
Abstract
Background
Colon cancer (CC) refers to malignant tumor of the digestive tract worldwide and is also among the cancers with high mortality rates.
Objective
The aim of this work was to evaluate the diagnostic performance of multislice spiral CT (MSCT), magnetic resonance imaging (MRI), and MSCT + MRI in different stages of colon cancer (CC) (T1-T2, T3, T4). This work compared the differences in sensitivity (Sen), specificity (Spe), accuracy (Acc), and area under the curve (AUC) values among these methods and explored the optimal diagnostic strategy.
Methods
A total of 120 patients with CC confirmed by pathological biopsy and 30 individuals suspected of CC but without detected tumors (as controls) were selected. All subjects underwent MSCT, MRI, and combined MSCT + MRI examinations. Statistical analyses of Sen, Spe, Acc, and AUC values were performed.
Results
In the T1-T2 stage, MSCT had a Sen of 85.2%, Acc of 86.8%, and an AUC value of 0.878; MRI had a Spe of 91.0%, Sen of 81.6%, and an AUC value of 0.865; the combined MSCT + MRI examination had a Sen of 90.6% and an AUC of 0.903. In the T3 stage, MRI had a significantly higher Sen (91.7%) than MSCT (80.0%), with an AUC of 0.887, while the combined MSCT + MRI examination had a Sen of 98.3% and an AUC of 0.942. In the T4 stage, the combined MSCT + MRI examination performed the best, with a Sen of 100% and an AUC of 0.933, and compared with MSCT or MRI alone, the differences were statistically significant (P < 0.05).
Conclusion
MSCT and MRI each have their own advantages in the diagnosis of different stages of CC. MSCT is suitable for initial screening in the T1-T2 stage, while MRI is more effective in assessing tumor invasiveness in the T3 and higher stages. The combined MSCT + MRI examination can provide more comprehensive diagnostic information, especially in the T4 stage, where it shows the highest Sen and Acc. Selecting the appropriate examination method based on the patient's specific condition and staging needs is of great significance in improving the diagnostic Acc of CC.
Keywords
Introduction
Colon cancer (CC) refers to malignant tumor of the digestive tract worldwide and is also among the cancers with high mortality rates.1–3 According to data from the Global Cancer Statistics, CC ranks third in incidence among all cancers, following lung and breast cancer. Its incidence and mortality rates exhibit significant regional variations, generally being higher in high-income countries and regions. 4 This variation is closely related to multiple factors, including lifestyle, dietary habits, and genetic predispositions. Notably, a family history of CC is a major risk factor, with hereditary CC syndromes such as familial adenomatous polyposis and hereditary nonpolyposis colorectal cancer (Lynch syndrome) substantially increasing individual risk. 5 Dietary habits (e.g., high-fat, low-fiber diets), smoking, excessive alcohol consumption, and a sedentary lifestyle are strongly associated with the development of CC. Common symptoms in patients include abdominal pain, bloating, changes in bowel habits, mucous or bloody stools, black stools, weight loss, fatigue, anemia, and loss of appetite.6,7 In clinical practice, early diagnosis and accurate staging of CC are crucial for developing effective treatment plans and improving patient outcomes.
Imaging technologies have played a critical role in the diagnosis and assessment of CC. CT colonography (CTC) is a non-invasive imaging modality utilized for the screening and diagnosis of colorectal cancer. This technique leverages computed tomography to provide detailed visualizations of the gastrointestinal tract. The advantages of CTC include the absence of endoscopic insertion, which minimizes patient discomfort, as well as the capability to assess other abdominal structures. However, its limitations encompass a relatively low sensitivity (Sen) for detecting small lesions, potentially leading to missed early-stage cancers, and the inherent health risks associated with radiation exposure.8,9 Multislice spiral computed tomography (MSCT) with contrast enhancement has become a commonly used tool for preoperative diagnosis of various tumors due to its high resolution, rapid scanning capabilities, and excellent tissue contrast.10,11 Liu et al., (2022) conducted MSCT and MRI examinations in patients with rectal cancer, finding that both MSCT and MRI demonstrated similar performance in the preoperative restaging of rectal cancer, although neither modality effectively staged ypT0-1 rectal cancer. 12 Liu et al. (2023) performed a retrospective analysis of MSCT findings in 27 cases of primary pulmonary mucinous epidermoid carcinoma, including lesion location, size, margins, density, enhancement patterns, and associated features. 13 The results indicated that MSCT imaging effectively revealed characteristic changes in primary pulmonary mucinous epidermoid carcinoma, which could enhance diagnostic accuracy (Acc). Existing research confirmed that MSCT with contrast enhancement can provide detailed visualization of the anatomical structures surrounding the tumor, effectively assess local tumor extension, lymph node metastases, and distant metastases.14–16 The application of MSCT does present certain limitations, such as insufficient soft tissue resolution and low Sen to intraluminal gas, which may result in diminished image quality and subsequently affect diagnostic Acc. Specifically, the presence of gas within the gastrointestinal tract can induce image artifacts, thereby reducing the clarity of surrounding soft tissue structures and impairing clinicians’ ability to accurately identify and assess lesions. To address these issues, magnetic resonance imaging (MRI) offers great advantages as a high-contrast, high-resolution imaging modality with superior soft tissue contrast and no radiation exposure, making it valuable in tumor assessment. 17 Light et al., (2024) conducted MRI scans on 181 patients with suspected radiation-induced recurrence of prostate cancer and demonstrated that MRI could accurately detect recurrent prostate cancer post-radiotherapy, with missed cancers being smaller and lower grade. 18 Relative to CT, MRI provides higher resolution and more accurate assessment in evaluating the relationship between tumors and surrounding tissues, the extent of bowel wall invasion, and local lymph node involvement. 19 Specifically, MRI offers clearer imaging when analyzing the layered structure of the bowel wall, aiding physicians in determining the depth of tumor invasion. However, MRI's limitations in assessing bone structures, calcifications, and gas restrict its use in certain clinical scenarios. 20 Therefore, combining MSCT with MRI can complement each other's deficiencies and provide more comprehensive and accurate diagnostic information.
Thus, this work applied the combined use of MSCT with contrast enhancement and MRI in the diagnosis of CC to analyze the effectiveness of various imaging technology combinations, aiming to provide more comprehensive imaging support for clinical treatment and prognostic assessment. Future research should further explore the best practices and outcomes of this combined approach to advance the field of imaging evaluation in CC.
Materials and methods
Research object
A total of 120 patients with CC confirmed by pathological biopsy at Shaanxi Second People's Hospital between January 1, 2021, and July 1, 2024, were selected as this work cohort. Additionally, 30 individuals with suspected CC but without detectable tumors during the same period were chosen as controls. Among the initially enrolled 151 patients, a total of 120 individuals were ultimately included in the study after applying the exclusion criteria. Specifically, 10 patients were excluded due to the presence of comorbid gastrointestinal diseases (such as Crohn's disease and ulcerative colitis), 6 were excluded due to recent surgical or invasive interventions, 5 were excluded due to significant motion artifacts observed in imaging, and 5 were excluded due to contraindications to the contrast agent. Consequently, a total of 31 patients were excluded from the study.
All study participants provided written informed consent after obtaining approval from their family members. This work received ethical approval from the hospital's ethics committee.
Inclusion criteria were: (1) imaging results indicated that the tumor size was ≥1 cm and suitable for assessment; (2) patients included were those with a first diagnosis, excluding cases of recurrence; (3) patients were aged 18 years or older; (4) ability to communicate effectively.
Exclusion criteria were: (1) patients with comorbid gastrointestinal diseases (such as Crohn's disease or ulcerative colitis) that may affect the assessment of colorectal cancer; (2) patients who underwent recent surgical or invasive interventions prior to imaging; (3) patients with a history of allergies or contraindications to the contrast agent used; (4) patients with missing clinical data; (5) patients exhibiting significant motion artifacts during imaging; (6) history of uterine surgery.
MSCT examination methods
The examination utilized a Philips Brilliance 64-slice CT scanner. Patients were advised to follow a low-residue diet starting 24 h prior to the scan to minimize gas and contents in the bowel. Fasting was required for 6 h before the scan, followed by a 3% contrast enema (90 mL) for retention after a water enema. During the scan, patients were positioned supine on the examination table, and intravenous injection of iohexol (1.5 mL/kg) (Beijing Beilu Pharmaceutical Co., Ltd) was administered intravenously at an infusion rate of approximately 3 mL/second. Patients were required to remain still, with the scanning duration typically ranging from a few minutes to over ten minutes. All patients underwent a three-phase enhanced scan from the chest to the pelvis to ensure a comprehensive assessment of potential tumor lesions and their impact on surrounding structures, thereby enhancing diagnostic Acc. Although this approach may result in a higher radiation dose, measures have been implemented to optimize scanning parameters, ensuring that the radiation exposure remains within safe limits and adhering to the ALARA principle (as low as reasonably achievable). Images were acquired and transferred to a computer image processing system to generate arterial, venous, and delayed-phase CT images. Scanning parameters included a tube voltage of 120 kV, tube current of 400 mA, slice thickness of 1.5 mm, and pitch of 1 mm. The scanning range extended from the lower chest to the pelvis, covering the entire abdomen and pelvis.
MRI examination methodologies
The examination was conducted using a GE 1.5 T MRI SIGNA Voyage system with a 16-channel body phased-array coil. Patients were instructed to take oral laxatives six hours prior to the examination. During the scan, patients were positioned supine on the MRI table, with adjustments made as necessary to ensure proper coverage of the scanning area. The MRI scan required the patient to remain still, with the scan area extending from the upper abdomen to the pelvis, covering the entire abdominal and pelvic regions. T2-weighted imaging of the entire abdomen and pelvis was performed, with customized small field-of-view orthogonal plane scans tailored to the tumor's location. This included targeted scanning of the tumor region to enhance image resolution and Acc. The scanning sequences included: (1) Axial T1-weighted imaging (T1WI) and T2WI with a repetition time (TR) of 577 ms, echo time (TE) of 10 ms, slice thickness (ST) of 3 mm, and interslice spacing of 0.3 mm; (2) Sagittal T2WI with a TR of 3000 ms, TE of 110 ms, ST of 3 mm, and interslice spacing of 0.3 mm; (3) Coronal T2WI with a TR of 3580 ms, TE of 120 ms, ST of 3.5 mm, and interslice spacing of 0.4 mm. During contrast-enhanced imaging, gadolinate glucosamine injection (Jiangsu Hengrui Medicine Co., Ltd) was injected intravenously at 0.2 mmol/kg body weight, with an injection rate of 2 mL/second.
T-staging criteria for CC using MRI and MSCT
MRI T staging criteria assessed tumor invasion depth as follows. T1 indicates that the tumor invades the mucosal layer only. T2 signifies invasion into the submucosal layer. T3 denotes that the tumor extends into the outer layer of the bowel wall but does not penetrate the serosal layer. T4 represents tumors that invade the serosal layer or extend to adjacent organs. This classification helps in determining the extent of local disease and planning appropriate treatment strategies.
MSCT T staging criteria were similar but with slight variations. T1 denotes that the tumor is confined to the mucosal layer. T2 describes invasion into the submucosal layer. T3 indicates that the tumor has reached the outer layer of the bowel wall without breaching the serosal layer. T4 is used when the tumor penetrates the serosal layer or invades neighboring organs.
Observation indicators
Using postoperative pathological results as the gold standard, the Sen, specificity (Spe), and Acc of MRI, MSCT, and the combined MRI and MSCT for preoperative staging were calculated. receiver operating characteristic (ROC) curves were plotted to analyze the area under the curve (AUC) of MRI, MSCT, and the combined MRI and MSCT for each stage of the disease.
Statistical analysis
The processing and analysis of the research data were conducted using the SPSS 22.0 statistical software. Continuous variables that followed a normal distribution were represented by the mean ± standard deviation (x̄ ± s), while those that did not follow a normal distribution were expressed as the median (M) with interquartile range (Q1-Q3). Categorical variables were described using frequencies and percentages (%). For continuous variables following a normal distribution, one-way analysis of variance (ANOVA) was used for intergroup comparisons. For continuous variables that did not follow a normal distribution, the Mann-Whitney U test (for two-group comparisons) or the Kruskal-Wallis H test (for comparisons involving three or more groups) was applied. For categorical variables, the chi-square test was used for intergroup comparisons. Following one-way ANOVA, if significant differences were found (P < 0.05), post hoc analyses were conducted using Fisher's PLSD test or Scheffé test (based on the F statistic) to identify significant differences between specific groups. If the assumptions for ANOVA were not met, alternative methods such as Tukey-Kramer or Bonferroni/Dunn correction could be used. These methods did not require ANOVA but had specific distributional assumptions. For diagnostic performance metrics, including Sen, Spe, Acc, and AUC, ROC curve analysis was performed. AUC values closer to 1 indicated higher diagnostic accuracy. All statistical analyses were two-sided. A P value less than 0.05 was considered statistically significant, indicating significant differences between groups.
Results
Patient clinical data
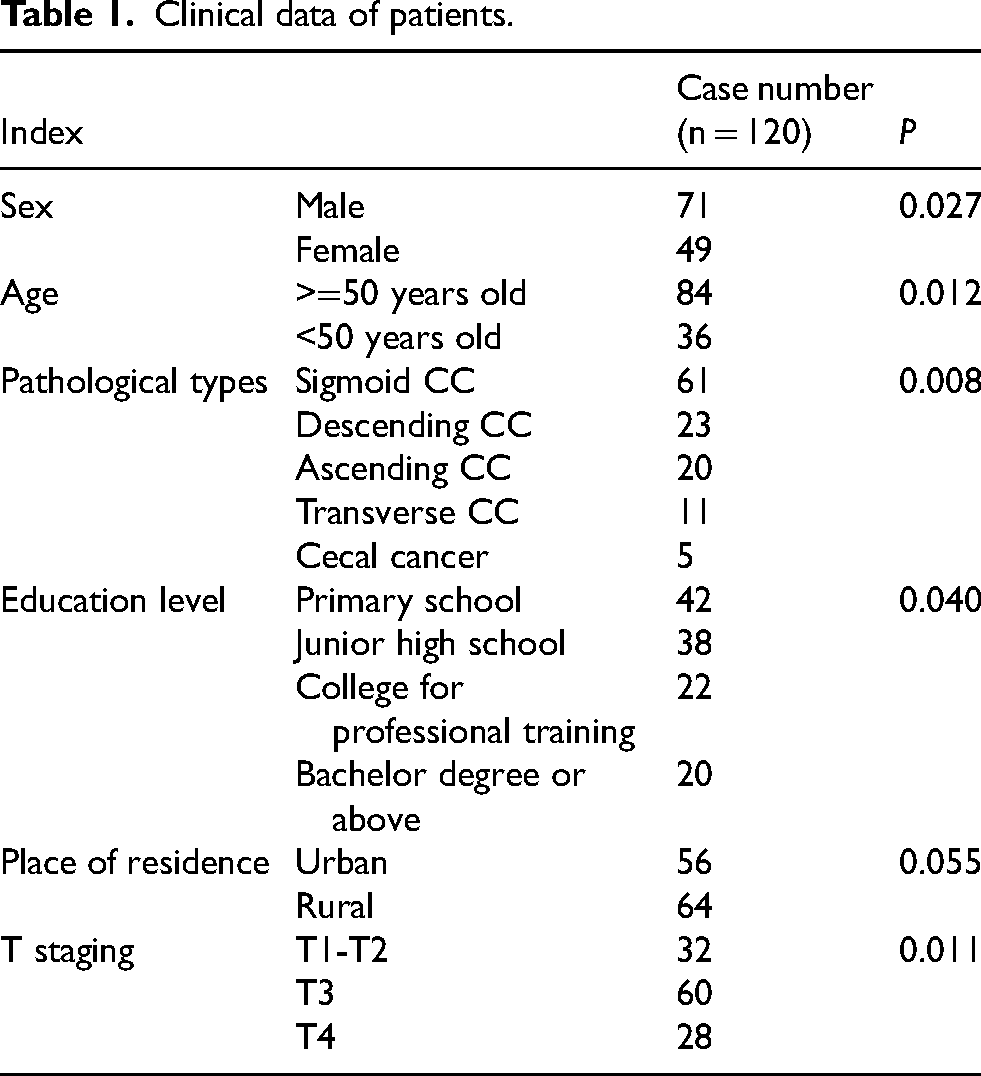
In Table 1, among the 120 patients undergoing imaging, there were more males than females, more patients aged ≥50 compared to those <50, and the highest number of cases were sigmoid CCs, with the least being cecal cancers. In terms of education, the majority had elementary or secondary school education, and the number of patients from urban and rural areas was similar. The highest number of patients were in stage T3, followed by those in stages T1-T2.
Clinical data of patients.
Patient case information
In Figure 1, a 58-year-old female patient with change in defecation habit and mild rectal bleeding was shown. The area marked by the red box in the T1-weighted MRI image displayed a low-signal lesion located in the colonic mucosa without invasion into the submucosal layer. The lesion appeared as a low-signal area in the image, consistent with the typical presentation of a tumor. The area marked by the blue box in the MSCT image showed a tumor located in the descending colon, confined within the bowel wall without significant invasion into the surrounding fat.
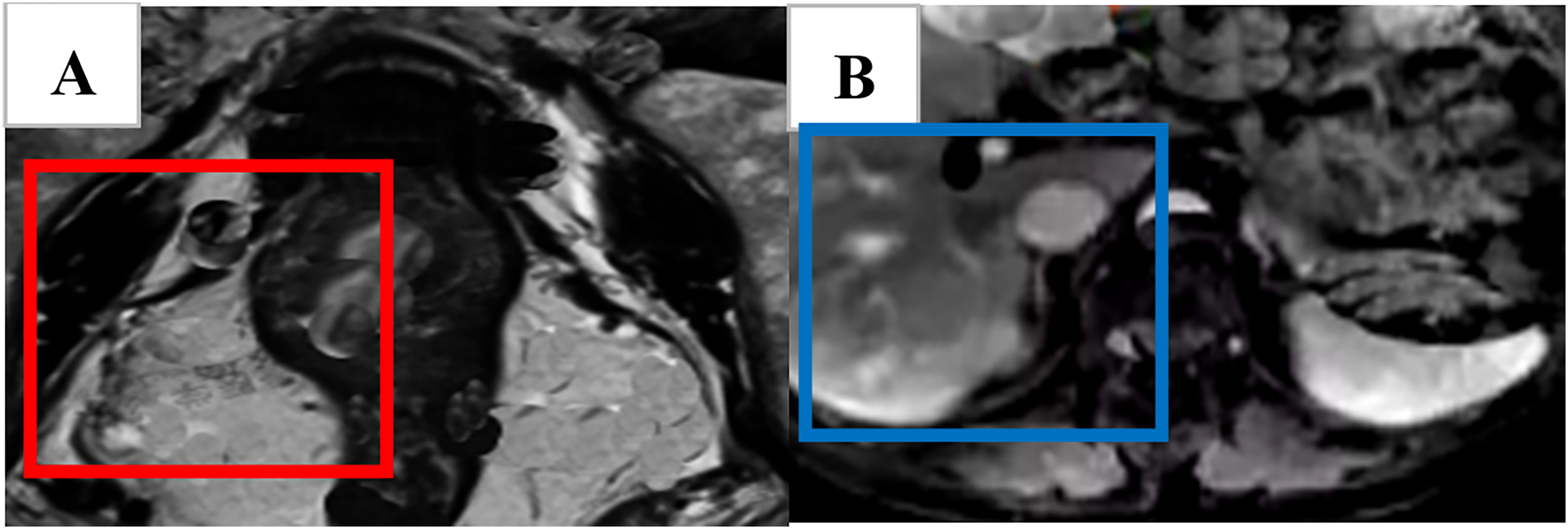
A female patient (58 years old, T1 stage).
In Figure 2, a 62-year-old male patient presented with abdominal pain and a mass on imaging. The area marked by the red box in the T2-weighted MRI image showed a high-signal lesion with bowel wall thickening and invasion into the muscularis, but without perforation of the serosa. The area marked by the blue box in the MSCT image demonstrated a tumor invading the muscularis of the colonic wall with mild edema in the surrounding fat tissue.
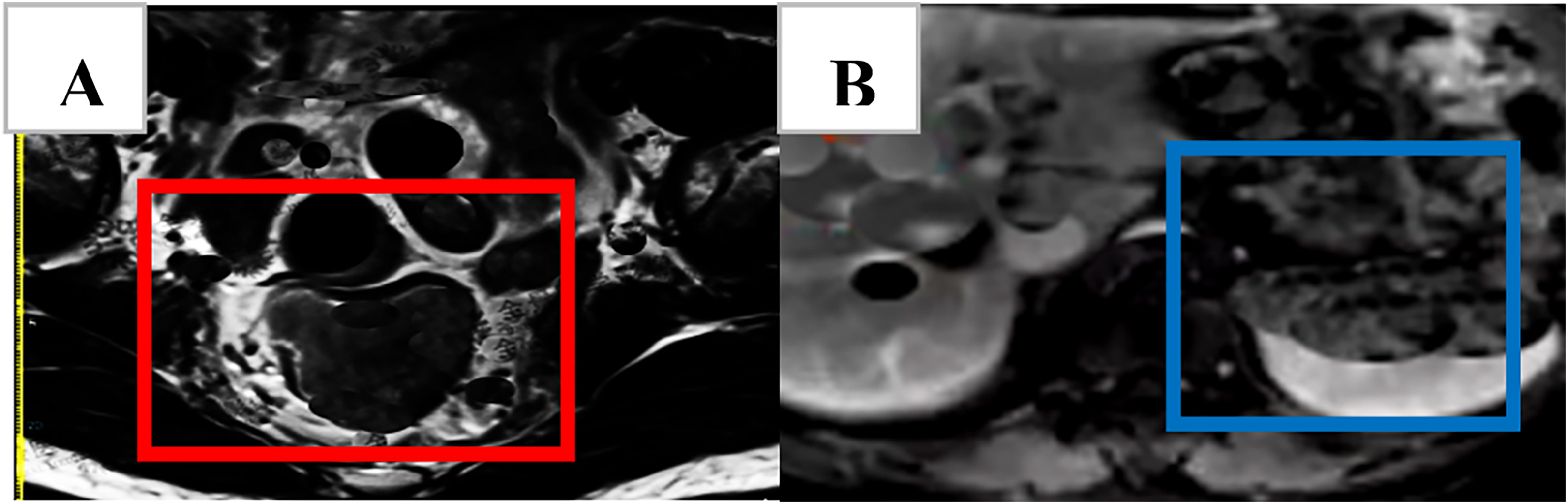
A male patient (62 years old, T2 stage).
In Figure 3, a 70-year-old female patient presented with persistent abdominal pain and weight loss, with a tumor shown on imaging. The area marked by the red box in the T2-weighted MRI image showed a high-signal lesion, with the tumor having penetrated the serosa and invaded the surrounding fat tissue. The area marked by the blue box in the MSCT image demonstrated the tumor penetrating the bowel wall, invading the serosa and extending into the surrounding fat tissue. Multiple enlarged lymph nodes were also visible in the MSCT image, suggesting that the tumor might have undergone lymphatic metastasis.

A female patient (70 years old, T3 stage).
Diagnostic performance comparison of MSCT and MRI in the T1-T2 staging
Table 2 shows that the Sen of MSCT was 85.20%, which was significantly higher than that of MRI at 81.60% (P = 0.02). This indicates that MSCT was more effective in detecting CC patients in the T1-T2 staging. The Spe of MRI was 91.00%, which was significantly higher than MSCT's 88.40%, suggesting that MRI performed better in excluding non-CC patients (P < 0.05). Additionally, the Acc of both methods was similar, with MSCT at 86.80% and MRI at 86.00%, but no significant difference was observed (P > 0.05). The AUC of the MSCT + MRI combination was 0.903, which was higher than that of MSCT alone (0.878), and the difference was statistically significant (P = 0.15). This indicated that the combination of MSCT and MRI provided superior diagnostic performance in the T1-T2 staging.
Comparison of diagnostic Sen, Spe, Acc, and AUC of MSCT and MRI for T1-T2 stage.

Note: * indicates that the difference is statistically significant (P < 0.05).
Diagnostic performance comparison of MSCT and MRI in the T3 staging
In Table 3, the Sen of MRI (91.70%) was significantly higher than that of MSCT (80.00%), indicating that MRI was more effective in identifying CC patients at the T3 stage (P = 0.03). MRI (87.50%) also slightly outperformed MSCT (85.00%) in Spe, although the difference was not statistically significant. In terms of Acc, MRI (89.40%) was superior to MSCT (82.00%), with a significant difference (P = 0.03), suggesting that MRI provided a more accurate diagnosis for the T3 stage. The MSCT + MRI combination demonstrated the highest AUC (0.942), significantly outperforming both MSCT (0.85) and MRI (0.887) (P = 0.01), indicating a substantial improvement in diagnostic accuracy for the T3 stage when using the combined modality, and demonstrating clear superiority.
Comparison of diagnostic Sen, Spe, Acc, and AUC of MSCT and MRI for T3 stage.

Note: * indicates that the difference is statistically significant (P < 0.05).
Diagnostic performance comparison of MSCT and MRI in the T4 staging
In Table 4, the MSCT + MRI combination performed best in terms of Sen, achieving 100%, which was significantly higher than both MSCT (75.00%) and MRI (79.50%). This indicated that the combination of MSCT and MRI was able to accurately identify all CC patients at the T4 stage (P = 0.02). MSCT has a higher Spe (85.00%) compared to MRI (83.00%), with the difference being statistically significant (P = 0.12). The MSCT + MRI combination also exhibited the highest Acc (91.50%), outperforming both MSCT (80.00%) and MRI (81.00%), significantly improving diagnostic accuracy for the T4 stage (P = 0.02). Furthermore, the AUC of the MSCT + MRI combination (0.933) was the highest, demonstrating its superior diagnostic performance for the T4 stage.
Comparison of diagnostic Sen, Spe, Acc, and AUC of MSCT and MRI for the T4 stage.

Note: * indicates that the difference is statistically significant (P < 0.05).
Discussion
The diagnostic performance of MSCT, MRI, and MSCT + MRI in the staging of CC (T1-T2, T3, T4) was evaluated in this work. Based on the analysis of Sen, Spe, Acc, and AUC values, as well as the results of one-way ANOVA and post hoc analysis, the following discussion was reached.
In the diagnosis of CC, MSCT has been found to have a high Sen and Acc, especially in the T1-T2 stages, where its Sen (85.2%) and Acc (86.8%) are particularly notable. Due to the high spatial resolution of CT scanning, MSCT is able to clearly display the shape and location of tumors and provide important information when tumors invade the bowel wall and surrounding structures. 21 In the T1-T2 stages, MSCT demonstrates a high Sen, effectively identifying early-stage tumors and being particularly suitable for initial screening. MRI shows better performance in the T3 and T4 stages, especially in the T3 stage, where its Sen (91.7%) is significantly higher than that of MSCT (80.0%). With its advantage in soft tissue contrast, MRI can clearly show the invasion of tumors into the bowel wall and surrounding fat, helping to assess the extent of tumor spread. 22 For T4 stage tumors, MRI can accurately display tumor penetration through the serosa and invasion into surrounding fat, providing important guidance for surgical planning.23,24 MSCT + MRI examination has been shown to outperform single methods in all stages, especially in the T4 stage, where the Sen of MSCT + MRI reaches 100%, significantly higher than that of MSCT and MRI alone. This indicates that the combination of MSCT and MRI can compensate for the shortcomings of single methods, providing more comprehensive diagnostic information, particularly in the assessment of tumor invasiveness. 25
MSCT is characterized by its high spatial resolution, which enables it to clearly display the location, size, and shape of tumors. Given its fast-scanning speed, MSCT is suitable for large-scale screening, particularly showing good effectiveness in the early diagnosis of CC.26,27 However, CT examinations involve the use of ionizing radiation, which may pose radiation risks to patients with long-term or frequent exposure. Moreover, MSCT's resolution of tumor soft tissues is inferior to that of MRI, presenting certain limitations in assessing the depth of tumor invasion. 28 MRI, on the other hand, involves no radiation and can provide images with soft tissue contrast, especially excelling in the T3 and T4 stages, where it can assess the invasiveness of tumors and their relationship with surrounding structures, thus offering high accuracy in tumor evaluation. The downside of MRI is its longer scanning time, during which patients need to remain still inside the MRI machine for an extended period. Some patients may find it difficult to tolerate due to claustrophobia or other reasons. Additionally, MRI equipment is costly, with examination fees higher than those of MSCT. It may also pose certain compatibility issues for some patients, such as those with severe obesity. The combined examination, by integrating the strengths of MSCT and MRI, can provide more comprehensive information. MSCT's strong anatomical imaging capability helps quickly determine the exact location of tumors, while MRI offers better soft tissue contrast, suitable for assessing tumor invasiveness. The combined use of these two imaging techniques can enhance diagnostic Acc, especially in the assessment of T3 and T4 stages. However, the combined examination requires longer scanning time, increasing the burden on patients. Moreover, the cost of MSCT + MRI is high, which may not be suitable for all patients, particularly those with limited financial resources. According to research data, MSCT + MRI examination performs the best across all stages, with a Sen of 100% in the T4 stage, allowing precise assessment of tumor invasiveness and its relationship with surrounding tissues. However, due to its high cost and long scanning time, it may not be accessible to every patient. Therefore, in clinical practice, MSCT and MRI can be selectively used based on specific clinical needs and patient conditions. MSCT is more appropriate as an initial screening tool in the T1-T2 stages, while MRI is more suitable in the T3 and T4 stages, especially when more accurate assessment of tumor invasiveness is required.
Conclusion
Although the sample size in this work was relatively sufficient, there may still be some selection bias. Future studies could further increase the sample size and consider the collection of multicenter data to enhance the generalizability of the results. While MRI does not involve radiation, the radiation exposure from MSCT remains an important issue. Future developments could focus on low-radiation or radiation-free imaging techniques to reduce patients’ radiation risks. Meanwhile, with the advancement of artificial intelligence (AI) and deep learning technologies, the image analysis of MSCT and MRI will become more intelligent, which may further improve diagnostic Acc, especially in tumor staging and metastasis assessment. In conclusion, MSCT, MRI, and MSCT + MRI each have their own advantages. The choice of the appropriate examination method should be made based on a comprehensive consideration of the patient's specific condition, staging requirements, and affordable costs. Moreover, future technological advancements will further improve the diagnostic precision and treatment outcomes for CC.
Footnotes
Ethics approval and consent to participate
The study was approved by the local ethics committee of the Norinco General Hospital. All experiments were performed in accordance with relevant guidelines and regulations such as the Declaration of Helsinki and the patients signed the informed consent form and agreed to be published.
Authors contributions
CL, YW, LW, JB, DW and FZ analyzed data and writing, participated in collection of data and experimental operations, participated in design testing and supervision testing. All authors read and approve the manuscript version final.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All data generated or analysed during this study are included in this published article.