Europe, research on welfare attitudes in Eastern Europe is still relatively scarce. Drawing on previous research that found Eastern in comparison with Western Europeans to be relatively similar in their normative but different and more negative in their evaluative attitudes towards the healthcare system (Missinne et al., 2013; Schneider and Popic 2018), we explore the underlying reasons for the East–West differences in healthcare evaluations. In contrast to the legacy explanation that dominates the existing literature and highlights the importance of the socialist past for the formation of normative welfare attitudes of Eastern Europeans (Andreß and Heien, 2001; Evans, 1998; Kulin and Meuleman, 2015; Lipsmeyer and Nordstrom, 2003; Roller, 1999; Svallfors, 2010), we argue that East–West differences in healthcare evaluations are best explained by differences in the current institutional set-up of healthcare systems in the two regions. In other words, we argue that specific features of the institutional and policy design of the existing healthcare systems, such as the amount of financial resources invested into the system, its supply of healthcare services and the way the system regulates access to these services, are key factors influencing citizens’ evaluations of the system and explain the East–West difference.
There are several reasons why understanding factors that drive healthcare evaluations is of vital importance for the welfare state and broader public debates. Evaluations of welfare programmes, similar to satisfaction measures, are related to an individual’s direct and indirect experience with existing institutions, and as they express views on a welfare state’s performance, they can play a crucial role in improving or eroding the legitimacy of the welfare state (Kumlin and Stadelmann-Steffen, 2014; Roosma et al., 2013). Evaluations can also act as indirect indicators of the acceptability of sector-specific reforms and inform us how reforms are experienced at the individual level (Footman et al., 2013; Mossialos, 1997). If a reformed healthcare system is perceived as malfunctioning, the voters may not accept it in the long run, which can create public pressure for policy change (Kohl and Wendt, 2004).
The contribution of this study to the existing literature is twofold. First, the study contributes to the literature on the role of institutions in the formation of welfare attitudes, providing evidence on institutional ‘feedback effects’ (see Gingrich and Ansell, 2012; Rothstein, 2001; Svallfors, 1997). Our study analyses the impact of institutions on attitudes towards the healthcare sector (Gevers et al., 2000; Jordan, 2010, 2013; Kohl and Wendt, 2004; Missinne et al., 2013; Wendt et al., 2010). We find support for the institutional argument but emphasize the need to analytically distinguish between two types of institutional effects. The first refers to the effect of past institutions on attitudes through socialization processes and past experiences, termed the ‘legacy’ impact, and the second stresses the effect of the current institutional design. Our second contribution concerns the literature on differences in welfare attitudes between Eastern and Western Europeans. While the majority of available studies on East–West differences focuses on normative attitudes (Andreß and Heien, 2001; Evans, 1998; Kulin, 2011; Kulin and Meuleman, 2015; Lipsmeyer and Nordstrom, 2003; Renwick and Toka, 2008; Roller, 1999), our study emphasizes welfare state performance in explaining differences in East–West attitudes. Furthermore, and in comparison with existing studies on healthcare attitudes which mainly focused on Western Europe (Gevers et al., 2000; Jordan, 2010; Kohl and Wendt, 2004; Wendt et al., 2010), we use a larger set of comparative data including Eastern European countries. We add to the study of Missinne et al. (2013) by exploring institutional characteristics responsible for explaining East–West differences in healthcare evaluations.
The article is divided into four sections. The first section, ‘Institutional effects on healthcare attitudes’, outlines the theoretical framework and specifies the institutional argument. The next section, ‘East–West differences in healthcare evaluations: the role of institutions’, focuses on differences in the institutional design of healthcare systems in Eastern and Western Europe and formulates the main hypothesis. The third section, ‘Data and methods’, describes the data and methodology while the final section, ‘Results’, presents the empirical results and is followed by the concluding section in which we summarize and discuss our research findings, and also provide suggestions for further research.
Institutional effects on healthcare attitudes
During the last couple of decades, research on welfare attitudes has been increasingly concerned with institutional feedback effects. According to the feedback effects approach, the institutional and policy design of the welfare state in modern democracies is seen as the product of public opinion and preferences. At the same time, institutions create an environment in which the public forms its views towards the welfare state, thus ‘feeding back’ into individual welfare preferences and attitudes (Gingrich and Ansell, 2012; Kumlin, 2002; Kumlin and Stadelmann-Steffen, 2014; Soss and Schram, 2007). Focusing on institutional effects on attitudes, scholars suggested that not only the size but also the design of the welfare state can have a profound impact on how individuals form their welfare views. The design of the welfare state influences attitudes as it represents the structure of direct encounters between citizens and welfare state institutions, and therefore affects their personal experiences, which in turn serve as the basis for the formation of citizens’ attitudes (Kumlin, 2002).
Studies on the effect of institutional design on attitudes often studied the impact of ‘welfare state regimes’ (Esping-Andersen, 1990) and focused on more general attitudes towards welfare (Andreß and Heien, 2001; Arts and Gelissen, 2001; Evans, 1996; Jakobsen, 2011; Larsen, 2008; Meier Jaeger, 2009; Svallfors, 1997). In contrast, studies analysing the links between institutions and more specific attitudes towards healthcare pointed out that ‘welfare regimes’ or even traditional healthcare system typologies have limitations in explaining these attitudes (Jordan, 2010, 2013; Kohl and Wendt, 2004; Missinne et al., 2013; Wendt et al., 2010). They argued that distinctions between, for example, Liberal and Social Democratic regimes are based on concepts that are too broad to be useful in identifying more precise links between the rather distinctive institutional designs of countries’ healthcare systems and attitudes (Kohl and Wendt, 2004; see also Bambra, 2005). Similarly, they claimed that traditional differentiations between the ideal types of healthcare systems, such as the National Health Service (NHS) and the Social Health Insurance (SHI), conceal the complexity of actual systems and their changes over time, rendering the use of typologies as analytical tools for cross-country comparisons rather limited (Kohl and Wendt, 2004; Wendt et al., 2009, 2010).
To better capture the complexity of the institutional design of healthcare systems and to study the impact of existing institutions on healthcare attitudes, Wendt et al. (2010) provide a conceptualization, which defines and interlinks different institutional dimensions of the healthcare service ‘production process’. This conceptualization distinguishes between three different dimensions: (1) ‘monetary input’, which accounts for the financing of healthcare services; (2) ‘real input’, which reflects the supply of resources in terms of both healthcare facilities and personnel; and (3) ‘institutional set-up’, which regulates access to healthcare services (see also Kohl and Wendt, 2004; Marmor and Wendt, 2012). Importantly, all three dimensions, although causally related, allow us to capture different aspects of the healthcare system design experienced by individuals in ‘real time’ and test the importance of each dimension for the formation of their healthcare attitudes.
Various cross-national studies found evidence for strong correlations between specific aspects of the actual institutional arrangement of healthcare systems and the public views of healthcare system performance, such as the satisfaction with or the evaluation of healthcare services. Analysing Western European countries, they show that high monetary input in the form of total and public healthcare expenditure and a large supply of healthcare services and personnel correlates with high levels of satisfaction (Kohl and Wendt, 2004; Mossialos, 1997; Wendt et al., 2010). More specifically, Wendt et al. (2010) find a strong link between high satisfaction and high supply of primary care services, measured by the density of general practitioners (GPs), but surprisingly no link between satisfaction and access regulations. Some of these findings are also supported by Missinne et al. (2013); they use a larger sample of Eastern and Western European countries and find that high levels of public expenditure and healthcare service supply have a positive effect on healthcare evaluations.
In line with the literature, we expect evaluations of healthcare systems to be affected by their institutional design. More specifically, we expect higher healthcare spending and more generous healthcare supply to be associated with positive evaluations. In respect of the third dimension, access regulations, we expect healthcare evaluations to be more positive if access rules are less restrictive and provide more choice to the individual: 1
H1a. The higher the monetary input into the healthcare system (i.e. the higher the total and public spending on healthcare, and the lower the private spending on healthcare), the more positive the healthcare evaluation.
H1b. The higher the real input into the healthcare system (i.e. the larger the supply of healthcare services and personnel), the more positive the healthcare evaluation.
H1c. The more freedom of choice patients have in accessing healthcare services (i.e. the less restrictive the access regulations), the more positive the healthcare evaluation.
East–West differences in healthcare evaluations: the role of institutions
Existing studies of welfare attitudes comparing the Eastern, formerly communist and the Western part of Europe have relied strongly on the legacy explanation to account for East–West differences in attitudes. The legacy approach assigns primary importance to the effects of past policy choices. The underlying assumption of this approach is that perceptions and expectations towards welfare are formed through socialization processes within particular regime types. Political regimes play an active role in these socialization processes as they seek to inculcate attitudes that support the current regime and justify its structure (Dennis and Jennings, 1970; Greenberg, 1970). The socialization and the experience of living under socialism have therefore been considered crucial for the formation of welfare attitudes of Eastern Europeans and explain why they differ from attitudes of Western Europeans (Pop-Eleches and Tucker, 2014; Roller, 1999; Svallfors, 2010).
In contrast to the legacy explanation, we expect differences in healthcare system evaluations between Eastern and Western Europeans to be explained by variation in the ‘production process’, that is, institutional designs of the current healthcare systems in the two regions. Since the fall of communism in 1989, Eastern European healthcare systems underwent a series of radical institutional changes. Under communism, most of the countries from this region featured the so-called ‘Semashko’ model of healthcare, similar to the NHS, which was centrally planned and funded exclusively from public sources. This system provided universal access to medical care but was also characterized by weak primary care, territorial limitation in access to services, chronic underfunding and corruption (Field, 1967; Kornai and Eggleston, 2001; Weinerman and Weinerman, 1969). In the post-communist period, reforms of Eastern European healthcare systems implied wide-ranging transformations at the systemic level, in most countries marked by the shift from the ‘Semashko’ to the SHI system, involving change from a tax-based to a contributions-based model of healthcare financing. Apart from this systemic change, the post-communist reforms also introduced a series of more specific policy changes in healthcare financing, which often implied mechanisms for improved public financing and partial privatization of healthcare costs through user fees and co-payments for medical goods and services. In healthcare delivery, changes involved the introduction of patients’ choice and improvement of healthcare infrastructure, which were often combined with privatization, mainly in primary care, and incentives for competition among healthcare providers (Bartlett et al., 2012; Cerami, 2006; Kutzin et al., 2010; Marree and Groenewegen, 1997; Rechel et al., 2014).
Despite these large-scale changes and variation in policy paths taken by the different post-communist countries, empirical evidence on trends in Eastern European healthcare systems indicates significant institutional differences in comparison with Western European systems. First, Eastern European systems generally have fewer financial resources and patients tend to spend more on both formal and informal out-of-pocket payments (OOP; Busse, 2002; Rechel et al., 2014; Rechel and McKee, 2009). Second, these healthcare systems tend to feature stronger specialist and secondary care and significantly weaker primary care, characterized by lower supply of primary care physicians and underdeveloped family medicine (Rechel and McKee, 2009; Seifert et al., 2008). Third, Eastern European healthcare systems differ in respect of access regulations: although they have abandoned the territorial limitations in healthcare access, they have introduced stringent gatekeeping that controls users’ access to secondary health services (Groenewegen et al., 2013; Kringos et al., 2015).
This evidence on distinctive institutional features of the post-communist health systems indicates that there are significant differences in the institutional design of the ‘production processes’ of healthcare services in Eastern in comparison with Western Europe. This also suggests that some specific aspects of the citizens’ experience with healthcare services in the two regions are notably different. Therefore, we assume that the East–West differences in healthcare system evaluations are not caused by the past institutional structures and socialization processes under communism – as it is often suggested in the literature – but are due to the different institutional designs of current healthcare systems in the two regions:
H2. Differences in the current institutional design of healthcare systems – lower monetary input in total and from public sources, higher out-of-pocket payments, lower real input in primary care and stricter regulations of access to secondary care – in Eastern compared to Western European countries explain lower healthcare evaluations in Eastern compared to Western Europe.
Data and methods
Data
The empirical analysis is based on data from the fourth round of the European Social Survey (ESS) from 2008/09. The ESS is a high-quality, cross-comparative data set that provides biannual information representative for the European population living in private households aged 15 and above. The fourth round of the ESS covers the largest number of Eastern European countries and was therefore selected for the empirical analysis. In total, the empirical analysis is based on data of 12 Eastern and 15 Western European countries. 2 Turkey and Israel are excluded from the analysis as they are not considered European. Lithuania is omitted due to missing information on the weighting variable. Cyprus is excluded due to the unavailability of information on the number of GPs. In total, the sample counts 27 countries and includes 51,001 individuals living in private households in Europe for whom information on all variables was available.
Variables
Dependent variable
The evaluation of healthcare services forms the main dependent variable of our analysis. Respondents were asked what they think overall about the state of health services in their country nowadays on an 11-point scale ranging from 0 (extremely bad) to 10 (extremely good).
Independent variables – country level
Following our theoretical framework, we selected the following indicators to measure the three different institutional dimensions of the healthcare system’s ‘production process’ (Wendt et al., 2010).
‘Monetary input’ is measured by three indicators publicly available at the World Bank database. The amount of total healthcare expenditure (THE) (per capita, US dollars) reflects the general level of economic development and stands for the overall financial investment in healthcare. The relative amount of public healthcare expenditure (PHE) as a percentage of total government expenditure (TGE) indicates cross-country differences in the ‘interventionist’ power of the state and the political ‘priority’ of healthcare in the country (Alber, 1988; Immergut, 1992; Kutzin et al., 2010). The relative amount of out-of-pocket expenditure as a percentage of THE provides direct information on the public–private expenditure mix, also indicating the level of ‘risk privatization’ (Hacker, 2004), that is, the level of relative financial burden placed on the shoulders of the healthcare users (see also Wendt et al., 2010).
Data publicly available at the World Health Organization’s (WHO) Health for All Database provide information on the availability of healthcare personnel and infrastructure which measure the supply, that is, the ‘real input’, of the healthcare system. To provide a more differentiated picture of the healthcare services supplied to healthcare users, we chose to differentiate between different types of care: inpatient and outpatient care as well as primary and secondary care. The number of GPs (per 1000 of population) reflects the supply of healthcare personnel for primary (outpatient) healthcare services; the number of specialists (physicians as medical group of specialties, per 1000 of population) reveals information on the supply of healthcare personnel for secondary (inpatient and outpatient) care; the number of hospital beds (per 1000 of population) indicates the supply of inpatient services (see Kohl and Wendt, 2004).
Since data on the institutional regulations of patients’ access to healthcare services were not available for 2008, we extracted the information on access regulations from the MISSOC database and the WHO Health in Transition country-specific reports. Following the previous literature (Reibling, 2010; Reibling and Wendt, 2008; Wendt et al., 2010), we distinguish between three types of access regulations that may limit the freedom of choice for individuals seeking healthcare. The first two types relate to access to primary care. In the case of obligatory GP registration, patients have to register with a particular GP to receive medical treatment – either formally, when they are obliged to register as residents, or informally, when registration is the only way to access primary healthcare services. Another type of access regulation is based on geographical restriction, which limits the choice of GP services to the geographic unit in which the patient resides. Countries also differ in their regulation of access to specialist care. We distinguish between referral systems, in which access to specialist care is only permitted with referral by the GP (without a referral, a patient has to cover the full costs for the service delivered by a specialist); pay and skip systems, which require a referral by the GP but allow direct access to specialist care for patients without referral who are willing to pay a fee; and free access systems, which allow free access to specialist care, as they neither require a GP’s referral nor do they charge extra fees for those without referral (Reibling, 2010; Reibling and Wendt, 2008).
Table 1 provides an overview of these institutional characteristics for all 27 European countries included in the empirical analysis.
Institutional characteristics of healthcare systems.
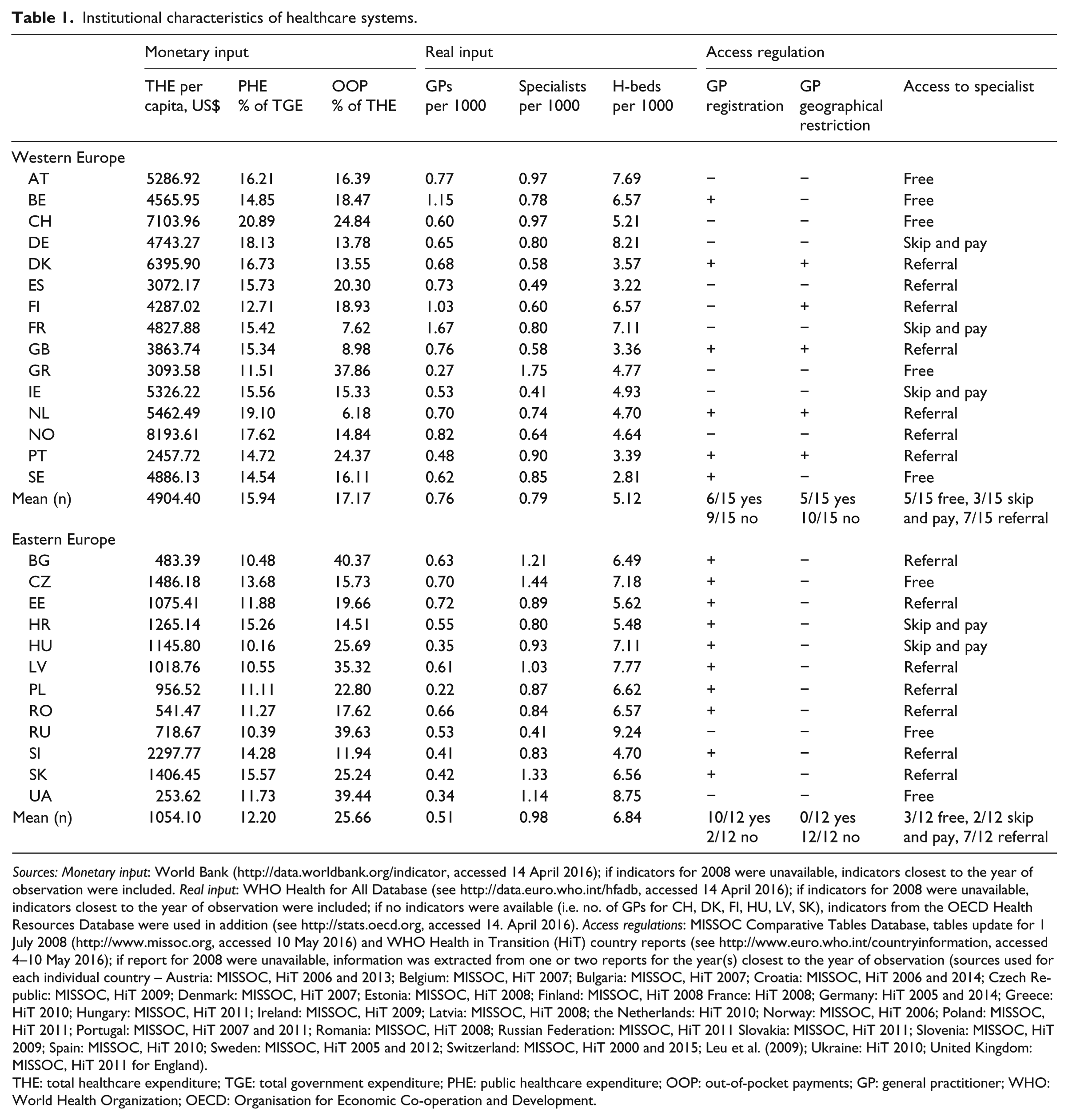
Sources: Monetary input: World Bank (http://data.worldbank.org/indicator, accessed 14 April 2016); if indicators for 2008 were unavailable, indicators closest to the year of observation were included. Real input: WHO Health for All Database (see http://data.euro.who.int/hfadb, accessed 14 April 2016); if indicators for 2008 were unavailable, indicators closest to the year of observation were included; if no indicators were available (i.e. no. of GPs for CH, DK, FI, HU, LV, SK), indicators from the OECD Health Resources Database were used in addition (see http://stats.oecd.org, accessed 14. April 2016). Access regulations: MISSOC Comparative Tables Database, tables update for 1 July 2008 (http://www.missoc.org, accessed 10 May 2016) and WHO Health in Transition (HiT) country reports (see http://www.euro.who.int/countryinformation, accessed 4–10 May 2016); if report for 2008 were unavailable, information was extracted from one or two reports for the year(s) closest to the year of observation (sources used for each individual country – Austria: MISSOC, HiT 2006 and 2013; Belgium: MISSOC, HiT 2007; Bulgaria: MISSOC, HiT 2007; Croatia: MISSOC, HiT 2006 and 2014; Czech Republic: MISSOC, HiT 2009; Denmark: MISSOC, HiT 2007; Estonia: MISSOC, HiT 2008; Finland: MISSOC, HiT 2008 France: HiT 2008; Germany: HiT 2005 and 2014; Greece: HiT 2010; Hungary: MISSOC, HiT 2011; Ireland: MISSOC, HiT 2009; Latvia: MISSOC, HiT 2008; the Netherlands: HiT 2010; Norway: MISSOC, HiT 2006; Poland: MISSOC, HiT 2011; Portugal: MISSOC, HiT 2007 and 2011; Romania: MISSOC, HiT 2008; Russian Federation: MISSOC, HiT 2011 Slovakia: MISSOC, HiT 2011; Slovenia: MISSOC, HiT 2009; Spain: MISSOC, HiT 2010; Sweden: MISSOC, HiT 2005 and 2012; Switzerland: MISSOC, HiT 2000 and 2015; Leu et al. (2009); Ukraine: HiT 2010; United Kingdom: MISSOC, HiT 2011 for England).
THE: total healthcare expenditure; TGE: total government expenditure; PHE: public healthcare expenditure; OOP: out-of-pocket payments; GP: general practitioner; WHO: World Health Organization; OECD: Organisation for Economic Co-operation and Development.
Independent variables – individual level
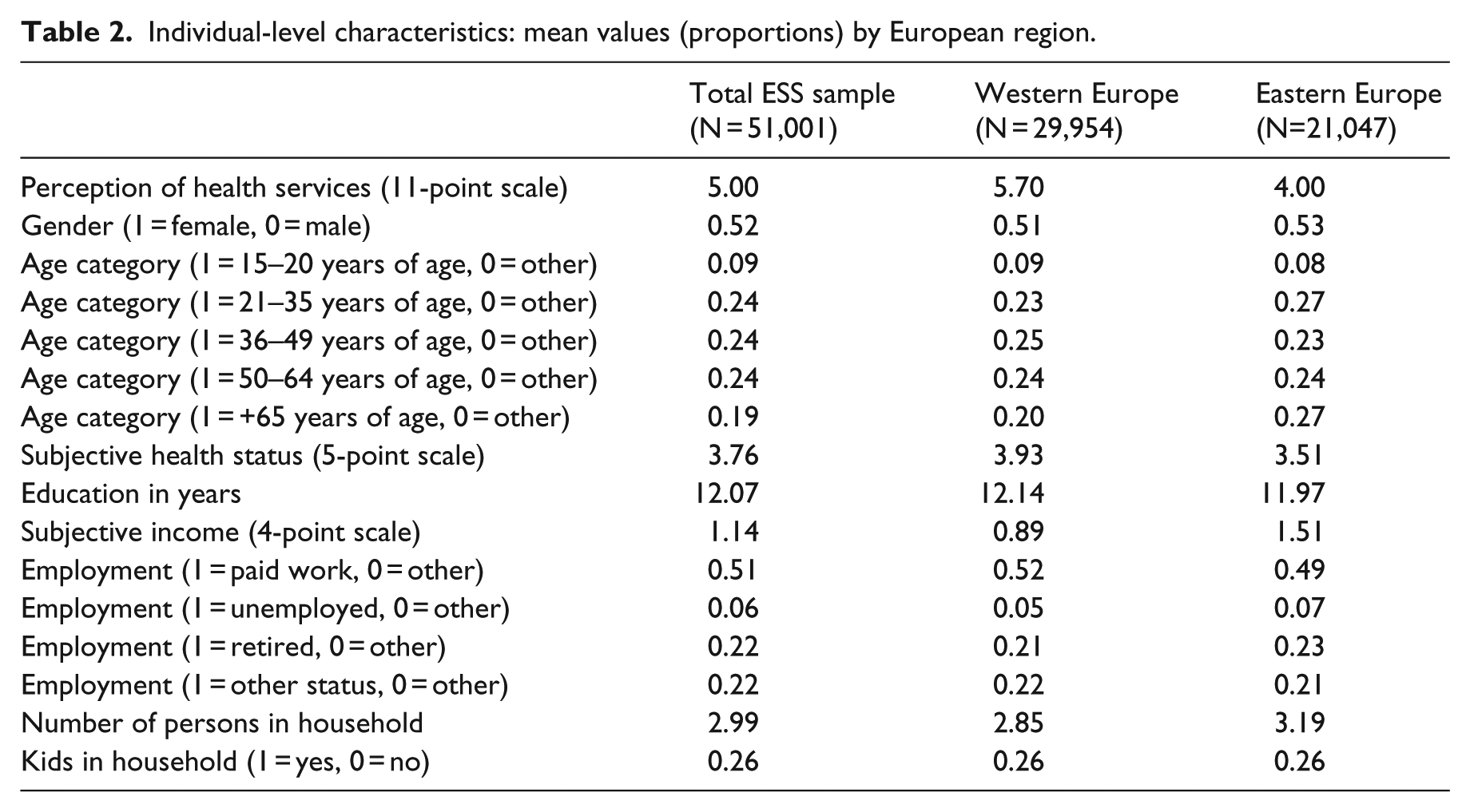
We control for additional demographic and economic characteristics of individuals that influence the evaluation of health services (Missinne et al., 2013) (Table 2). The respondent’s sex and age are included in the analysis as standard control variables. In order to control for health needs, we included the respondent’s self-reported health status measured on a 5-point scale, ranging from very good to good, fair, bad and very bad. We also control for socio-economic characteristics that are reported to influence people’s attitudes, such as years of education and the current employment status (paid work, unemployed, retired, other status). To avoid the exclusion of countries from our analysis due to missing income information, we include a subjective income indicator that serves as a proxy for the financial resources available to the household. 3 Respondents were asked how they feel about their household income nowadays and whether they live comfortably on their present income, cope on their present income, find it difficult on their present income or find it very difficult on their present income. To control for other household characteristics, we include the household size and whether children under 15 years of age are living in the household. Health-related limitations in daily lives and routines as well as sources of household income did not reveal any significant effects and were therefore excluded from the analysis. We mean-centred all metric variables (here, years of education). The health status variable was recoded ranging from –2 (very bad) to +2 (very good) (0 = fair).
Individual-level characteristics: mean values (proportions) by European region.
Statistical methods
We apply multilevel modelling techniques with robust standard errors (SEs) to estimate the effects of both individual- and country-level characteristics. Unlike conventional regression analysis, multilevel models account for hierarchical or nested data structure (Hox, 2010), whereby observations at the lower (individual) level are nested in higher order units (countries). Considering the multiple levels in the computation process controls for the interdependency of observations and produces more accurate estimates.
First, we run random intercept models which allow the measurement of contextual variation in the outcome variable. Variation in the country-specific intercepts is explained later by the above-stated country-level predictor variables. For realistic estimates of the portion of explained variance at the different levels of analysis, the amount of unexplained variance is decomposed into level-specific variance components (Bryk and Raudenbush, 1992).
We also used multilevel mediation models to test for potential mediating effects of institutional variables in the explanation of East–West differences in healthcare system evaluations. In general, multilevel mediation models allow us to model more complex relationships and to estimate direct and indirect relationships between a set of variables within a multilevel framework. Mediator variables (here, institutional characteristics) change from being dependent to being independent and are therefore treated as endogenous in the path model. We apply a 2-2-1 multilevel mediation analysis (MMA) following Preacher et al. (2010) given that our independent variable (here, Eastern and Western region) and our mediator variables (here, institutional characteristics) are located at the macro level (level 2), while evaluations are individual-level characteristics and located at the micro level (level 1). The mediation is measured at the between level, partitioning the variances of the individual-level variable into a between- and within-level component. The mediation effect is the product of (1) the effect of region (East/West) on the mediator (institutions) and (2) the effect of the mediator (institutions) on the outcome variable (healthcare system evaluations) at the macro level.
Analyses are computed with MPlus version 7. At all stages, we control for individual characteristics including health needs. To control for differences in sampling methods across countries, we use post-stratification weights following the recommendations of the ESS. 4
Strategy of analysis
First, we present descriptive analysis of healthcare system evaluations across European countries. Second, we report results of the multilevel regression models which provide a more fine-grained picture on cross-country variation in healthcare evaluations. We analyse the degree to which Eastern and Western Europeans differ in their evaluation of the current healthcare system before we investigate the effects of institutional characteristics on healthcare system evaluations. Next, we use MMA to test for the mediating power of institutional characteristics for the explanation of East–West differences in healthcare evaluations. We complete our analysis by presenting subgroup-specific models for different birth cohorts to test the robustness of our findings with regard to previous research on legacy effects.
Results
With a mean of 5.00 (standard deviation (SD) = 2.59) measured on an 11-point scale, Europeans on average evaluate the healthcare services of their countries moderately well. However, and in line with previous research, evaluations vary across countries and regions. The results in Figure 1 indicate a strong divide between Eastern and Western European countries: Western Europeans (M = 5.74, SD = 1.12) rate the healthcare system of their countries on average 1.69 scale points higher than Eastern Europeans (M = 4.04, SD = 0.83, F = 19.20, p < 0.001). The Belgium healthcare system receives the best evaluation of all European countries with a mean of 7.38 (SD = 1.59), followed by Switzerland (M = 6.99, SD = 1.87), Finland (M = 6.64, SD = 1.97) and Austria (M = 6.56, SD = 2.36). Greece (M = 3.38, SD = 2.34), Ireland (M = 4.19, SD = 2.37) and Portugal (M = 4.30, SD = 2.14) have the lowest healthcare system rating in Western Europe and even score lower than some Eastern European countries. Among the group of Eastern European countries, the Czech Republic (M = 5.40, SD = 2.45), Estonia (M = 5.08, SD = 2.24) and Slovenia (M = 4.84, SD = 2.38) receive the best evaluations of healthcare services. Ukraine scores particularly low with a mean of 2.49 (SD = 2.03), followed by Bulgaria with a mean of 3.24 (SD = 2.39).
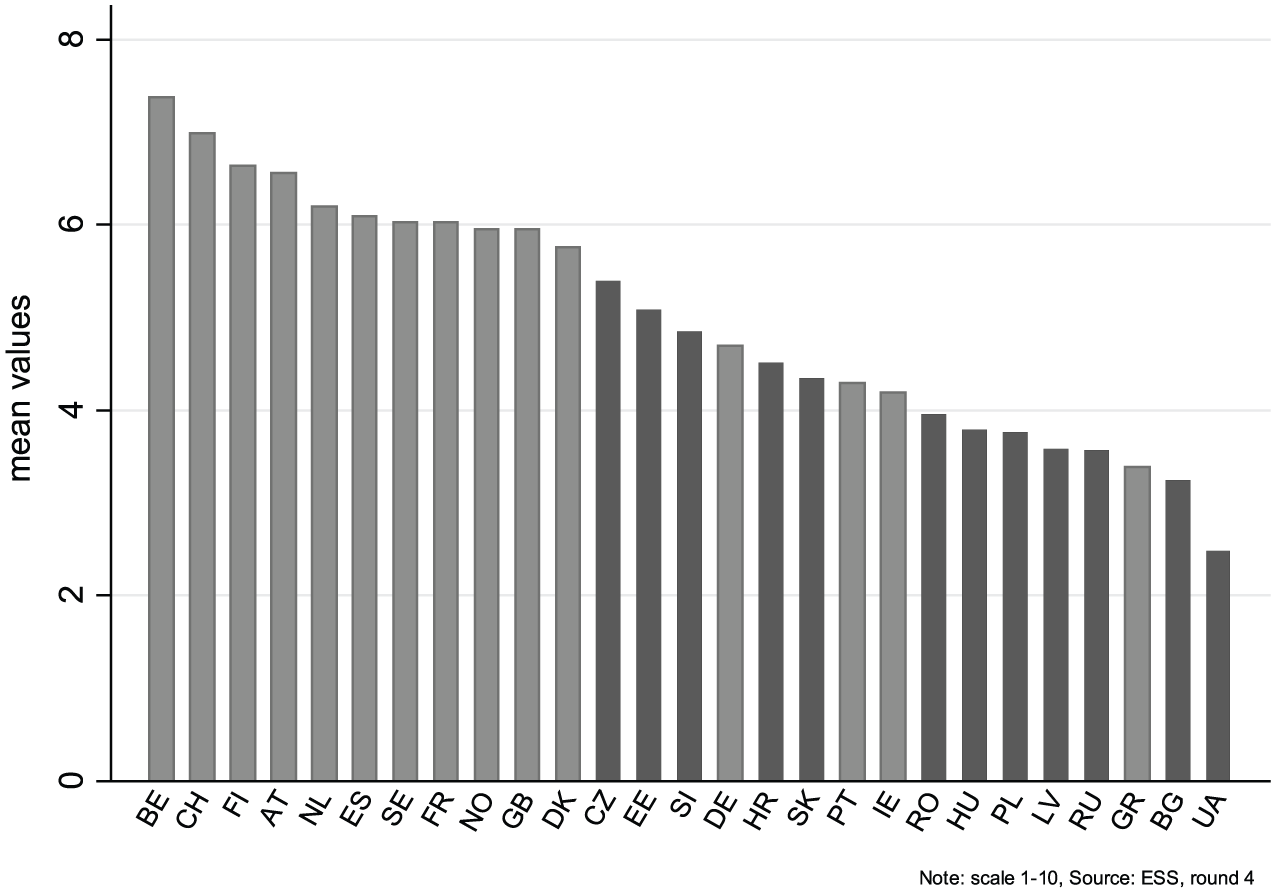
Evaluation of health services across European countries (mean values).
The results of the multilevel regression models support the descriptive findings and show that evaluations vary strongly between countries (intraclass coefficient = 0.24; design effect = 461.65) and regions (β = −1.69, SE = 0.36) (Table 3, Model 1). Differences in the population composition within European countries only partly explain regional differences in healthcare service evaluations. After controlling for demographic and socio-economic characteristics at the individual level, we find that Eastern Europeans still rate the healthcare services of their countries lower than Western Europeans (β = −1.46, SE = 0.34) (Table 3, Model 2). In total, East–West differences explain 38.8 percent of the cross-country variation in healthcare evaluations. Demographic and socio-economic characteristics can only explain 3.9 percent of the variance at the individual level.
East–West differences in the evaluation of health services – results of the multilevel analysis.
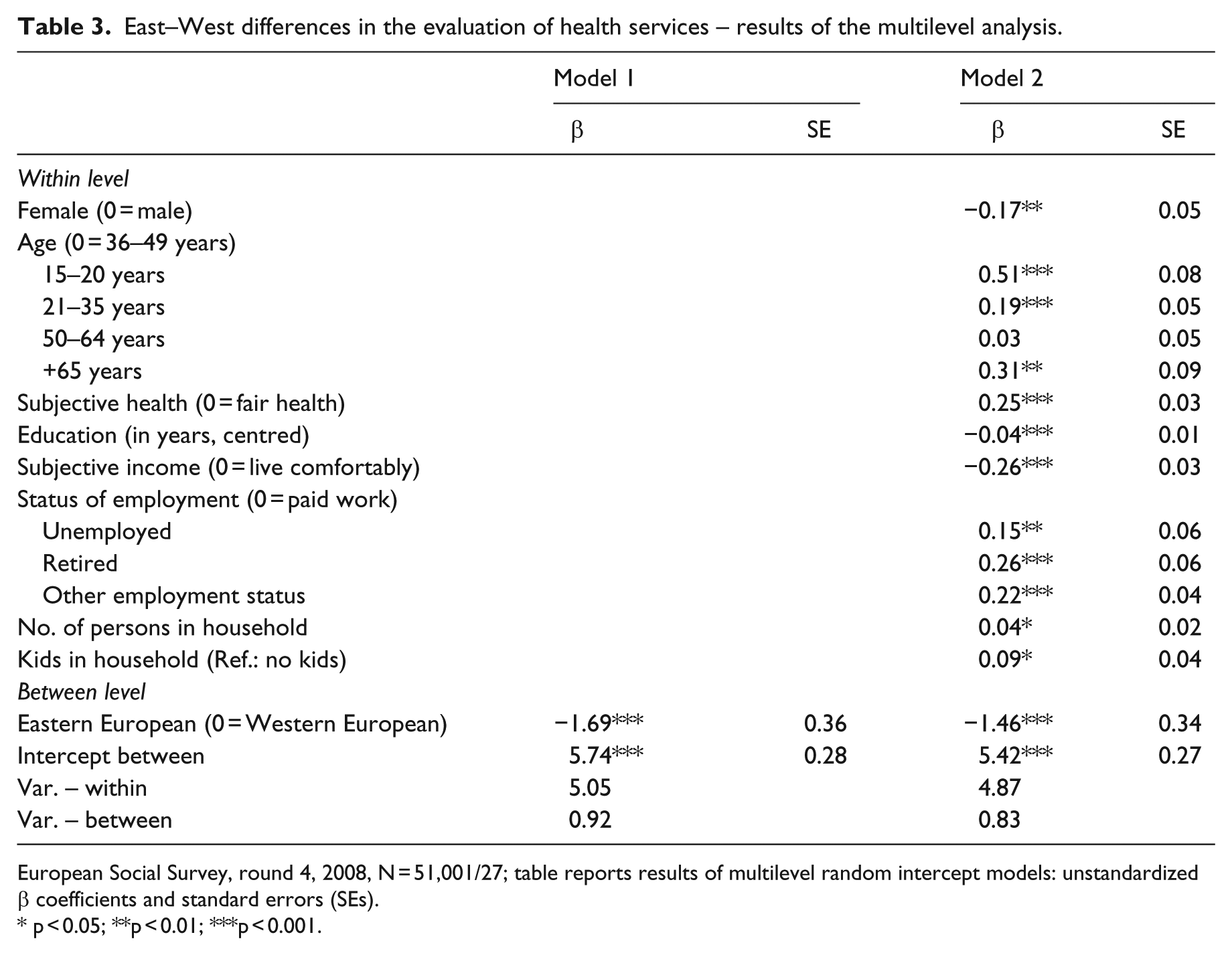
European Social Survey, round 4, 2008, N = 51,001/27; table reports results of multilevel random intercept models: unstandardized β coefficients and standard errors (SEs).
p < 0.05; **p < 0.01; ***p < 0.001.
According to our theoretical framework, differences in the current institutional set-up of healthcare systems are crucial for the explanation of cross-country and cross-regional differences in healthcare evaluations, which requires empirical testing. Table 4 reports the results of the multilevel regression analysis on institutional effects after controlling for demographic and socio-economic characteristics at the individual (within) level. To avoid biases in the estimation process due to multi-collinearity and small numbers of degrees of freedom at the country level, we tested the effects of each institutional characteristic separately before including them in dimension-specific regression models.
Institutional effects on evaluation of health services – results of the multilevel analysis.

THE: total healthcare expenditure; TGE: total government expenditure; PHE: public healthcare expenditure; GP: general practitioner
European Social Survey, round 4, 2008, N = 51,001/27; table reports results of multilevel random intercept models: unstandardized β coefficients and standard errors; all analyses control for demographic and socio-economic characteristics (see Table 3, Model 2).
p < 0.1; *p < 0.05; **p < 0.01; ***p < 0.001.
In line with our hypothesis (H1a), we find monetary inputs to be crucial for healthcare service evaluations. Evaluations are more positive, (1) the more financial resources healthcare systems have available (THE, per capita) (Table 4, Model 1.1), (2) the larger the amount of public resources spent on healthcare relative to other government expenditures (PHE, % of TGE) (Model 1.2) and (3) the less money individuals have to spend out of their own pockets (OOP, % of THE) (Model 1.3). Combining all three indicators, and testing for their competing impact on healthcare evaluations, we find the levels of THE and OOP to be particularly important for healthcare service evaluations (Model 1.4).
With regard to real inputs, that is, supply of healthcare services and personnel, we find partial support for our hypothesis (H1b). Findings reveal that the higher the supply of primary care services (number of GPs, per 1000 of population) in the country, the better the public’s evaluation of the healthcare system (Model 2.1 and 2.4). Interestingly, however, we find neither the number of specialists (Model 2.2) nor the number of hospital beds (Model 2.3) to significantly alter the public’s opinion on healthcare services, suggesting that supply of inpatient and secondary care is not important for the explanation of cross-country differences in healthcare evaluations.
Contrary to our expectation that freedom of choice in accessing medical services will have a positive impact on evaluations (H1c), our results show that none of the three access regulation indicators significantly affect how the public evaluates the healthcare system (Table 4, Models 3.1–3.4).
Overall, our results underline the importance of specific institutional characteristics of healthcare systems on public opinion. The absolute amount of financial resources invested in healthcare (THE, per capita), as well as the supply of primary healthcare services (number of GPs, per 1000 of population), translates into more positive evaluations of healthcare services, while OOP have a negative impact on evaluations. Although individuals directly experience access regulations as these regulations affect the choices of those seeking healthcare, they do not seem to influence the public’s evaluation of healthcare services; nor does the supply of secondary and inpatient care, measured by the density of specialists and hospital beds.
Do institutional characteristics explain East–West differences in the evaluation of healthcare services? MMA allows us to empirically test if and to what degree institutional characteristics explain regional differences in healthcare evaluations by distinguishing between direct effects (DEs) and indirect effects (IEs) on evaluations. A strong and significant indirect effect of region (East/West) together with a drop in the significance of the direct regional effect underlines the relevance of institutional characteristics. The effect size of the IE indicates the strength in which institutional characteristics explain East–West differences in healthcare evaluations.
The results in Figure 2 indicate that East–West differences in healthcare service evaluations are fully explained by THE (per capita) (DE: β = 0.26, SE = 0.55; IE: β = −1.72, SE = 0.40) and the PHE relative to the TGE (DE: β = −0.83, SE = 0.52; IE: β = −0.62, SE = 0.32). OOP relative to the THE (DE: β = −1.00, SE = 0.36; IE: β = −0.46, SE = 0.19) and the number of GPs (per 1000 of population) (DE: β = −0.96, SE = 0.35; IE: β = −0.50, SE = 0.18) partly explain why Eastern Europeans evaluate healthcare services so differently to Western Europeans. Although regional differences are also observed with respect to the number of specialist and hospital beds as well as access regulation patterns (see Table 1), they do not affect the public’s opinion on healthcare services and thus do not contribute to the explanation of East–West differences in healthcare service evaluations.

Direct and indirect effects on evaluation of health services: results of the multilevel mediation analysis.
Our results support our argument showing that institutions of the current healthcare systems matter to the public’s evaluation of healthcare services and explain differences in evaluation patterns between the East and the West. More specifically, they reveal that differences in the financial resources, particularly in the THE (per capita) and public healthcare expenditure (% TGE), are crucial for explaining regional differences in healthcare attitudes. Differences in the supply of primary healthcare services (number of GPs, per 1000 of population) and the amount of OOP (% of THE) partly contribute to this explanation.
Often, scholars studying East–West differences in welfare attitudes have claimed that past experiences and socialization processes in different political regimes explain regional differences in public expectations and evaluations (Andreß and Heien, 2001; Kulin and Meuleman, 2015; Lipsmeyer and Nordstrom, 2003; Renwick and Toka, 2008; Svallfors, 2010). Following this reasoning, (1) older birth cohorts in the East and in the West are expected to differ more strongly in their evaluations than younger birth cohorts (Svallfors, 2010), and (2) institutional characteristics of the current healthcare system are not expected to explain regional differences in healthcare evaluations for older age cohorts, those who grew up and lived in the socialist system (Western capitalist system, respectively) for the majority of their lives. To support our argument on the impact of current institutions and to further check the robustness of our findings, we re-ran our analysis for different birth cohorts. Following Svallfors (2010), we distinguish between (1) individuals born before 1951 who grew up and lived in the socialist system for the majority of their lives, (2) individuals born between 1951 and 1974 who have been in full adulthood by the time of the fall of communism and (3) individuals born after 1974 who have at best experienced communism for 14 years.
Our findings show that – although differences in healthcare evaluations between Eastern and Western Europeans are strongest for the oldest birth cohort – institutional differences have fairly similar effects across birth cohorts (Table A1 in Supplementary Appendix). Interestingly, and contrary to our hypothesis on access regulations, cohort-specific analysis of institutional effects on healthcare service evaluations show that registration with a GP positively affects evaluation of healthcare services. This finding suggests that the obligatory registration with a GP may not be seen as a limitation of patient’s rights, but rather as a guarantee for the continuity and stability in the doctor–patient relationship. This effect is only significant for the oldest birth cohort and appears to be an expression of age-specific preference patterns rather than a cohort-specific result.
Overall, findings of the cohort-specific analysis support our previous results and strengthen our argument. The findings on institutional effects on healthcare service evaluations appear independent of the length of time individuals have been socialized in different political systems, suggesting that the socialist past may not be essential for explaining East–West differences in evaluative attitudes towards healthcare. In other words, these findings suggest that it is not the past but rather the current institutional set-ups of healthcare systems that matter for the public’s evaluations of healthcare services and explain regional differences in evaluation patterns between Eastern and Western Europeans.
Conclusions
In this article, we investigated differences in welfare attitudes between Eastern and Western Europeans. While previous research has emphasized past institutions and socialization processes under the communist regime as important for the explanation of differences in attitudes between the two regions, we argued that current institutions explain these differences in attitudes and tested this claim on evaluations of healthcare services.
In line with our theoretical expectations, we found that differences in the institutional design of healthcare systems have a significant impact on cross-regional differences in healthcare evaluations between Eastern and Western Europe. These differences are explained by institutional characteristics of the healthcare system – lower financial resources, higher OOP and less supply of primary healthcare services – in Eastern compared to Western European countries. Furthermore, we found these institutional aspects to be similarly important across birth cohorts.
Our results thus confirm prior research on institutional effects on attitudes (Jordan, 2010, 2013; Missinne et al., 2013; Wendt et al., 2010), suggesting that the design of healthcare policies and institutions can have a significant impact on public opinion towards the health system as a whole. However, the results also stress that not all aspects of the institutional set-up are equally relevant for citizens’ evaluations. Policies that determine the financial aspects of healthcare provision – the amount of resources invested in healthcare, the priority government assigns to the health sector and the way it manages the public–private mix – as well as the supply of healthcare personnel in primary care are more important for citizens’ evaluations, than policies that regulate access to care. Our results hence suggest that policymakers should be more careful when introducing policies that change the public–private mix, for example, by cutting public healthcare spending or introducing user fees for medical services, as these policies could backfire, worsening the perception of the healthcare system as a whole. Similarly, as evaluations improve with a higher number of GPs in the system, emphasis on primary care could improve the healthcare system’s reputation in the eyes of the public.
Furthermore, our results highlight regional disparities in terms of financing and supply of healthcare services between Eastern and Western Europe that exist even two decades after the fall of communism and that influence how the public evaluates the healthcare system. Regional disparities in the total levels of financing for healthcare services, despite wide-ranging transformations of the Eastern European health sectors and cross-country variations, are still severe and may express the generally lower level of economic development in the Eastern European region. Nevertheless, our findings also suggest that East–West differences are not only due to economic development but also due to policy decisions. Regional differences in the public healthcare spending (as % of TGE) indicate that, on average, healthcare enjoys higher government priority in Western than in Eastern European countries. Similarly, a higher financial burden in the form of OOP (as % of THE) placed on the shoulders of the patients in Eastern compared to Western Europe indicates that governments have either withdrawn from healthcare financing (through formal OOP) or proved incapable of fighting corruption in the healthcare sector (through informal OOP). Finally, the lower supply of GPs (in contrast to a high supply of specialist and hospital beds) in the East indicates a difference in policy priority in healthcare delivery. These differences hence suggest that it may be due to the policy choices, not only levels of economic development, as to why Eastern Europeans are more negative in their healthcare evaluations in comparison with their Western European neighbours.
Our study is not without limitations, however. While our findings support the argument that underlines the importance of the current institutional design for the explanation of public healthcare evaluations and regional differences in these evaluations between Eastern and Western Europeans, they do not rule out the legacy hypothesis emphasized in the literature. Scholars such as Wendt et al. (2010) have indeed found that the institutional design of the current healthcare system is of greater relevance for evaluative attitudes, on the performance of the healthcare system, than for normative attitudes towards healthcare. This suggests that we should be careful in distinguishing between two different types of healthcare attitudes (normative and evaluative) as well as between two possible types of feedback effects (effect by old and new institutions). In addition, legacies (i.e. old institutions and experiences) could be more relevant for normative attitudes than for the attitudes focused on welfare state performance, for which the current institutional design is found to play an important role. In order to properly test the legacy argument against the impact of current institutions, further research is therefore needed. The recent work by Pop-Eleches and Tucker (2017) on the impact of communist legacies on attitudes formation can be particularly useful in this respect.
In addition, our study focused on explaining welfare attitudes that express citizens’ evaluations by looking at more general institutional characteristics of the healthcare system using cross-sectional data. In comparison with this, studies that use longitudinal data and focus on the impact of specific institutional reforms of the healthcare system on attitudes can not only empirically but also theoretically contribute to the better understanding of institutional feedback effects. Refined analyses that distinguish between different types of welfare attitudes and look at the modes in which these attitudes are influenced by different institutional organizations of the welfare state and their change over time will provide promising avenues for further research.
Footnotes
Acknowledgements
The authors would like to thank Ellen Immergut, Karen Anderson, Maria Oskarson, the editors of the Journal of European Social Policy and the anonymous reviewers for their valuable comments on earlier drafts of this manuscript. The authors would also like to thank Bertha Banda for her help in preparing the data set. For all statements of fact, data analyses and interpretation of results, the authors alone bear responsibility.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is part of the NORFACE Welfare State Futures funded research project ‘The Paradox of Health State Futures’ (HEALTHDOX) (EC ERA-Net Plus funding, grant agreement number 618106, file number 462-14-070).
Supplementary material
Supplementary Appendix is available online.